
Abstract
Study Design:
A retrospective cohort study.
Objective:
The objective of this study was to identify important predictors of poor functional recovery in patients undergoing surgery for cervical ossification of the posterior longitudinal ligament (OPLL).
Methods:
This was a retrospective cohort study of 142 OPLL patients with laminoplasty; 135 had complete radiographical data and were followed up for ≥2 years. The following OPLL characteristics were compared between patients with “good” and “poor” outcomes (Japanese Orthopedic Association [JOA] recovery rate ≥50% and <50%, respectively): number of ossified levels, OPLL classification, ossification shape, K-line, canal-occupying ratio, and increased magnetic resonance imaging (MRI) signal intensity. Predictors of functional recovery were identified.
Results:
Pre- and postoperative (2 years following surgery) JOA scores were 10.6 ± 2.9 and 14.1 ± 2.2, respectively, indicating significant improvement following laminoplasty (P < .001). The average JOA recovery rate was 53.4% ± 34.7%, with 81 (60.0%) and 54 (40.0%) patients in the better and poorer neurological outcome groups, respectively. The canal occupation ratio of OPLL ≤60%/>60% were 117 (86.7%) and 18 (13.3%) patients, respectively. In the stepwise logistic regression analysis, an occupation ratio greater than 60% was identified as a significant factor for poor postoperative neurological outcome (relative risk, 4.82; 95% confidential interval, 1.61-14.46, P = .005).
Conclusions:
This multivariate analysis demonstrated a large size OPLL (occupying ratio >60%) was associated with a risk of poor neurological recovery roughly 5 times greater, and therefore other types of surgery are recommended in cases with such a ratio.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) is defined by pathological ossification within the posterior longitudinal ligament. OPLL can reduce the space available for the spinal cord, cause myelopathy and radiculopathy and increase the risk of a spinal cord injury following minor trauma. 1,2 Although cervical OPLL represents a common cause of degenerative cervical myelopathy (DCM) worldwide, it is most commonly diagnosed among Asian patients. 3
Several factors related to the morphology, severity, and distribution of OPLL have been defined using computed tomography (CT), radiography, and magnetic resonance imaging (MRI). These include the classification system proposed by the Japanese Ministry of Health, Labor and Welfare (continuous, segmental, mixed, or circumscribed), 4 the shape of ossification (hill- or plateau-shaped), 5 the extent of OPLL relative to a K-line (positive or negative), 6 and the canal occupying ratio. These factors may be associated with myelopathy severity, influence treatment decisions, and predict functional outcomes, disease progression and risk of complications.
Recently, a systematic review of the literature was conducted to evaluate the association between various features of OPLL and outcomes following surgery for cervical myelopathy. 7 Based on this review, there was low evidence that patients with hill-shaped OPLL have worse Japanese Orthopaedic Association (JOA) scores after laminoplasty than those with plateau-shaped ossification. Unfortunately, there was insufficient evidence to determine whether other characteristics of OPLL are important predictors of surgical outcomes. This review identified critical knowledge gaps and highlighted major limitations in the current body of literature, including inconsistent results, unknown precision of effect estimates and lack of multivariate analyses controlling for important confounders.
The purpose of this study was to investigate the association between various features of cervical OPLL and postoperative functional recovery using multivariate analysis.
Materials and Methods
Patient Population
From 2008 to 2014, a total of 142 consecutive patients with cervical OPLL patients underwent cervical laminoplasty in the 2 hospitals with the approval of institutional ethics committees. Patients who had sudden neurological deterioration due to minor trauma, spinal cord injury, histories of cervical spine, malignancies, or neurological diseases such as cerebral infarction or spinal diseases at other levels were not included in the original 142 patients. After exclusion of patients with follow-ups of less than 2 years or incomplete radiographical data, 135 were retrospectively evaluated with the institutional review board approval. A clinical diagnosis of cervical OPLL was confirmed by CT in all patients. We investigated clinical and radiographical features and assessed the factors affecting postoperative poor neurological outcomes. Each patient’s neurological status was evaluated using the Japanese Orthopedic Association score for cervical myelopathy (maximum score 17), and the JOA score recovery rate was calculated using this formula: (postoperative JOA score − preoperative JOA score) / (17 − preoperative JOA score) × 100 (%). Regarding neurological recovery, the patients were divided into better (JOA recovery rate ≥50%) and poor (JOA recovery rate <50%) recovery groups at 2 years postoperatively. 8
Assessment of OPLL
Number of ossification levels (longitudinal extent of OPLL), K-line (positive or negative), 6 JOA welfare classification (continuous, segmental, mixed, and circumscribed), 4 shape of OPLL lesion (hill-shaped or plateau-shaped), 5 spinal canal occupation ratio of OPLL on axial CT at the maximum cord compression level, and signal intensity change on T2-weighted MRI were investigated by 2 independent orthopedic spine doctors (H.N. and S.K.). All patients underwent high-resolution MRI with a 1.5-T Signa (GE Medical Systems, Milwaukee, WI) imager before surgery. The slice width was 4 mm and the acquisition matrix was 512 × 256. The sequence parameters were repetition time (TR) 400 ms/echo time (TE) 11 ms for T1-weighted images, and TR 4000 ms/TE 126 ms for T2-weighted images. Signal intensity changes in the spinal cord were classified into 3 groups based on sagittal T2-weighted images 9 : grade 0, none; grade 1, light (increased intensity, but less intense compared with cerebrospinal fluid signal); and grade 2, intense (similar intensity to cerebrospinal fluid signal). Grades 1 and 2 signal-intensity changes were judged as signal intensity change on MRI in this study.
K-line is a straight line connecting the midpoints of the spinal canal at C2 and C7 on a neutral lateral radiograph; K-line (–) indicates that OPLL extends beyond the K-line, whereas K-line (+) indicates that it does not. 6 In the JOA welfare classification system, “continuous” indicates a long lesion extending over several vertebral bodies, “segmental” indicates 1 or several separate lesions behind vertebral bodies, “mixed” indicates a combination of the continuous and segmental types, and “circumscribed” indicates a location posterior to a disc space. 4 “Hill-shaped” means a massive beak-shaped ossification localized to certain levels, whereas “plateau-shaped” means a relatively narrow spinal canal without any localized massive ossification. 5 C2-7 lordotic angle (the angle between the C2 inferior and C7 inferior end- plates) and C2-7 sagittal vertical axis (SVA; the distance between a plumb line dropped from the centroid of C2 and posterior superior corner of C7) were also measured.
Statistical Analysis
SPSS version 21 (IBM SPSS Statistics 21.0, IBM Corporation, Armonk, NY) was used for statistical analysis. The mean values are presented as mean ± standard deviation. Student t test and chi-square test were used to compare the 2 groups, and 1-way analysis of varaince (post hoc: Tukey) was used to compare more than 3 groups. Risk factors associated with poor surgical outcomes were identified by stepwise multivariate logistic regression analysis. P < .05 was considered to be a statistically significant difference.
Results
Ultimately, a total of 135 patients were included in the current study (average age 62.5 ± 10.9 years old; 105 males and 30 females), 4 patients with inadequate follow-up and 3 patients with incomplete radiographical data having been excluded from the initial 142 patients. The length of laminoplasty was 5.0 ± 0.7 levels. Laminoplasty was performed over a wider range of levels with ossification because of the existence of spinal cord compressions at other levels due to disc bulging and hypertrophy of yellow ligament. French-door laminoplasty 10 was performed in all cases.
Pre- and postoperative (2 years following surgery) JOA score averages were 10.6 ± 2.9 and 14.1 ± 2.2, respectively. The average JOA recovery rate was 53.4% ± 34.7%, and 81 (60.0%) and 54 (40.0%) patients were in the “better” and “poor” neurological outcome groups, respectively.
The average number of ossification levels was 3.0 ± 1.3, and the K-line was positive in 111 (82.2%) and negative in 24 (17.8%) of the patients. Regarding the JOA welfare classification, 33 (24.4%) were segmental, 47 (34.8%) continuous, 47 (34.8%) mixed, and 8 (5.9%) circumscribed. Hill-shaped ossification was identified in 31 (23.0%) of the patients, and plateau-shaped in 104 (77.0%) of the patients. The average spinal-canal occupation ratio of OPLL was 40.9% ± 15.8%; occupation ratios ≤60% were found in 117 (86.7%) of the patients, and ratios >60% in 18 (13.3%) of the patients. Increased signal intensity on MRI was found in 48 (35.6%) of the patients.
In the comparison between patients with better and poor JOA recovery rates, an occupying ratio greater than 60% was significant (P < .003), whereas age, gender, presence of diabetes mellitus, preoperative JOA score, duration of symptoms, number of ossification levels, K-line state (+/−), JOA welfare classification, shape (hill- or plateau-shaped), cervical alignment and increased signal intensity change on MRI were not significant factors (Table 1). In the stepwise logistic regression analysis, an occupying ratio greater than 60% was a significant risk factor resulting in poor postoperative JOA recovery rate following laminoplasty (relative risk, 4.82; 95% confidential interval [CI], 1.61-14.46; P = .005; Table 2).
Comparison of Factors in the “Better” and “Poor” Surgical Outcome Groups.
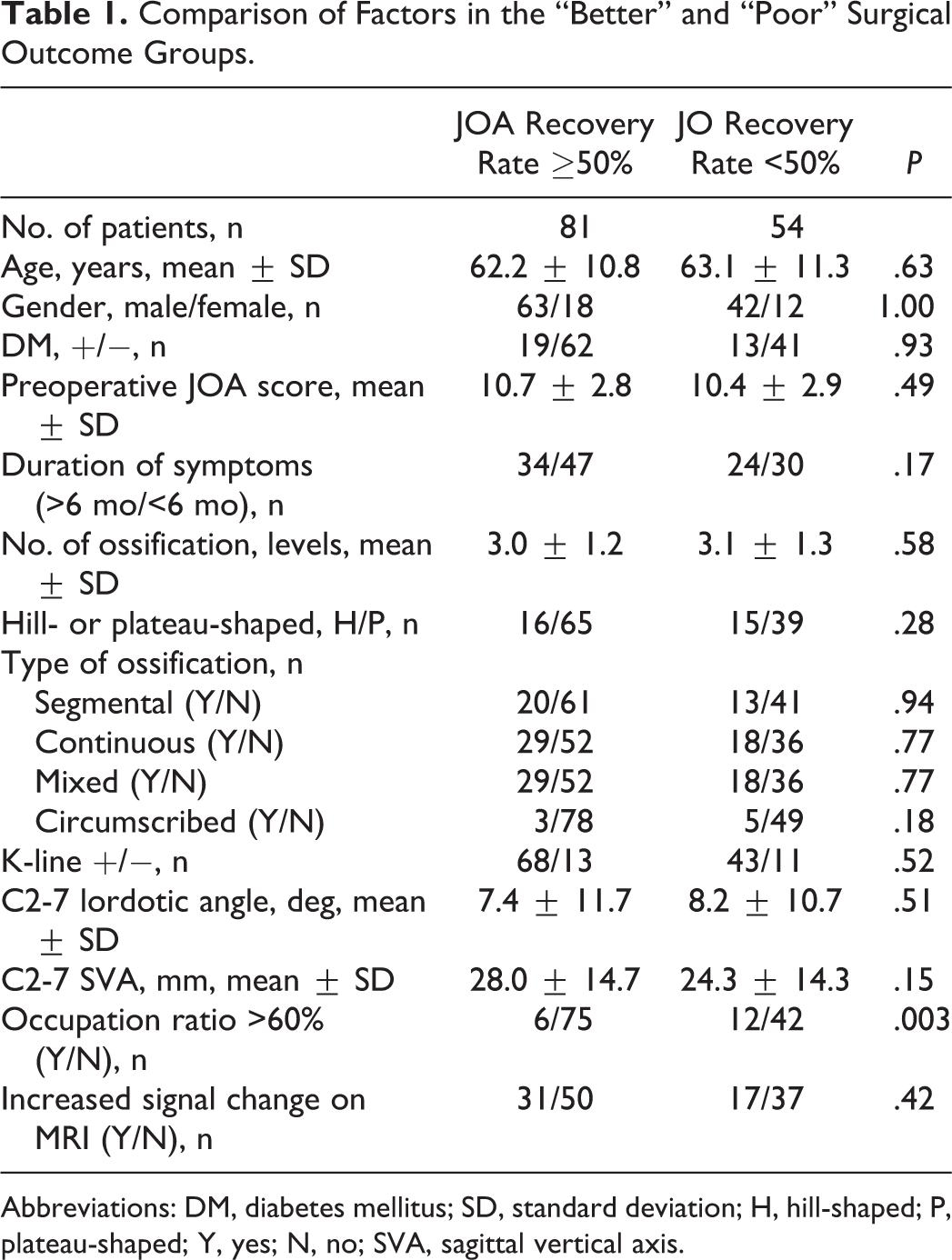
Abbreviations: DM, diabetes mellitus; SD, standard deviation; H, hill-shaped; P, plateau-shaped; Y, yes; N, no; SVA, sagittal vertical axis.
Multivariate Analysis.

In a comparison of shapes and occupation ratios, continuous type included significantly higher ratio (48.5% ± 12.3%) compared with segmental (33.0% ± 17.0%; P < .001) and mixed (38.3% ± 15.7%; P < .01) types, although there were no differences with circumscribed type (42.4% ± 6.5%). When comparing shape and neurological recovery, although JOA recovery rate was higher in cases with segmental (57.4% ± 30.4%) or continuous (57.5% ± 29.3%) types than with mixed (48.7% ± 40.8%) or circumscribed (40.2% ± 35.4%) types, there was no statistically significant difference (P = .38). In the comparison between occupation ratio and K-line, occupation ratio was higher in cases with K-line negative (43.5% ± 13.6%) than with K-line positive (40.3% ± 13.6%); however, there was no statistically significant difference (P = .38).
A Representative Case
A 66-year-old man with cervical OPLL. His comorbid illness was only hypertension. His JOA welfare classification was continuous type and his ossification was plateau-shaped (Figure 1). His preoperative K-line was positive on his radiograph with a preoperative C2-7 lordotic angle of 29°. His preoperative occupying ratio of OPLL was 74.5% and increased signal intensity change was identified on MRI. He underwent cervical laminoplasty from C3 to C6 and laminectomy at C2. His preoperative JOA score was 7 but had deteriorated to 6 at 2 years following surgery (JOA recovery rate was −10%). His cervical alignment was found to have changed to kyphotic on radiograph and K-line had changed to negative at 2 years following surgery.
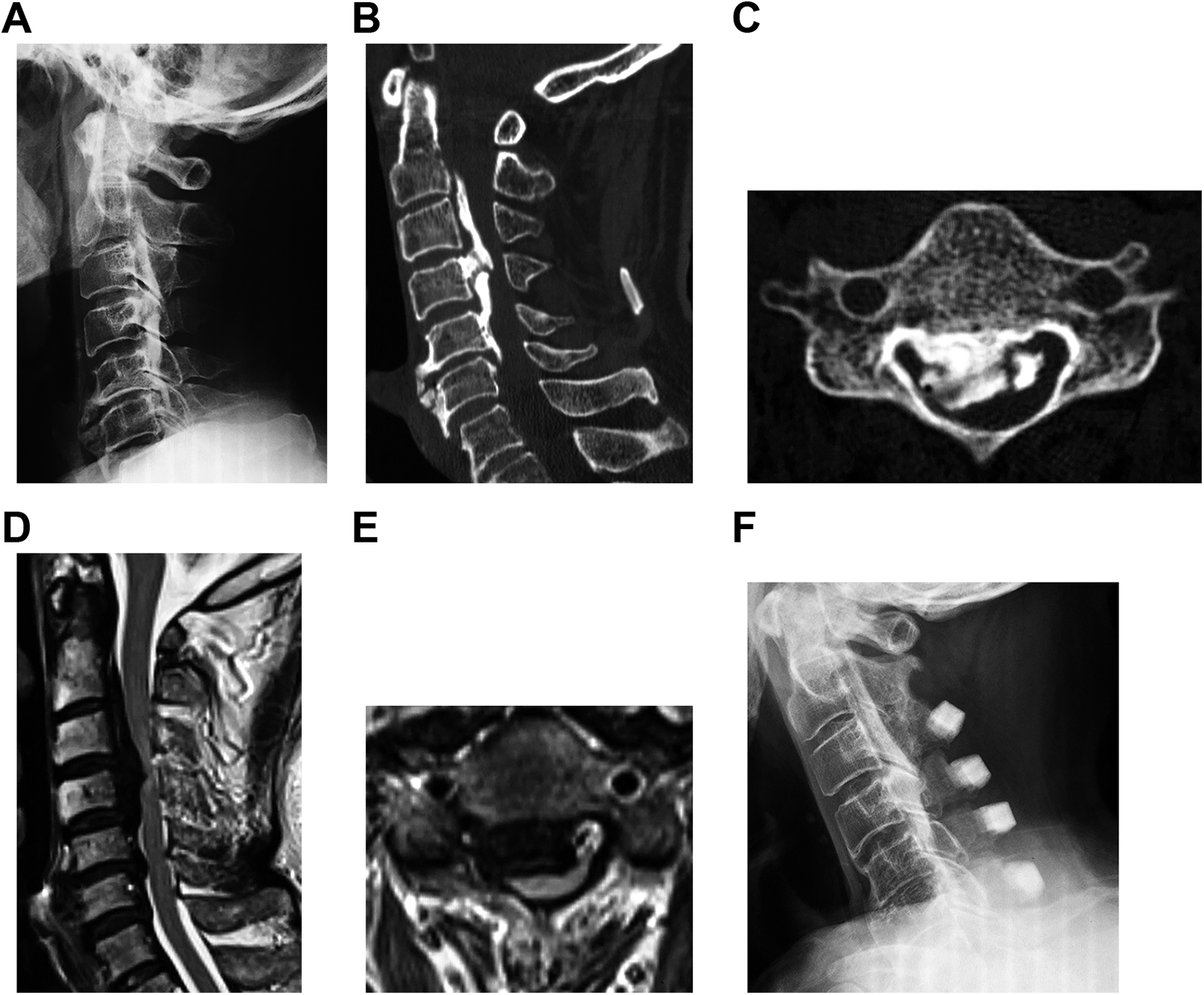
A 66-year-old man with cervical ossification of the posterior longitudinal ligament (OPLL). (A) Preoperative lateral radiograph; preoperative computed tomography on sagittal (B) and axial (C) images; preoperative magnetic resonance imaging on sagittal (D) and axial (E) images; and postoperative lateral radiograph at 2 years after cervical laminoplasty (F).
Discussion
This study analyzed the association between OPLL factors and poor surgical recovery following laminoplasty for cervical myelopathy. To evaluate important predictors of surgical outcomes, a multivariate analysis must be conducted that controls for important confounding variables. 7 In a recent systematic review, 7 28 prognostic cohort studies were identified that evaluated the association between characteristics of ossification, features of spinal cord compression and surgical outcomes; however, only 7 of these studies conducted a multivariate analysis. The objective of this current study was to address the limitations in the current body of evidence and conduct a rigorous multivariate analysis that considered a number of important OPLL variables. Based on our results, patients with an OPLL occupying ratio >60% are more likely to exhibit a poor JOA recovery rate than those with a ratio ≤60%. In contrast, K-line negative, hill-shaped OPLL, and increased signal intensity change on MRI were not identified as significant predictors of functional outcomes.
There is controversy surrounding the surgical strategies for cervical OPLL, but posterior decompression surgery, “laminoplasty,” is one of the most common approaches because cervical laminoplasty provides satisfactory clinical and radiographical outcomes in patients with OPLL, 11 -14 while being less technically demanding and resulting in fewer complications, especially when patients with long segments (>3 levels) are involved. 13 The anterior approach and posterior decompression with fusion could also be effective alternatives, as they permit better cervical alignment or spinal cord decompression in some cases, 13 but both might be costlier, and can result in a number of complications (cerebrospinal fluid leakage, graft dislocation, or intraoperative neurological injury in the case of anterior surgery; instrumentation failure or adjacent segment disease in the case of posterior decompression with fusion). 13,15,16 The logical approach would thus be to select candidates for laminoplasty who can be expected to achieve sufficient clinical results following that procedure, and opt for the anterior approach or posterior decompression with fusion with patients who might not achieve sufficient clinical results with laminoplasty.
To know the risk factors for poor surgical outcomes, it is crucial to conduct a multivariate analysis, yet few analyses of this type have been conducted. 7 For example, several parameters for ossification and spinal cord compression features have been reported, but few studies have included all of these factors together 16 and the relationship between these parameters and neurological outcomes is unclear from these studies. Gu et al 17 conducted a multivariate analysis to investigate the risk factors for poor surgical outcomes (=JOA recovery rate <50%) in 184 cervical OPLL cases in 2016, with the analysis including K-line, occupying ratio, MRI signal intensity change, and shape of ossification (hill- or plateau-shaped). 17 They reported that a longer duration of symptoms, T1 hypointensity on MRI, and a history of minor trauma were closely associated with poor neurological recovery. However, this study had some potential limitations: (a) several types of surgical approaches were included, and it was hard to tell the prognosis for each approach; (b) K-line was measured on sagittal CT, which would seem to be at odds with the approach introduced in an original article 6 using lateral radiograph to evaluate 2 factors, cervical alignment and OPLL size, as 1 parameter; (c) their subjects were heterogeneous, namely a mixture of cases of neurological damage due to trauma and those due to degenerative change. A rigorously conducted multivariate analysis avoiding shortcomings such as those here still needs to be conducted in order to clearly establish the risk factors for poor surgical outcomes, thereby greatly facilitating the selection of patients who could benefit from laminoplasty.
K-line was developed by Fujiyoshi et al 6 to predict poor clinical outcomes after laminoplasty. Patients with cervical OPLL who exhibit a negative K-line (−) are thought to have poor clinical outcomes if laminoplasty is selected. 6,18,19 K-line is a concise evaluation method, and it is widely used these days. However, some limitations exist: (a) It can be hard to clearly see the OPLL and/or the midpoints of the spinal canal at C7 in the lateral radiograph compared with CT, and interobserver error sometimes occurs. (b) K-line can be easily affected by patients’ cervical position when taking radiographs, and several reports have doubted the validity of predictions based just on one neutral radiograph. 18 Li et al 18 claimed that patients with a positive K-line (+) in the neck extension position could have good neurological outcomes, even those with a negative K-line (−) in the neck neutral position. Takeuchi et al, 19 however, have suggested that the neck-flexed position is the crucial one when evaluating K-line. (c) Postoperative kyphotic change can occur in some cases after cervical posterior decompression surgery, as shown in our representative case, and it is hard to predict whether patients’ K-lines will become negative following surgery and whether there will be enough spinal cord decompression, even in patients exhibiting a positive K-line (+) preoperatively. Thus, it is as yet unclear whether K-line can actually be an accurate predictor of neurological outcomes or not as previously reported. 20,21
Hill- and plateau-shaped classification was reported on by Iwasaki et al. 5 They found that patients with hill-shaped lesions had significantly lower JOA scores after laminoplasty than those with plateau-shaped lesions. However, in our systematic review of neurological outcomes after surgery in patients with OPLL, there was little evidence to suggest that patients with a hill-shaped lesion have a worse postoperative JOA score after laminoplasty than those with a plateau-shaped lesion. 7 It is still unknown whether hill-shaped lesion shape is really associated with poor surgical outcomes 5,17,20 ; however, this classification did not have any significance in the current study.
An occupation ratio of OPLL >60% has been reported as a risk factor for poor surgical outcomes following laminoplasty in patients with OPLL. Iwasaki et al 5 first reported that the surgical outcome was significantly poorer in patients with an occupation ratio of OPLL in the spinal canal >60%, and that an occupation ratio of 60% is the limit for successful laminoplasty. It has also been reported that laminoplasty does not provide as sufficient of outcomes as other surgeries. Kim et al 22 retrospectively compared surgical outcomes between patients with anterior decompression and fusion (71 cases) and laminoplasty (64 cases), and reported that anterior surgery provided more favorable outcomes in patients with an occupation ratio >60% (JOA recovery rate 75.70 ± 30.26, compared with 41.65 ± 84.02 for laminoplasty, P = .048). Fujimori et al 20 reported on long-term results (mean duration of follow-up 10.1 years [range, 2-22 years]) following surgery in patients with an occupation ratio >60%, comparing results with anterior decompression and fusion (12 cases) and those with laminoplasty (15 cases). Anterior surgery cases displayed significantly better recovery rates at final evaluation (53%, compared with 30% with laminoplasty, P = .04). 20 Chen et al 23 conducted a meta-analysis including 10 nonrandomized controlled studies involving 819 patients, and concluded that anterior corpectomy and fusion resulted in better JOA recovery rates in cases with an occupation ratio >60%, while there was no significant difference in cases with an occupying ratio ≤60%. Although several studies have claimed that a high occupation ratio is not associated with poor neurological results, 7 taking into consideration the results of the current study as well as others mentioned here, other types of surgeries should probably be recommended in cases with an occupying ratio >60% in view of the prospects for better neurological recovery.
There are some limitations to the current study: (a) It was a retrospective analysis. (b) The subjects were limited to Japanese people (although our previous findings showed no racial differences in neurological recovery following cervical decompression 24 ). (c) A minimum of 2 years of follow-up is not a very long term following surgery: further long-term follow-up should be conducted to evaluate postoperative enlargement and progression of OPLL and assess neurological deterioration after surgery. (d) Although we used JOA recovery rate in the current study because this method has been most widely used, better recovery rate could be obtained in cases with severe preoperative JOA. So far there have been no papers published regarding minimum clinically important difference in “JOA” score, but future sturdies regarding neurological recovery based on minimum clinically important difference are needed. (e) There are numbers of risk factors we did included in this study: the extent of signal change, T1 hypo signal, shape of the cord, snake eyes on MRI, and others. Increasing the number of elements to be examined to include those connected with risk factors unrelated to ossification could complicate the analysis, and so we could not include all factors in the current article. (f) The focus of this study was a mere 142 OPLL patients, and so it was not a large scale-study like those involving more than 1000 patients. Consequently, the value of the statistical results for reaching a definitive conclusion was limited. Future large-scale prospective multicenter studies are needed.
In conclusion, a large-sized OPLL (occupying ratio >60%) was found to be associated with a risk of poor neurological recovery roughly 5 times greater than that in cases with smaller OPLLs at 2 years after laminoplasty. In such cases, anterior approach or posterior decompression with fusion surgery should therefore be considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.