
Abstract
Study Design
Retrospective multicenter study.
Objectives
To investigate surgical outcomes following posterior decompression for cervical ossification of the posterior longitudinal ligament (OPLL) when performed by board-certified spine (BCS) or non-BCS (NBCS) surgeons.
Methods
We included 203 patients with cervical OPLL who were followed for a minimum of 1 year after surgery. Demographic information, medical history, and imaging findings were collected. Clinical outcomes were assessed preoperatively and at the final follow-up using the Japanese Orthopedic Association (JOA) score and the visual analog scale (VAS) for the neck. We compared outcomes between BCS surgeons, who must meet several requirements, including experience in more than 300 spinal surgeries, and NBCS surgeons.
Results
BCS surgeons performed 124 out of 203 cases, while NBCS surgeons were primary in 79 cases, with 73.4% were directly supervised by a BCS surgeon. There was no statistically significant difference in surgical duration, estimated blood loss, and perioperative complication rates between the BCS and NBCS groups. Moreover, no statistically significant group differences were observed in each position of the C2-7 angle and cervical range of motion at preoperation and the final follow-up. Preoperative and final follow-up JOA scores, VAS for the neck, and JOA score recovery rate were comparable between the two groups.
Conclusions
Surgical outcomes, including functional recovery, complication rates, and cervical dynamics, were comparable between the BCS and NBCS groups. Consequently, posterior decompression for cervical OPLL is considered safe and effective when conducted by junior surgeons who have undergone training and supervision by experienced spine surgeons.
Keywords
Introduction
Cervical ossification of the posterior longitudinal ligament (OPLL) is a significant condition characterized by the ossification of spinal ligaments, predominantly observed in Asian countries.1,2 Approximately half of individuals with cervical OPLL undergo ossification progression, leading to symptomatic myelopathy.1,2 Surgical decompression is commonly applied to halt neurological deterioration, and the clinical outcomes following these procedures are generally favorable and stable. There are two main methods of decompression in cervical OPLL: direct decompression through anterior approach and indirect decompression through posterior approach. 3 In particular, laminoplasty and muscle preserving selective laminectomy serve as safe and effective posterior procedures, offering the advantages of preserving cervical motion and reducing cervical instability and kyphosis.4-7
Residency programs in orthopedic surgery and spine fellowship training have traditionally taken place at academic medical centers, where surgical skills are developed through a structured approach that includes graduated responsibility and autonomy within the operating room. Fellows and residents begin their careers assisted by the primary attending in various spine surgeries, and after much experience, they have the opportunity to operate as primary surgeons.8,9 Several previous reports have suggested that when junior surgeons perform or assist in spine surgery, there is a potential increase in the risk of surgical site infections, displaced pedicle screws, and insufficient correction of scoliosis.10-15 On the other hand, comparable results were found in other studies comparing other outcomes, including postoperative results and perioperative complications, between cases led by junior and senior surgeons.16-24 Especially in the context of the cervical spine, there is limited evidence regarding how the involvement of inexperienced surgeons influences on outcomes following surgery.25,26 Recently, we investigated the outcomes of posterior decompression for cervical spondylotic myelopathy (CSM) when conducted by board-certified spine (BCS) or non-BCS (NBCS) surgeons. 27 Despite the longer surgical duration in the NBCS group, postoperative functional recovery, the rate of perioperative complications, and changes in cervical dynamics on radiographs were comparable between the groups. However, given that the primary lesion in CSM stems from age-related degeneration, its pathological condition is fundamentally distinct from cervical OPLL. This variance in pathology can impact postoperative functional recovery, spinal alignment, and the frequency of complications.28,29 Therefore, investigating the impact of surgeon experience on clinical outcomes and perioperative complications in cervical OPLL is crucial to determine the benefits of posterior decompression surgery for patients with this condition.
This study aimed to compare and evaluate radiographic changes in the cervical spine, as well as the associated clinical outcomes, between BCS and NBCS surgeons following posterior decompression surgery in patients with cervical OPLL.
Materials and Methods
Study Design, Patient Demographics, and Characteristics
This retrospective study involved 203 patients with cervical OPLL, who underwent posterior decompression surgery at 16 Japanese institutions between January 2012 and December 2014. All investigators were seasoned orthopaedics spine surgeons. To be eligible for inclusion, subjects had to meet the following criteria: (1) Presentation of at least one clinical sign of myelopathy, (2) Evidence of cervical spinal cord compression on magnetic resonance (MR) imaging and OPLL on X-ray or computed tomography (CT), (3) No history of previous cervical spine surgery, and (4) A minimum follow-up period of 1 year following the surgery. Meanwhile, patients were excluded if they were asymptomatic or diagnosed with CSM, cervical kyphosis, active infection, rheumatoid arthritis, ankylosing spondylitis, neoplastic spinal disease, or concomitant lumbar stenosis.
Patients participating in this study were evaluated at an outpatient clinic prior to surgery by the doctor designated as the primary surgeon, irrespective of whether the surgery was ultimately performed by a BCS or NBCS surgeon. The decision regarding the indication for surgery, technique employed, and the range of decompression levels was made collaboratively by a spine team at each institute. Three distinct surgical techniques were performed in the present study: expansive open-door laminoplasty (OD), double-door laminoplasty (DD), or selective laminectomy with muscle preservation (SL). OD, DD, and SL were performed at 10, 4, and 7 institutions, respectively.4-7 Generally, these techniques were recommended in cases of multi segmental stenosis with a narrow spinal canal and without kyphotic cervical alignment.
We examined a retrospective collection of demographic information, medical history, symptomatology, imaging, surgical summaries, and other data for all subjects in this study. The current study received approval from the Ethics and Institutional Review Board (Keio university school of medicine, approval number: #20110142), and all participants provided informed consent to be included in the study before undergoing surgery.
BCS and Non-BCS Surgeons
In Japan, the designation of a BCS surgeon requires meeting several criteria: (1) authorization as a Spine Specialist Approved by the JOA, (2) membership in the Japanese Society for Spine Surgery and Related Research (JSSR), (3) a surgical track record of over 300 spine and spinal cord operations, including at least 200 as the primary surgeon, with a minimum of 20 involving the cervical spine and 60 involving the lumbar spine, (4) participation in at least 2 annual meetings of the JSSR within the past 5 years, and (5) publication of at least 5 clinical papers related to spine and spinal cord disorders. In our study, 21 BCS and 18 NBCS surgeons were included. At the study’s outset (the first patient registration), the mean age and practice time as an orthopedic surgeon for NBCS surgeons were 32.1 ± 3.5 and 6.8 ± 3.4 years, respectively. Their average duration of practicing surgery at a spine training center was 1.3 ± 1.7 years. Throughout the NBCS surgeons’ careers, they had performed an average of 393.7 ± 179.8 orthopedic-related surgeries and 77.3 ± 100.0 spine surgeries. Additionally, those in this group who performed surgery without direct BCS supervision had carried out an average of 162.8 ± 172.6 spinal surgeries up to that point. Unlike the North American medical educational system, the Japanese training period for physicians lacks resident or fellow grades, categorizing spine surgeons into BCS or NBCS.
Radiographical Images and MRI Findings
In this study, we examined radiological evaluations of the cervical spine by measuring intermittent C2-7 angles from plain radiographs in the neutral, flexion, and extension position at two distinct time points: “preoperation” and “final follow-up.” The assessment of C2-7 angles involved measuring the Cobb angle, which quantified the angle between the lower endplate of the C2 vertebra and the lower endplate of the C7 vertebra. Additionally, the cervical range of motion (ROM) was calculated by subtracting the flexion C2-7 angle from the extension angle. The types of OPLL were categorized as localized, segmental, continuous, and mixed. The occupying ratio of OPLL, and the K-line were assessed through preoperative plain X-ray or CT. Preoperative MRI was utilized to evaluate the stenotic levels in OPLL and the presence of intraspinal high signal intensity area on the T2-weighted images.
Clinical Outcomes
The assessment of clinical outcomes involved evaluations at both the preoperation and final follow-up. These assessments utilized the JOA score, which can reach a maximum of 17 points. Additionally, the extent of neck pain was measured using the Visual Analog Scale (VAS), with scores ranging from 0 to 10. Lower VAS scores indicate a more comfortable condition, free from pain. The JOA score recovery rate (%) was calculated as follows: (final follow-up JOA score - preoperative JOA score)/(17 - preoperative JOA score) × 100. This calculation reveals the percentage improvement in JOA scores from the preoperative baseline.
Statistical Analysis
Comparative analyses of baseline demographics, surgical characteristics, radiographical findings and clinical outcomes were performed between the BCS and NBCS group using the Wilcoxon signed-rank test or Mann-Whitney test for continuous variables and the chi-square test for categorical variables. Statistical significance was considered for P-values less than .05, .01, and .001. All statistical analyses were performed using SPSS version 29.0 (IBM Corp., Armonk, NY, USA).
Results
Patient Demographics and Clinical Characteristics
Demographics of 203 Patients With OPLL Who Underwent Posterior Cervical Decompression by BCS and NBCS Surgeons.
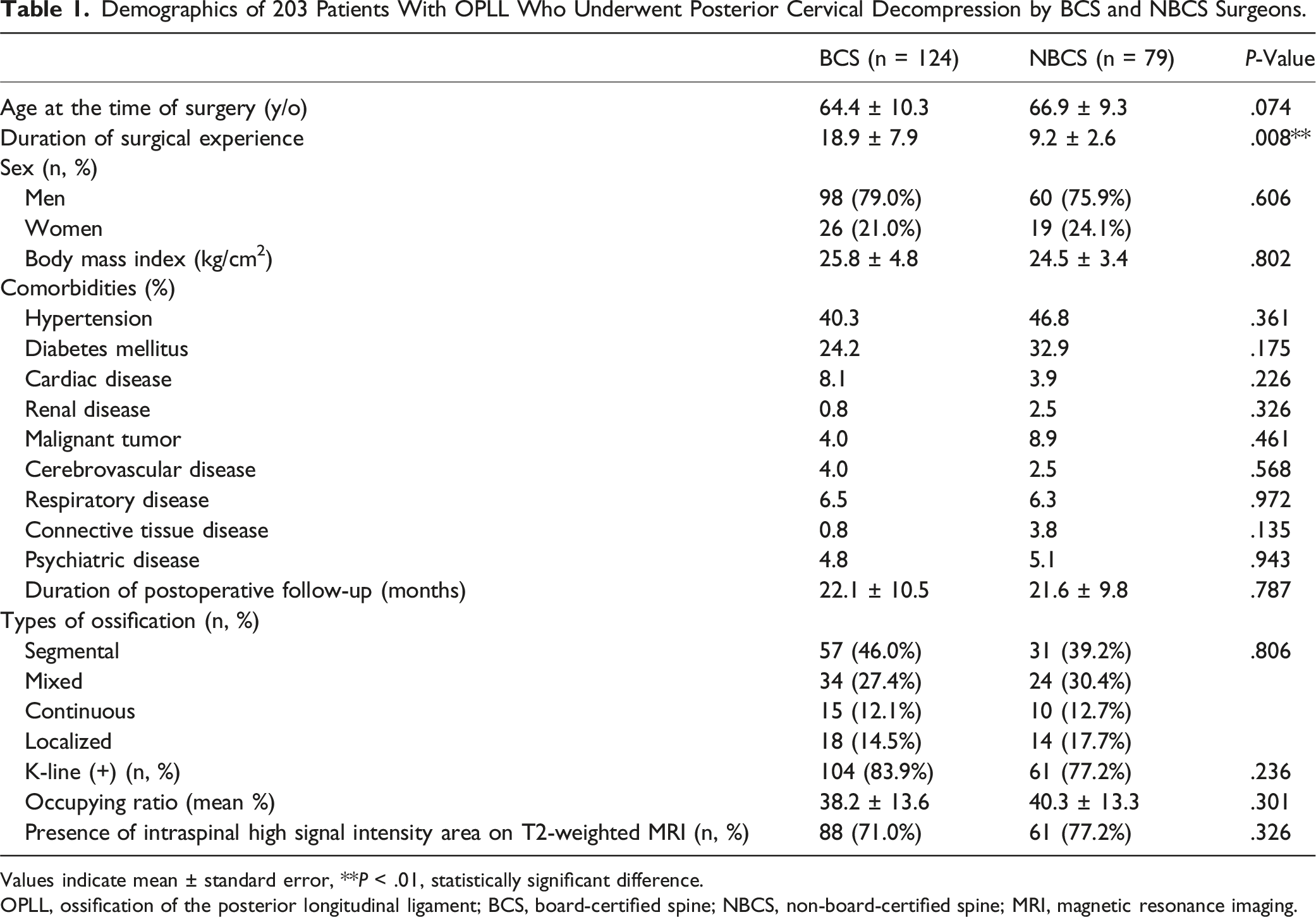
Values indicate mean ± standard error, **P < .01, statistically significant difference.
OPLL, ossification of the posterior longitudinal ligament; BCS, board-certified spine; NBCS, non-board-certified spine; MRI, magnetic resonance imaging.
Surgical Information and Perioperative Complications
Comparison of Surgical Information and Perioperative Complications Between BCS and NBCS Group.
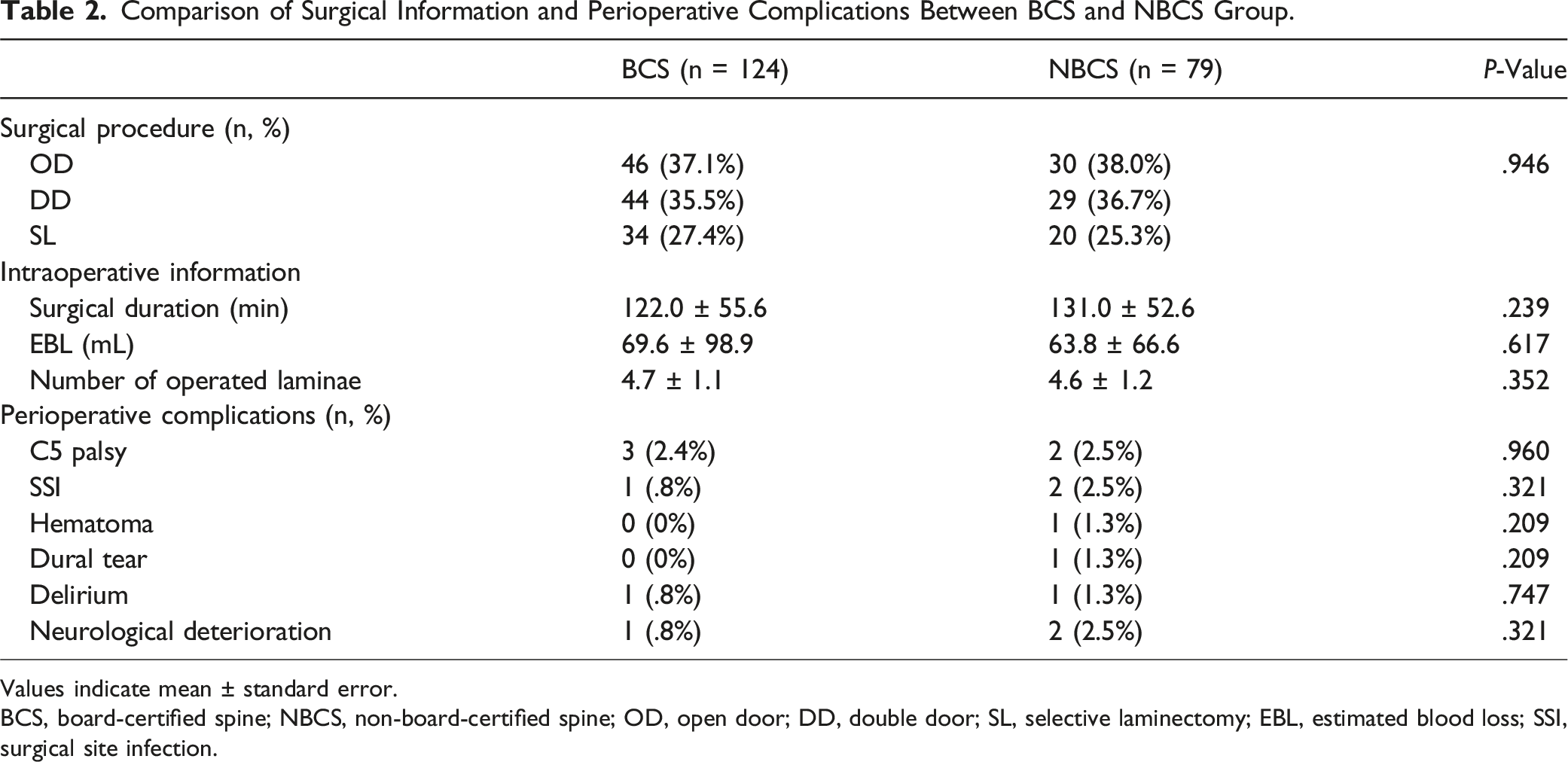
Values indicate mean ± standard error.
BCS, board-certified spine; NBCS, non-board-certified spine; OD, open door; DD, double door; SL, selective laminectomy; EBL, estimated blood loss; SSI, surgical site infection.
Comparison of the Intraoperative Information Between the BCS and NBCS Groups for Each Surgical Technique.
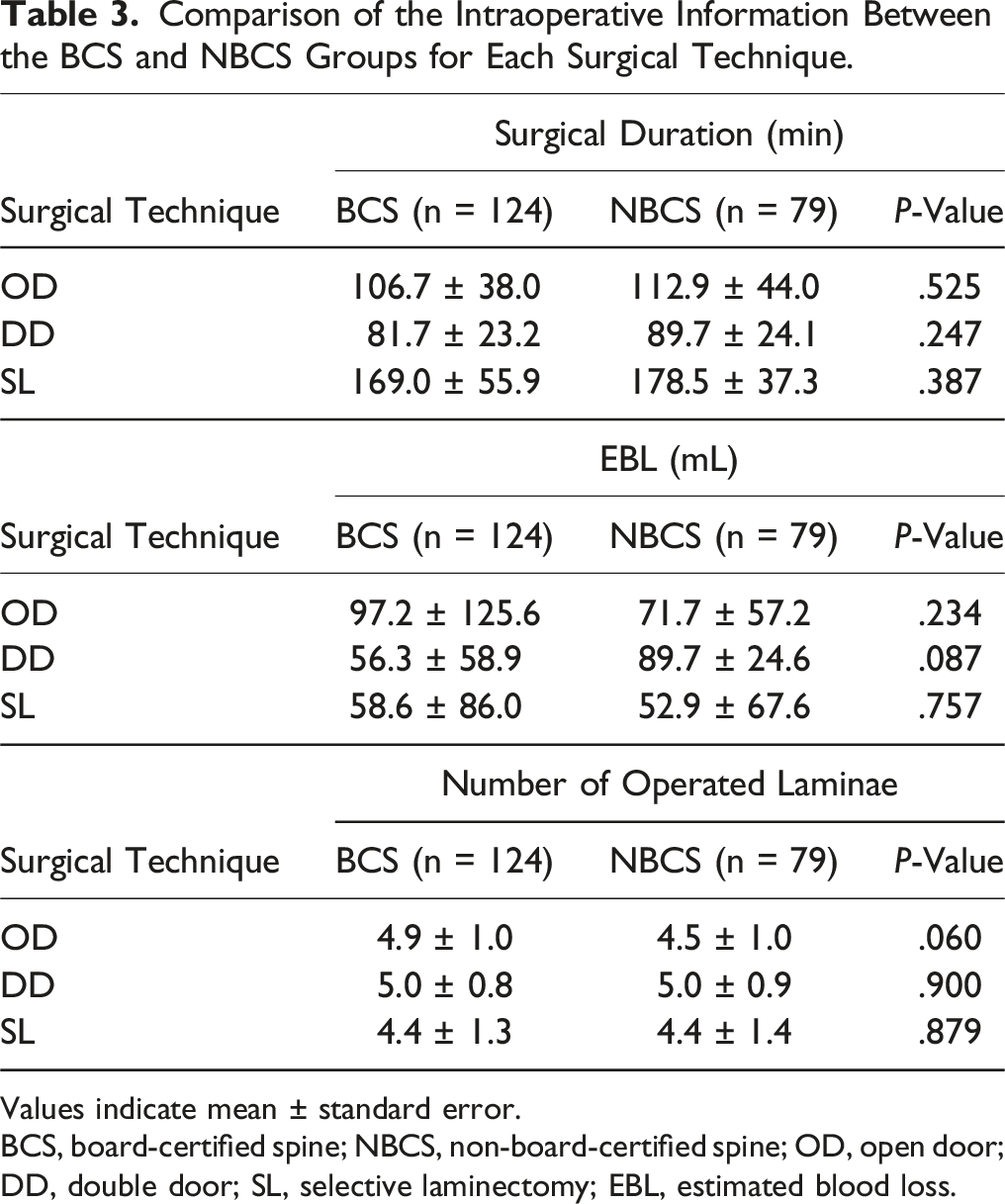
Values indicate mean ± standard error.
BCS, board-certified spine; NBCS, non-board-certified spine; OD, open door; DD, double door; SL, selective laminectomy; EBL, estimated blood loss.
Postoperative Alterations in Cervical Alignments
Comparison of Preoperative and Final Follow-Up Each Cervical Sagittal Parameter Between BCS and NBCS Group.
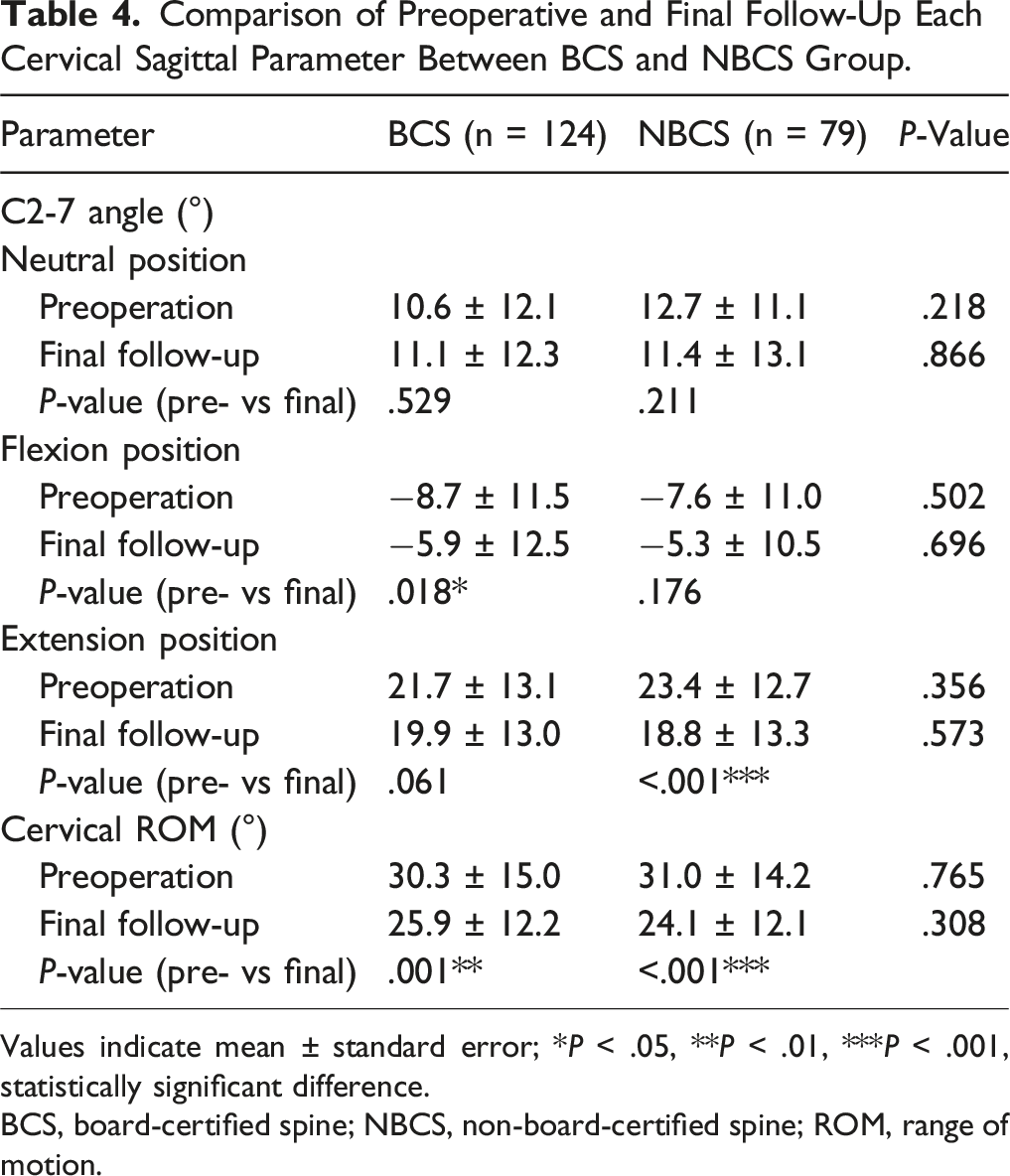
Values indicate mean ± standard error; *P < .05, **P < .01, ***P < .001, statistically significant difference.
BCS, board-certified spine; NBCS, non-board-certified spine; ROM, range of motion.
Furthermore, at the postoperative assessment, there was no evidence of new spondylolisthesis, the development of scoliosis, or progress of OPLL at the site of posterior cervical decompression.
Clinical Outcomes After Posterior Decompression
Comparison of Surgical and Clinical Outcomes Between BCS and NBCS Group.
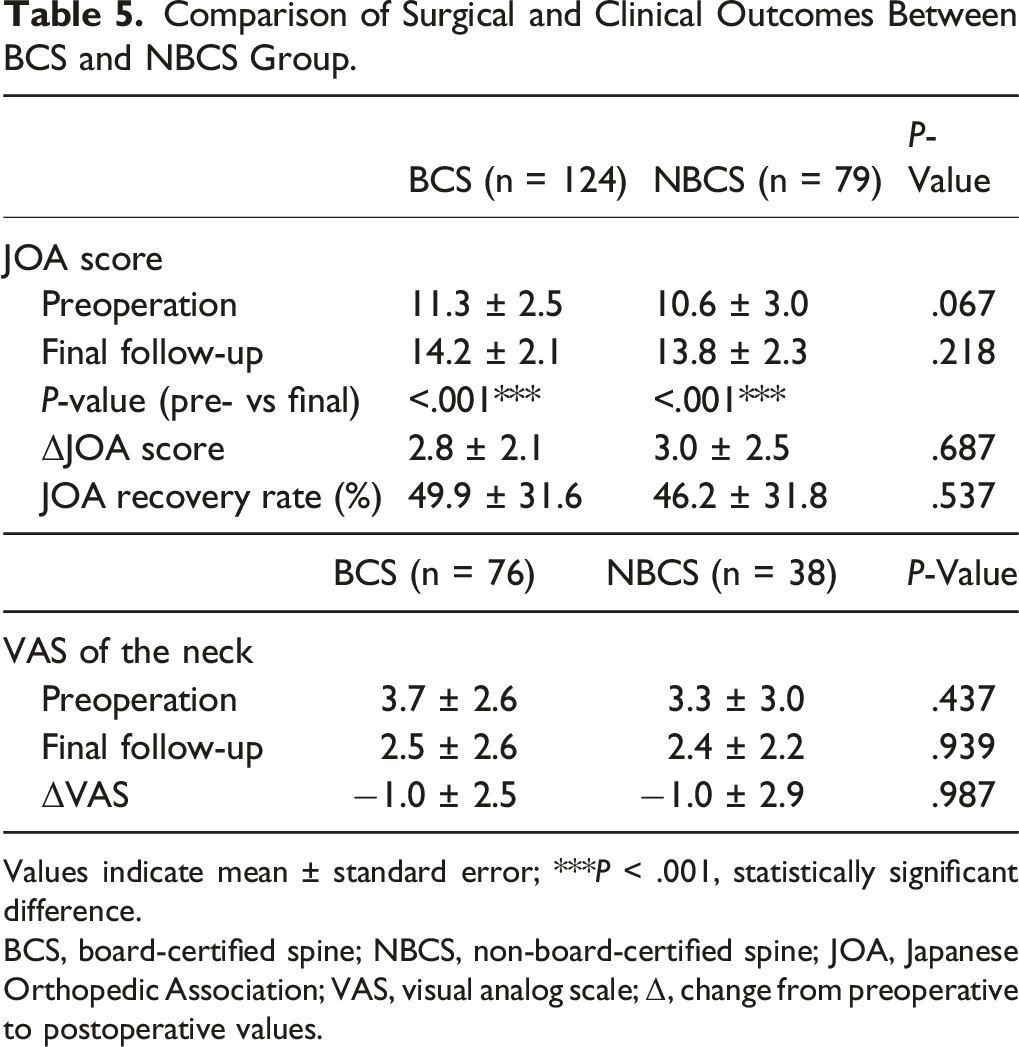
Values indicate mean ± standard error; ***P < .001, statistically significant difference.
BCS, board-certified spine; NBCS, non-board-certified spine; JOA, Japanese Orthopedic Association; VAS, visual analog scale; Δ, change from preoperative to postoperative values.
Comparison of the Alterations in JOA Scores Between the BCS and NBCS Groups for Each Surgical Technique.
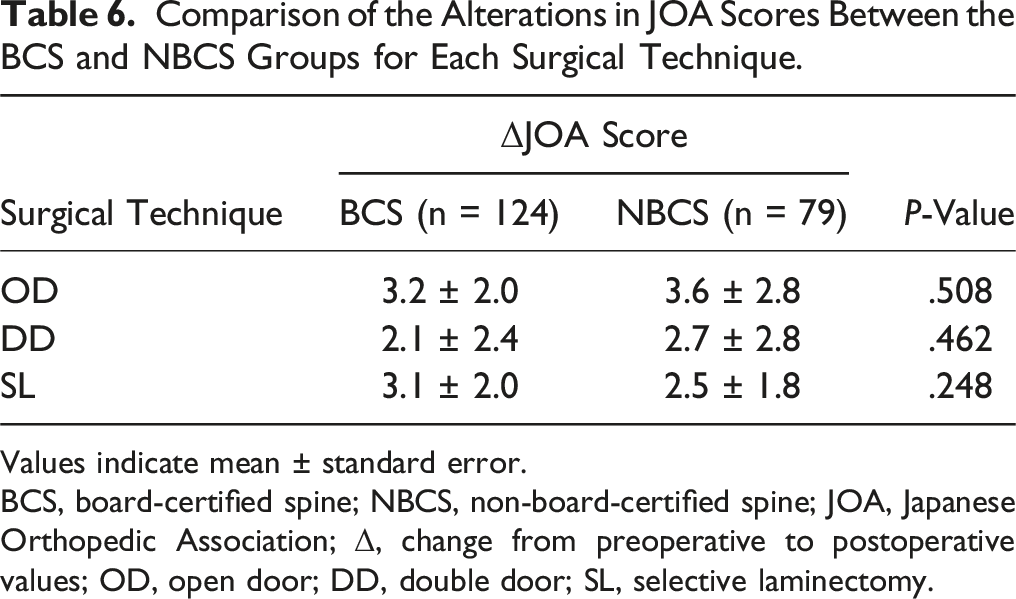
Values indicate mean ± standard error.
BCS, board-certified spine; NBCS, non-board-certified spine; JOA, Japanese Orthopedic Association; Δ, change from preoperative to postoperative values; OD, open door; DD, double door; SL, selective laminectomy.
Discussion
This retrospective multicenter study is the first to assess the impact of posterior decompression performed by inexperienced spine surgeons on surgical outcomes in patients with cervical OPLL, and our study has the largest sample size to date. There was no discernible influence on surgical outcomes, as evaluated by changes in the rate of perioperative complications, postoperative C2-7 angle, cervical ROM, JOA scores, and VAS for the neck. Additionally, under predominant supervision by experienced surgeons, NBCS surgeons can achieve results comparable to those of BCS surgeons. These findings strongly indicate that posterior decompression surgery for cervical OPLL is equally safe and effective, whether conducted by a BCS or NBCS surgeon, and have significant implications for research aiming to examine the viability of posterior decompression for patients with cervical OPLL.
Typically, the selection of surgical procedure for cervical spine is left to the discretion of institutions, and each institution is unlikely to use the several techniques based on pathophysiology. The current ratio of OD, DD, or SL is considered to reflect the actual prevalence of laminoplasty techniques in Japan.4-7 However, to date, there are no reports that have clarified the prevalence rate of each technique. For cervical OPLL, past comparisons of clinical outcomes between OD and DD have consistently shown similar postoperative JOA scores and recovery rates.30,32 In addition to evaluating neurological function, a recent meta-analysis of postoperative complications and radiographic parameters found no advantage of one technique over the other. 1 In the present study, OD was the most frequent procedure of surgical decompression for cervical OPLL, followed by DD and SL, which did not vary significantly between the BCS and NBCS groups. Therefore, our study demonstrates that neurological recovery and complication rates were favorable, whether the surgery was performed by a BCS or an NBCS surgeon, irrespective of the variance in surgical technique for posterior decompression. Although additional studies are necessary to compare SL outcomes with those from other procedures, the methodological differences did not impact the surgical outcomes or complications in this study.
Lordosis of cervical sagittal alignment and ROM are known to reduce after posterior decompression surgery.30-32 Similar results were obtained in this study. However, the reductions in angles were less than 5 to 7°, and patients showed significant neurological recovery by the time of the final follow-up, irrespective of the surgical procedures. Of particular importance, there were no statistically significant differences between the BCS and NBCS groups regarding postoperative changes in cervical alignment or ROM, suggesting that posterior decompression performed by inexperienced spine surgeons has a comparable effect on dynamics of cervical spine compared to when performed by more experienced spine surgeons. Therefore, despite the postoperative reduction in cervical lordotic alignment or ROM, posterior decompression remains a useful surgical procedure for cervical OPLL whether the primary surgeon is a BCS or an NBCS.
Reviewing the literature on posterior decompression for cervical OPLL, long-term outcomes for several surgical procedures are generally favorable, although late neurological deterioration can sometimes occur.1,4,30 Notably, marked preoperative kyphosis of the cervical spine and severe (>60%) compromise of the spinal canal by OPLL seem to be limiting factors for the indication of posterior decompression.33,34 To address the aforementioned limitations, posterior decompression with spinal instrumentation is utilized in the treatment of cervical OPLL cases with these characteristics. However, there is controversial whether to adopt posterior decompression with or without spinal fusion for cervical OPLL. Recently, some reports suggested that the participation of junior surgeons increases the risks of displaced pedicle screws and insufficient correction of scoliosis.10,11,13,14 Additionally, Lee et al 12 found that the involvement of a resident in posterior cervical fusion surgery was a significant predictor for blood transfusion, operative time, and length of hospital stay. Unfortunately, our evaluation in this study was focused solely on the clinical outcomes after posterior decompression and lacked control groups of patients who underwent posterior decompression with spinal fusion. Therefore, a prospective study comparing the outcomes of posterior decompression with or without spinal fusion for cervical OPLL, performed by BCS or NBCS surgeons, should be considered in the future.
When assessing the outcomes of operations conducted by NBCS surgeons, it is crucial to consider whether an experienced senior surgeon participated in the operation and directly instructed the less experienced surgeon. In our previous report on posterior decompression surgeries for patients with CSM, BCS surgeons attended approximately 77% of the operations in which an NBCS surgeon was the primary operator. The postoperative functional outcomes and complication rates were comparable in operations performed by NBCS surgeons with or without supervision by a BCS surgeon. 27 In this study, the subjects were patients with cervical OPLL, and BCS surgeons participated as assistants in approximately 73% of posterior decompression surgeries performed by NBCS surgeons, yielding results similar to those observed for CSM, as described above. Because an NBCS surgeon is anticipated to possess a certain level of surgical experience before conducting operations without the supervision of a BCS surgeon, it is suggested that the surgical outcomes in the NBCS group was comparable whether a BCS instructor was present or not. These results indicate that posterior decompression surgery for cervical spine can be effective even when performed by inexperienced surgeons if supervised by an experienced surgeon.
Our study had several notable limitations. First, it adopted a retrospective methodology, inherently diminishing the level of evidentiary support. Second, there was no standardized educational protocol system for residents or fellows among the various institutions, and decisions regarding surgical technique and the number of decompression levels were made at the discretion and preference of the surgeons. Third, the postoperative follow-up period in this study was relatively brief for a comprehensive investigation of postoperative radiographical complication development and long-term clinical outcomes. Consequently, future assessments with a more extended observation period are imperative to validate the posterior decompression surgery for cervical OPLL. Finally, postoperative rehabilitation for patients with cervical OPLL was not consistently defined and likely varied among institutions. Despite these limitations, our study provides valuable insights into the absence of a significant difference in surgical outcomes, such as functional recovery, complication rates, and cervical dynamics between the BCS and NBCS groups. The significance of our study is underscored by the unprecedented analyses that specifically evaluated the outcomes of posterior decompression surgery for cervical OPLL when performed by BCS or NBCS surgeons.
Conclusion
The present study explored the influence of surgeon experience on treatment outcomes for cervical OPLL following posterior decompression surgery. In this investigation, surgical duration, the rate of perioperative complications, postoperative clinical outcomes, and changes in cervical dynamics on radiographs were comparable in the BCS and NBCS groups. These findings suggest that posterior decompression surgery for cervical OPLL is a safe and effective technique, even when performed by junior surgeons under the supervision of experienced spine surgeons.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.