
Abstract
Study Design
Retrospective multicenter study.
Objectives
To investigate the impact of preoperative cervical range of motion (ROM) on clinical outcomes after posterior decompression for cervical ossification of the posterior longitudinal ligament (OPLL).
Methods
We analyzed data from 156 patients with cervical OPLL who underwent posterior decompression and were followed for at least 2 years. Patients were divided into two groups based on preoperative gap ROM, which was a novel indicator representing the difference between flexion and extension ROM: the gROM <0° and >0° groups, and their outcomes were compared.
Results
There were no significant differences in patient demographics or surgical details between the gROM <0° and >0° groups. The gROM <0° group exhibited less lordosis in C2-7 angles before and after surgery compared to the gROM >0° group. Cervical ROM significantly decreased following posterior decompression regardless of whether preoperative gROM was <0° or >0°. Meanwhile, the incidence of perioperative complications was similar between the two groups. Furthermore, both groups showed significant improvement in Japanese Orthopaedic Association (JOA) scores postoperatively; however, there were no significant group differences in JOA scores, recovery rates, or visual analog scale for neck pain between the two groups at the preoperation and final follow-up.
Conclusions
The incidence of perioperative complications and postoperative clinical outcomes were comparable regardless of the magnitude of preoperative cervical gROM. Although cervical ROM decrease postoperatively, posterior decompression for cervical OPLL can offer favorable clinical outcomes irrespective of the preoperative cervical ROM magnitude, consequently.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) occurs most frequently in the cervical spine and is one of the main causes of degenerative cervical myelopathy, particularly prevalent in Asian populations.1-4 Roughly half of individuals with cervical OPLL experience progression, resulting in symptomatic myelopathy. Posterior decompression is a common intervention for cervical OPLL, aimed at halting neurological deterioration, with generally favorable and stable postoperative clinical outcomes.3,5,6 Laminoplasty and selective laminectomy with muscle preservation are preferred techniques as they maintain cervical spine motion without fusion, offering the benefits of preserving motion while reducing instability and kyphosis.7-12 In addition, adequate decompression is achieved by maintaining cervical lordosis, allowing a posterior shift of the spinal cord post-procedure. 13 However, after cervical posterior decompression, loss of cervical lordosis can sometimes lead to inadequate spinal cord decompression and contribute to neck pain.13,14 Furthermore, postoperative loss of cervical lordosis in OPLL may necessitate reoperation due to increased ossification. 15 Therefore, preventing postoperative loss of cervical lordosis following posterior decompression and identifying potential risk factors remain crucial objectives.
Cervical range of motion (ROM) has been closely linked to loss of cervical lordosis after posterior decompression.16-18 Studies have identified a greater flexion ROM (fROM) as a risk factor for kyphotic change after posterior decompression, 16 while a smaller extension ROM (eROM) has been deemed the definitive predictor. 17 Despite presenting differing conclusions, these studies would underscore a common phenomenon: an imbalance characterized by a greater fROM and smaller eROM, contributing to an increased risk of kyphotic change after posterior decompression. Nevertheless, in reality, fROM and eROM do not always exhibit a complementary relationship, as the total cervical ROM varies among individuals. An indicator capable of relatively representing both fROM and eROM independently may prove even more effective in predicting loss of cervical lordosis after surgery than considering fROM or eROM alone. Recent study demonstrated that the gROM (a novel indicator: the gap between fROM and eROM, which independently represents a greater fROM and/or smaller eROM) was a highly useful indicator for predicting whether cervical lordosis was markedly lost after posterior decompression. 18 However, the aforementioned studies focused on patients with cervical spondylotic myelopathy (CSM). As the primary lesion in CSM arises from age-related degeneration, its pathological condition differs fundamentally from that of cervical OPLL.19,20 This discrepancy in pathology can influence postoperative functional recovery, spinal alignment, and the incidence of complications.3,11,19,20 Therefore, exploring the influence of cervical ROM on clinical outcomes in cervical OPLL is imperative to ascertain the advantages of posterior decompression for patients with this condition.
This study aimed to examine the alterations in pre- and postoperative cervical ROM among patients with cervical OPLL and evaluate how it affects clinical outcomes following posterior decompression, by comparing perioperative complications, changes in cervical sagittal alignment, and postoperative outcomes.
Materials and Methods
Study Design, Patient Demographics, and Characteristics
This retrospective cohort study included 156 patients diagnosed with cervical OPLL who underwent posterior decompression across 14 Japanese medical institutions from January 2012 to December 2014. All investigators were board-certified orthopaedics spine surgeons (a surgical track record of over 300 spine and spinal cord operations, including at least 200 as the primary surgeon, with a minimum of 20 cervical and 60 lumbar surgeries, the average duration of surgical experience was 18.9 ± 7.9 years). Inclusion criteria necessitated: 1) Manifestation of at least one clinical sign indicative of myelopathy, 2) Radiological evidence demonstrating cervical spinal cord compression via magnetic resonance imaging (MRI) alongside OPLL detection on X-ray or computed tomography (CT), 3) Absence of prior cervical spine surgeries, and 4) A minimum follow-up period of 2 years post-surgery. Conversely, patients exhibiting asymptomatic status or diagnosed with concurrent conditions such as CSM, cervical kyphosis, neoplastic spinal disease, rheumatoid arthritis, ankylosing spondylitis, active infection, or concomitant lumbar stenosis were excluded.
Decisions regarding surgical indication, techniques employed, and extent of decompression were collaboratively determined by a spine team at each institution. The study encompassed three distinct surgical techniques: expansive open-door laminoplasty (OD), double-door laminoplasty (DD), and selective laminectomy with muscle preservation (SL).7-10 Among these, OD, DD, and SL were respectively performed at 10, 3, and 3 institutions. Generally, these techniques were recommended in cases of multilevel stenosis featuring a narrow spinal canal and devoid of kyphotic cervical alignment.
Ethical clearance for the study was obtained from the Ethics and Institutional Review Board at Keio University School of Medicine (approval number: #20110142), with all participants providing informed consent before undergoing surgical interventions.
Radiographical Images and MRI Findings
In this investigation, the principal investigator thoroughly explained the measurement techniques to the board-certified orthopedic spine surgeons, based on radiological evaluation methods outlined in previous research. 18 The surgeons at each institution then conducted cervical spine assessments by measuring intermittent C2-7 angles from plain radiographs in neutral, flexion, and extension positions at two distinct time points: “preoperation” and “final follow-up.” The evaluation of C2-7 angles involved quantifying the Cobb angle, which represents the angle between the lower endplate of the C2 vertebra and the lower endplate of the C7 vertebra. A positive value for the C2-7 angle indicated lordosis, while a negative value denoted kyphosis. Moreover, total ROM was determined by subtracting the flexion C2-7 angle from the extension angle. fROM indicated the difference between C2-7 angles in neutral and flexion positions, and eROM indicated the difference between C2-7 angles in neutral and extension positions. The gROM was defined as follows: gROM (°) = fROM − eROM. Various types of OPLL were categorized as localized, segmental, continuous, and mixed. The occupying ratio of OPLL and the K-line were evaluated using preoperative plain X-ray or CT. Preoperative MRI was performed to assess stenotic levels in OPLL and the presence of intraspinal high signal intensity areas on T2-weighted images.
To investigate the impact of preoperative cervical ROM on postoperative radiographic and clinical outcomes, the 156 patients with cervical OPLL in this study were stratified into two groups based on the magnitude of preoperative gROM, defined as the gROM <0° and >0° groups, respectively. A retrospective compilation of demographic information, medical history, symptomatology, imaging findings, surgical summaries, and other pertinent data was examined for all subjects in this study.
Clinical Outcomes
The evaluation of clinical outcomes involved assessments at both preoperation and final follow-up. These evaluations utilized the Japanese Orthopaedic Association (JOA) score, which ranges up to a maximum of 17 points. In addition, the severity of neck pain was quantified using the visual analogue scale (VAS), with scores ranging from 0 to 100. Lower VAS scores show a more comfortable condition, indicative of freedom from pain. The JOA score recovery rate (%) was computed as follows: (final follow-up JOA score − preoperative JOA score) / (17 − preoperative JOA score) × 100. This calculation elucidates the percentage improvement in JOA scores from the preoperative baseline.
Statistical Analysis
Comparative analyses of baseline demographics, surgical characteristics, radiographic findings, and clinical outcomes were conducted between the gROM <0° and >0° groups utilizing the Wilcoxon signed-rank test or Mann-Whitney test for continuous variables and the chi-square test for categorical variables. Statistical significance was considered for P-values less than 0.05. All statistical analyses were carried out using SPSS version 29.0 (IBM Corp., Armonk, NY, USA). No statistical sample size calculations were performed in advance of the present study. However, post hoc power analysis was conducted to indicate their reliability in terms of attained power (0.0 < 1−β < 1.0) using G*Power software (version 3.1.9.2, Heinrich-Heine-Universität Düsseldorf).
Results
Patient Demographics and Clinical Characteristics in This Study
Demographics of 156 Patients With Cervical OPLL Who Underwent Posterior Decompression.
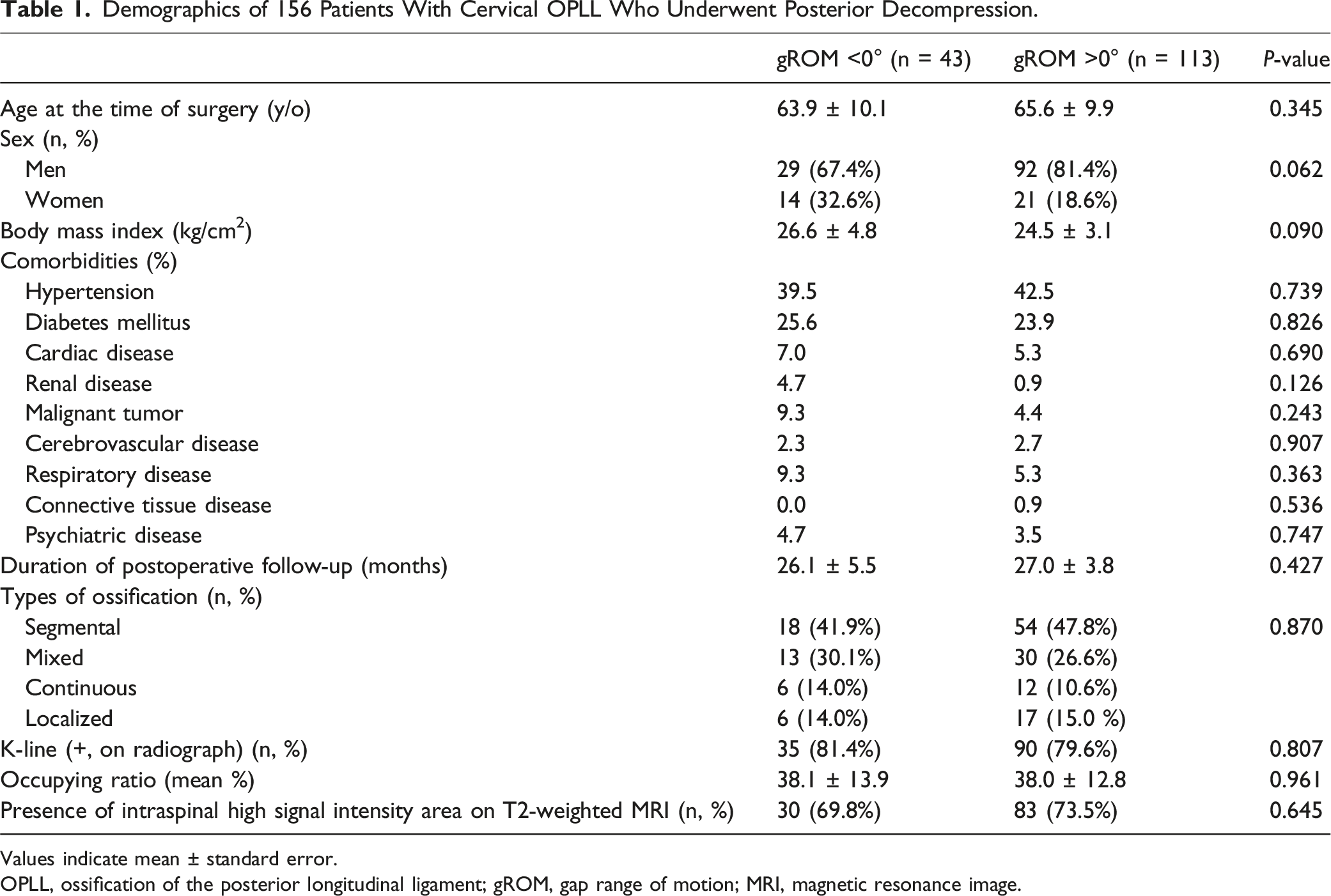
Values indicate mean ± standard error.
OPLL, ossification of the posterior longitudinal ligament; gROM, gap range of motion; MRI, magnetic resonance image.
Surgical Details and Perioperative Complications
Comparison of Surgical Information and Perioperative Complications Between gROM <0° and >0° Group.
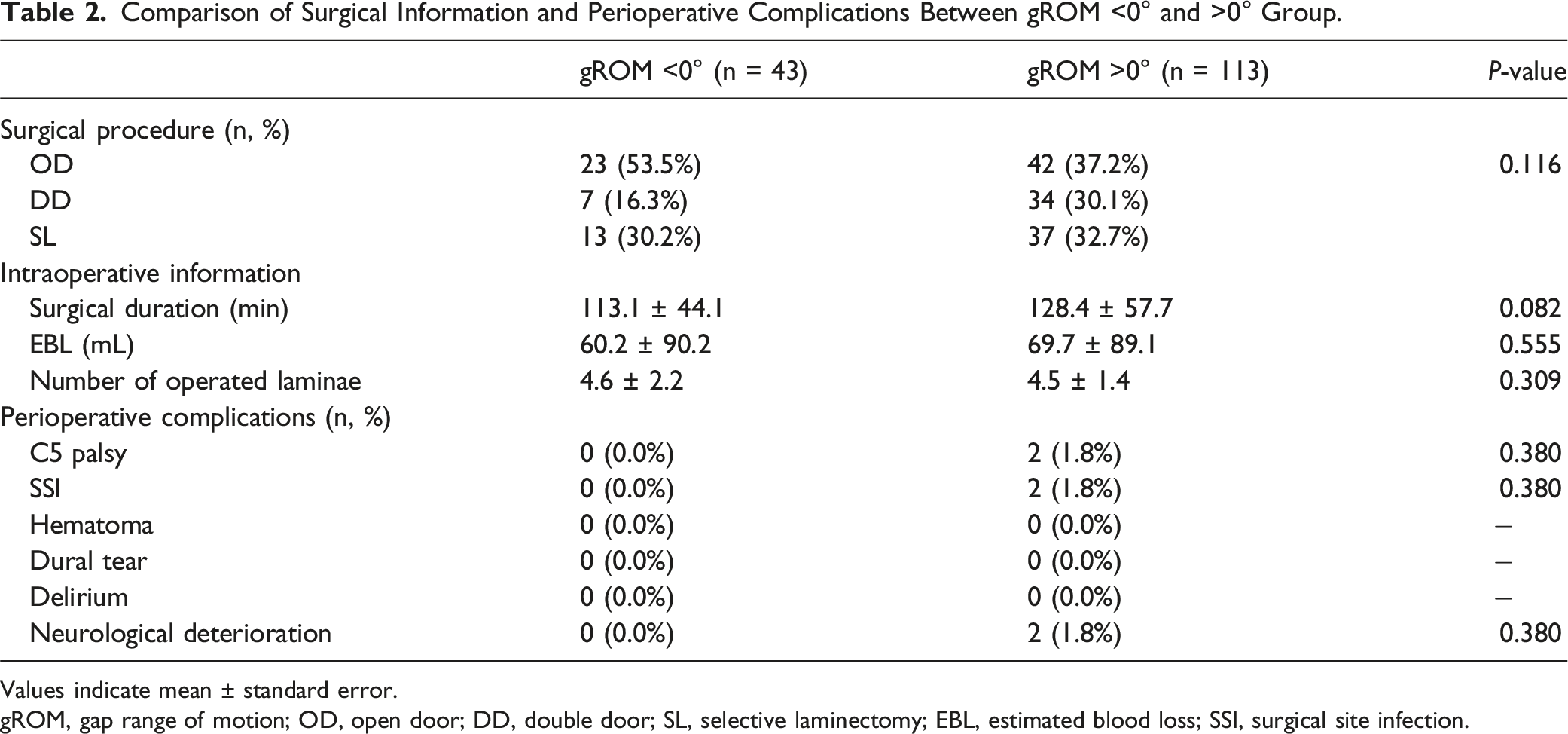
Values indicate mean ± standard error.
gROM, gap range of motion; OD, open door; DD, double door; SL, selective laminectomy; EBL, estimated blood loss; SSI, surgical site infection.
Postoperative Changes in Cervical Sagittal Alignments and ROM
In the gROM <0° group, no statistically significant differences were observed between preoperative and final follow-up assessments in the neutral position (5.0 ± 10.4° vs 5.8 ± 12.0°, P = .591) and flexion position (−6.5 ± 10.5° vs −8.0 ± 11.0°, P = .350) of the C2-7 angle, and fROM (11.5 ± 7.3° vs 13.8 ± 9.6°, P = .098). However, significant reductions were found in the extension position of the C2-7 angle (23.0 ± 12.9° vs 17.4 ± 14.4°, P = .002), total ROM (29.5 ± 14.0° vs 25.4 ± 15.1°, P = .032), and eROM (18.0 ± 8.4° vs 11.6 ± 8.8°, P < .001), with increases observed in gROM (−6.5 ± 7.2° vs 2.2 ± 10.4°, P < .001) and C2-7 SVA (27.0 ± 14.0 mm vs 30.3 ± 13.5 mm, P = .024) after surgery.
Conversely, in the gROM >0° group, comparing preoperative and final follow-up assessments revealed no statistically significant differences in the neutral position (14.5 ± 10.7° vs 13.5 ± 12.5°, P = .209) and extension position (23.5 ± 12.0° vs 19.5 ± 12.5°, P = .067) of the C2-7 angle, and eROM (8.9 ± 5.7° vs 8.1 ± 5.8°, P = .243). Meanwhile, total ROM (33.2 ± 11.9° vs 26.7 ± 10.9°, P < .001), fROM (24.2 ± 9.3° vs 18.5 ± 9.5°, P < .001), and gROM were significantly reduced (15.3 ± 9.8° vs 9.4 ± 11.3°, P < .001), and flexion position of the C2-7 angle (−9.7 ± 10.9° vs −5.0 ± 11.7°, P < .001) and C2-7 SVA were increased after surgery (26.0 ± 11.6 mm vs 27.9 ± 13.0 mm, P = .022).
Comparison of Preoperative and Final Follow-Up Cervical Sagittal Parameters Between gROM <0° and >0° Group.
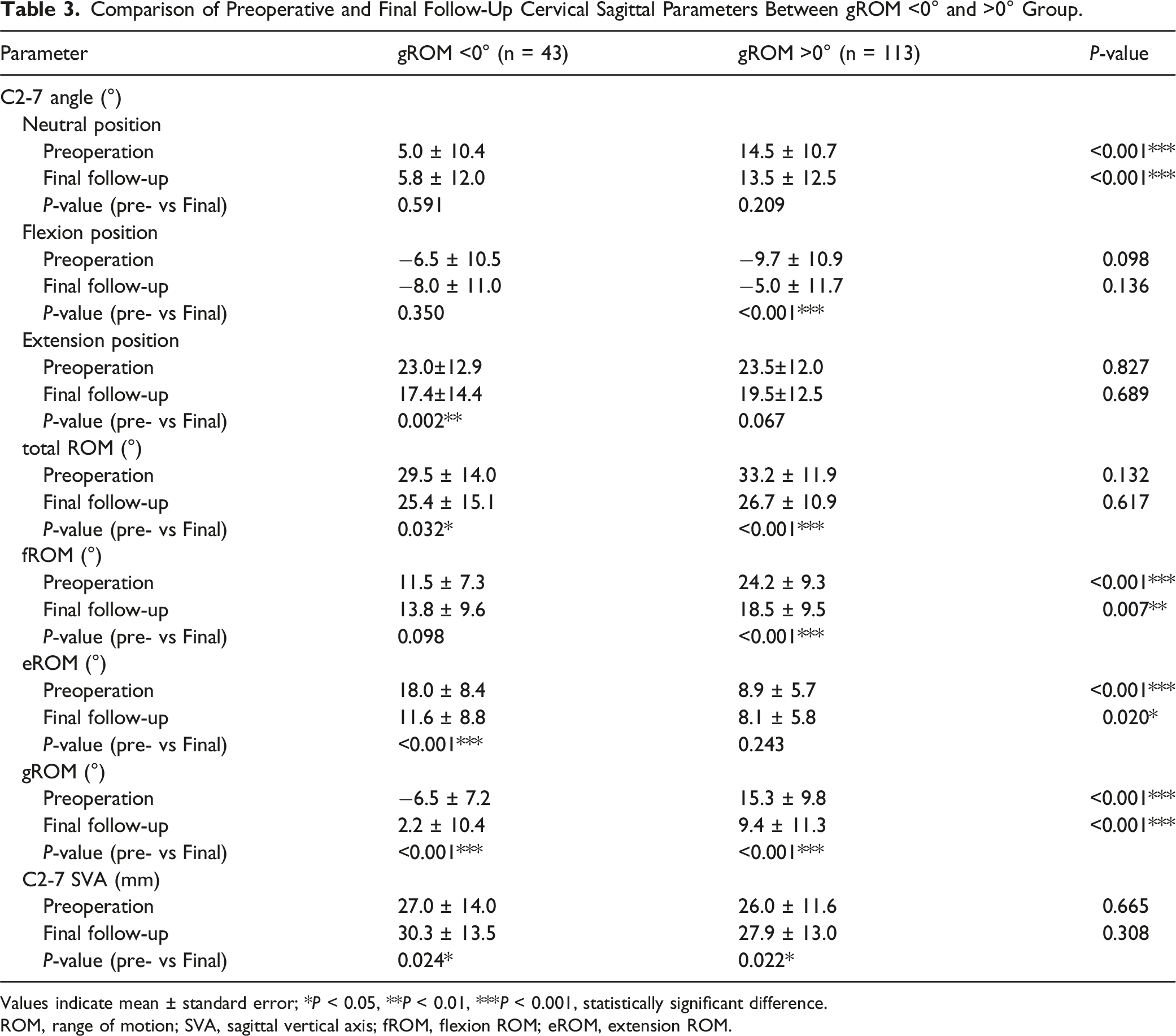
Values indicate mean ± standard error; *P < 0.05, **P < 0.01, ***P < 0.001, statistically significant difference.
ROM, range of motion; SVA, sagittal vertical axis; fROM, flexion ROM; eROM, extension ROM.
At the postoperative assessment, no evidence of new spondylolisthesis, development of scoliosis, or progression of OPLL at the site of posterior cervical decompression was observed.
Clinical Outcomes after Posterior Decompression
JOA score exhibited a significant improvement after posterior decompression in both the gROM <0° (11.4 ± 2.7 vs 13.9 ± 2.1, P < .001) and gROM >0° (11.2 ± 2.6 vs 14.1 ± 2.3, P < .001) groups. On the other hand, no significant group differences were found in preoperative and final follow-up JOA scores (preoperation, P = .743; final follow-up, P = .683), nor in the changes in JOA scores (2.5 ± 1.9 vs 2.8 ± 2.4, P = .399) between the two groups. Furthermore, JOA score recovery rates were comparable (45.4 ± 26.9% vs 48.3 ± 34.5%, P = .583).
Comparison of Clinical Outcomes Between gROM <0° and >0° Group.
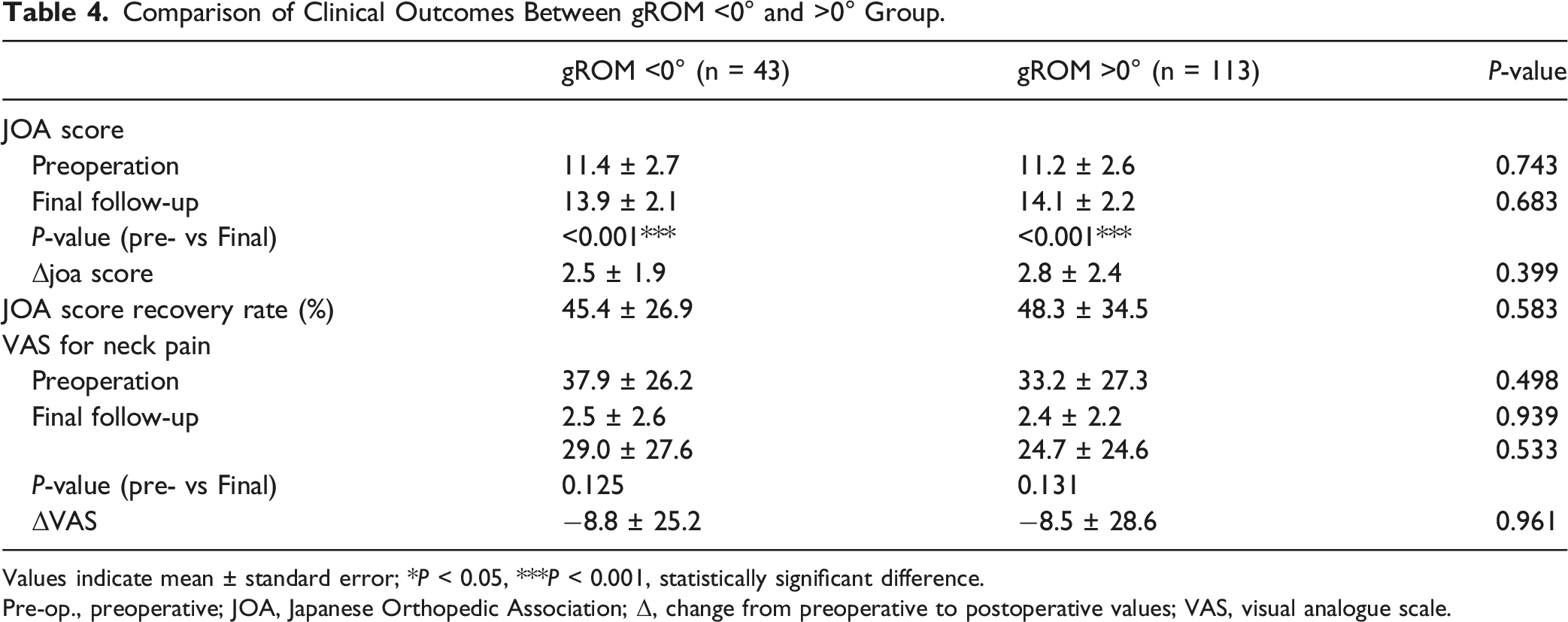
Values indicate mean ± standard error; *P < 0.05, ***P < 0.001, statistically significant difference.
Pre-op., preoperative; JOA, Japanese Orthopedic Association; Δ, change from preoperative to postoperative values; VAS, visual analogue scale.
Discussion
This retrospective multicenter study is the first to evaluate the influence of preoperative cervical ROM, including a novel indicator of gROM, on postoperative radiographic and clinical outcomes among patients with cervical OPLL who underwent posterior decompression. Patients with preoperative gROM <0° had less lordosis in cervical sagittal alignment by C2-7 angle both before and after surgery compared to patients with preoperative gROM >0°. Although no significant difference was found the incidence of perioperative complications, total ROM significantly decreased following surgery regardless of whether preoperative gROM was <0° or >0°. Additionally, within the gROM <0° group, eROM experienced a significant reduction postoperatively, while in the gROM >0° group, fROM demonstrated a decrease postoperatively. Both groups exhibited significant improvement in JOA scores postoperatively. These findings strongly advocate for the efficacy of posterior decompression in yielding favorable outcomes for cervical OPLL, irrespective of the magnitude of preoperative gROM. Importantly, they bear significant implications for further research endeavors aimed at exploring the feasibility and efficacy of posterior decompression in patient with cervical OPLL.
To date, many studies have investigated the impact of surgery on cervical ROM in patients with cervical OPLL.3,6,12,21,22 Kimura et al 21 reported a marked 65.8% decrease in cervical ROM following DD laminoplasty. Additionally, Nagoshi et al 12 observed reductions in cervical ROM postoperatively following OD and DD procedures. Maruo et al 22 emphasized the importance of preoperative cervical ROM, revealing that it was significantly higher in patients with poor surgical outcomes. They further indicated that patients with a preoperative cervical ROM exceeding 20° faced a 4.6-fold higher risk of poor clinical outcomes, suggesting dynamic factors may influence the success of DD laminoplasty. In our present study, we observed a significant reduction in total ROM after posterior decompression for cervical OPLL in both the g ROM <0° and >0° groups. Specifically, the gROM <0° group experienced a significant decrease in eROM postoperatively. Conversely, the gROM >0° group demonstrated a significant decrease in fROM postoperatively. Therefore, it was suggested that depending on whether cervical ROM was greater in the flexion or extension position preoperatively, ROM in the corresponding position decreased after surgery, resulting in an overall reduction in cervical ROM.
In fact, the fROM and eROM do not always exhibit a complementary relationship, as the total cervical ROM varies individually.16-18 An indicator that can effectively represent fROM and eROM independently would be even more useful in predicting loss of cervical lordosis after surgery than considering fROM or eROM alone. Building upon this issue, Fujishiro et al 18 devised a novel metric, the gap between fROM and eROM known as gROM. They hypothesized that gROM could serve as a highly effective indicator for predicting loss of cervical lordosis after laminoplasty. Previously, Nakashima et al examined the occurrence of loss of cervical lordosis following laminoplasty in 165 cases of cervical OPLL, incorporating gROM as one of their assessment indicators. They found that while gROM was significantly greater in cases with postoperative loss of cervical lordosis >10°, it showed comparable in cases with postoperative loss exceeding 20°. 23 In this study, we focused on the magnitude of preoperative gROM and evaluated its impact on postoperative outcomes and cervical alignment. In comparison between preoperative and postoperative, the mean C2-7 angles did not show significant changes in either of the preoperative gROM <0° or >0° groups. This difference of results could be attributed to the incidence of cases experiencing postoperative loss of cervical lordosis. In the study by Nakashima et al, 32 out of 165 cases (19.4%) showed postoperative loss of cervical lordosis >10°. On the other hand, postoperative loss of cervical lordosis >20° occurred in only five cases (4.2%), and no significant difference was found regarding the magnitude of gROM. In the current study, no cases in the gROM <0° group and only 6 out of 113 cases (5.3%) in the gROM >0° group exhibited postoperative loss of cervical lordosis >10°. Therefore, we believe that further study is needed to increase the number of cases in the future. Interestingly, another new finding, preoperative gROM <0° group showed a rather significantly smaller of the mean C2-7 angle in neutral position both before and after surgery compared to gROM >0° group. These findings suggest that patients with cervical OPLL who have a gROM <0° originally have smaller lordosis in cervical sagittal alignment, and this difference is likely to be maintained after posterior decompression.
With regard to CSM, cervical ROM has also been reported to decrease after posterior decompression.18,24-26 Fujishiro et al 18 found that a higher gROM value suggest reduced structural stability in preventing the cervical spine from transitioning into a kyphotic alignment. It could signify diminished efficacy of the posterior neck muscular-ligament complex in maintaining lordotic alignment, thereby indicating a heightened risk of loss of cervical lordosis after laminoplasty. However, the aforementioned studies primarily focused on patients with CSM and excluded those with cervical OPLL. Unfortunately, the present study did not compare between patients with OPLL and those with CSM. In the past, Fujimori et al 24 compared the clinical outcomes of patients with CSM and OPLL to investigate whether there were differences in cervical ROM changes before and after posterior decompression. They showed that plated laminoplasty in patients with either OPLL or CSM decreases cervical ROM, especially in the extension angle. Among patients who have undergone laminoplasty, those with OPLL lost more ROM than do those with CSM. From these results, the cervical OPLL was likely to fuse after laminoplasty due partially spontaneously to OPLL progression, which would affect postoperative cervical ROM reduction. Although CSM and OPLL differ in pathogenesis and etiology,4,5,19,20 and it is likely not simply compare the two, future comparative studies of CSM and OPLL are needed in terms of gROM.
Spinal fusion is often combined with posterior decompression to prevent loss of cervical lordosis, postoperatively.27-29 Yuan et al 27 showed an obvious reduction in cervical ROM following laminoplasty and laminectomy with fusion in patients with cervical OPLL. Major reduction was observed in extension, and less impact was detected on rotation. Laminoplasty was found to better preserve ROM compared to laminectomy with fusion. Nakashima et al 28 reported significantly smaller cervical ROM in patients undergoing posterior fixation compared to those undergoing laminectomy alone. Ha et al demonstrated laminoplasty was superior to laminectomy with fusion in preserving cervical ROM, preoperative cervical lordosis, and minimizing neck disability. Especially, loss of cervical lordosis and cervical ROM were significantly larger in the cervical laminectomy with fusion group. The stabilization obtained by adding instrumented fusion could suppress the progression of OPLL thickness. 29 In contrast, Ma et al 30 indicated that no significant differences between laminoplasty and laminectomy with fusion in terms of pre-, postoperative cervical ROM, and preoperative cervical lordosis. Although our study did not include cases of cervical OPLL with spinal fusion, even if postoperative loss of cervical lordosis appeared and progressed, it eventually reached a plateau, and satisfactory postoperative outcomes were obtained. Especially, Hyun et al documented a time-dependent decline in cervical ROM after laminoplasty, stabilizing by 18 months post-surgery, without further reduction. They also noted the potential for recovery in post-laminoplasty ROM reduction over several years, unless laminar autofusion occurred. 31 Furthermore, Lee et al 32 reported favorable long-term outcomes of laminectomy for cervical OPLL, with minimal risk of post-laminectomy kyphosis. This suggests the possibility that OPLL itself would provide support for the spinal column. Therefore, since the observation period of the results of this study was short, further evaluation during long-term follow-up is desirable.
Our study is subject to several notable limitations. First, it utilized a retrospective methodology, inherently reducing the level of evidential support. Second, the postoperative follow-up period was relatively short, limiting a comprehensive investigation into the development of postoperative radiographic complications and long-term clinical outcomes. Hence, future assessments with extended observation periods are essential to validate the efficacy of posterior decompression for cervical OPLL. Third, the sample size was relatively small, and the statistical power was insufficient to draw precise conclusions regarding the clinical outcomes of patients with cervical OPLL. Finally, cervical sagittal alignment is influenced by global spine alignment, and adequate thoracic spine mobility is crucial for achieving full cervical ROM. Reduced thoracic spine mobility has been associated with neck pain and dysfunction. Therefore, when evaluating the impact of OPLL on cervical spine function, it is vital to consider the presence of OPLL throughout the entire spine, not just in the cervical region. Recognizing these limitations is clinically significant when assessing cervical spine function in patients with OPLL. The significance of our study lies in its unprecedented focus on analyzing the magnitude of preoperative gROM in patients with cervical OPLL who underwent posterior decompression.
Conclusion
The present study investigated how the preoperative cervical ROM impacts on surgical and clinical outcomes in patients with cervical OPLL who underwent posterior decompression. Our findings indicate that the patients with preoperative gROM <0° exhibited less lordosis in cervical sagittal alignment before and after surgery compared to those with preoperative gROM >0°. Additionally, cervical ROM significantly decreased following surgery regardless of whether preoperative gROM was <0° or >0°. Meanwhile, the incidence of perioperative complications and postoperative clinical outcomes were comparable between the two groups. These results suggest that posterior decompression for cervical OPLL offers favorable clinical outcomes irrespective of the magnitude of preoperative gROM. However, due to the relatively small sample size in this study, larger-scale investigations are needed to draw more precise conclusions in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.