
Abstract
Study Design
Systematic review.
Objective
To investigate the incidence and risk factors of neurological complications following anterior lumbar interbody fusion (ALIF) for minimizing their occurrence.
Methods
A comprehensive literature search was conducted to identify articles reporting neurological complications following an ALIF. Studies evaluating outcomes following a lateral antepsoas or transpsoas approach, abstracts without full text available, and non-English manuscripts were excluded. For outcome measures, we collected information on the type of neurological complications and their incidence.
Results
A total of 16 articles met the final inclusion criteria. The overall rate of neurological complications following an ALIF ranged from 4.1% to 7.7%, While the rates of nerve root injury/lumbar plexus injury in patients undergoing surgery for degenerative pathology were less than 4%, the rates were notably higher in patients undergoing an ALIF at L5-S1 and those with spinal deformity (up to 38.4%). The risk for retrograde ejaculation (RE, due to sympathetic nerve injury) was 0.1-3.2% with a retroperitoneal approach. Reported risk factors for neurological complications included the subluxation of the superior articular facet and excessive traction by the ALIF interbody for nerve root injury, transperitoneal approach, aggressive traction on the plexus, electrocautery use, and the application of recombinant human bone morphogenetic protein. However, technical pearls to avoid neurological complications remain controversial.
Conclusions
Several neurologic complications have been reported following ALIF procedures across various pathologies. To mitigate the neurological complications following ALIF, careful preoperative surgical planning and meticulous attention to disc space distraction as well as manipulation of critical structures are essential.
Keywords
Introduction
The loss of harmonious lumbar lordosis is associated with lower back pain and sagittal malalignment. Since 50-80% of the total lumbar lordosis is commonly observed at the L4-S1 levels,1,2 surgical treatment in the lower lumbar spine often has the goals of a robust fusion and restoration of lumbar lordosis.3-5 In the setting of lumbar hypolordosis and sagittal imbalance, multi-level posterior column osteotomies or three-column osteotomies (3CO) can be used, yet these strategies are technically demanding and associated with high risk of complications which include significant blood loss and morbidity.6-9 Anterior lumbar interbody fusion (ALIF) has gained popularity as a highly effective alternative approach which can improve lumbar lordosis, provide a large surface area for circumferential fusion and may increase the ability to achieve appropriate sagittal alignment goals in degenerative and deformity spinal pathologies. 10 An ALIF performed with a lordotic interbody cage can achieve target lumbar lordosis with a degree of correction comparable to that of PSO with lower rates of complications.10,11
The utilization of ALIF has increased considerably in the past decade. The annual volume of ALIF procedures increased from 4227 in 2000 to 29 285 in 2019, a nearly 600% increase over this 20-year period. During the same period, the annual volume of posterolateral fusion increased by about 84%, posterior lumbar interbody fusion increased by less than 1% and the annual volume of single and multi-level 3COs decreased as well.12-14
ALIF is associated with several potential perioperative complications including vascular, ureteral, visceral, and neurologic injury.15,16 A systematic review has found neurologic complications following anterior lumbar surgery to be the third most common complication after vascular injury and thrombosis. 17 While multiple studies have reported on the overall incidence of neurologic complications following ALIF, there is a lack of granularity on the different types of nerve injuries following these procedures. Understanding the characteristics and risk factors of neurological complications associated with ALIF is crucial for minimizing their occurrence. The aim of this article is to investigate the incidence and quantify the risk of neurological complications in ALIF through a systematic review of existing literature in order to mitigate preventable complications.
Methods
Selection Criteria and Study Collection
This systematic review was designed in accordance with the standard recommendations of the Primary Reporting Items for Systematic Reviews and Meta-Analyses (PRIMSA) guidelines.18,19 The study protocol for this systematic review was registered on the PROSPERO (International Prospective Register of Systematic Reviews; ID No. 608715). A comprehensive literature search was conducted by 2 independent authors through 2 electronic databases, PubMed and Embase, using a software “Nested Knowledge” in August 2024. The combinations of following keywords were searched using the Boolean operators “AND” and “OR”: (1) Search terms for ALIF: “ALIF” and “Anterior lumbar interbody fusion”. (2) Search terms for Neurological complication: “Neurological complication”, “Neurologic deficit”, and “Nerve injury”. An updated search was conducted before data analyses with the same screening and selection process as the initial search. Inclusion criteria were (1) studies reporting outcomes following ALIF for lumbar surgery or spinal deformity surgery, (2) studies mentioning neurological complications associated with ALIF. Exclusion criteria were: (1) literature evaluating outcomes following lateral approach (lateral lumbar interbody fusion (LLIF) performed via either an antepsoas or transpsoas approach, (2) abstracts without full text available, (3) systematic review, (4) studies based on administrative databases, (5) reports that may involve overlapping patient cohorts from the same institution, and (6) literature not written in English.
Abstracts and full texts of retrieved studies were reviewed independently by 3 authors to identify studies that potentially met the inclusion criteria. Any disagreements on paper eligibility were resolved by consensus among the authors. A data extraction sheet was created, outlining the variables to be collected.
Risk of Bias and Quality of Evidence
Each included study was assessed for risk of bias by 2 authors using the Risk Of Bias In Nonrandomized Studies-of Interventions (ROBINS-I) tool. 20 A visualization tool (Robvis) was used to visualize the risk of bias assessment in this systematic review. 21 The ROBINS-I tool includes 7 domains of bias, including bias due to confounding bias, bias in selection of participants, bias in classification, bias due to deviations from intended interventions, bias due to missing data, bias in measurement of outcomes, and bias in selection of the reported result. Finally, the overall quality of evidence per outcome was assessed using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) method. 22 In cases of discrepancies in RoB assessment results among the reviewers, a discussion between the 2 reviewers was arranged to achieve consensus.
Results
A literature search found a total 550 publications meeting the search criteria. After eliminating duplicates and screening studies, 40 articles were selected for full text review. Of these, 24 were excluded from the analysis because quantitative data of neurological complications were not reported or wrong study design (systematic review and studies based on administrative databases). The remaining 16 publications met the inclusion criteria in the review (Figure 1). We identified 14 retrospective studies,23-36 1 prospective study,
37
and 1 case series.
38
A total of 3795 patients were included in our analysis excluding those reported in review articles. The mean age of patients included in the studies ranged between 43.8 and 66.1 years. The primary diagnosis for the studies included degenerative disc disease (DDD), spondylolisthesis, adult spinal deformity (ASD) and pseudoarthrosis. The levels at which ALIFs were performed varied across studies: 1 study focused on ALIF at T12-S1, 2 studies at L2-S1, 5 studies at L3-S1, 1 study at L4-S1, and 3 studies at L5-S1, while other studies did not specify the levels involved. PRISMA chart for neurological complications following ALIF. This chart outlines the study selection process for the systematic review. It details the number of studies identified, screened, assessed for eligibility, and included in the final analysis, highlighting reasons for exclusions at each stage.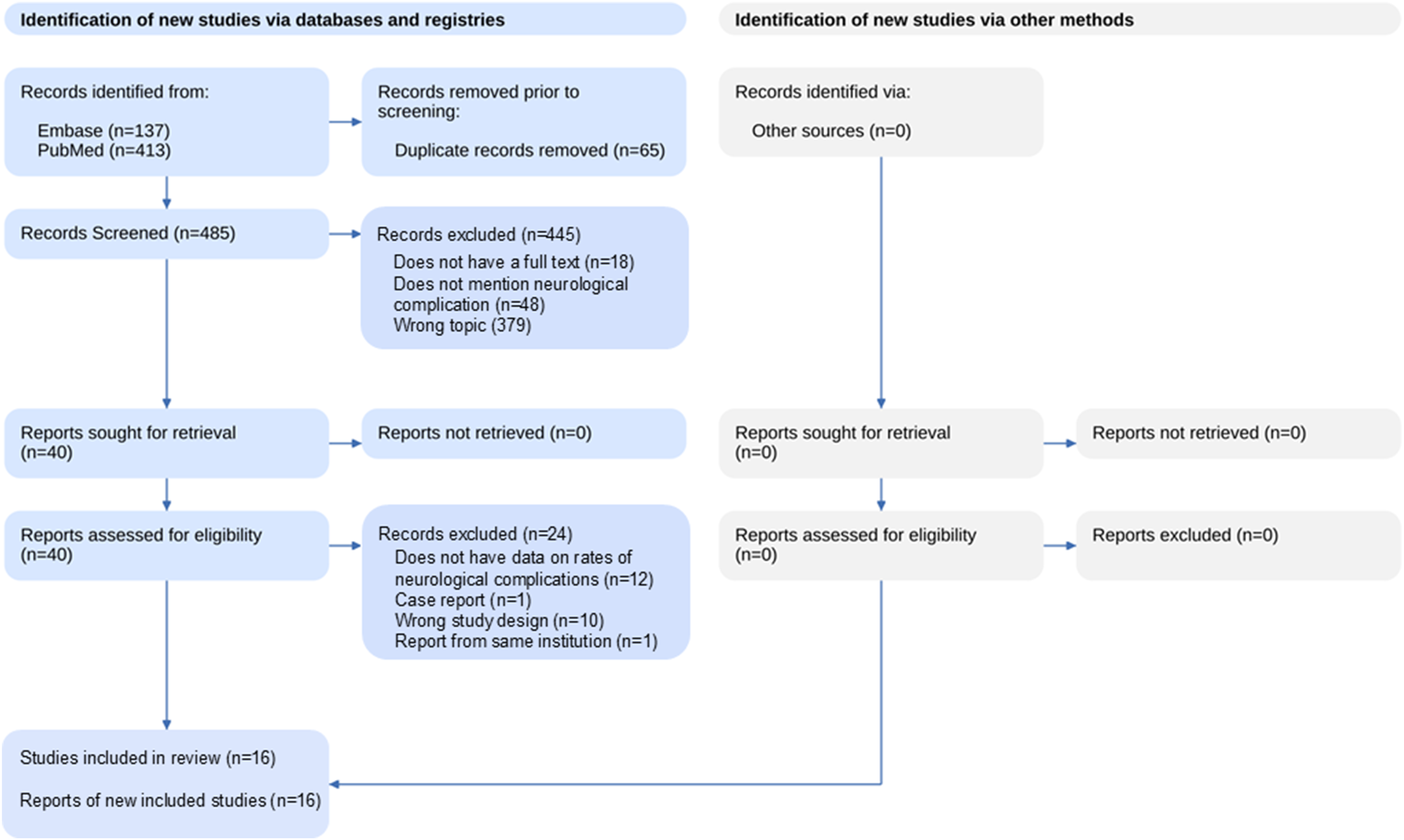
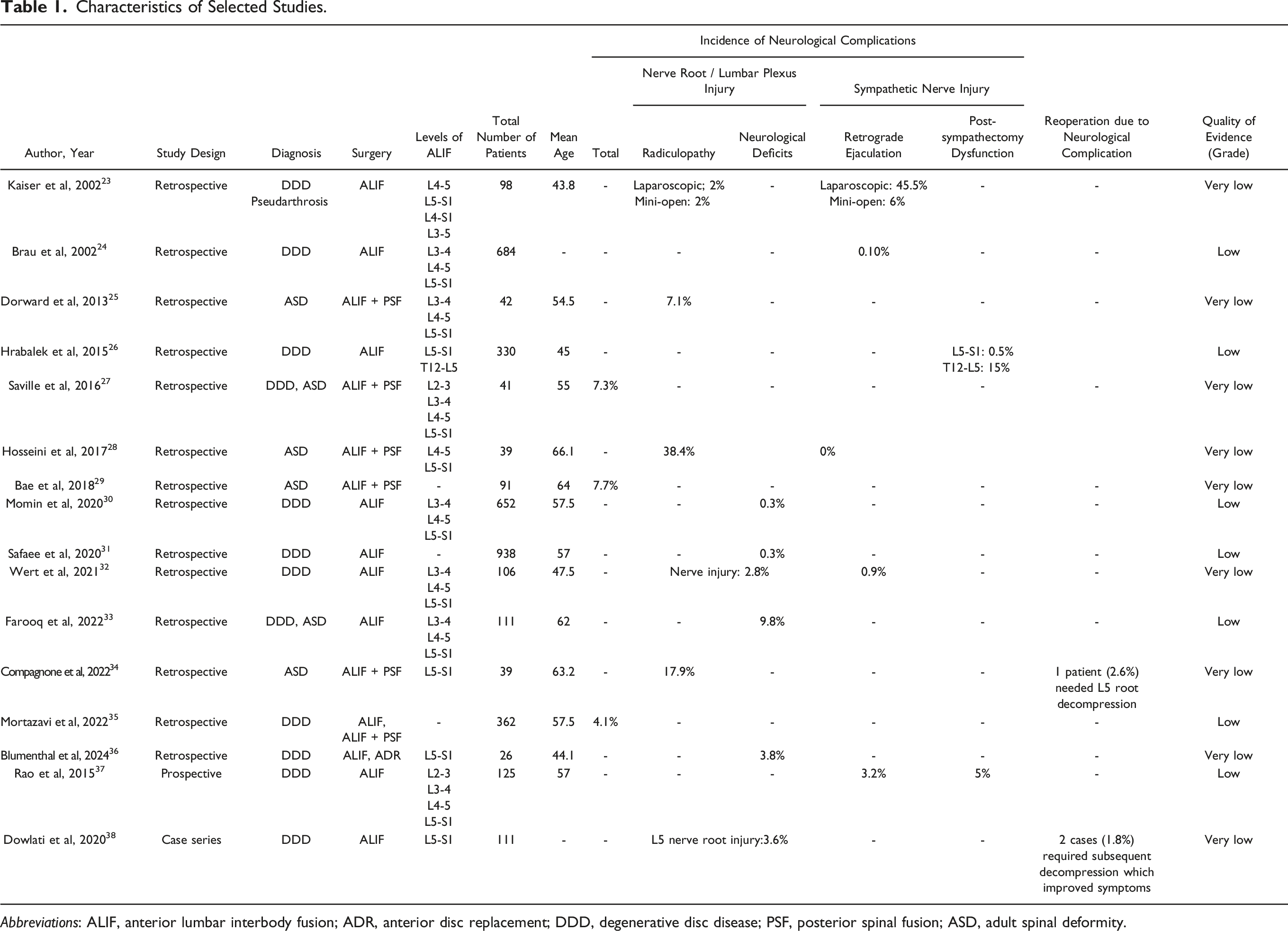
In the 16 articles included in this review, the overall rate of neurological complication following an ALIF ranged from 4.1% to 7.7%. However, rates of specific neurological complications were highly variable; 0.1-38.4% for nerve root or lumbar plexus injury (radiculopathy and neurological deficit) and 0-45.5% for sympathetic nerve injury (retrograde ejaculation (RE) and post-sympathectomy dysfunction). Forest plot of the incidence rate of nerve root / lumbar plexus injury. Per person-case year showed the incidence rates of nerve root injury were relatively higher in ASD patients than in those with DDD (Figure 2). Reoperation rates due to neurological complications ranged from 1.8% to 2.6%, all of which were motivated by nerve root involvement in L5-S1 cases.34,36 (Table 1). In all of the cases requiring reoperation for neurologic complications, additional direct decompression surgery was performed to improve radiculopathy or motor weakness following L5-S1 ALIF. Forest plot showing the incidence rate of nerve root/lumbar plexus injury. Per person-case year. The incidence rates of nerve root injury were relatively higher in adult spinal deformity (ASD) patients than in those with degenerative disc disease (DDD). Characteristics of Selected Studies. Abbreviations: ALIF, anterior lumbar interbody fusion; ADR, anterior disc replacement; DDD, degenerative disc disease; PSF, posterior spinal fusion; ASD, adult spinal deformity.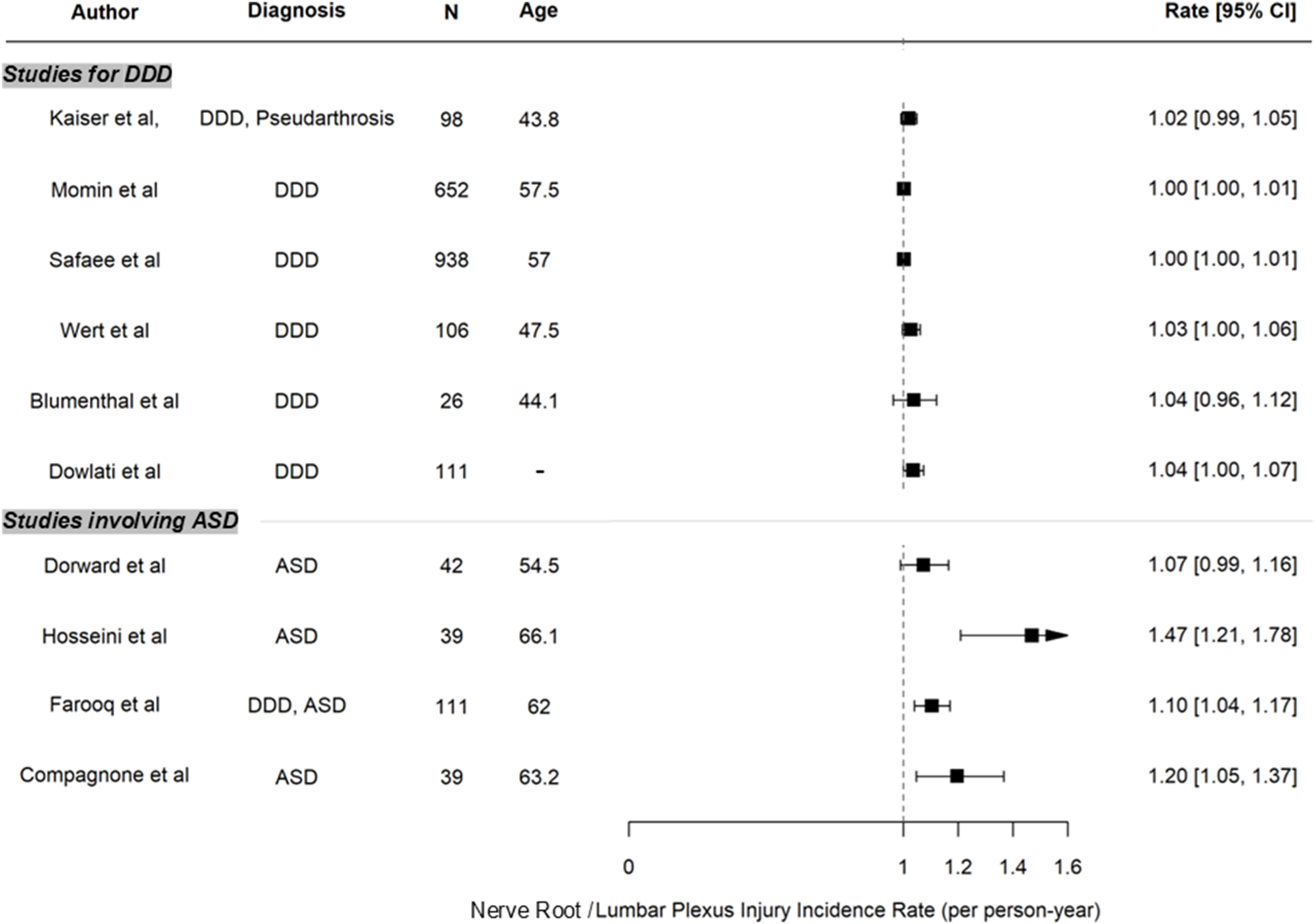
Risk Assessments
A risk of bias assessment was performed for each included study (Figure 3). Eleven of the 16 studies were judged to hold moderate risk of bias, while 3 studies demonstrated serious risk of bias, and 2 studies showed a critical risk of bias. Since the vast majority of the studies were retrospective, their bias was primarily due to confounding factors and participant selection. The overall risk of bias in the study set was moderate or greater when considering all 7 domains together, likely influenced by the inclusion of nonrandomized studies. The overall quality of evidence per outcome assessed by GRADE showed 8 studies were deemed to have very low-quality evidence, and 8 with low quality. Risk of bias measured using the ROBINS-I (Risk Of Bias In Non-randomized Studies of Intervention) tool.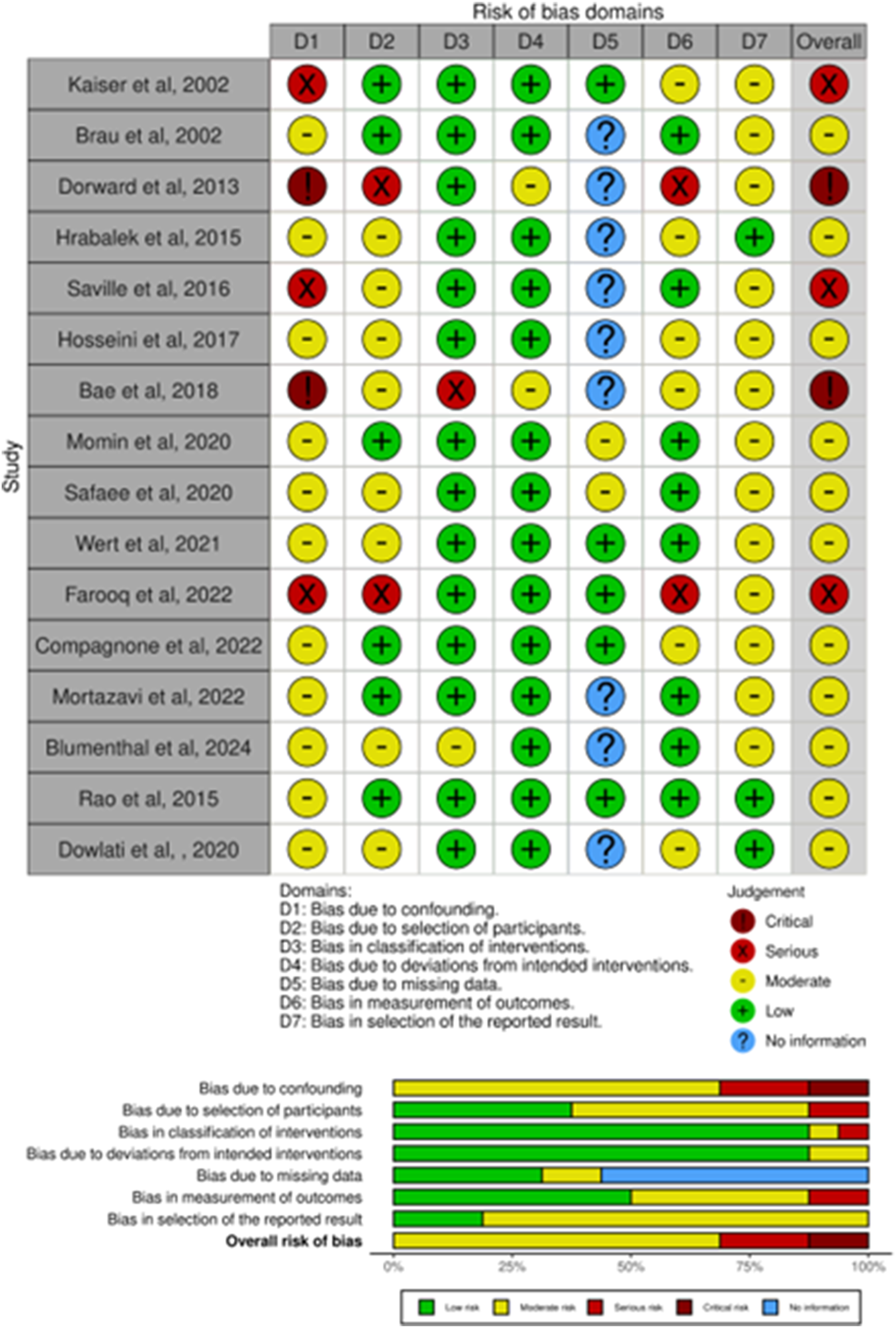
Discussion
The overall incidence of neurological complications associated with ALIF procedures included in this review was relatively low, ranging from 4.1% to 7.7%. The rates varied by type of neurological complications and are divided here into 2 main categories: nerve root/lumbar plexus injury (radiculopathy and neurological deficit) or sympathetic nerve injury (retrograde ejaculation and post-sympathectomy dysfunction).
Nerve Root/Lumbar Plexus Injury
Symptoms ascribed to nerve root or lumbar plexus injury generally presented with radicular pain, motor weakness, and/or sensory deficit in the lower extremity (ies). The rate of nerve root/lumbar plexus injury included in this study ranged from 0.1% to 38.4%. While the rates of nerve root injury in degenerative disc disease (DDD) cases ranged from 0.3% to 3.8%, studies involving adult spinal deformity (ASD) reported higher rates between 7.1% and 38.4%. Prior studies have described independent risk factors for neurologic complications following an ALIF, which include a procedure at L5-S1, higher body mass index, higher grade of anterolisthesis, and severe facet arthropathy. 39 In light of the results of this review, an ALIF performed in the setting of ASD may also serve as an additional risk factor for neurological complications.
In the articles focusing on ALIFs performed at L5-S1 in this review, rates of L5 nerve root injury were less than 4% for DDD cases36,38 and 17.9% for ASD cases.
34
Given that all the cases that required reoperation in this study were at the L5-S1 level,34,38 an ALIF performed at L5-S1 should be considered to carry the greatest risk of nerve root injury when compared to other lumbar levels. This assertion is supported by a study by Farooq et al who evaluated neuromonitoring changes during ALIF procedures and observed that all intraoperative neuromonitoring changes occurred during procedures at the L5-S1 level.
33
The mechanisms for L5 radiculopathy after an L5-S1 ALIF were discussed in 2 studies.34,38 One common mechanism for nerve root injury following an L5-S1 ALIF was worsening foraminal stenosis due to the “pincer mechanism” (Figure 4A). Compagnone et al evaluated patients who developed an L5 radiculopathy or weakness after a hyperlordotic (HL) ALIF at L5-S1 with posterior fusion to correct spinal deformity and observed that the posterior disc height and the amount of segmental correction may be correlated with the onset of post-operative radicular pain. They also described a postoperative change in foraminal morphology whereby subluxation of the S1 superior articular facet can impinge on the exiting L5 nerve root.
34
At their institution, a similar case series reported that 2 out of 12 patients (16.7%) who underwent ALIF at L5–S1 for revision surgery developed L5 radiculopathy. In both cases a large difference between anterior and posterior height caused by the placement of a HL cage led to worsened foraminal stenosis and compression of the exiting L5 nerve root.
40
This postoperative anatomical feature may result in a similar “pincer mechanism” etiology of radiculopathy. Postoperative L5 radiculopathy may also result from overdistraction of the L5-S1 foramen with tension on the exiting L5 nerve root. Dowlati et al performed a retrospective review of 111 patients undergoing stand-alone ALIFs at L5-S1 and concluded that significant disc height and foraminal height restoration can lead to overdistraction of the foramen with L5 stretch neuropraxia with potential for permanent neurological injury.
38
Coronal CT reconstructions in these patients revealed possible displacement of the L5 nerve against a posteroinferior osteophyte at L5–S1 as a result of the disc height reexpansion in patients who experienced symptomatic nerve root injury despite no obvious foraminal pathology on postoperative MRI and CT imaging (Figure 4B). Scheme illustrating anatomical features of L5 and S1 spine along with L5 nerve root. (A) Sagittal view showing postoperative change in foraminal stenosis. After the placement of the ALIF cage, the L5 nerve root is irritated due to the subluxation of the S1 superior articular facet z (arrow head), resulting in secondary stenosis of the neural foramina (pincer mechanism). (B) Coronal view. Overdistraction due to significant reexpansion in disc height by ALIF cage may result in a neuropraxia stretch injury, or a possible displacement of the L5 nerve against a posteroinferior sharp osteophyte (arrow head).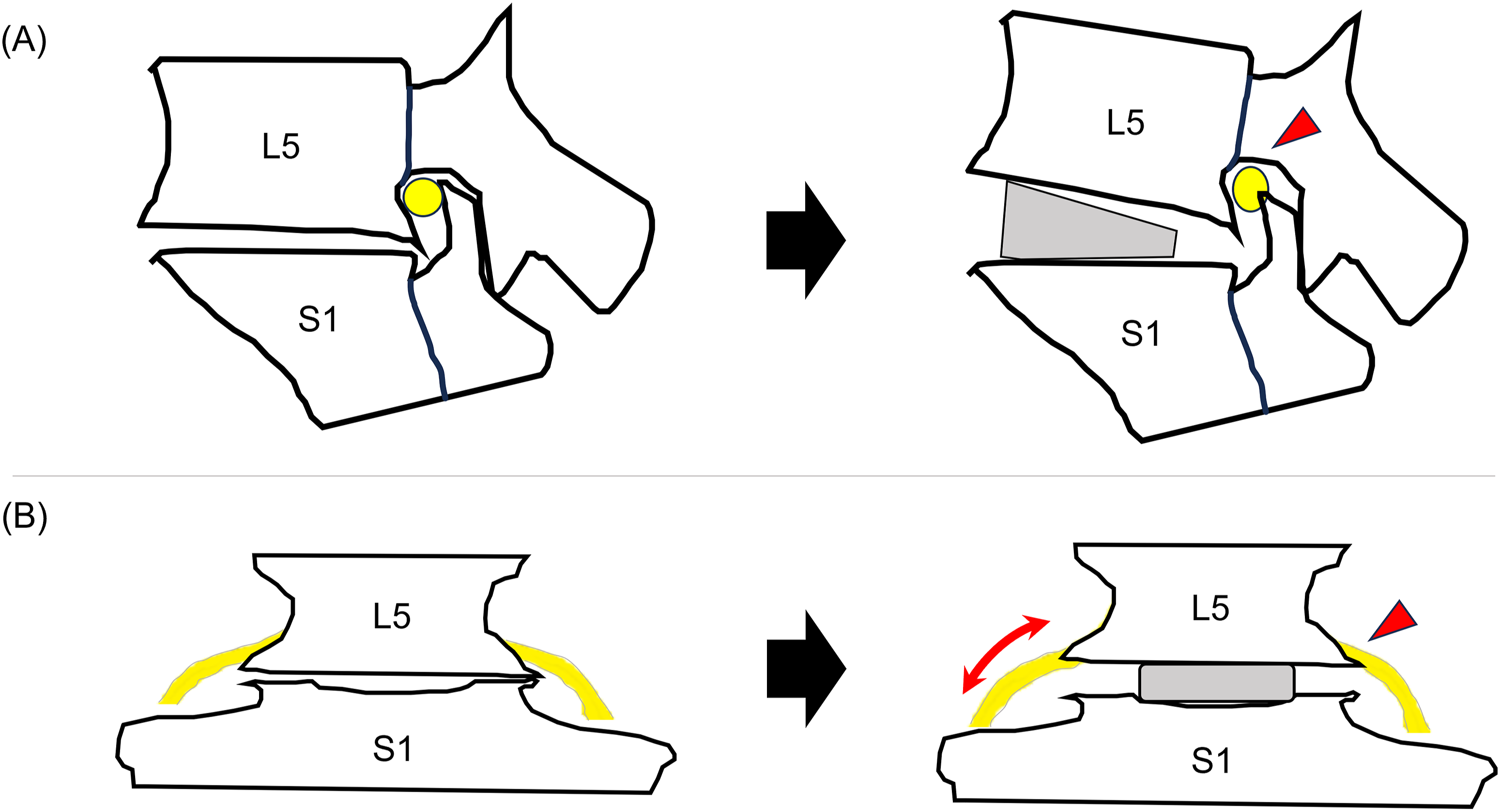
Sympathetic Nerve Injury
Damage to the sympathetic nerve chain, particularly the superior hypogastric plexus in males, can result in retrograde ejaculation (RE) as well as leg and groin dysesthesias. The superior hypogastric plexus lies beneath the peritoneum and ventral to the aorta and aortic bifurcation. It continues over the anterior surface of L5–S1 as it carries sympathetic fibers down into the pelvis.41-43 Injury to the plexus causes relaxation of the internal bladder sphincter at time of ejaculation resulting in retrograde flow of seminal fluid from the posterior urethra into the bladder.42,43 The incidence of RE varied among the studies included in this review from 0% to 45.5%. Despite this wide variation, it should be noted that occurrence of RE was highly related to the approach to prevertebral space. The incidence of RE was 0.1-3.2% with a retroperitoneal exposure while it was significantly higher (ranging from 6% to 45.5%) with a mini-open or laparoscopic transperitoneal approach. As studies were published showing increasing rates of RE with transperitoneal approaches, retroperitoneal approaches have largely become the standard approach to the anterior lumbar spine.17,37,41 Even with an injury leading to RE, Body et al reported that nearly half of the patients who experienced RE following anterior lumbar surgery recovered between 3 and 48 months. 43 Several risk factors for RE were described including a transperitoneal approach, aggressive traction on the plexus, accidental ligation of the hypogastric plexus with electrocautery, and the use of recombinant human bone morphogenetic protein–2 (rhBMP-2) in ALIF.17,41,43 Despite some data suggesting that the risk of RE may be different with procedures at L4-5 vs L5-S1, this systematic review was not able to determine the relative risk between lumbar spine levels. 37
In addition to injury to the superior hypogastric plexus, the lumbar sympathetic trunk is also at risk of injury in its location on the antero-lateral aspect of the lumbar vertebral bodies. Injury to the lumbar sympathetic trunk typically results in post-sympathectomy dysfunction which can be characterized by an increase in skin temperature, reduced perspiration and sometimes by dysesthesias, discoloration and swelling of the lower limb on the side of the anterior approach. 44 This effect commonly causes patients to complain of a relative “coolness” in their contralateral foot. Hrabalek et al identified post-sympathectomy dysfunction in 0.5% of patients following an ALIF at L5-S1 and in 15% of patients that underwent an ALIF between T12-L5. 26 Since the lumbar sympathetic trunk originates from the retroperitoneal space at the level of L2 vertebrae and sits parallel to the anterior border of the psoas major in the normal lumbar spine, 45 the anterior approach at the L5-S1 level is often safe. At the L4-5 level and cephalad, in contrast, the sympathetic chain often lies in the middle of the disc necessitating its separation and in some cases sacrifice to allow surgical access to the disc space. 26
Technical Recommendations to Reduce the Risk of Neurological Complications
Based on the results of this study, technical pearls to avoid neurological complications remain unclear and controversial (Figure 5). Several specific recommendations were proposed by the past studies to reduce the risk of neurologic injury including using a retroperitoneal approach, utilizing an experienced access surgeon and avoiding the placement of rhBMP-2.17,41-43,46 Two studies evaluated the use of intraoperative neuromonitoring (IONM) to detect post-operative neurological complications. Farooq et al demonstrated potential benefits of IONM for patients undergoing ALIF,
33
reporting that intraoperative changes in IONM signals resulted in surgical adjustments that likely prevented neurological deficits postoperatively, especially in complex spine surgeries. A study by Blumenthal et al, conversely, indicated that IONM did not provide any benefit for lumbar anterior approach surgery noting 1 false-positive change in monitoring and 2 false-negative results of IONM for the 2 patients with a postoperative foot drop.
36
These numbers may be too small to draw a meaningful clinical determination of the utility of IONM to reduce the risk of postoperative neurologic deficit. Agreement and disagreement on the risks and considerations associated with neurological complications following ALIF.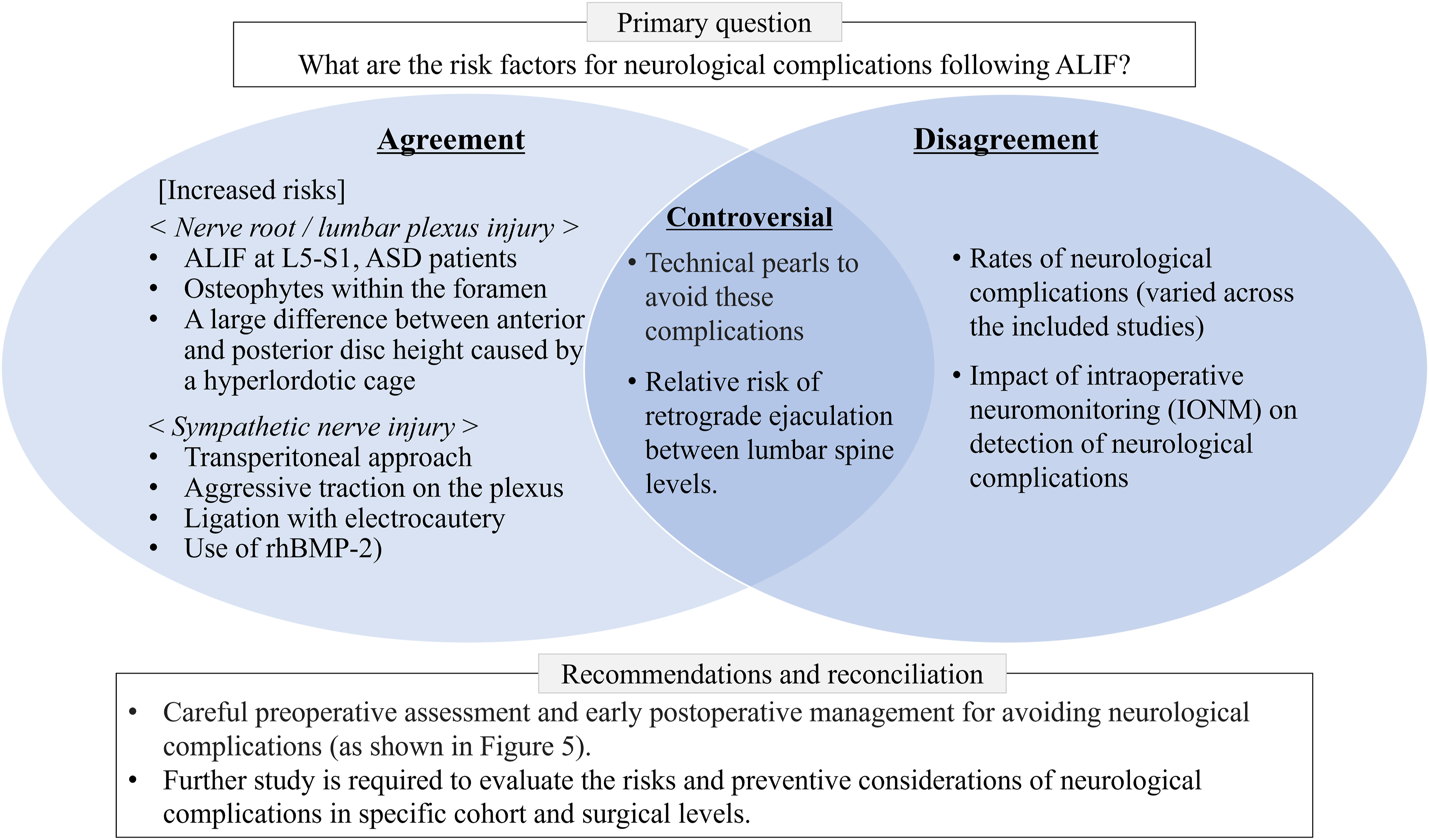
Preoperative planning and meticulous understanding of the neurologic anatomy during surgery are crucial to reduce the neurological complications following an ALIF procedure. For the cases in which the L5-S1 level is addressed, surgeons should carefully evaluate preoperative CT scans specifically for osteophytes on the superior articular process of S1 within the L5-S1 foramina or at the posteroinferior corner of the L5 vertebral body. If present, surgeons should consider a posterior foraminal decompression following the placement of the ALIF cage. Careful selection of implant size is also essential to mitigate the risk for overdistraction of the foramen with stretch injury of the exiting nerve root. In the case of a postoperative deficit, close evaluation of postoperative imaging might provide valuable information
37
with coronal CT plane images being useful to identify posteroinferior sharp osteophytes which can cause impingement and stretch on the L5 exiting nerve root (Figure 6). A proposed strategic management flowchart for foraminal stenosis following ALIF.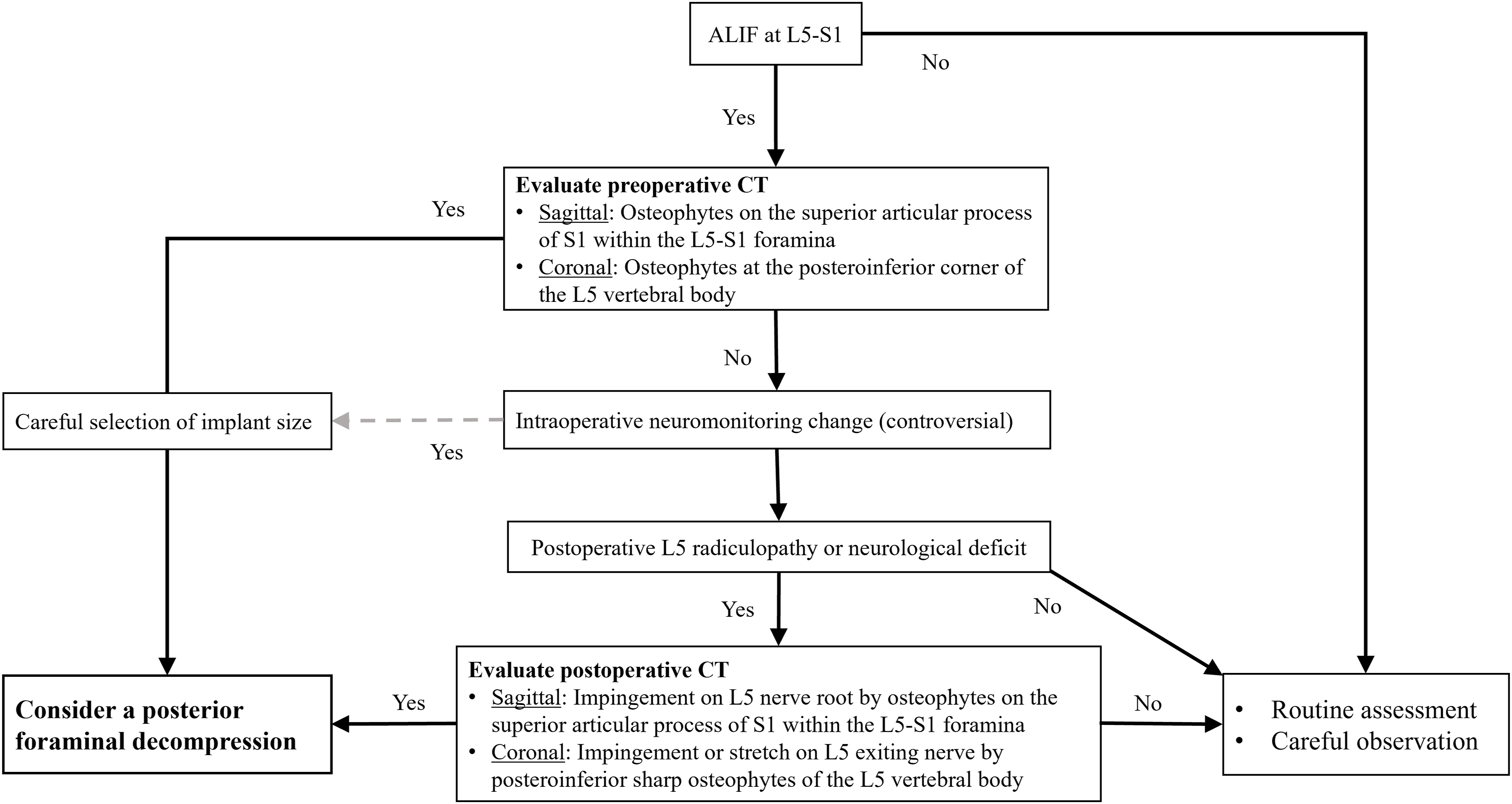
To avoid sympathetic nerve injury, gentle dissection of the peritoneum during exposure of the ventral spine may reduce the risk of injury to the plexus. However, the risk of RE should be thoroughly discussed with male patients as part of the informed consent process prior to surgery.
Limitations
Variability of Outcomes as Neurological Complications Across the Included Studies.
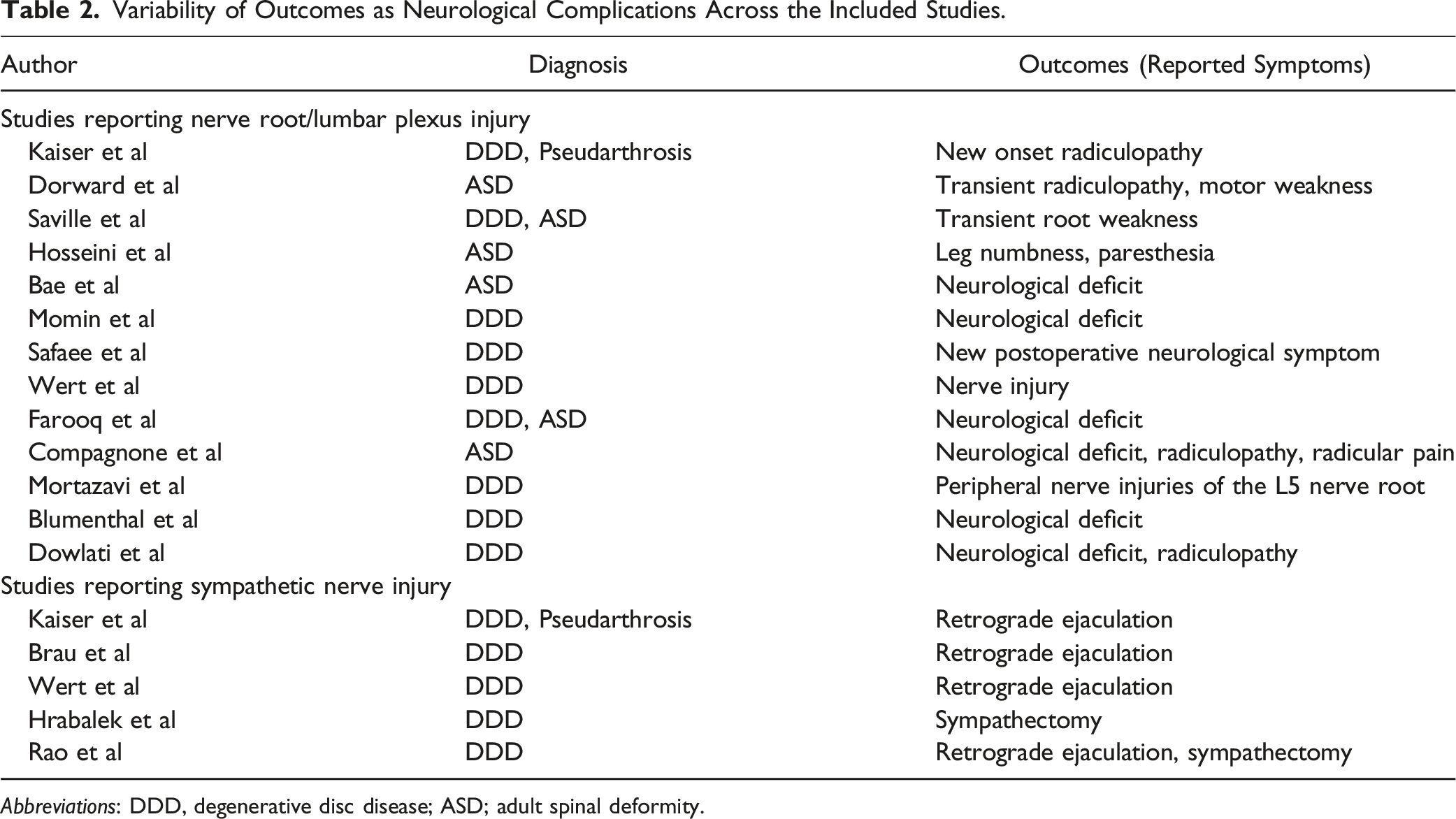
Abbreviations: DDD, degenerative disc disease; ASD; adult spinal deformity.
Conclusion
The overall incidence of neurological complications following an ALIF procedure ranged from 4.1% to 7.7%. This rate varied among the type of nerve injury, surgical level, approach and diagnosis. The incidence of nerve root or lumbar plexus injury was notably higher in patients undergoing ALIF at L5-S1 and those with ASD, reaching up to 38.4%. Particularly for ALIFs at L5-S1, osteophytes on the superior articular process of S1 at the L5-S1 foramen and a posteroinferior osteophyte on the L5 vertebral body can be risk factors for postoperative L5 foraminal stenosis. In terms of sympathetic nerve injury, the risk for RE in this study was 0.1-3.2% with a retroperitoneal approach, excluding cases with transperitoneal approach. Reported risk factors for sympathetic nerve injury included transperitoneal approach, aggressive traction on the plexus, accidental ligation using electrocautery, the use of rhBMP-2, and ALIF at L4-5 and above. To mitigate the neurological complications following ALIF procedures, careful preoperative surgical planning and gentle dissection through carefully evaluated anatomy are essential.
Footnotes
Author Contributions
Takeshi Fujii, MD, PhD (Study design, performed measurements, manuscript preparation). Rakesh Kumar MD (Study design, performed measurements, manuscript preparation). Jihun Cha, BS (Study design, performed measurements, manuscript preparation). Aiyush Bansal, MD (Study design, risk of bias assessment, manuscript preparation), Rafael Garcia de Oliveira, MD (Study design, results review, risk of bias assessment, manuscript preparation), Philip K. Louie MD (Study design, results review, manuscript preparation), Venu Nemani, MD, PhD (Results review, manuscript preparation). Jean-Christophe Leveque MD (Results review, manuscript preparation). Rajiv K. Sethi MD, PhD (Results review, manuscript preparation).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval/Research Ethics Committee,or Local Equivalent
This study did not include any identifying information and was based on anonymous, voluntary participation in a survey. No IRB was needed for this study.
Data Availability Statement
A list of include studies and the search strategy have been provided in the manuscript and table.