
Abstract
Study Design
Systematic Review and meta-analysis.
Objective
To conduct an updated systematic review and meta-analysis of complications associated with different anterior fusion techniques/approaches and adjuvant resources (i.e., computed tomography angiography (CTA), rhBMP-2, and access surgeons).
Methods
A systematic review was conducted from 1/1/2014-4/1/2024 for studies evaluating the incidence of complications associated with anterior lumbar procedures. Comparisons of complications were made between surgical approach, use of CTA, rhBMP-2, and access surgeons. Meta-analyses were conducted using a generalized linear mixed model.
Results
54 studies were included in the final analysis with 8066 patients and an average follow-up of 31.2 months. The overall complication rate associated with anterior lumbar surgery was 13.1%, including an intraoperative complication rate of 3.8%, postoperative complication rate of 7.4%, infection rate of 1.5%, and reoperation rate of 1.7%. Forest plot analysis showed no significant difference in overall complication rates between open and mini-open techniques, although mini-open techniques were associated with lower overall reoperation rates. The use of CTA was associated with an increase in intraoperative and overall complications, and the use of an access surgeon was associated with a decreased risk of reoperation. The use of rhBMP-2 was not associated with overall complication risk.
Conclusions
While anterior lumbar surgery provides numerous benefits, surgeons and patients alike should be aware of the complication and safety profile prior to surgery. High quality studies are warranted to help elucidate the true benefit of certain techniques and adjuvant resources in reducing complications.
Keywords
Introduction
Since the first lumbar fusion procedure, the field of spine surgery has undergone considerable advancements in surgical techniques, graft/implant materials, and stabilization systems.1-3 Patient-specific demographics, unique anatomy, and surgical indications have also allowed the emergence of different approaches to the lumbar spine. Recent years have shown an increased incidence of anterior approaches to the lumbar spine, with particular evolutions in minimally invasive techniques and advanced imaging modalities.4-6
Anterior lumbar techniques for both anterior lumbar interbody fusions (ALIF) and artificial disc replacement (ADR) provide numerous benefits, including: (1) sparing of posterior lumbar paraspinal musculature and stabilizing ligaments, (2) direct access to the anterior column of the spine, (3) reduced long-term muscle-related pain, (4) improved postoperative mobility, (5) suitable intervertebral disc distraction, (6) ability to address sagittal balance, (7) larger contact area for fusion, (8) cancellous bone interface, (9) compressive loading between bone surfaces, and 10) direct access to the degenerative pathology.7-11 Despite these advantages, surgeons should be aware of potential anterior approach complications and the incidence with which they occur. In addition to helping surgeons avoid and manage intraoperative complications, knowledge of potential pitfalls helps facilitate conversations between surgeons and their patients to improve patient expectations.
Surgeons have employed various resources to help reduce the rate of complications, including for anterior lumbar surgery. In an older meta-analysis of studies published from 1992 to 2013, Bateman et al. 12 report an overall complication rate of 14.1% for anterior lumbar surgery. However practice patterns over the past few years have changed due to innovations in approach techniques (retroperitoneal vs transperitoneal), use of recombinant human bone morphogenetic protein-2 (rhBMP-2), computed tomography angiography (CTA), and dedicated approach surgeon training.13-16 As a result, the purpose of the current study was to conduct an updated systematic literature review and meta-analysis of complications associated with anterior lumbar surgery with the aim of assessing the incidence of complications associated with different anterior fusion techniques/approaches and adjuvant resources.
Methods
Literature Search Including Inclusion/Exclusion Criteria
A systematic review and meta-analysis was conducted by two independent reviewers using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 17 An electronic literature search for relevant studies was conducted using the PubMed MEDLINE and Cochrane Central Register of Controlled Trials (CENTRAL) databases. A systematic search was done using a combination of the following search terms from January 1st, 2014 to April 1st, 2024: (“anterior lumbar”) AND (“surgery” OR “procedures” OR “operations”) AND (“complications”). No minimum/maximum number of studies was determined prior to conducting the study. The reference lists of review articles, clinical trials, and meta-analyses were reviewed to collect additional relevant studies. Only reports with the most recent or complete follow-up data for clinical studies utilizing the same patient cohorts were included.
Studies were included in the final analysis if the following criteria were satisfied: (1) randomized clinical trials (RCTs), prospective/retrospective cohort studies, case-control studies, (2) study participants were 18 years or older, (3) the details of surgical technique were described, and (4) incidence of specific complications were reported. Required surgical details included description of the type of procedure, approach, use of preoperative computed tomography angiography (CTA), and identification of which surgeon performed the approach. Studies were excluded if (1) studies were case reports, review articles, editorials or letters, (2) studies were not in English, or (3) more than 5% of the patient sample underwent anterior lumbar surgery for trauma, tumor, or infection.
Data Extraction/Synthesis
All articles included in the final analysis were manually reviewed and analyzed to extract the following data: author, location of study, year, study design, level of evidence (based on Wright et al. 18 ), length of follow-up, demographic information (patient sample size, average age, sex, smoking status, previous lumbar surgery, worker’s compensation status, number of levels operated), surgical case characteristics (anterior approach [open vs mini-open, retroperitoneal vs transperitoneal], type of procedure [ALIF, ADR, circumferential fusions, and hybrid procedures], preoperative use of CTA, intraoperative use of rhBMP-2, and use of an access surgeon to help direct exposure. Open surgeries were traditional anterior lumbar incisions while mini-open incisions were those that were performed with a mini-Pfannenstiel incision or one of similar size. A hybrid surgery was defined as a simultaneous ALIF and ADR. An “access surgeon” was defined as a general, vascular, or urologic surgeon who completely exposed or assisted in the initial surgical exposure.
Complications were stratified into two groups: intraoperative and postoperative complications. Intraoperative complications included: arterial/venous injury, ureter/bladder injury, peritoneal injury, dural injury, bowel injury, neurologic/nerve root injury, arterial thrombi, retrograde ejaculation, and incisional hernia. Postoperative complications included: deep vein thrombosis (DVT), ileus, pulmonary embolism, hematoma/seroma, infection (superficial/deep), wound dehiscence, pneumonia/atelectasis, urologic complications, prosthesis-/graft-/cage-related complications, and other. Furthermore, rates of reoperation surgery were recorded for each study, when available.
Quality Assessment
Two different scales were used to evaluate the quality of all included studies. Randomized controlled trials were assessed using the Jadad Scale, and a high quality study was defined as a score greater than or equal to 4. 19 Non-randomized studies were assessed using the Newcastle-Ottawa Scale (NOS), and a high quality study was defined as a score greater than or equal to 7. 20
Statistical Analysis
Overall incidences of complications (intraoperative, postoperative, overall, reoperations) were reported as weighted proportions. Incidences of all other complications were reported as simple proportions. Data extracted from included studies were combined using a generalized linear mixed model (GLMM). Forest plots were created to compare odds ratios between each variable of interest. Regression analysis of approach (ie, mini-open/laparoscopic and transperitoneal) used open and retroperitoneal procedures as the reference, respectively. Complete analysis of all complications was unable to be included in forest plots due to limited incidence. Statistical significance was established at P < 0.05. All analyses were conducted using R software (R Foundation for Statistical Computing, Vienna, Austria).
Results
Search Results
A systematic search of databases resulted in 7430 records. Combined with 8 additional records identified from other sources, 4898 records were screened after removing duplicates, and 271 were deemed eligible for full-text review. Ultimately, 54 studies were included in qualitative and quantitative analysis (Figure 1). PRISMA flowchart.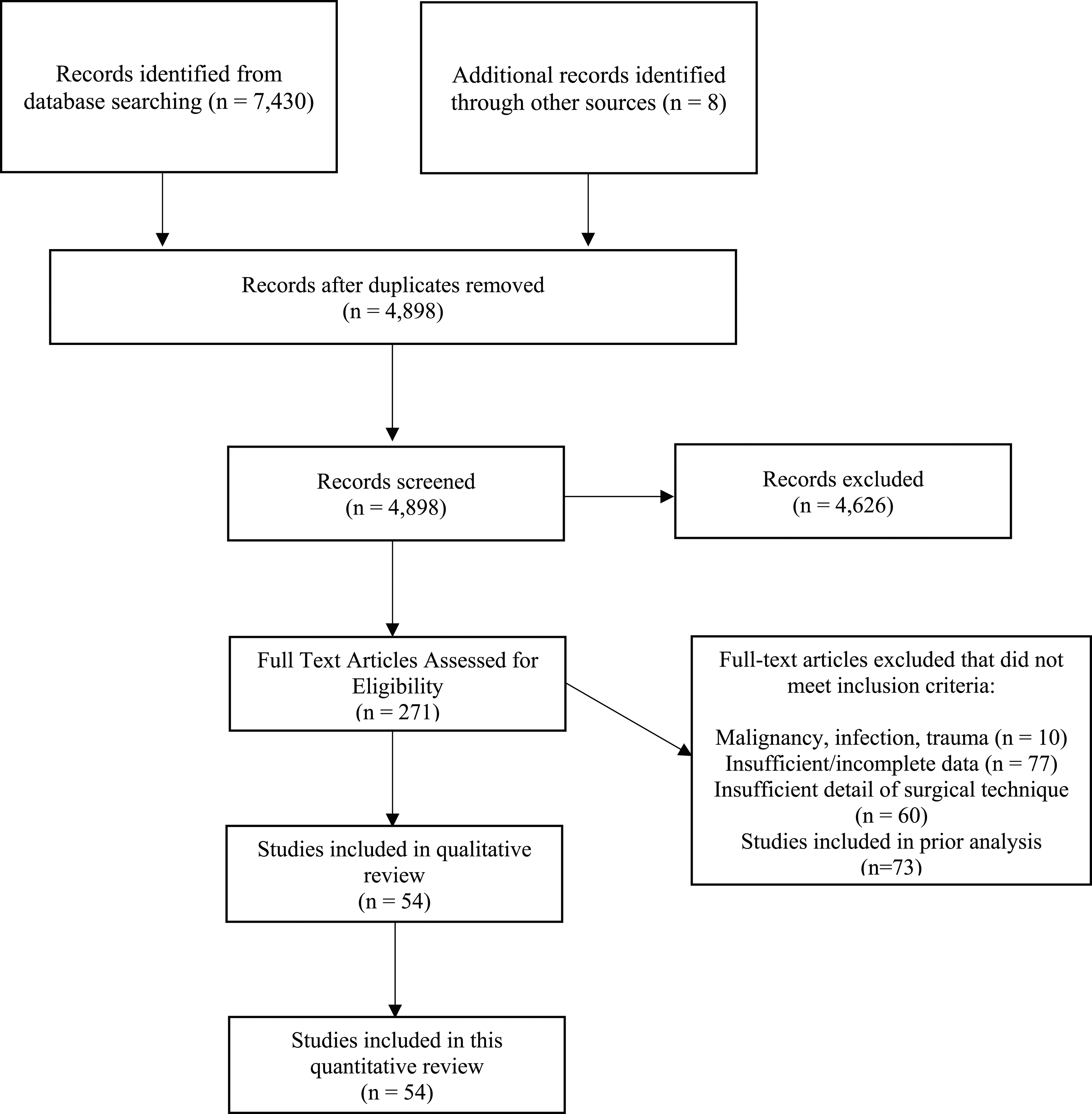
Study Characteristics
Demographic and Surgical Information.
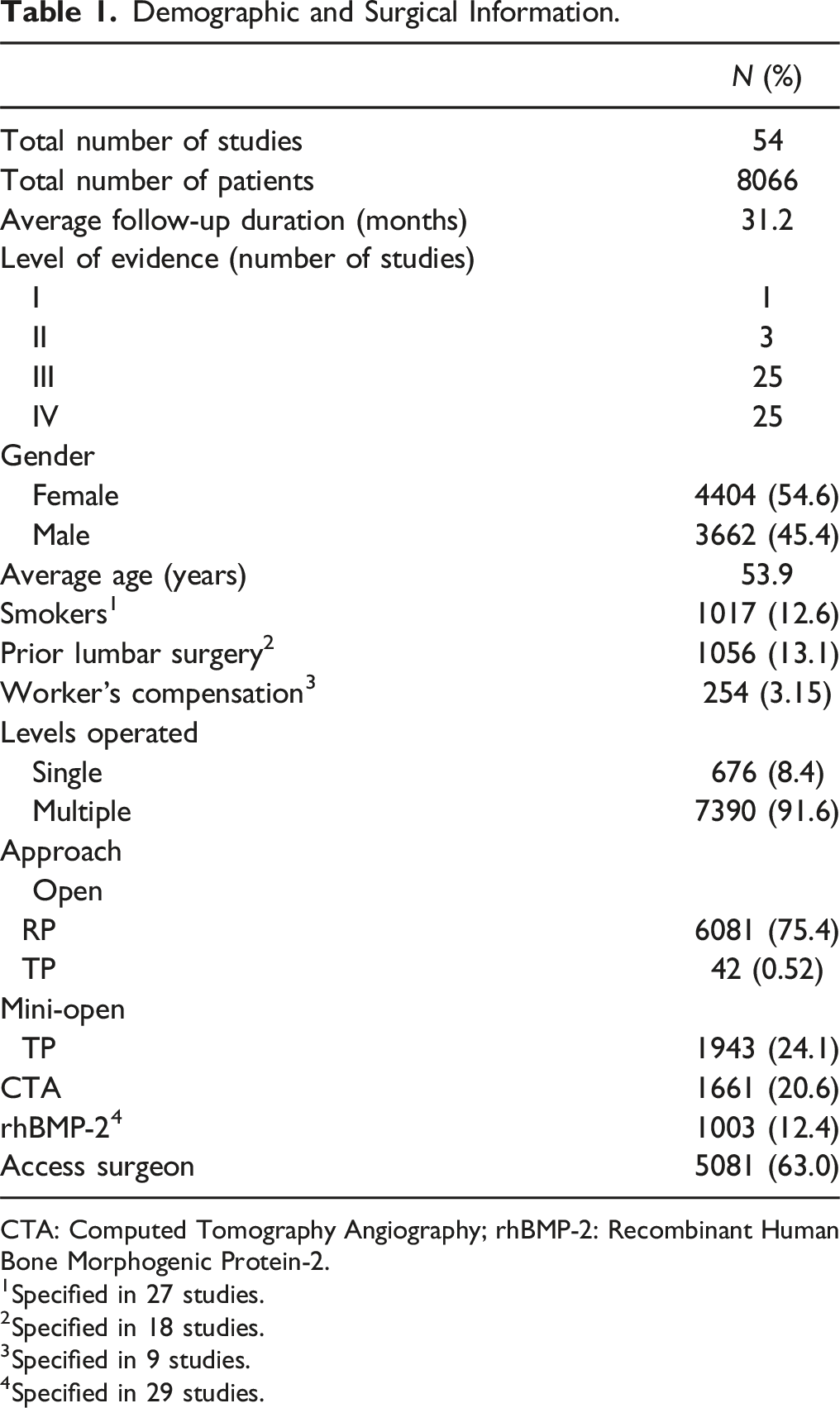
CTA: Computed Tomography Angiography; rhBMP-2: Recombinant Human Bone Morphogenic Protein-2.
1Specified in 27 studies.
2Specified in 18 studies.
3Specified in 9 studies.
4Specified in 29 studies.
Quality Assessment
Study Characteristics.
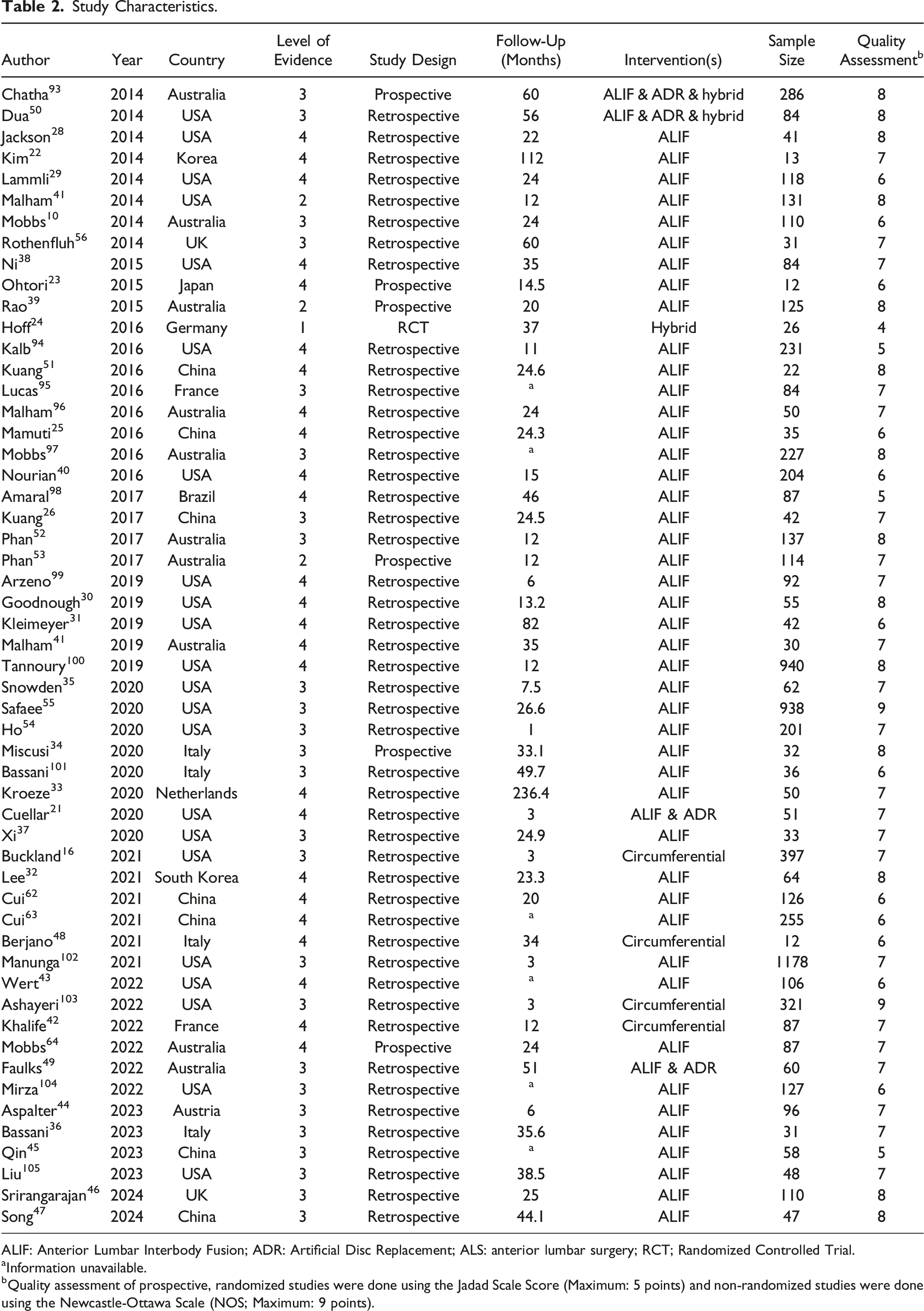
ALIF: Anterior Lumbar Interbody Fusion; ADR: Artificial Disc Replacement; ALS: anterior lumbar surgery; RCT; Randomized Controlled Trial.
aInformation unavailable.
bQuality assessment of prospective, randomized studies were done using the Jadad Scale Score (Maximum: 5 points) and non-randomized studies were done using the Newcastle-Ottawa Scale (NOS; Maximum: 9 points).
Overall Complication Rate
Complication Rates of Each Study.
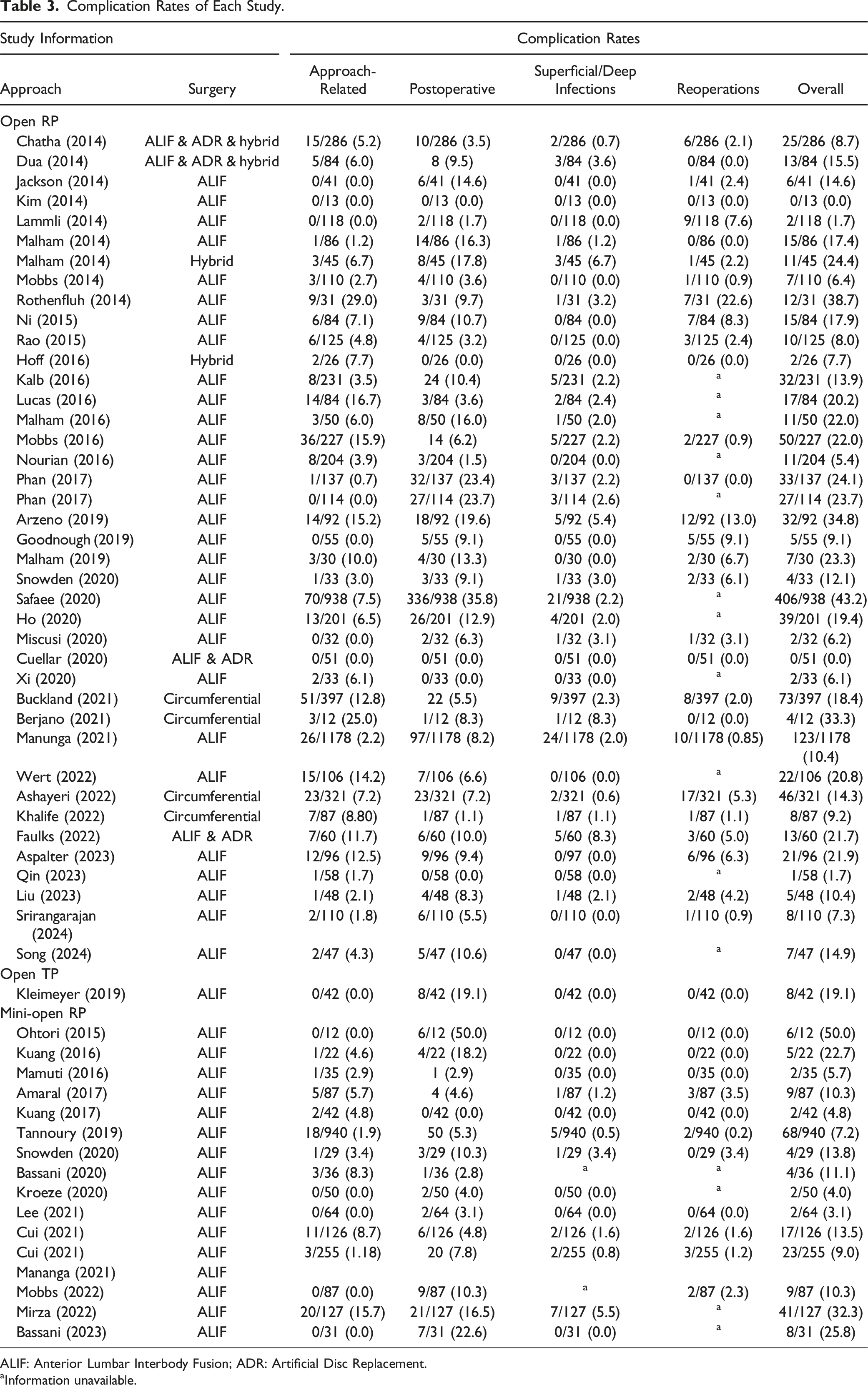
ALIF: Anterior Lumbar Interbody Fusion; ADR: Artificial Disc Replacement.
aInformation unavailable.
The three most common intraoperative complications were: (1) venous injury (1.9%), (2) neurologic injury (1.6%), and (3) incisional hernia (0.6%). The most common postoperative complications were: (1) ileus (2.6%), (2) urologic (1.2%), superficial infection (1.2%), and (3) other complications (1.7%).
Complication Rate by Approach
Comparisons stratified by approach showed that open procedures experienced a greater rate of overall (18.5% vs mini-open: 11.6%), intraoperative (6.1% vs mini-open: 2.6%) complications, postoperative complications (12.4% vs mini-open: 7.6%), superficial/deep infections (1.3% vs mini-open: 0.93%) and reoperations (1.6% vs mini-open: 0.8%). Forest plot analysis showed patients who underwent mini-open procedures were less likely to undergo reoperation (OR: 0.09; CI: 0.02, 0.41; P < 0.05) compared to patients undergoing open procedures.
Compared to patients who underwent a retroperitoneal approach, patients who underwent a transperitoneal approach experienced a higher overall (19.1% vs 13.6%) and postoperative complication rate (19.1% vs 7.1%), irrespective of the lumbar surgery performed. On the other hand, a retroperitoneal approach was associated with increased intraoperative complication (4.5% vs 0%), superficial/deep infection (1.7% vs 0%), and reoperation (2.2% vs 0%) rates (Figure 2). Complication rate by approach.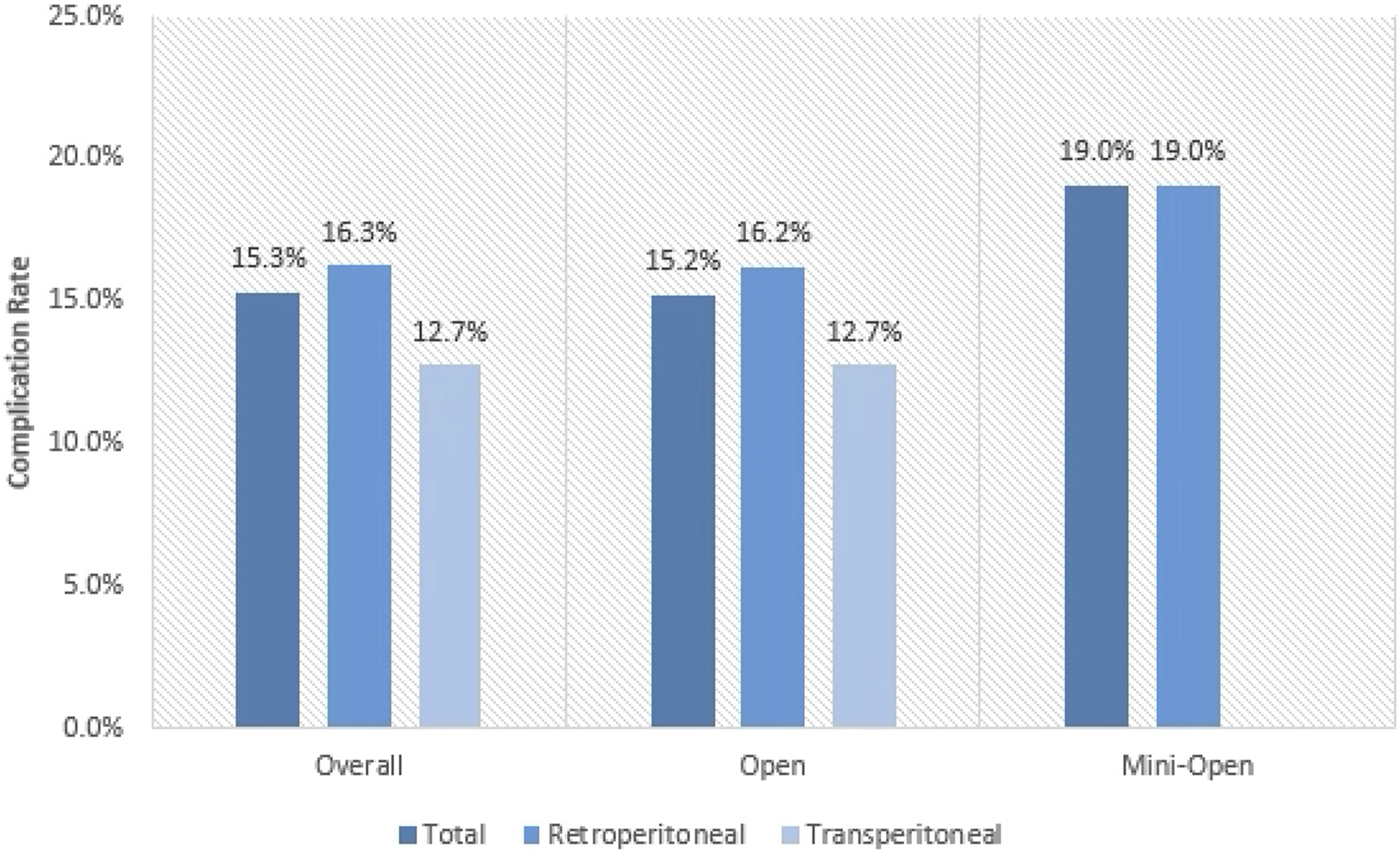
Complication Rate by Surgery Type
Four anterior surgical techniques were analyzed: ALIF, ADR, circumferential fusions, and hybrid procedures. Hybrid procedures exhibited the highest rates of overall (18.3% vs circumferential: 16.0% vs ADR: 13.3% vs ALIF: 16.6%) and superficial/deep infections (4.2% vs circumferential: 1.5% vs ADR: 4.1% vs ALIF: 1.5%). ALIF procedures exhibited the highest rate of postoperative complications (11.7% vs circumferential: 5.8% vs ADR: 7.2% vs hybrid: 11.3%). Circumferential procedures exhibited the highest rates of intraoperative complications (10.8% vs hybrid: 8.5% vs ADR: 6.2% vs ALIF: 4.9%) and the highest rate of reoperations (1.8% vs ADR: 1.5% vs hybrid: 1.4% vs ALIF: 1.3%) (Figure 3). Complication rate by type of surgery.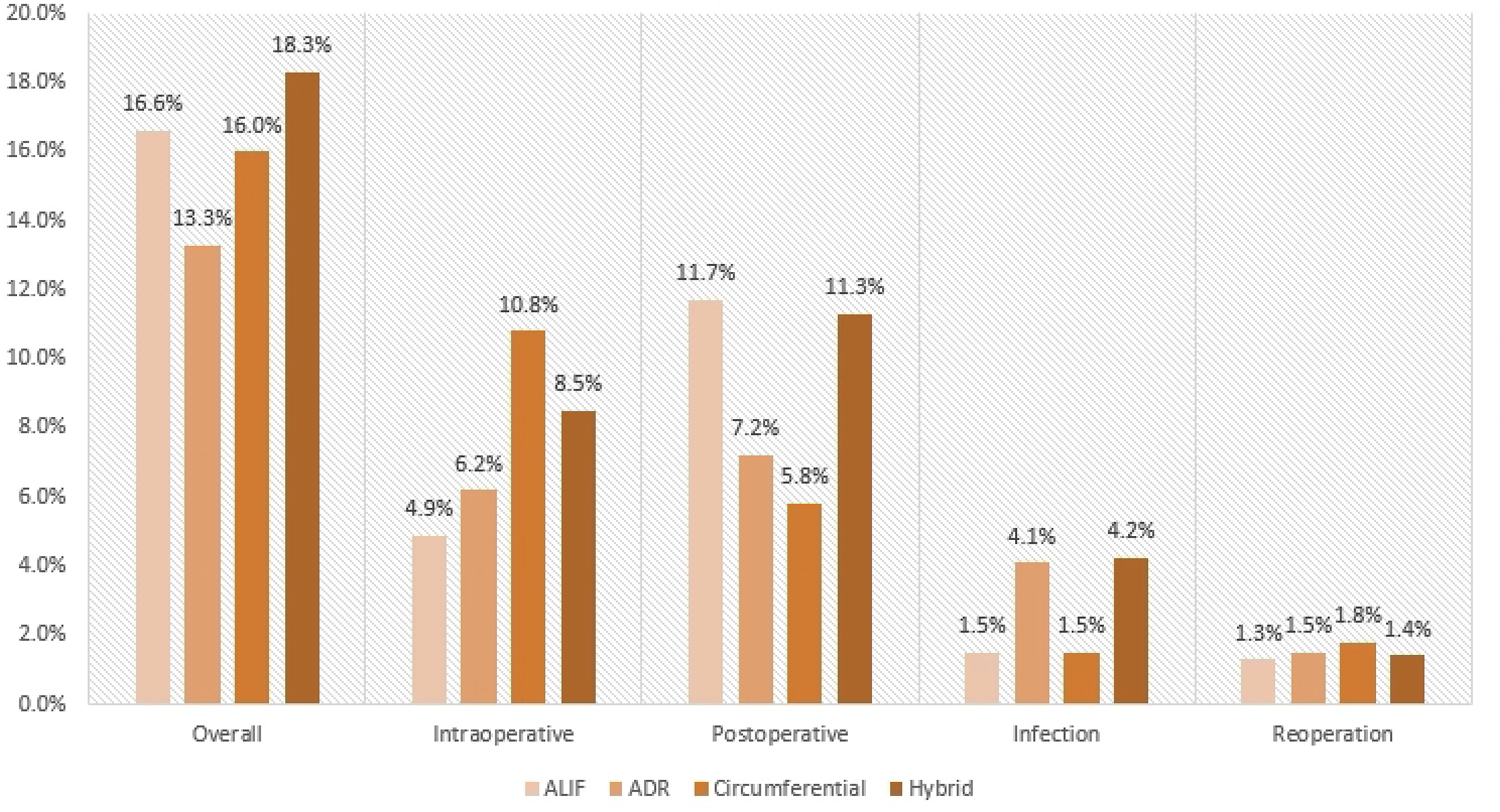
Complication Rate Associated With Adjuvant Measures
Complication Rates by Approach and Use of CTA, rhBMP-2, and Access Surgeon.
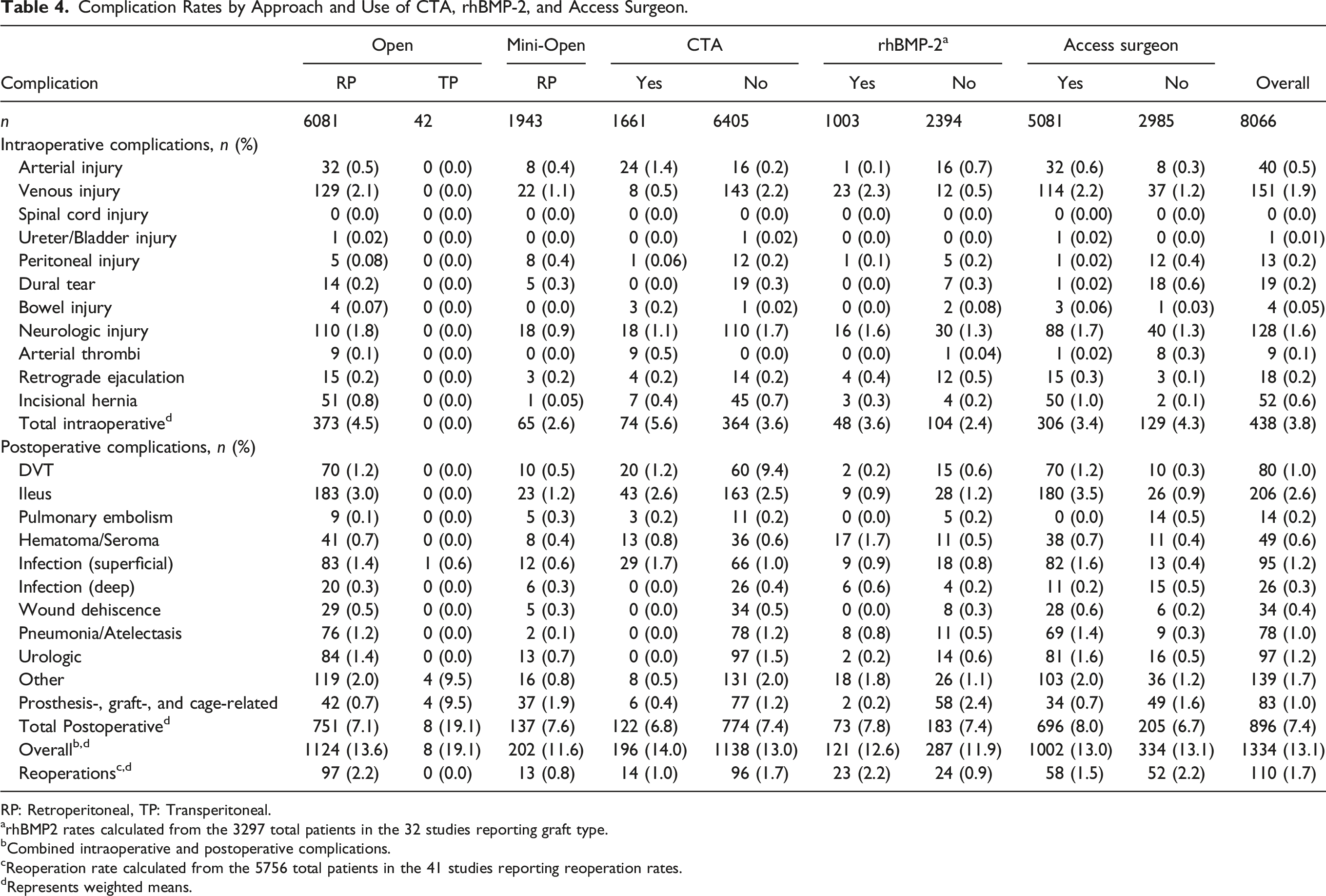
RP: Retroperitoneal, TP: Transperitoneal.
arhBMP2 rates calculated from the 3297 total patients in the 32 studies reporting graft type.
bCombined intraoperative and postoperative complications.
cReoperation rate calculated from the 5756 total patients in the 41 studies reporting reoperation rates.
dRepresents weighted means.
The number of overall complications (14.0% vs 13.0%) and intraoperative complications (5.6% vs 3.6%) was higher with the use of pre-operative CTA. Generalized mixed models showed that the use of pre-operative CTA conferred a significant increase in overall complications (OR: 2.69, CI: 1.60, 4.52, P < 0.05) and intraoperative complications (OR: 4.55, CI: 2.25, 9.19, P < 0.05), but no difference in postoperative complications (P > 0.05). Using an access surgeon did not affect the overall incidence of intraoperative complications (OR: 0.56, CI: 0.27, 1.13, P > 0.05) or postoperative complications (OR: 1.09, CI: 0.55, 2.19, P > 0.05) in aggregate, however it decreased the rate of reoperations (OR: 0.32; CI: 0.11, 0.89; P < 0.05). Similarly, neurologic injury (OR: 0.32, CI: 0.28, 1.19, P > 0.05) was not significantly associated with access surgeon subspeciality. Use of rhBMP-2 was not associated with postoperative complications (OR: 0.88; CI: 0.39, 1.98; P > 0.05) (Figure 4). Forest plots by approach, CTA, rhBMP-2, and access surgeon.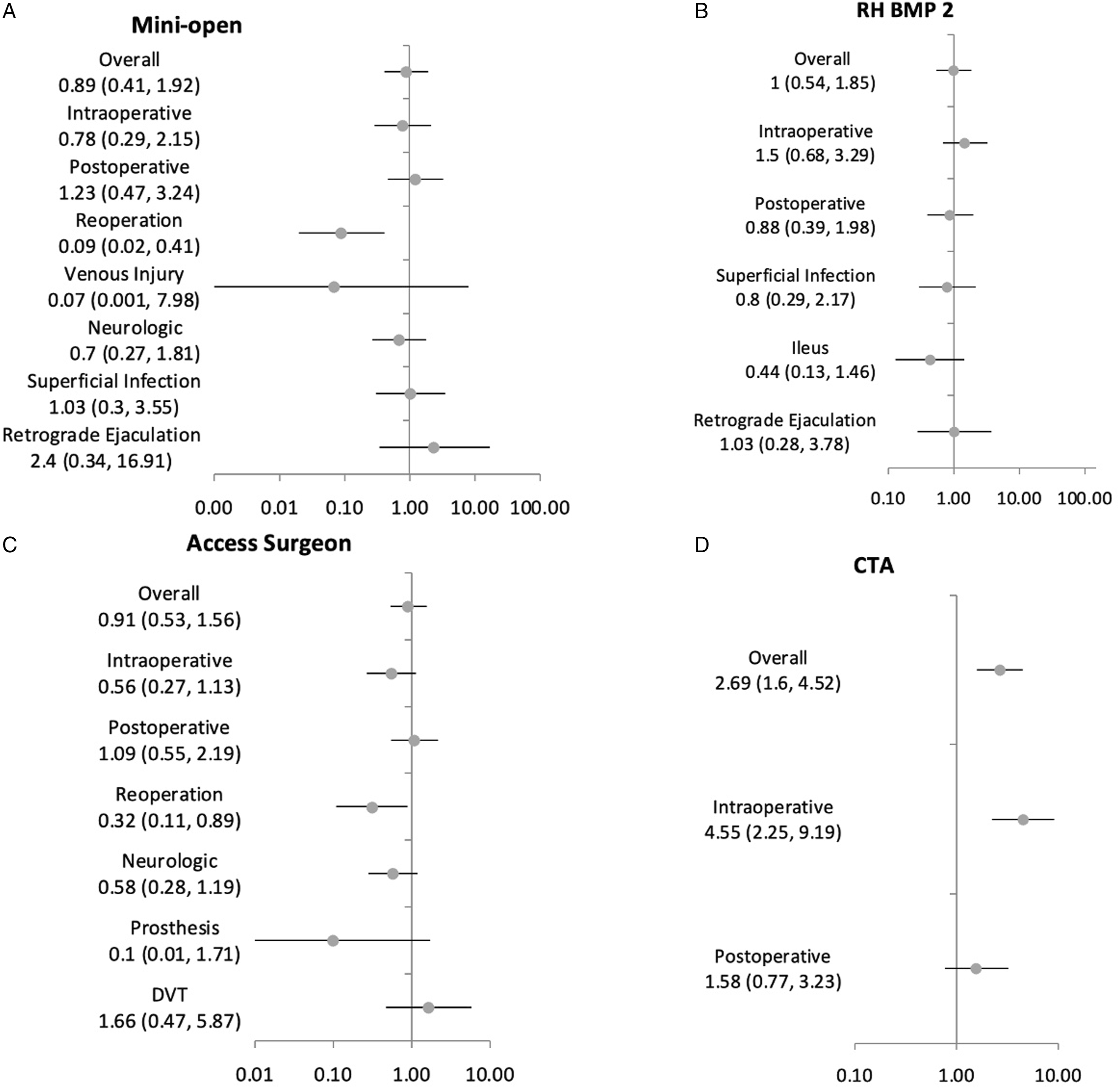
Discussion
Anterior lumbar surgical techniques are superior to posterior based procedures with regards to reduced rates of neurologic injury, increased disc space distraction with greater potential for sagittal alignment correction, and minimal disruption of paraspinal musculature.54,57,58 Recent advancements in spinal implants/instrumentation and increasing expertise in minimally invasive techniques have created a renewed interest in anterior procedures and have contributed to reduced morbidity in spinal surgery.59,60 The current study aimed to analyze the overall complication rate associated with anterior lumbar surgery, as well as examine complication rates by open vs minimally invasive approaches, procedure type, and use of other measures (ie, pre-operative CTA, rhBMP-2, and access surgeon). Previously, Bateman et al. 12 reported a mean complication rate of 14.1% using an anterior lumbar approach among studies between 1992 and 2013, with venous injury, retrograde ejaculation, and neurologic injury being the most common complications. The present study reports a decreased overall complication rate of 13.4%, with venous injury, ileus, and neurologic complications being the most common complications by incidence rate. Our analysis did not include studies in which laparoscopic anterior lumbar surgery was performed, as was the case in the previous Bateman study, a finding which accurately reflects the trend of decreased use of the laparoscopic technique. Encouragingly, given the advancements in surgical techniques and technologies and increasing surgeon familiarity and training with anterior lumbar surgery, the overall complication rates have decreased over time.
Minimally invasive techniques have continued to garner popularity with studies showing comparable surgical outcomes to open procedures with reduced associated morbidities.59,61 The mini-laparotomy also known as the mini-open approach was first described by Mayer in 1997 as a retroperitoneal approach for L2-3 to L4-5 and a transperitoneal approach to L5-S1.1,4,29,33,35,62-64 The present study suggests that patients with mini-open procedures experience significantly lower rates of reoperations compared to open procedures, and they do not have increased risk of intraoperative complications. Utilizing a mini-open procedure allows surgeons to obtain direct visualization of the anatomy, while likely minimizing disruption of surrounding visceral structures. 65 Furthermore, the reduced exposure of soft tissue and bony elements decreases the surface area for contact by potential pathogens. 66 One major limitation involving minimally invasive surgery is the learning curve associated with these procedures. However, increased utilization and training in minimally invasive approaches throughout surgical training may have lowered the risk of intraoperative complications previously attributed to mini-open approaches.67-69
Prior studies appropriately attributed an increased risk of retrograde ejaculation and postoperative ileus in patients who underwent a transperitoneal approach, due to proximity of the hypogastric plexus to the iliac vein wherein injury may occur during vessel traction or peritoneal dissection.58,70,71 However, recent literature suggests anterior lumbar surgery through a transperitoneal approach does not increase the risk of post-operative ileus and retrograde ejaculation. 12 These findings can be explained by the relatively simpler plane of dissection in the retroperitoneal approach combined with decreased direct manipulation of abdominal contents, limiting disruption of small/large bowel contexts and the hypogastric nerve plexus.55,72,73
Notably, our analysis found a reduction in prosthetic/graft/cage-related complications compared to the prior systematic review by Bateman and colleagues (1.2% vs 1.97%). This is likely reflective of our increased understanding in biomaterials and construction of implants that facilitate bony fusion. While titanium implants were among the first interbody devices to be used because of their optimal fusion rates, high subsidence rates led to the development of PEEK implants. Unsurprisingly, the lower subsidence rates of PEEK implants were met with lower fusion rates.74,75 We theorize that several newer generation devices, including titanium coated PEEK interbody devices and three-dimensional printed cages, are offering superior clinical outcomes and may lead to the lower complication rate although this needs further analysis. 76 Furthermore, while anterior plating was initially thought to increase stabilization providing biomechanical superiority, 77 they have not been shown to significantly improve clinical outcomes compared to standalone fusion procedures. 78 Moreover, standalone ALIFs and those with minimally invasive posterior percutaneous screw fixation are increasingly performed to minimize surgical morbidity which may contribute to the lower risk of complications. As a result of these demonstrated benefits, stand-alone ALIF procedures have become increasingly more popular, reducing overall implant-related complications by reducing the per patient implant burden.
A variety of resources can be utilized to limit complications associated with anterior lumbar procedures. CTA is a highly utilized imaging modality to help assess vascular disease and visualize blood flow. 79 For spine surgeons, particularly those performing minimally invasive procedures, preoperative CTA imaging may help evaluate anatomic relationships of the iliac veins and aortic bifurcation with careful attention to possible anatomic variations that need to be considered intraoperatively. Notably, the current study showed significantly increased odds of overall complications and intraoperative complications when CTA was performed. This finding is surprising given that preoperative CTA imaging is typically expected to assist in navigating the surgical field. One possible explanation for this observation is that CTA may have been selectively used in patients who were expected to have more challenging vascular anatomy.13,79,80 These patients may have been at an inherently increased risk of arterial or venous injury, potentially skewing the reported complication rates. Bateman et al. 12 also found a moderate increase in postoperative complications when preoperative CTA was employed, though there was no difference in intraoperative or overall complications. These findings raise important questions regarding the utility of preoperative CTA, particularly when exposure to radiation is considered. 13 Nevertheless, its utility in high-risk patients, as well as during the early learning process of minimally invasive procedures, is something that should continue to be explored.81,82
Dedicated access surgeons provide a unique resource and multidisciplinary approach to spine surgery. A recent meta-analysis by Phan et al evaluating the use of access surgeons in patients undergoing ALIF procedures found decreased odds of postoperative complications, neurologic complications, and reoperations. 83 Access surgeons, commonly vascular surgeons, have an extensive training in vascular anatomy and may be able to identify complex vascular anatomy more readily. 84 Moreover, careful dissection should be performed when attempting an anterior approach to the L5-S1 disc which generally lies between the bifurcation of the great vessels, but close to the commonly injured left common iliac vein. 85 Despite the expected advantage associated with use of an access surgeon, we identified a higher risk of venous injury when the anterior approach was performed by an access surgeon. These findings are similar to previous studies, which have shown higher rates of venous injuries with the use of access surgeons.15,83,86,87 While this finding seemingly contradicts the stated benefit of an access surgeon for anterior lumbar procedures, as was the case with preoperative CTA imaging, this assessment neglects to account for the fact that access surgeons are more commonly employed for patients whose vascular anatomy is expected to be more complex. Additional studies are needed to characterize the benefit of using an access surgeon in patients with similarly intricate vascularity.
Debate continues on the use of access surgeons, but a recent international Delphi study achieved consensus that spine surgeons can safely perform a lateral ALIF without an access surgeon for routine cases. 88 Moreover, our updated meta-analysis suggests that the overall rate of intraoperative complications when performed without an access surgeon are lower than previous reports of earlier literature, 12 likely representing significantly enhanced training for spine surgeons. However, the utilization of access surgeons may still be warranted in cases with complex anatomical considerations, significant history of prior abdominal surgery, or relatively less experience.
Finally, rhBMP-2 is a bone graft that was approved in 2002 by the United States Food and Drug Administration (FDA) for single-level ALIF procedures to enhance bony fusion. 89 Despite its association with superior fusion rates, a variety of studies have reported its association with retrograde ejaculation and increased infection rates.90,91 The present study reports no increased risk of retrograde ejaculation, infection rates, or overall complication rates with use of rhBMP-2. In contrast to our findings, a meta-analysis by Vavken et al. 92 suggests rhBMP-2 use is associated with significantly higher odds of retrograde ejaculation and heterotopic ossification. However the limited incidence of surgical site infection in our cohort may make differences difficult to delineate.
The present study does come with limitations. First, pooling of outcomes can result in significant heterogeneity with an increased risk of Type I errors. Additionally, combining data between patients with varying perioperative protocols could be a significant source of confounding. Furthermore, statistical analyses controlling for pertinent factors, such as prior lumbar surgery and levels operated were unable to be conducted in the present study. The grouping of patient complications into broad categories (ie, intraoperative, postoperative), while supported by prior studies, 12 can result in increased risk of bias, as well as limit the ability of the data to be generalizable. Second, while every effort was made to identify studies satisfying the inclusion and exclusion criteria, selection bias may have been introduced by missing potential studies. A third limitation is the inclusion of all studies that fulfilled our study criteria, regardless of the score it received using the two quality scales we implemented. These lower quality studies may lessen the accuracy and strength of our conclusions and affect the heterogeneity of the include data. Additionally, the varying sample sizes of included studies can skew data towards complication rates reflective of studies with larger sample sizes. A fourth limitation is that there was an unequal distribution of procedures performed, with ALIF procedures having the highest prevalence. This limits our ability to comprehensively determine which approach has higher rates of complications. Additionally, given the retrospective nature of this study, it is impossible to know how accurately the details regarding adjuvant resources (use of CTA, access surgeon, BMP2 use) were recorded in each included study. Inconsistencies in reporting of these details may have affected the accuracy of those sub-analyses. Finally, certain complications considered as not occurring within our analysis may have not been considered in an included study, thus underestimating certain complication rates.
Overall, anterior lumbar surgery has undergone considerable advancements over the past decade with the recent introduction of minimally invasive techniques to help reduce morbidity. Anterior lumbar approaches have shown to better facilitate access to the central spinal column/disc spaces; however, this is at the risk of injury to major midline vascular, neural, and visceral structures. While higher quality studies are still warranted to elucidate the true effect of measures, such as preoperative CTA imaging, rhBMP-2, and access surgeons, our results help set a framework of the overall complication profile reported in recent literature.
Footnotes
Author’s Note
All authors significantly contributed to the document and have reviewed the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.