
Abstract
Study Design
A prospective observational study.
Objectives
To explore the potential utility of the Coin Test as a valuable tool for assessing and diagnosing cervical spondylotic myelopathy (CSM).
Methods
In the first cohort, 36 patients with balance issues were assessed for CSM using the new Coin Test. In the second cohort, the Coin Test and mJOA scores were compared in 36 CSM patients before and 6 weeks after surgery.
Results
Among the 36 patients with balance problems who failed tandem gait test, 15 out of 16 (94%) CSM patients failed the Coin Test. The other 20 patients (56%) without CSM completed the Coin Test successfully but failed the tandem gait test for various reasons. The Coin Test demonstrated high specificity (100%) and sensitivity (94%) for diagnosing CSM in patients who failed tandem gait test. In the second cohort, the mJOA score improved significantly from 12 to 15 6 weeks postoperatively, and the Coin Test completion time decreased from 29.5 seconds to 16.4 seconds postoperatively (P < 0.0001). Higher mJOA scores correlate with better performance (shorter time) on the Coin Test, both at baseline and 6 weeks post-surgery.
Conclusion
The Coin Test is a useful tool for evaluating hand fine motor and sensory function in CSM patients with high specificity. It also can serve as a tool for assessing surgical outcomes in patients with CSM.
Keywords
Introduction
Cervical spondylotic myelopathy (CSM) stands as a significant global health concern, representing a primary cause of non-traumatic spinal cord dysfunction.1,2 This multifaceted condition presents a diverse array of motor, sensory, and autonomic deficits, often posing a diagnostic challenge of considerable complexity. While magnetic resonance imaging (MRI) has traditionally served as the gold standard for cervical stenosis diagnosis,3,4 its high cost renders it less than ideal for widespread screening of cervical myelopathy. Moreover, occasional disparities between radiographic findings and patients’ symptomatic experiences emphasize the need for supplementary clinical assessments. 5
The Available Clinical Tests Used to Diagnose Cervical Myelopathy in Clinical Practice.
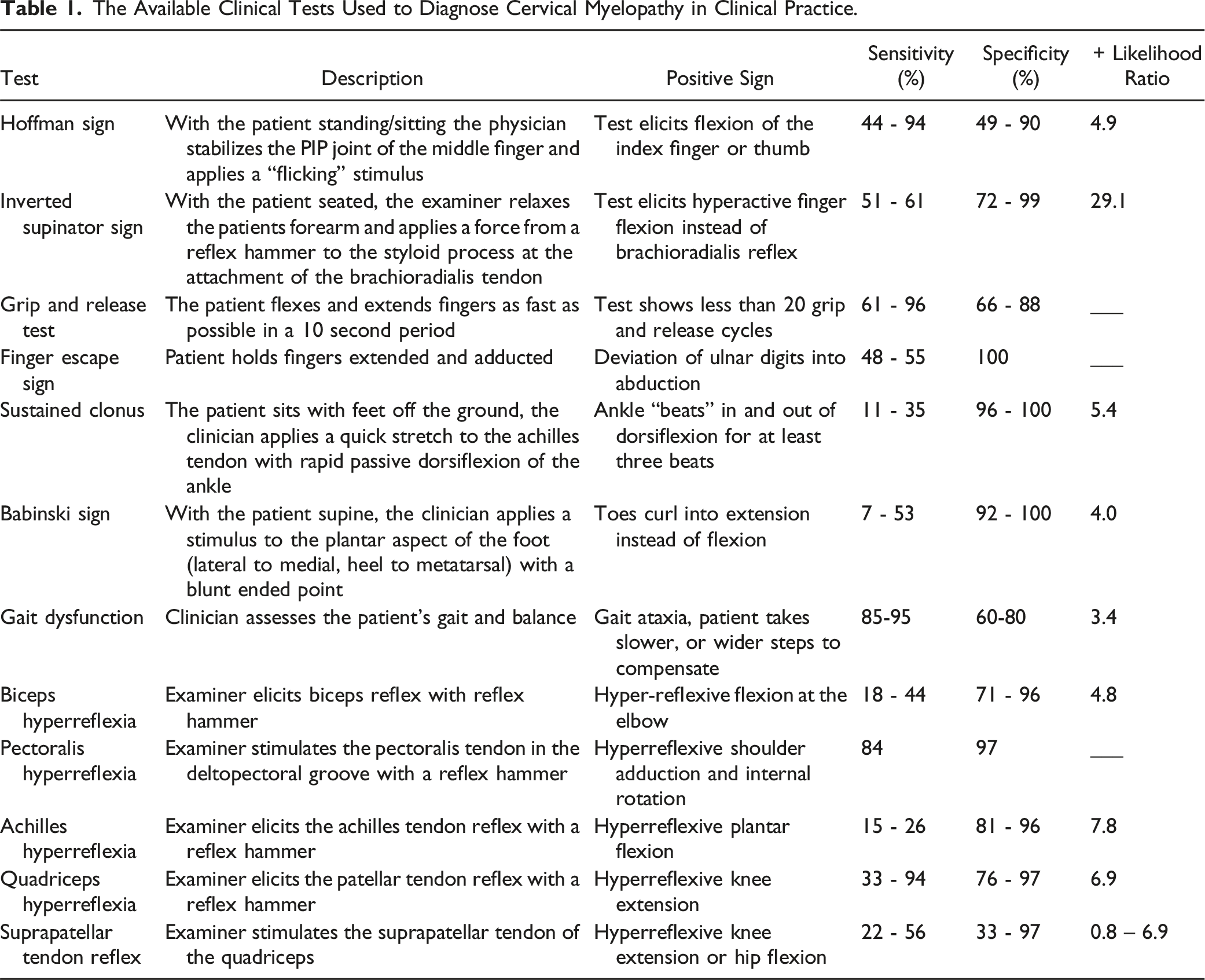
Early signs of CSM include gait instability and fine motor dysfunction.7-10 The tandem gait examination, commonly employed in diagnosing neurological and vestibular disorders, including myelopathy,11,12 is hampered by its low specificity. Various pathologies can influence tandem gait, and it mainly evaluates lower extremity function.
The only available test to assess upper extremity function is the 10-second grip-and-release test, often referred to as the “myelopathy hand” test, which uniquely evaluates hand dexterity.13,14 However, this test has notable limitations: it relies heavily on the subjective assessment of the examiner and does not effectively measure fine motor movements or sensory function, which are critical, as many patients with cervical myelopathy experience hand numbness. Thus, an easy and objective modality to measure fine motor and sensory function and coordination of upper extremity is urgently needed.
To address these critical limitations, we introduce the “Coin Test” as a novel diagnostic tool for evaluating upper extremity function in patients with CSM. This test requires a well-controlled coordination and directional movement of the arm and fingers. In this simple yet insightful assessment, patients are instructed to stack five penny coins on a flat surface—a seemingly straightforward task with profound diagnostic significance. While unaffected individuals typically perform with ease, CSM patients often encounter significant challenges, highlighting impairments in fine motor movements and sensory functions. The elegance of the Coin Test lies in its ability to illuminate subtle difficulties experienced by individuals with CSM in a practical, clinically relevant manner.
This pilot study includes two cohorts of patients and has two aims. Cohort 1 and Aim 1: To explore whether the Coin Test, when used in conjunction with the Tandem Gait Test, increases the specificity of cervical myelopathy diagnosis. Cohort 2 and Aim 2: To evaluate whether the Coin Test can serve as a tool for assessing surgical outcomes in patients with cervical myelopathy. Overall, this study aims to explore the potential utility of the Coin Test as a valuable tool for assessing, screening, and diagnosing cervical myelopathy, highlighting its promise as a practical and objective addition to the diagnostic toolkit.
Methods
Patient Recruitment: Cohort 1
A pilot study was conducted following the Institutional Review Board approval, involving 36 consecutive patients from October 2022 to August 2023, all presenting with symptoms of lower back pain or leg pain, but the clinical history and examinations raised concerns for cervical myelopathy due to balance issues and inability to perform Tandem gait. MRIs were ordered to evaluate myelopathy. Additionally, all patients underwent the novel Coin Test with their dominant hand. Their performances were video-recorded and timed. Neurologist consultations were sought for patients presenting with neuropathic symptoms, and reasons for inability to perform Tandem gait were evaluated. Control groups consisted of patients with cervical spondylosis but without cervical stenosis or dominant side radiculopathy confirmed by MRI.
Cohort 2
Another pilot study was conducted following the Institutional Review Board approval, involving 36 consecutive patients diagnosed with CSM from January 2023 to December 2023. CSM diagnosis was established based on clinical symptoms and the presence of cervical stenosis with or without myelomalacia on MRI studies. Prior to surgery, all patients took the new Coin Test, and the test was repeated 6 weeks after surgery, which included anterior cervical discectomy and fusion or laminoplasty. The modified Japanese Orthopaedic Association (mJOA) questionnaire was conducted at the same time points for assessment.
Coin Test (Figure 1)
The Coin Test involves placing a stack of five-penny coins randomly on a level tabletop, equidistant from the participant. Subjects are instructed to move one coin at a time, using their dominant hand, to create another stack. The goal is to transfer all five pennies to a new stack in the shortest time possible, maintaining precision and controlled movement. The entire process is video recorded to provide an objective measure for assessment, timing, and documentation. The time taken by the participant to complete the task is carefully measured using a stopwatch or digital timer, crucial for evaluating the speed and efficiency of their fine motor skills in diagnosing CSM. Participants are assessed based on time to completion, accuracy, and manual control by two investigators. Illustration of the Coin Test. Patients are instructed to use their dominant hand to move a stack of coins and create a new stack approximately 5 cm (2 inches) away. The procedure is designed to evaluate hand sensation, coordination and dexterity.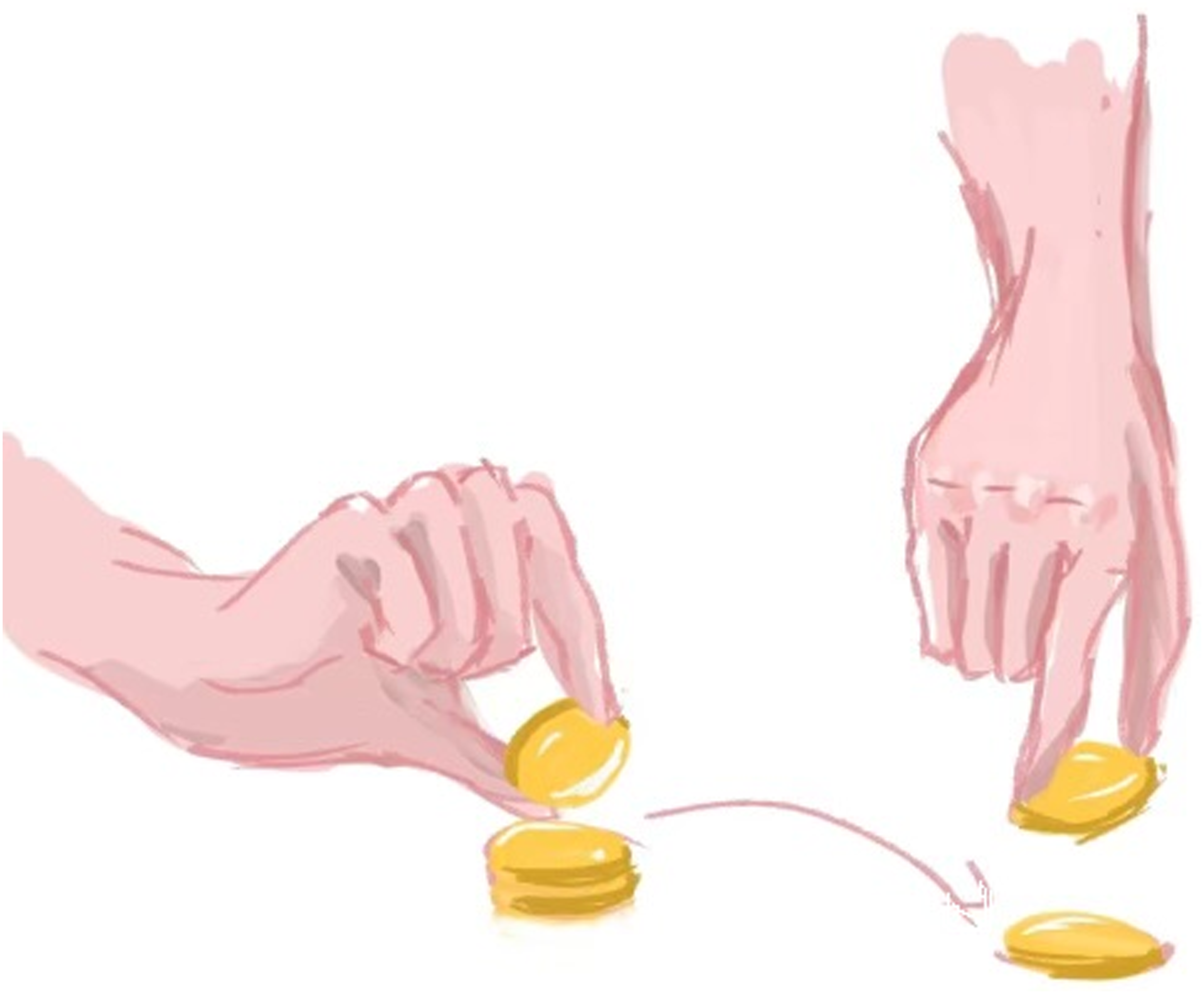
Statistical Analysis
Continuous data are presented as mean and categorical data as number (percentage, %). Two-sided P < 0.05 was considered statistically significant, and calculated by One-way ANOVA followed with Dunnett’s using Prism 9. Data that support the findings of this study are available from the corresponding author upon reasonable request.
Results
For normal controls, the average time to complete the Coin Test was 10.15 seconds, with two standard deviations of 4.06 seconds. Therefore, we considered a completion time longer than 15 seconds to be abnormal.
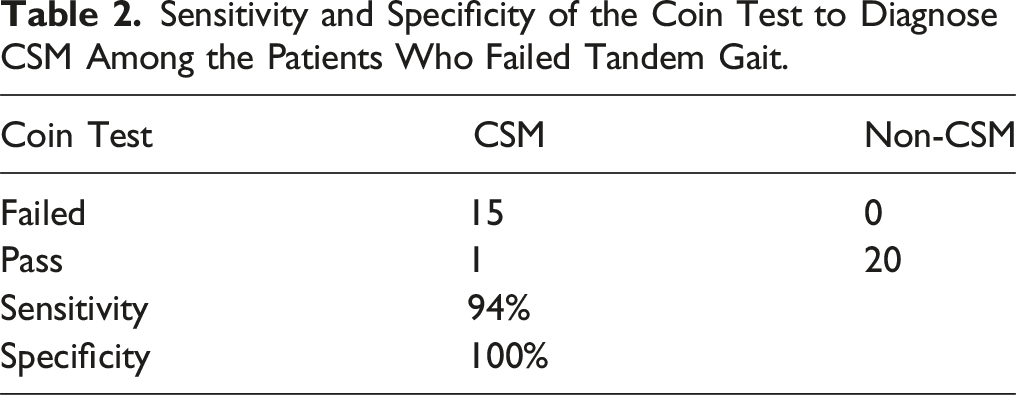
In the first cohort, they were patients with the concern of myelopathy as they could not perform the Tandem gait test. In order to evaluate hand dexterity function, the Coin Test was performed in addition to Tandem gait test. The average age of patients was 69 years (range: 59 - 89), with females comprising 42% of the cohort. Among the 36 patients, only 16 (44%) had CSM, which hindered their ability to perform Tandem gait and the Coin Test, except for one patient (6%) who passed the Coin Test with a completion time of 12 seconds (Figure 2). The remaining 20 patients (56%) without CSM failed Tandem gait test but successfully passed the Coin Test (Figure 2). Among these 20 patients, 12 (60%) had lumbar stenosis. The remaining 8 patients (40%) failed Tandem gait test due to different factors such as advanced age, diabetes, peripheral neuropathy, minor stroke, obesity, thoracic stenosis, and multiple sclerosis, highlighting the diverse array of factors contributing to Tandem gait impairments in these cases. The sensitivity of the Coin Test for CSM patients who failed Tandem gait was 94% with a specificity of 100% (Table 2). Diagnoses for patients with failed Tandem gait. Sensitivity and Specificity of the Coin Test to Diagnose CSM Among the Patients Who Failed Tandem Gait.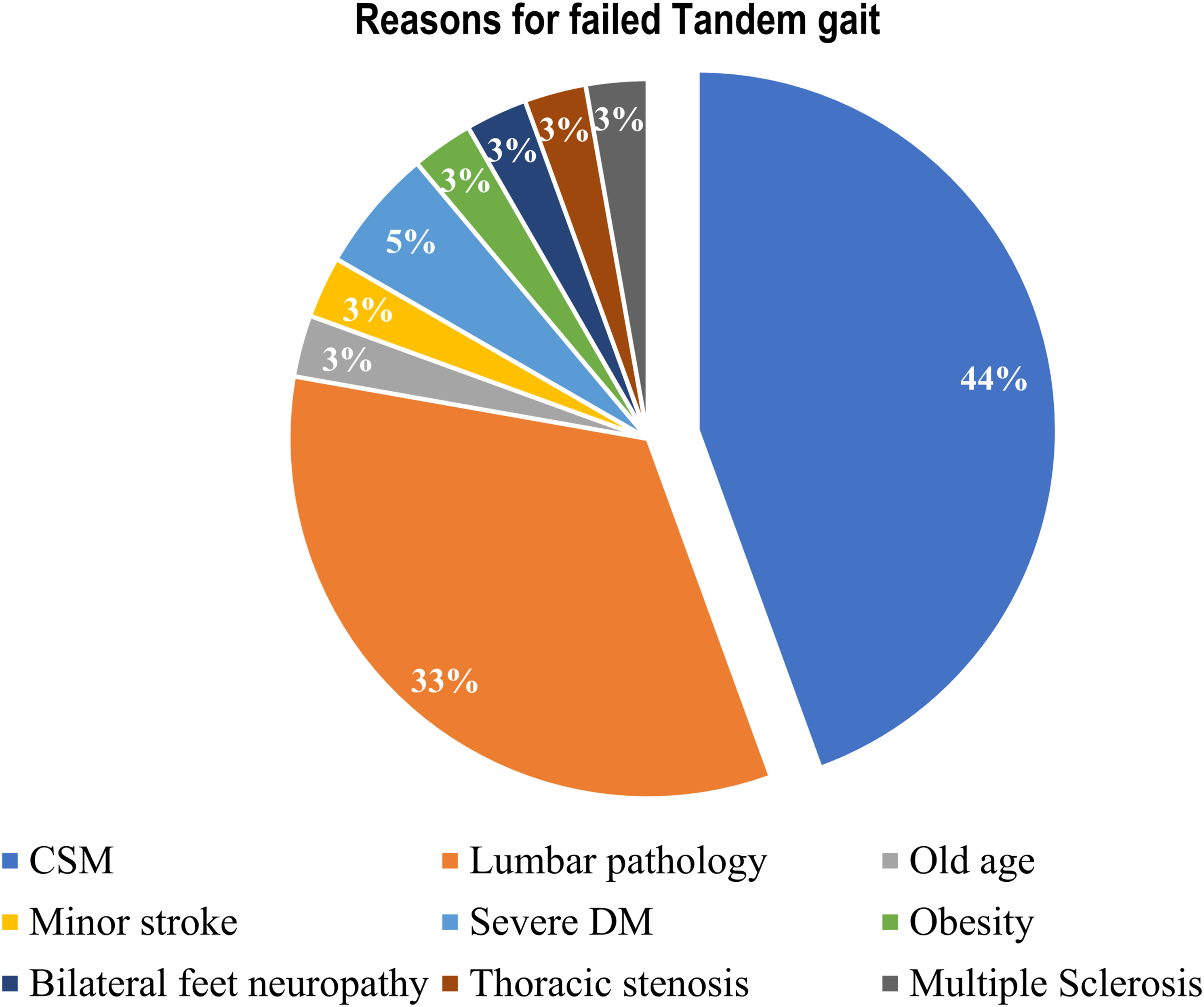
A 75-year-old male complained of left leg numbness and poor balance following a L5/S1 posterior fusion at an outside hospital in 2017. He could not perform Tandem gait test but successfully completed the Coin Test in 10 seconds. Clinical assessment revealed a positive Hoffman’s sign and a negative Babinski’s test. However, hyporeflexia was observed in both bilateral upper and lower extremities. Lumbar spine MRI revealed severe stenosis at L2/3 and moderate to severe stenosis at L3/4 (Figures 3(A) and (B)). Cervical and thoracic spine MRIs were ordered to evaluate myelopathy, which showed no high-grade stenosis (Figures 3(C) and (D)). Neurology electromyography study indicated inactive left L3/4 radiculopathy, with no evidence of large fiber polyneuropathy. Lumbar decompression surgery at L2/3 and L3/4 resulted in markedly improved balance and capability to perform Tandem gait. Case example 1. A 75-year-old male exhibits a failed tandem gait yet successfully passes the coin test. (A) and (B): sagittal and axial MRI images of the lumbar spine, revealing severe stenosis at the L2/3 level. (C) and (D): sagittal cuts of the cervical and thoracic spine, demonstrating an absence of high-grade stenosis in these regions.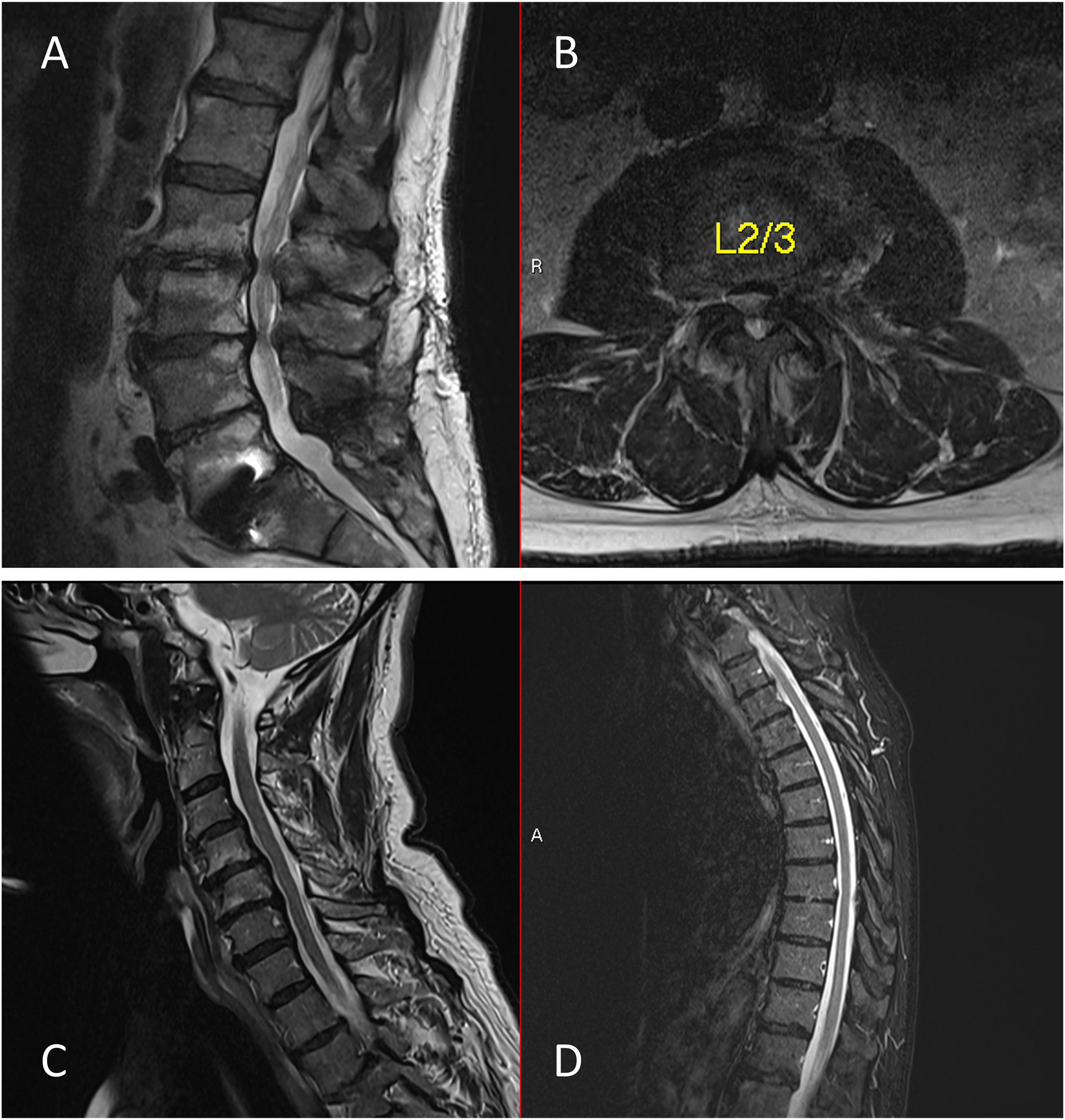
A 68-year-old male presented with lower back and bilateral leg pain for 1 year as well as balance problems. X-rays revealed grade 1 L4/5 spondylolisthesis, and MRI showed L4/5 stenosis (Figures 4(A) and (B)). Unable to perform the tandem gait test, he also could not complete the Coin Test (Supplemental video 1). His Hoffman’s test was negative on both sides. He exhibited hyperreflexia in the upper extremities and hyporeflexia in the lower extremities. A subsequent MRI of the cervical spine revealed C5-7 stenosis. Following anterior cervical discectomy and fusion (ACDF) surgery at C5-7, his Coin Test performance remarkably improved, completing it in 26 seconds (Supplemental video 2). Case example 2. Depicting a 68-year-old male experiencing bilateral leg pain, this figure corresponds to examinations revealing both failed tandem gait and coin test. (A): a lumbar lateral X-ray, indicating grade 1 L4/5 spondylolisthesis. (B): an MRI of the lumbar spine, confirming stenosis at the L4/5 level. (C): an MRI of the cervical spine, uncovering moderate to severe stenosis at C5/6 and C6/7. (D): a lateral cervical spine X-ray post-anterior cervical discectomy and fusion (ACDF) at C5-7.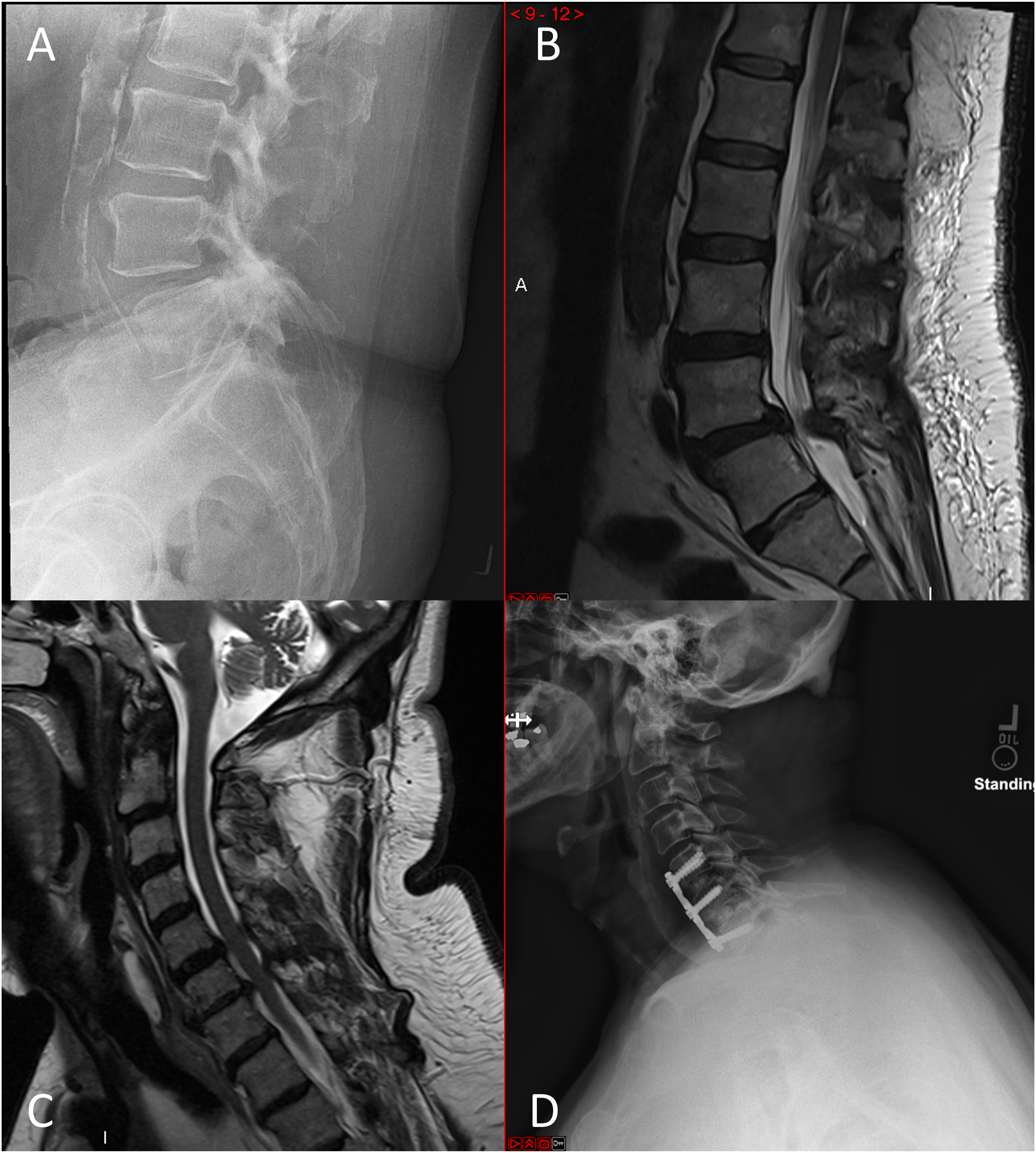
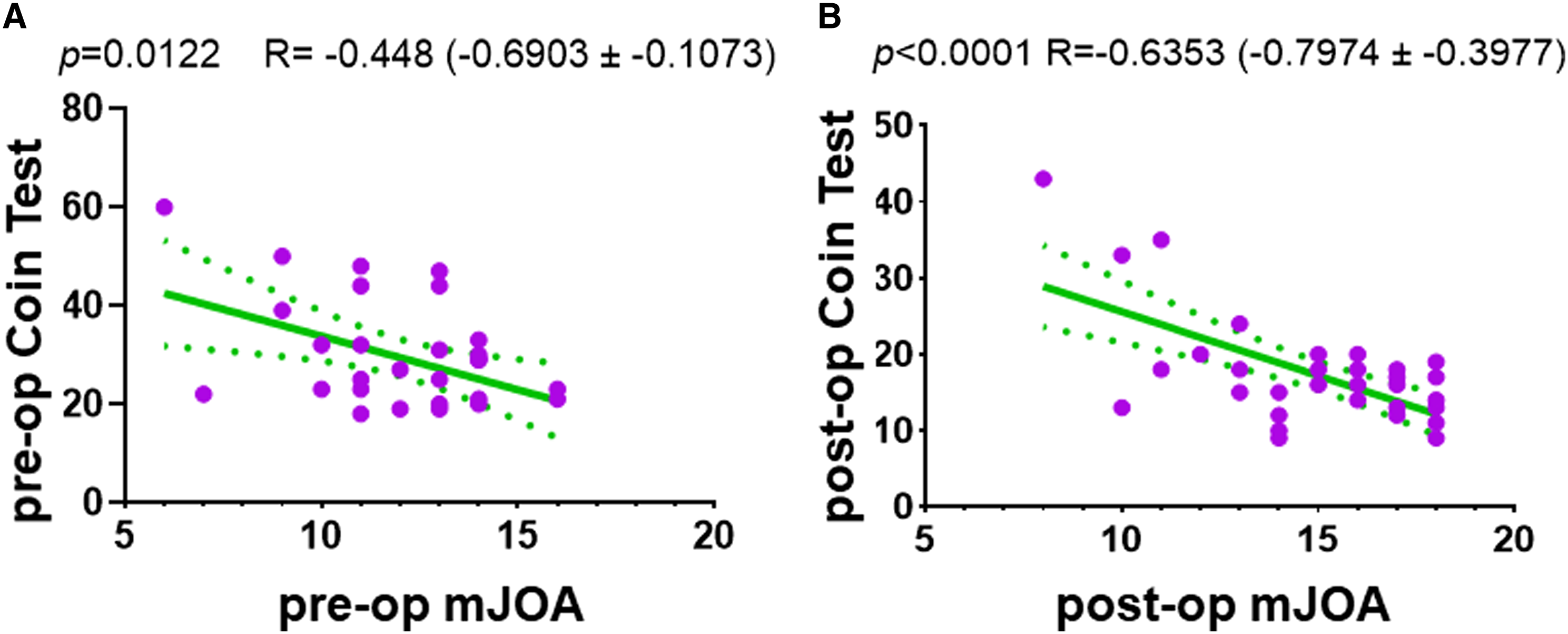
In the second Cohort of 36 patients with CSM, the average age of patients was 67 years (range: 49 - 82), with females comprising 50% of the cohort. Among the 36 patients, the mJOA score improved from 12 to 15 6 weeks postoperatively (P < 0.0001). Five patients could not complete Coin Test before surgery, but could complete the Coin Test successfully from 17 to 35 seconds after surgery. For the rest 31 patients, the time to complete the Coin Test decreased from 29.5 econds preoperatively to 16.4 seconds 6 weeks postoperatively (P < 0.0001) (Figure 5). Additionally, higher mJOA scores correlate with better performance (shorter time) on the Coin Test, both at baseline and 6 weeks post-surgery (Figure 6). mJOA scores and time (seconds) to complete the Coin Test for patients with CSM before and 6-week after surgery. The mJOA score improved from 11 to 15 6 weeks postoperatively (P < 0.0001). The time to complete the Coin Test decreased from 33.7 seconds preoperatively to 15.6 seconds 6 weeks postoperatively (P < 0.0001). The time taken to perform the Coin Test correlates significantly with modified Japanese Orthopaedic Association (mJOA) scores. (A) negative correlation between mJOA scores and the time required to complete the Coin Test is observed both pre-operatively (A) and 6 weeks post-operatively (B). The green solid lines represent the linear regression line, while the dotted green lines indicate the standard deviation.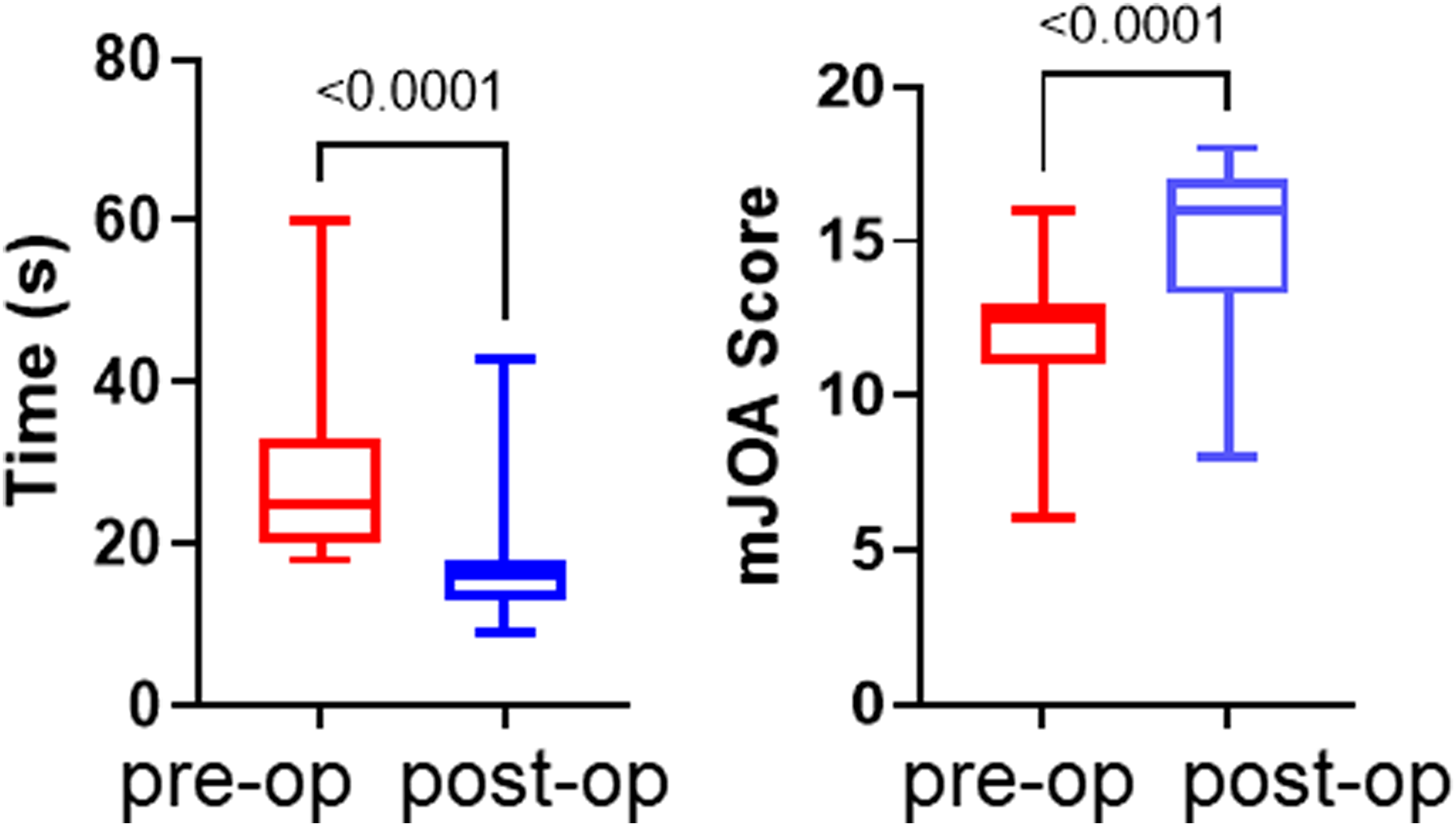
Discussion
Our study presents initial findings on the Coin Test, a new tool for evaluating hand dexterity in patients with CSM.
Shortcoming of Tandem Gait Test and Current CSM Exams
In the clinic, when a patient exhibits difficulty performing the Tandem gait test and presents with balance issues similar to those observed in cohort 1, our standard protocol involves ordering an MRI of the cervical spine to rule out Cervical Spondylotic Myelopathy (CSM). Harrop et al
15
2010 conducted a retrospective analysis of 103 patients evaluated for cervical degeneration to determine the utility of various physical examination findings in CSM. In their cohort of patients with CSM, they found the following prevalence of symptoms: gait abnormality (91%), any hyperreflexia (85%), lower extremity hyperreflexia (81%), upper extremity hyperreflexia (67%), Hoffman sign (83%), and Babinski reflex (44%). Gait dysfunction remains one of the most significant hallmarks of this condition but is significantly limited by a specificity of 60%–80% in the literature, as numerous pathologies can affect Tandem gait.
16
As shown in our current study, only 44% of patients who could not perform Tandem gait were diagnosed with cervical CSM. The remaining 56% had a variety of pathologies, including thoracic stenosis, lumbar stenosis, diabetes, neuropathy, obesity, aging, stroke, and multiple sclerosis (Figure 2), all of which can impact a patient’s ability to perform the Tandem Gait test. A. B. C. D.
Combination of CSM Exams
Many studies have investigated the validity and utility of clinical tests for diagnosing CSM.7,8,19 Cook et al. (2009) examined the reliability and diagnostic accuracy of seven physical exam maneuvers for CSM 20 . They found that combining these tests did not yield improved accuracy compared to single tests used in isolation. However, selected combinations of clinical findings, such as gait deviation, Hoffman’s test, inverted supinator sign, Babinski test, and age >45 years, were effective in ruling out and ruling in CSM. 21
Tandem Gait Plus the Coin Test
Tandem gait test primarily focuses on evaluating lower extremity function. By incorporating the Coin Test, which assesses both motor and sensory functions of the upper extremities, we may achieve a more accurate diagnostic evaluation for CSM. In our study, remarkably, all 20 patients (56%) without CSM but experiencing Tandem gait difficulty successfully passed the Coin Test, highlighting its potential as a complementary assessment tool to diagnose CSM. Conversely, with the exception of one patient (6%), all CSM patients failed the Coin Test. This leads us to believe that integrating the Tandem gait assessment (reflective of lower extremity function) with the Coin Test (evaluating upper extremity function both fine motor and sensation) enhances both sensitivity and specificity in diagnosing CSM. If a patient with balance issues cannot perform the Tandem Gait test but can do the Coin Test, they are unlikely to have cervical myelopathy. If they fail both tests, they almost certainly have cervical myelopathy.
Surgical Outcome Evaluation
The modified Japanese Orthopaedic Association (mJOA) score stands as a widely accepted clinical scoring system for evaluating the severity of cervical myelopathy.14,22 This comprehensive scoring system assesses various clinical parameters, including upper and lower extremity motor function, upper extremity sensory function, and bladder function. 6 However, the mJOA score is not tangible.
From the cohort 2 study, we showed that the Coin Test could be also used as a tool to evaluate the outcome of a procedure. We observed a significant improvement in the mJOA score from 12 to 15, and a notable reduction in the time taken to perform the coin test from 29 seconds to 16 seconds (Figure 5). Notably, five patients who could not complete Coin Test regained the capability to finish the Coin Test within 17 to 35 seconds. These patients were tested multiple times preoperatively, but consistently failed to complete the test, excluding the possibility of repetition improvement. Furthermore, patients with better mJOA scores got a greater performance in the Coin Test (Figure 6). This suggests that we can utilize this simple Coin Test to evaluate surgical outcomes in CSM treatment. Previously, Hassanzadeh et al. (2021) demonstrated that compared to controls, CSM patients exhibited slower, shorter, and broader gait patterns, with significantly increased compensatory angular momentum in various planes to maintain dynamic balance. 23 Furthermore, gait parameters improved post-surgery. However, gait analysis necessitates specialized equipment, technology, and trained personnel, whereas any health care professional or even patients themselves can administer the Coin Test.
Limitations
Several limitations are inherent in this pilot study. First, the Coin Test was exclusively administered to patients unable to perform Tandem gait in cohort 1, limiting its assessment scope. To comprehensively establish the specificity and sensitivity of the Coin Test itself for cervical myelopathy, it is imperative to evaluate a broader spectrum of patients, including those with cervical pathology who can and cannot perform Tandem gait. For example, patients with severe cervical radiculopathy, especially C6 radiculopathy on the dominant side affecting thumb and index, might has difficulty with Coin Test. Additionally, conditions such as brain pathology, rheumatoid arthritis, hand contracture, severe carpal tunnel disease, peripheral neuropathy, or other neurological disorders and long fingernails may affect the Coin Test. This necessitates the implementation of a clinical trial involving a substantial number of participants. This preliminary study serves as a foundation for conducting a power analysis, and we are actively recruiting at least 500 patients with neck symptoms, both with and without myelopathy, to better define the sensitivity and specificity of the Coin Test for diagnosing cervical myelopathy. Second, while improved Coin Test performance was observed following surgical decompression, the long-term effects require further investigation. A longitudinal analysis is essential to capture sustained changes over an extended period. Third, we only performed the Coin Test with the patients’ dominant hand. Non-dominant hand may show more differences for patients with myelopathy. Lastly, the current reliance on the time taken to complete the Coin Test as the primary parameter warrants expansion. Future research should encompass additional metrics such as accuracy, instances of dropping coins, hand shaking, and the inadvertent picking up of two coins instead of one, ensuring a more comprehensive and nuanced evaluation of hand dexterity.
Advantages
Several key advantages make our proposed novel Coin Test as a promising diagnostic tool for CSM, thereby enhancing our ability to understand and address the complexities of CSM. The Coin Test (hand sensation and fine motor function) plus Tandem gait (lower extremity motor function) demonstrates an extraordinary level of specificity, approaching 100%. This remarkable attribute ensures that the test reliably identifies individuals with impaired hand dexterity and sensation, thereby aiding in precise diagnosis and treatment planning. We routinely inquire about buttoning difficulty in patients with cervical stenosis, but this measure is often subjective and difficult to quantify. Unlike the Coin Test, which utilizes standardized coins (pennies) that are readily available, a buttoning test would require uniform button sizes and buttonholes to ensure consistency, which complicates its implementation. One of the most compelling aspects of the Coin Test is its accessibility. It requires no specialized training for examiners and can be conducted by a wide range of health care professionals, from specialists to primary care physicians. Moreover, it is sufficiently simple for patients to perform with appropriate guidance. This simplicity enhances the assessment process, making it widely available for use across diverse clinical settings. Furthermore, the materials needed for the test, that is penny coins, are ubiquitous and easily obtainable. We used pennies in our study. This simplicity streamlines the implementation of the test into routine clinical evaluations, eliminating barriers to its adoption. Beyond its diagnostic utility, the Coin Test has the potential to serve as a valuable outcome measure for assessing the effectiveness of surgical interventions in patients with CSM. By quantifying changes in hand dexterity post-surgery, it provides a tangible metric for evaluating treatment success and tailoring rehabilitation strategies.
Supplemental Material
Supplemental Material
Footnotes
Acknowledgements
We thank all patients who participated in this study and the spine clinic staff for assisting in patient assessing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIH; R01AR078888-01A1, R21 AR078547, R21AR082052.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.