
Abstract
Study Design:
Retrospective cohort study.
Objective:
The objective of the study was to determine rates of medical and surgical postoperative complications following anterior lumbar interbody fusion (ALIF) along with their associated predictors.
Methods:
Using the American College of Surgeons National Surgical Quality Improvement database, patients who underwent single-level ALIF surgery from 2006 to 2013 were identified. The 30-day rate of postoperative medical and surgical complications along with associated risk factors were evaluated by multivariable logistic regression.
Results:
In total, 1474 patients were included in the analysis. The overall rate of complications was 14.5%. The medical complication rate was 12.7%, while the surgical complication rate was 2.8%. Predictors of surgical complications were diabetes (odds ratio [OR] = 2.79, 95% CI = 1.20-6.01, P = .009), corticosteroid dependence (OR = 4.94, 95% CI = 1.73-14.08, P = .003), and preoperative transfusion of >4 units (OR = 7.12, 95% CI = 1.43-35.37, P = .016). Predictors of medical complications were longer operative times (OR = 4.25, 95% CI = 2.90-6.24, P < .001), preoperative anemia (OR = 2.29, 95% CI = 1.50-3.50, P < .001), >10% weight loss prior to surgery (OR = 6.79, 95% CI = 1.01-45.93, P = .049), and more severe American Society of Anesthesiologists classification (OR = 2.18, 95% CI = 1.54-3.11, P < .001).
Conclusions:
The present study determines postoperative medical and surgical complications among patients undergoing ALIF. The risk factors elucidated in this study indicate that clinical practices to curtail complications should be targeted toward patients with preoperative anemia, weight loss, corticosteroid dependence, and toward those at risk for perioperative transfusions.
Introduction
The importance of postoperative complications as a significant contributor to the increasing cost of health care in the United States is difficult to understate given that complications are the strongest indicator of full in-hospital costs per patient. 1 Preventing postoperative complications will not only improve quality of patient care, but is now fiscally incentivized by the provisions of the Affordable Care Act, which sanctions penalties toward hospitals that fail to achieve standards for hospital readmissions. 2 Complications within 30 days following spine surgery occur in about 7.6% of cases. 3 Risks for postoperative complications after spine surgery include older patient age, congestive heart failure and/or history of heart attack, preoperative neurological problems, history of spinal wound infection, corticosteroid use, history of sepsis, classification of 3 or higher according to the American Society of Anesthesiologists (ASA) physical status classification, and lengthened surgery times. 3
There are multiple approaches for lumbar fusion. Among these approaches, anterior lumbar interbody fusion (ALIF) carries a unique and complication profile compared to other lumbar fixation techniques. The unique morbidity profile reflects risks inherent to anterior retroperitoneal access that involves greater exposure of vasculature, visceral organs, the genitourinary system, and soft tissue. ALIF can be utilized to treat a wide variety of indications for degenerative pathologies of the lumbar spine. These pathologies may include spondylolisthesis, degenerative disc disease, degenerative lumbar scoliosis, pseudoarthrosis, adjacent segment disease, and other indications that may result in instability of the lumbar spine and chronic lower back pain. 4 The literature cites numerous advantages to an anterior approach over a posterior approach in interbody fusion surgery including improved access to the anterior column, which allows for complete discectomy and increased ability to place a large interbody fusion device. Taken together, these benefits have been shown to contribute to higher fusion rates and improved clinical outcomes. 4 There have been very few significant multicenter studies evaluating short-term postoperative complications following ALIF procedures.
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) is a continuing effort to produce a prospective multicenter registry tracking relevant outcomes of patients undergoing surgical procedures. Given the unique safety profile associated with anterior access, the present study aims to establish rates of surgical and medical complications following single-level ALIF and identify key predictors of medical and surgical complications utilizing the large, multicenter, and validated NSQIP database.
Methods
Patient Data
Patient data was obtained from the ACS-NSQIP database from 2006 to 2013. This nationwide database collects more than 300 variables on patient characteristics, comorbidities, perioperative features, and 30-day postoperative complications and mortality of patients undergoing surgical procedures across a wide range of participating hospitals. Surgical procedures are captured by Current Procedural Terminology (CPT) codes, and specific diagnoses can be identified by International Classification of Diseases, Ninth Edition (ICD-9) codes. The ASC-NSQIP website (http://www.ascnsqip.org) summarizes the sampling process and patient and hospital inclusion and exclusion criteria. The most recent interrater reliability audit, as a metric of data quality, identified an overall disagreement rate of 2% for listed variables. Institutional review board approval was not needed for this study.
All patients undergoing single-level ALIF were identified. The CPT code 22558, interbody fusion utilizing the anterior technique, in a single lumbar level, was used to identify all cases of ALIF. Patients with CPT code 22585, signifying additional levels, was used to exclude cases in which multilevel surgery was performed. Additionally, only patients undergoing ALIF with concurrent CPT code 22851, signifying intervertebral cage technique, were included. This comprised the majority (over 70%) of single-level ALIF cases. Those with autograft and allograft were excluded. Patients with concurrent posterior or transforaminal lumbar interbody fusion were excluded utilizing the CPT codes 22612, 22630, 22633.
Variables
The outcomes variables were surgical and medical complications occurring within the recorded 30-day postoperative period. Surgical complication comprised occurrence of at least one of the following variables: superficial surgical site infection (SSI), deep incision SSI, organ space SSI, or wound disruption. Similarly, occurrence of postoperative medical complications comprised occurrence of at least one of the following: pneumonia, unplanned intubation, ventilator dependence >48 hours, worsening renal insufficiency, acute renal failure, urinary tract infection, stroke, myocardial infarction, sepsis, or septic shock. Given the unique exposure of vasculature associated with anterior access, transfusions of red blood cells up to 72 hours postoperatively was included as a medical complication to create a more complete composite variable that would more comprehensively reflect postoperative adverse effects. Continuous values were binned into binary variables. Diabetes was defined by diabetes reliant on either oral medication or insulin. Increased operative time was defined by operative time greater than the 75th percentile (247 minutes) of all cases. Anemia was defined by preoperative hematocrit <39 in males and <36 in females. 5 Body mass index (BMI) was calculated by the World Health Organization obesity classification and was defined by weight × 703/(height) 2 and then classified as normal (18.5 ≤ BMI < 25), underweight (BMI< 18.5), and overweight (BMI ≥ 25). Older age was defined by age >75 years. Dyspnea includes both dyspnea with moderate exertion or at rest. Severe ASA physical status classification was defined by ASA class 3 or greater. A wound was defined by clean/contaminated, contaminated, or dirty wound classification. All postoperative complications occurred within 30 days of indexed operation.
Statistical Analysis
SPSS (version 20, IBM Corp, New York, NY) was utilized for all statistical analysis. Variables were created or recategorized as described above. Differences in patient features and preoperative comorbidities were analyzed with either Fisher’s exact test or Pearson’s χ2 test. To identify putative predictor variables for logistic regression, variables were first screened on univariate analysis based on either occurrence of medical or surgical complication. Variables with P < .10, along with variables of clinical interest, were subsequently included in 2 separate multivariable logistic regressions to identify predictors of surgical and medical complications. Variables were entered with a stepwise backward likelihood method. Odds ratios (ORs) are shown with 95% confidence intervals (CIs). All tests were 2 tailed with significance at P > .05. C statistic was calculated based on area under the receiver operative characteristic curve.
Results
Patient Demographics
A total of 1474 patients undergoing single-level ALIF utilizing intervertebral cage met study criteria and were included in study analysis. Of all patients, average age was 53.85 ± 13.6 years, with 55.0% females and 45.0% males. Overall rate of surgical and medical complications was 14.5% (n = 214). Rate of medical complications was 12.7% (n = 187), and rate of surgical complications was 2.8% (n = 41), P = .001. Incidences of specific surgical and medical complications are summarized in Tables 1 and 2.The most common surgical complications were SSI, while the most common medical complication was blood transfusion, urinary tract infection, thromboembolic events, and pneumonia. Indications for ALIF are summarized in Table 3.
Summary of Surgical Complications.
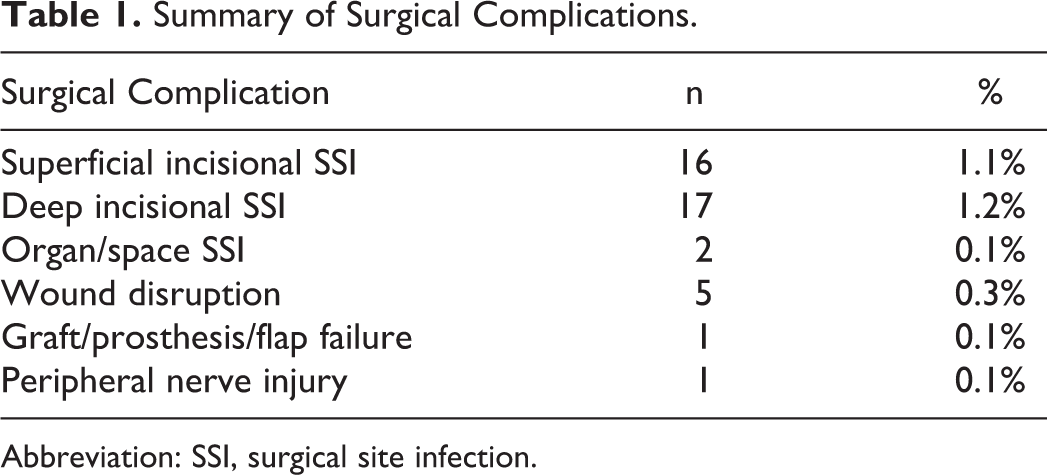
Abbreviation: SSI, surgical site infection.
Summary of Medical Complications.
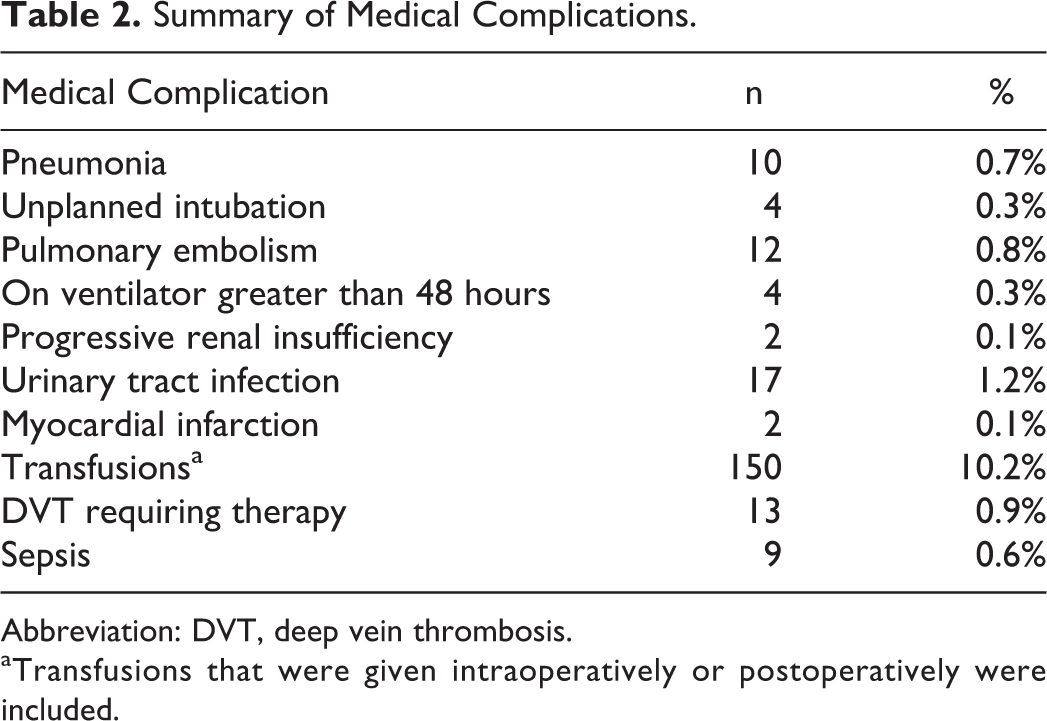
Abbreviation: DVT, deep vein thrombosis.
aTransfusions that were given intraoperatively or postoperatively were included.
Summary of Most Frequent Indications for Surgery by ICD-9 Code.
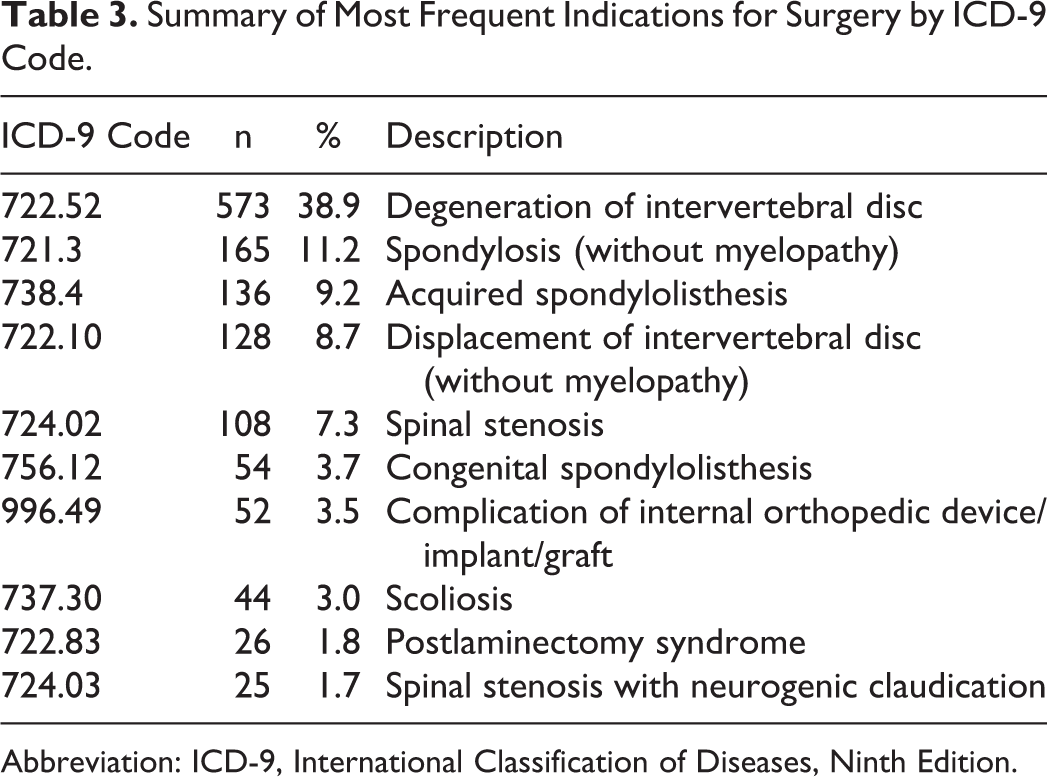
Abbreviation: ICD-9, International Classification of Diseases, Ninth Edition.
Surgical complications were more likely to occur in patients requiring medications for diabetes (24.4% vs 10.3%, P = .009), those who depend on corticosteroids for chronic medical conditions (13.5% vs 2.2%, P = .015), and those requiring greater than 4 units of red blood cells transfused preoperatively (4.9% vs 0.7%, P = .042; Table 4). Similarly, patients who experienced postoperative medical complications were characterized by a greater number of preoperative comorbidities, including a greater incidence of anemia (26.6% vs 11.7%, P < .001), hypertension requiring medications (52.4% vs 40.6%, P = .003), corticosteroids for chronic medical conditions (5.9% vs 2.0%, P = .004), >10% weight loss (1.6% vs 0.2%, P = .030), requiring preoperative blood transfusions (3.2% vs 0.5%, P = .002), and sepsis (3.7% vs 0.5% P < .001; Table 5). Moreover, medical complications was associated with surgeries requiring significantly longer operation times (244.47 vs 152.17 minutes, P < .001), and in patients with ASA classification 3 or greater (57.2% vs 32.9, P < .001). Of note, differences in BMI categorization were not significantly different between those with and without medical or surgical complications.
Summary of Patient and Operative Risk Factors Based on Postoperative Surgical Complications.
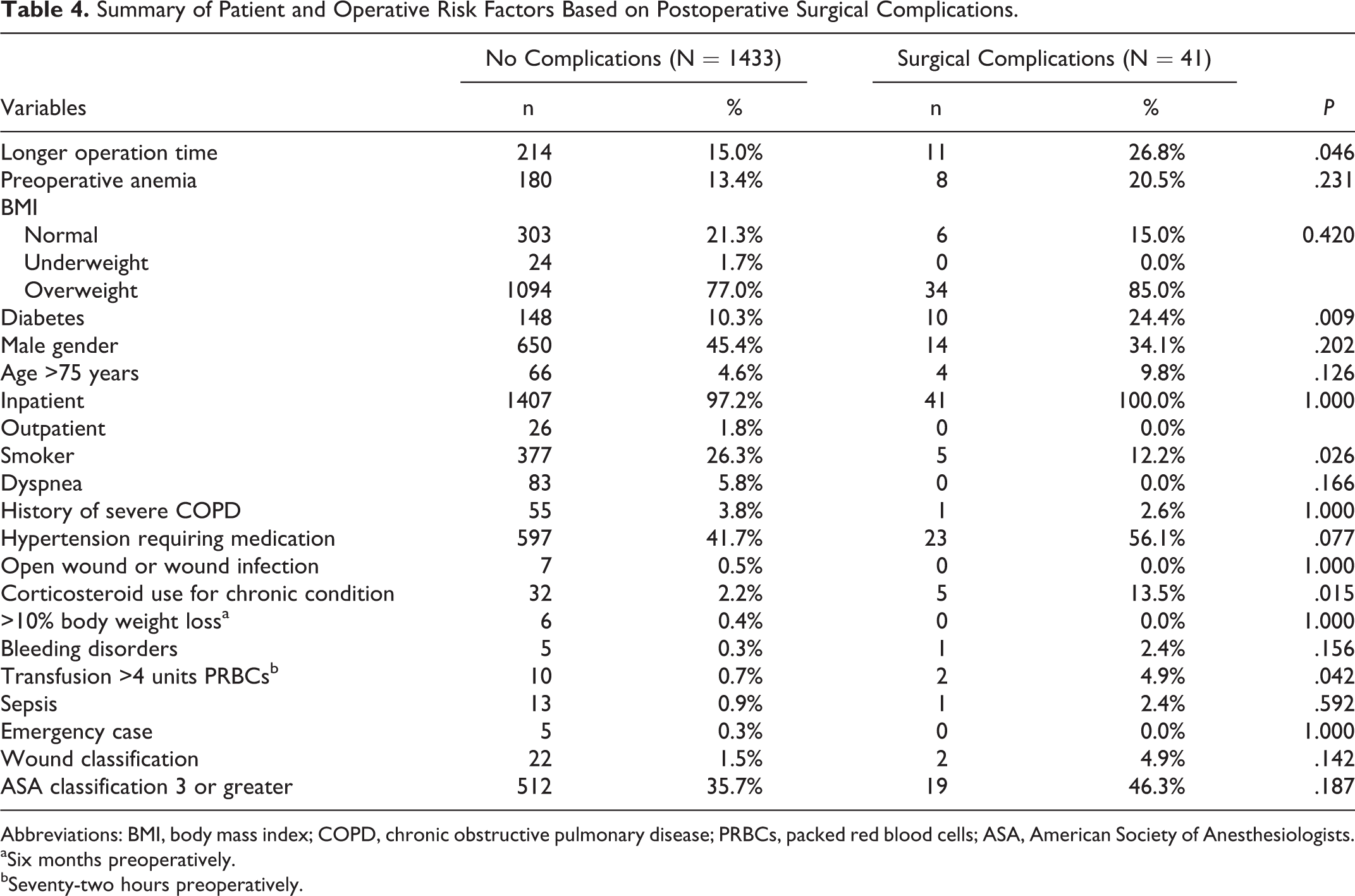
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; PRBCs, packed red blood cells; ASA, American Society of Anesthesiologists.
aSix months preoperatively.
bSeventy-two hours preoperatively.
Summary of Patient and Operative Risk Factors Based on Postoperative Medical Complications.
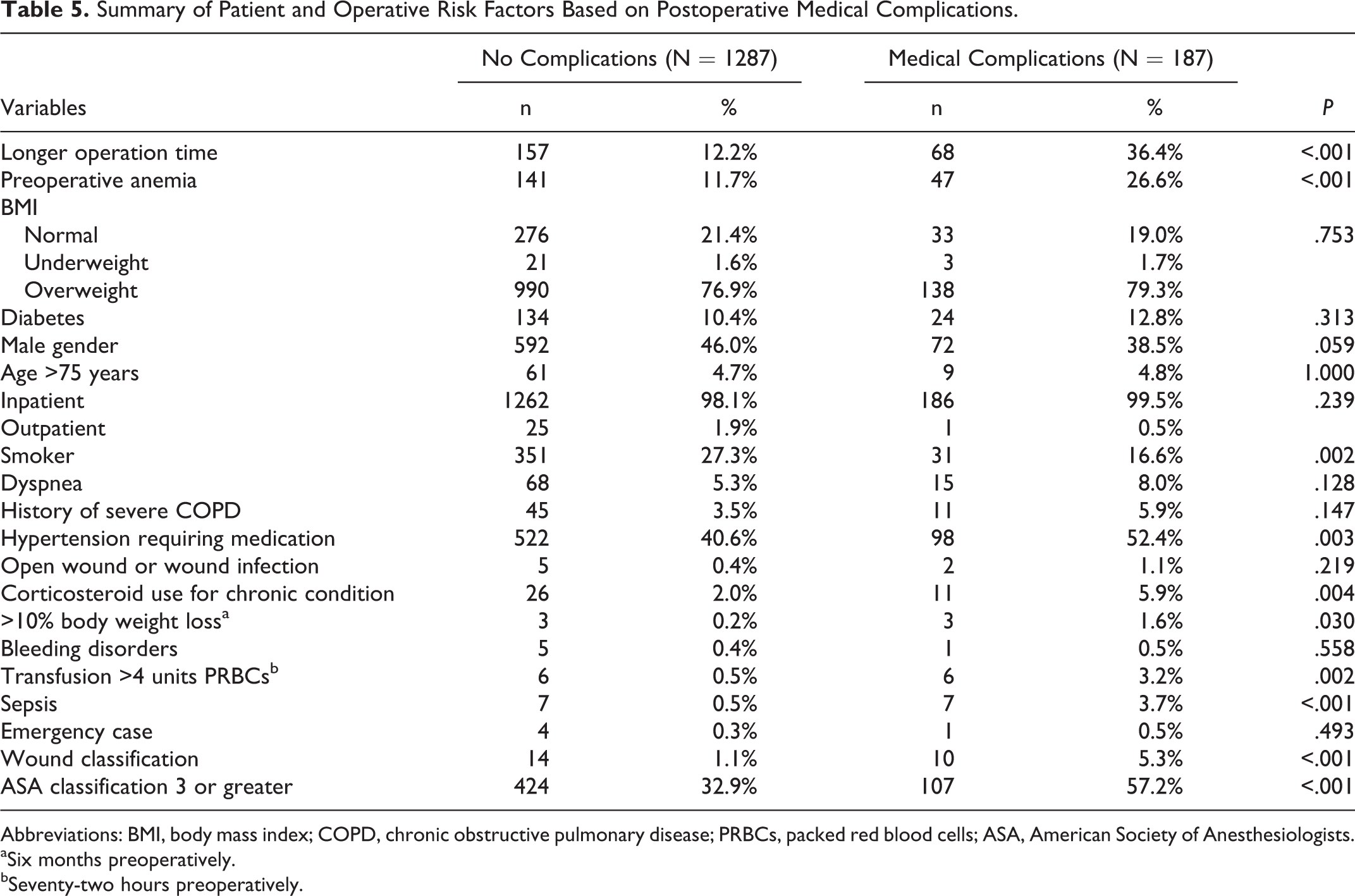
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; PRBCs, packed red blood cells; ASA, American Society of Anesthesiologists.
aSix months preoperatively.
bSeventy-two hours preoperatively.
Surgical Complications
To identify significant predictors of postoperative complications, 2 separate multivariable logistic regression analyses were utilized for surgical and medical complications following initial univariate screening (Tables 6 and 7). On multivariable analysis of surgical complications, diabetes (OR = 2.79, 95% CI = 1.20-6.01, P = .009), corticosteroid dependence (OR = 4.94, 95% CI = 1.73-14.08, P = .003), preoperative transfusion of >4 units (OR = 7.12, 95% CI = 1.43-35.37, P = .016) were significant predictors of surgical complications. C-index was 0.597 for this model.
Predictors of Surgical Complications From Multivariable Logistic Regression Analysis.
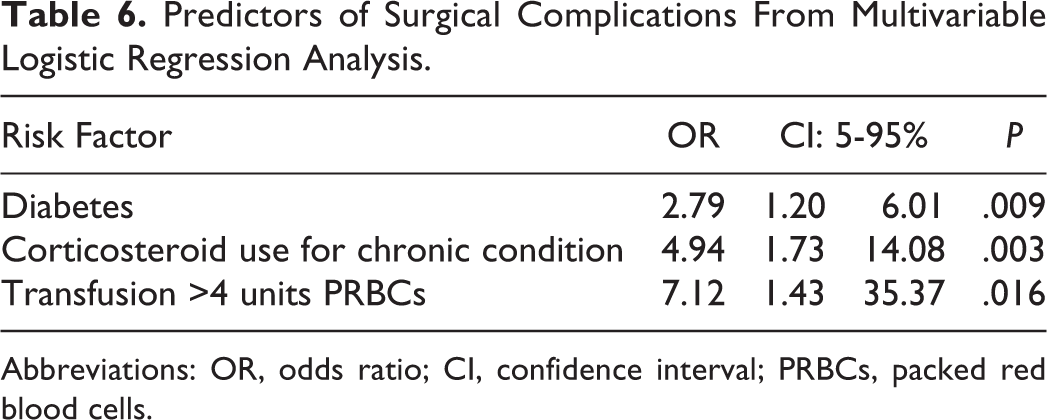
Abbreviations: OR, odds ratio; CI, confidence interval; PRBCs, packed red blood cells.
Predictors of Surgical Complications From Multivariable Logistic Regression Analysis.
Abbreviations: OR, odds ratio; ASA, American Society of Anesthesiologists.
aSix months preoperatively.
Medical Complications
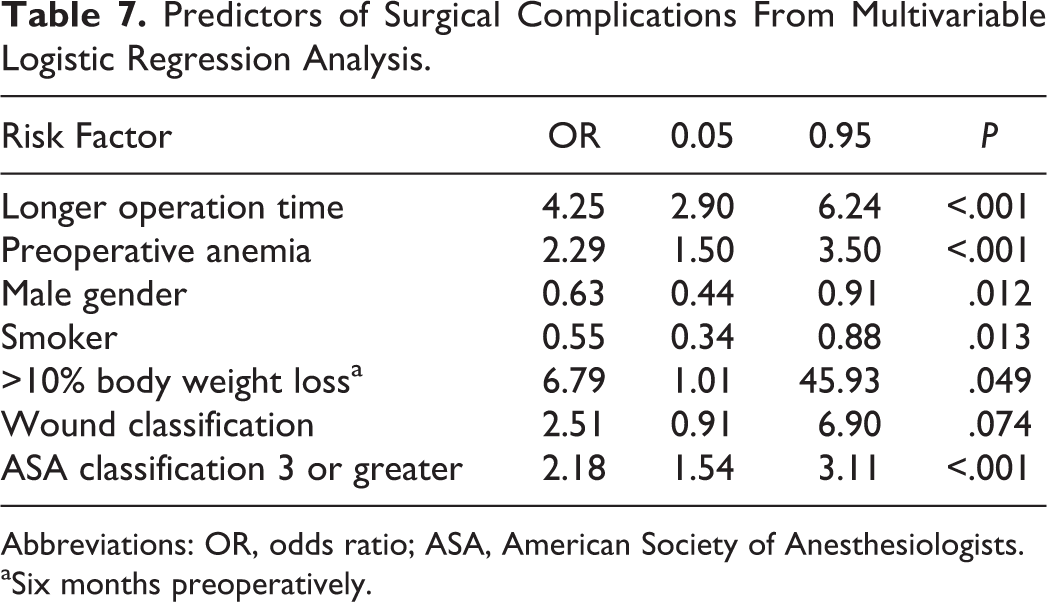
On multivariable analysis, longer operative times (OR = 4.25, 95% CI = 2.90-6.24, P < .001), preoperative anemia (OR = 2.29, 95% CI = 1.50-3.50, P < .001), >10% weight loss prior to surgery (OR = 6.79, 95% CI = 1.01-45.93, P = .049), and more severe ASA classification (OR = 2.18, 95% CI = 1.54-3.11, P < .001) were predictive of postoperative medical complications. C-index was 0.737 for the regression model.
Discussion
While there are numerous approaches for lumbar fixation, ALIF carries a unique complication profile reflecting challenges unique to anterior access. Although advances in microsurgical technique and improved instrumentation have paved the way for decreased perioperative complications, 6 –8 resulting morbidity carries a significant cost to both patients and health care systems. Thus, we elaborate on the safety profile of single-level ALIF and identify key risk factors that drive complications through the largest study of this kind to date.
Overall postoperative morbidity rates in the present study were 14.5%, and medical complications were the dominant cause for postoperative morbidity. Rates of complications associated with anterior approaches to the spine have been highly variable. Donnell et al reported 11% and 24% of patients experiencing major and minor complications, respectively, in a large study of 447 patients. 9 Other studies have cited postoperative complication rates of up to 40% in spinal surgeries utilizing an anterior approach. 10,11 As with spinal surgeries involving other approaches, ALIF carries surgical risks of SSIs and wound dehiscence. However, as compared to other approaches such as posterior lumbar interbody fusion (PLIF) where issues of wound infections, dehiscence, and pain dominate, the high rate of medical complications in ALIF likely reflects risks intrinsic to exposure of visceral and genitourinary structures, and mobilization of abdominal vasculature resulting in ileus or neurovascular complications that include bleeding and thrombotic events.
Rate of medical complications in our series was 12.7%, and was predicted by more severe ASA classification and the modifiable risk factors of preoperative anemia and weight loss prior to surgery. The most common medical complications were transfusion requirements, thromboembolic events and urinary tract infections. However, other complications such as genitourinary injury were not captured by NSQIP. Damage to the superior hypogastric plexus may result in retrograde ejaculation (RE) in males, with incidence of up to 45% in literature. 12 Thus, differences in complication endpoints collected in the present study may account for discrepancy in complication rates reported in literature. Importantly, postoperative ileus, not captured in NSQIP, may be a key driver for other medical complications such as thromboembolic events due to delayed ambulation. The highly variable range of reported complications in literature also likely stems from a large heterogeneity in surgeries included. While the present study specifically looks at single-level ALIF with anterior instrumentation, there are key variables not included by the NSQIP database that likely influences the risk profile of patients, such as the type and segmental level of ALIF performed.
Importantly, our study highlights the high frequency of transfusion requirement from the start of the surgery up to 72 hours postoperatively. As compared to other approaches such as PLIF that avoids exposure and mobilization of abdominal vessels, ALIF is associated with increased perioperative transfusions. A large study of 84 650 patients undergoing elective lumbar spine surgery found that perioperative allogenic blood transfusion was associated with increased risks of SSI. 13 Aside from the independent risk that transfusion may represent, it is also possible that transfusion may be acting as a proxy for preoperative anemia that is not sufficiently corrected in our study. Moreover, a recent large single-center study of 1187 spinal surgeries demonstrated a mean 60% increase in hospital stays in patients receiving transfusions. 14 The authors noted the effective use of perioperative surgical homes that coordinate care from the preoperative through the postdischarge period aimed at the optimization of high-risk patients to minimize transfusion requirements in surgical patients.
Anemia has been linked to increased risk for postoperative morbidity and mortality across a number of surgical specialties. 15 –18 In one of the largest studies to date, Musallam et al reviewed the postoperative outcomes of 227 425 patients undergoing noncardiac surgery. 19 Both mild anemia, defined by hematocrit >29 and <36 in females and hematocrit >29 and <39 in males (OR = 1.31), and severe anemia (OR = 1.56) were associated with significant increases in 30-day complications. Moreover, anemia has been associated with increased rates of hospital readmission following a variety of surgeries including spine surgery for lumbar decompression (OR = 1.48) in a study of 7016 patients 20 and plastic surgery (OR = 1.8) in a study of 10 669 patients. 21 Thus, early detection and correction of preoperative anemia, even in mild cases, can reduce incidence of medical complications in patients undergoing ALIF.
Preoperative weight loss, a proxy for medical deconditioning and poor nutritional status, was associated with increased medical complications. In an analysis of 13 660 patients undergoing spinal surgery, preoperative weight loss predicted increased rates of postoperative stroke (OR = 59.42), increased length of stay (OR = 3.06), and more frequent return to the operating room (OR = 3.08). 22 As the majority of cases evaluated were nonemergent, patients should be nutritionally optimized prior to ALIF to minimize all cause postoperative medical morbidity.
In addition to these comorbidities, higher risk surgeries characterized by longer operation times and higher ASA class were significant predictors of medical complications. ASA class has been widely used as a risk stratification system used a single metric to identify those at greater risk for postoperative complications. In patients undergoing ALIF, ASA classification >3 was a key medical complication risk factor. Those with higher ASA classification carry greater comorbidities, and a number of studies have consistently identified ASA class >3 as a risk factor for morbidity, mortality, and hospital readmissions across surgical procedures and specialties. 23 –25 In a review of 24 774 patients from the Veterans Affairs’ NSQIP undergoing spinal decompression and fusion, ASA class 3 (OR = 1.45) and ASA class 4/5 (OR = 1.66) were significantly associated with wound infections. 26 In one of the largest studies to date, Hackett et al, in a study of 2 297 629 patients conducted through NSQIP across a number of surgical specialties, demonstrated increasing risk of medical complications and mortality with each successive ASA class >1. 27
Surgical complications were less frequent, and significant predictors included diabetes mellitus, chronic preoperative steroid use, and blood transfusion. Diabetes has been identified by a systematic review and meta-analysis as an independent risk factor for SSI in a number of surgical procedures including spinal surgeries. 28,29 Though the precise mechanism by which diabetes increases surgical complication risk is not agreed upon, it has been suggested that hyperglycemia during or after surgery may be responsible. 28 However, a number of studies have indicated that diabetes may also act to increase risk for surgical complications through its role in instigating secondary conditions such as vascular changes and white cell dysfunction. 28 Thus, the association may result from poor wound healing via ineffective immune response to foreign pathogens. Optimizing glycemic control in patients with diabetes mellitus is an important point of preoperative intervention in these.
Similarly, Rami et al found that surgical patients with extensive preoperative glucocorticoid use are at higher risk of a variety of complications including both medical complications such as venous thromboembolism and surgical complications such as wound occurrence. 30 In a review of 635 265 patient cases sourced from NSQIP, Ismael et al found that patients undergoing treatment plans involving chronic steroid use were at significantly higher risk for superficial SSI, deep SSIs, organ/space SSIs, and wound dehiscence. 31 This is consistent with the findings of the present study, which included all of these variables in its examination of surgical complications.
The study carries limitations and biases shared by other retrospective analysis of the NSQIP. Variables included in regression models were limited to those collected by the national database. Outcomes that are more granular and specific to ALIF, such as genitourinary complications like RE, neurovascular complications, injury to visceral organs, or subsequent need for abdominal hernia repair following ALIF, are not provided within the NSQIP database. Moreover, other key risk factors such as previous ALIF, prior abdominal surgery, or segmental level of surgery are not included as variables in NSQIP. A large number of variables were excluded due to excessive null entries. Incomplete data entry in patients who were missing complication outcomes was excluded. Despite these limitations, this is the largest study to date elaborating on rates of complications following ALIF and key modifiable preoperative risk factors.
Conclusion
ALIF is associated with a unique complication profile as compared to other approaches that do not require anterior access. The present study establishes rates of surgical and medical complications following single-level ALIF based on large multicenter data. Importantly, the data elaborates on key risk factors to better identify high-risk patients. Overall rate of complications was 14.5%. However, medical complications dominate the complication profile following single-level ALIF. Patients with preoperative anemia, weight loss, corticosteroid dependence, or are at risk for perioperative transfusions may benefit from medical optimization prior to ALIF to minimize postoperative morbidity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.