
Abstract
Study Design
Retrospective cohort
Objective
Anterior lumbar interbody fusion (ALIF) may be complicated by subsidence, which can lead to significant morbidity including pain, disc space collapse, neural compression, segmental kyphosis, instability, and vertebral body fracture. This study sought to identify patient and procedural risk factors for subsidence in patients undergoing ALIF.
Methods
This study analyzed consecutive patients who underwent ALIF at a single institution with a minimum of 2 years follow-up. Patients were grouped as either Non-Subsidence (NS-ALIF) or Cage Subsidence (CS-ALIF) based on the final postoperative radiograph. Demographic variables, operative characteristics, and radiographic outcomes were evaluated to identify significant predictors on univariate and multivariate statistics.
Results
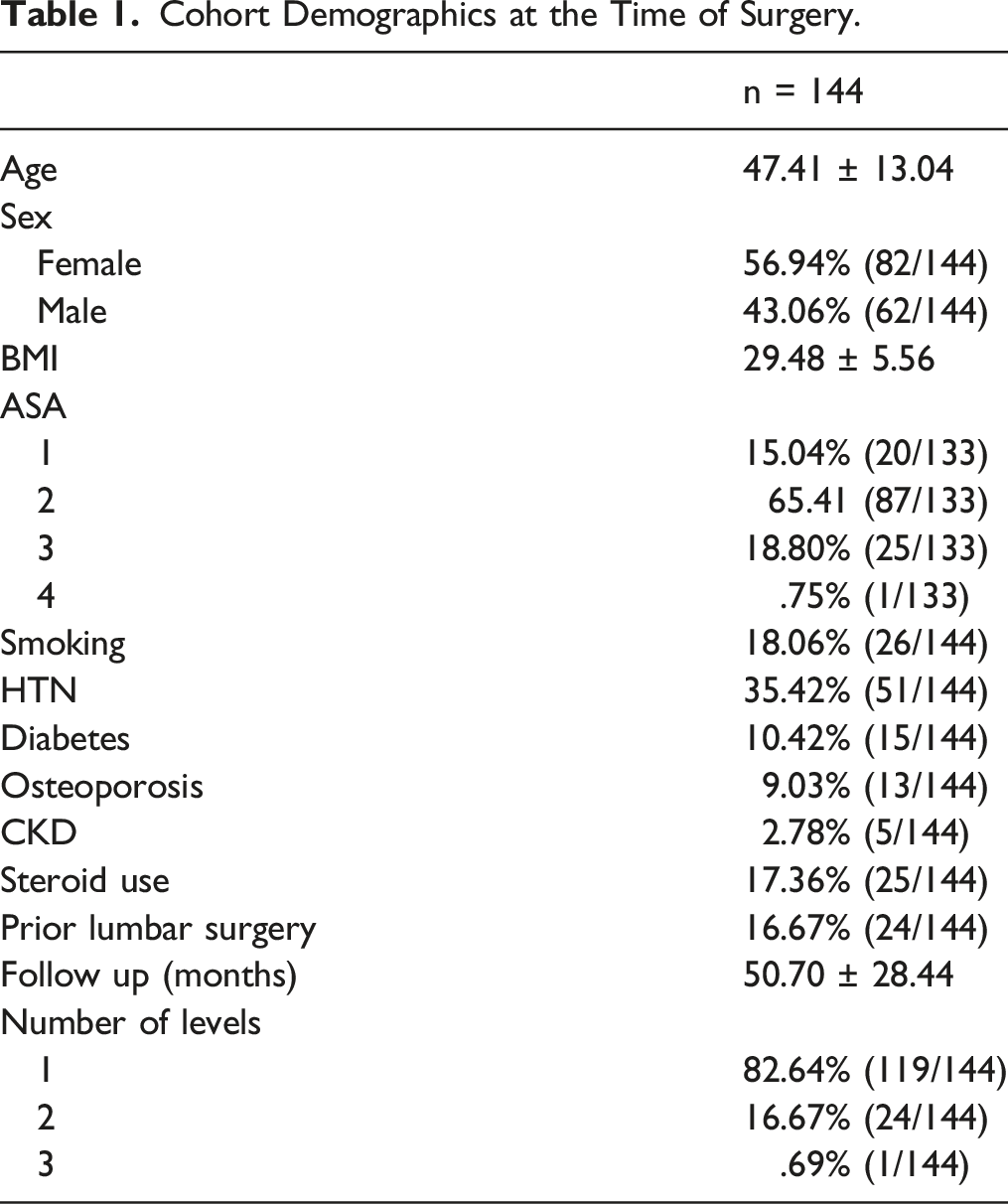
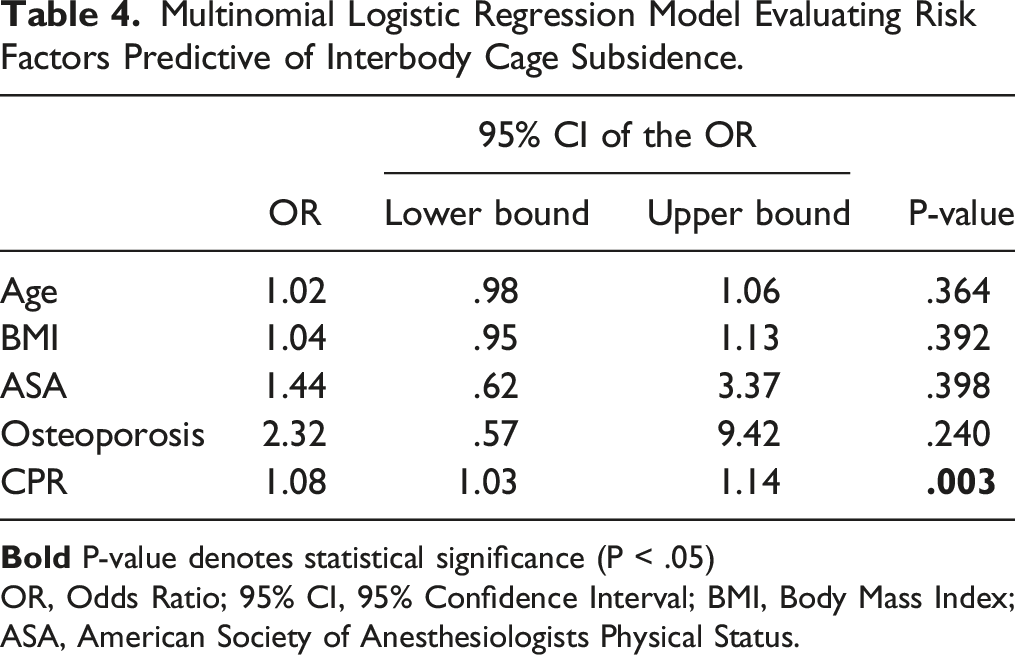
144 patients (170 levels) were included with an average follow-up of 50.70 ± 28.44 months (4.23 years). The incidence of subsidence was 22.94% (39/170 levels). On univariate statistics, the CS-ALIF group was significantly older (P = .020), had higher BMI (P = .048), worse ASA (P = .001), higher prevalence of comorbid osteoporosis (P < .001), and a more anteriorly placed interbody device (P = .005). On multivariate analysis, anterior cage placement remained the only significant predictor (OR: 1.08, 95% CI: 1.03–1.14; P = .003). There was a significantly higher rate of subsequent adjacent segment surgery among the CS-ALIF group (P = .035).
Conclusion
Factors contributing to subsidence in ALIF included older age, higher BMI, severe ASA, and osteoporosis, while anterior cage placement remained the only independent predictor on multivariate analysis. Subsidence was associated with a higher rate of subsequent adjacent segment surgery. Surgical technique should optimize placement of the interbody cage and avoid overstuffing the disc space.
Keywords
Introduction
Anterior lumbar interbody fusion (ALIF) is a less invasive approach to circumferential fusion of the lower lumbar spine with significant utility in the treatment of degenerative and isthmic spondylolisthesis, degenerative spondylosis, and deformity.1,2 The anterior approach forgoes the extensive dissection of paraspinal musculature inherent to posterior approaches, while also providing the surgeon with extensive exposure to the ventral disc space, therefore allowing for efficient disc space clearance and endplate preparation. Additionally, the direct anterior approach to the disc space allows the surgeon to maximize the size of the interbody cage implanted, thus providing the advantage of improved disc height, lordotic correction, and high rates of successful interbody arthrodesis. 3 Despite the advantages of the ALIF procedure, potential complications include approach-related injury to vascular and visceral structures, as well as subsidence of the interbody cage into the adjacent endplates.4-6
Interbody cage subsidence may be associated with significant morbidity including severe pain, disc height collapse, neural compression, segmental kyphosis, loss of stability, and vertebral body fracture.6-8 These sequelae may subsequently lead to persistent motion at the device-host bone interface, thereby increasing the risk for pseudarthrosis at the operative motion segment. 9 Past studies have identified several procedural and patient-specific factors that may increase the risk for interbody subsidence in the context of various other fusion procedures. Among these are low bone mineral density (BMD), increased age, body mass index (BMI), overpreparation of the endplates, and off-center cage placement.9-12 Despite the extensive literature on patient outcomes and subsidence rates following ALIF, there is a paucity of clinical studies evaluating risk factors for subsidence in the context of the ALIF procedure.
This study sought to identify patients who experienced subsidence of the interbody cage following ALIF in order to evaluate for surgical and patient-specific risk factors that may have contributed to its development.
Methods
Patient Selection
Institutional Review Board approval was obtained (ORA 20073102) to retrospectively review a prospectively maintained surgical database for all patients who underwent ALIF at a single tertiary academic medical institution between the years 2006 and 2019. Due to its retrospective nature, this study was exempt from obtaining informed consent. The inclusion criteria were patients over the age of 18 who underwent ALIF for the treatment of severe degenerative disc disease (DDD), degenerative spondylolisthesis, isthmic spondylolisthesis, degenerative scoliosis, or symptomatic pseudarthrosis of a prior lumbar fusion with a minimum of 2 years radiographic and clinical follow-up. Patients were excluded from the analysis if they were receiving concomitant treatment for the indications of tumor, trauma, or infection.
Outcome Selection
Following patient identification and inclusion, demographic variables, operative characteristics, and radiographic outcomes were collected. Demographic variables of interest included the patient’s age, sex, BMI, American Society of Anesthesiologists Physical Status (ASA) score, medical comorbidities (hypertension, diabetes, osteoporosis, chronic kidney disease), perioperative steroid use, and smoking status. Operative data included the operative levels and number of operative levels, interbody cage characteristics (manufacturing material, height, lordosis), and the use of iliac crest autograft and/or recombinant human bone morphogenetic protein-2 (rhBMP-2).
Standing lateral radiographs were assessed at the preoperative, 6 weeks postoperative, and final postoperative (beyond 2 years) time points. Cage height was assessed at the preoperative and 6 weeks postoperative time points using the Farfan index. This is calculated as the sum of the anterior disc height (a) and the posterior disc height (b), divided by the anteroposterior depth of the superior endplate of the inferior vertebra (c) and multiplied by 100 to obtain a percentage ( (A) Demonstrates measurements of anterior disc height (a), posterior disc height (b), endplate width (c), and the distance of the interbody cage center point from the posterior edge of the disc space (x). (B) Demonstrates the magnitude of interbody cage subsidence (z) into the vertebral endplate (y).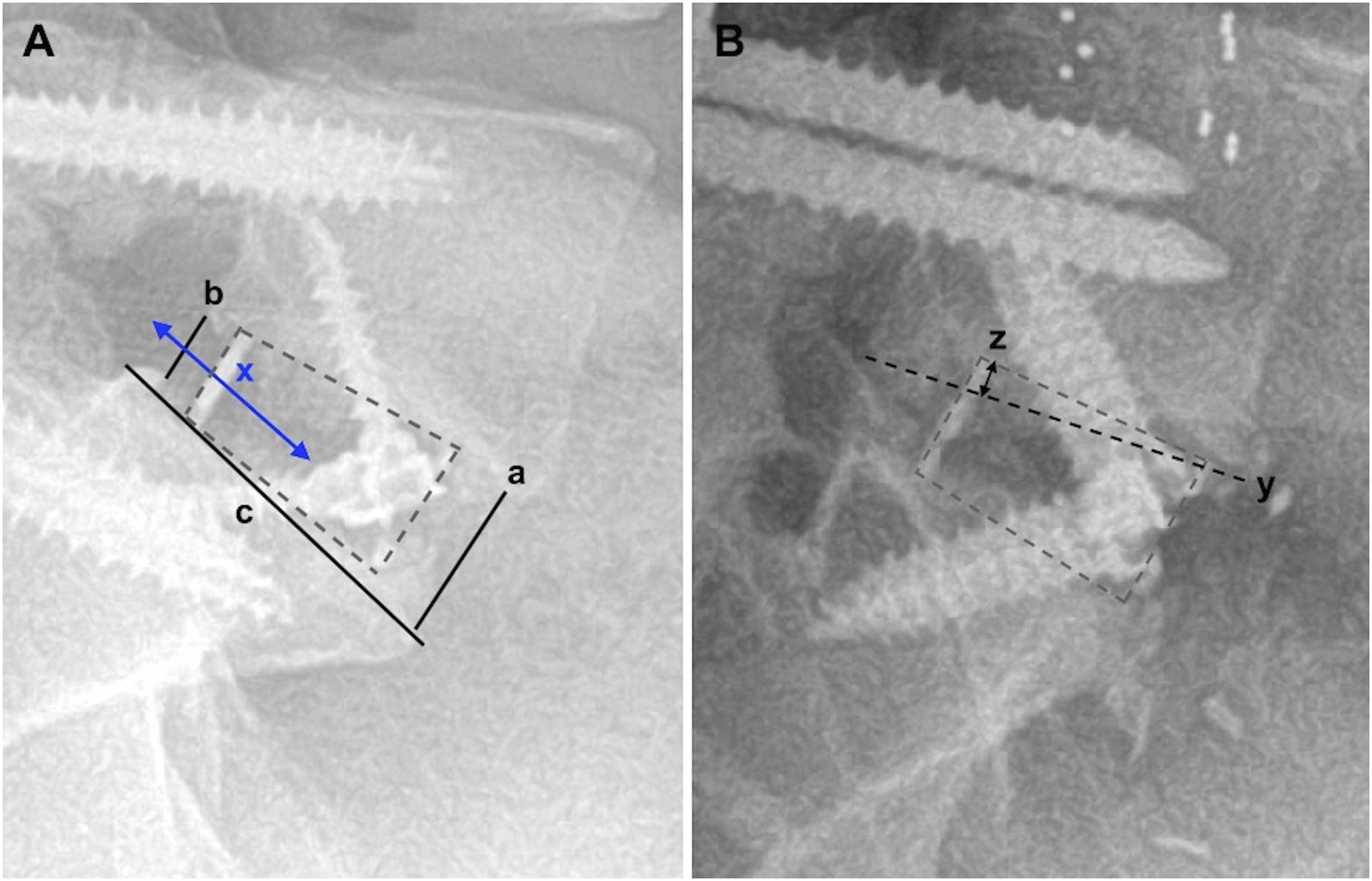
Statistical Analysis
All statistical methods were performed using SPSS version 28.0 (IBM Corporation, Armonk, NY) and STATA v16.1 (Stata Corp, Houston, TX). Descriptive statistics were used to describe the characteristics of the whole cohort. Categorical and continuous variables were compared between NS-ALIF and CS-ALIF groups via univariate analysis which included chi square and independent samples t-test, respectively. Risk factors that were significant on univariate analysis were retained for multivariate testing employing a multinomial logistic regression model. The results of the multinomial logistic regression were reported as the odds ratio (OR) and corresponding 95% confidence interval (95% CI). Dominance analysis was performed to determine the relative contribution of each covariate to the overall model fit, as described by the McFadden pseudo-R2. The threshold for statistical significance was set to P < .05.
Results
Cohort Demographics at the Time of Surgery.
Univariate Risk Factors
Univariate Comparison of Patient Demographics Between Non-Subsidence and Cage Subsidence ALIF groups.
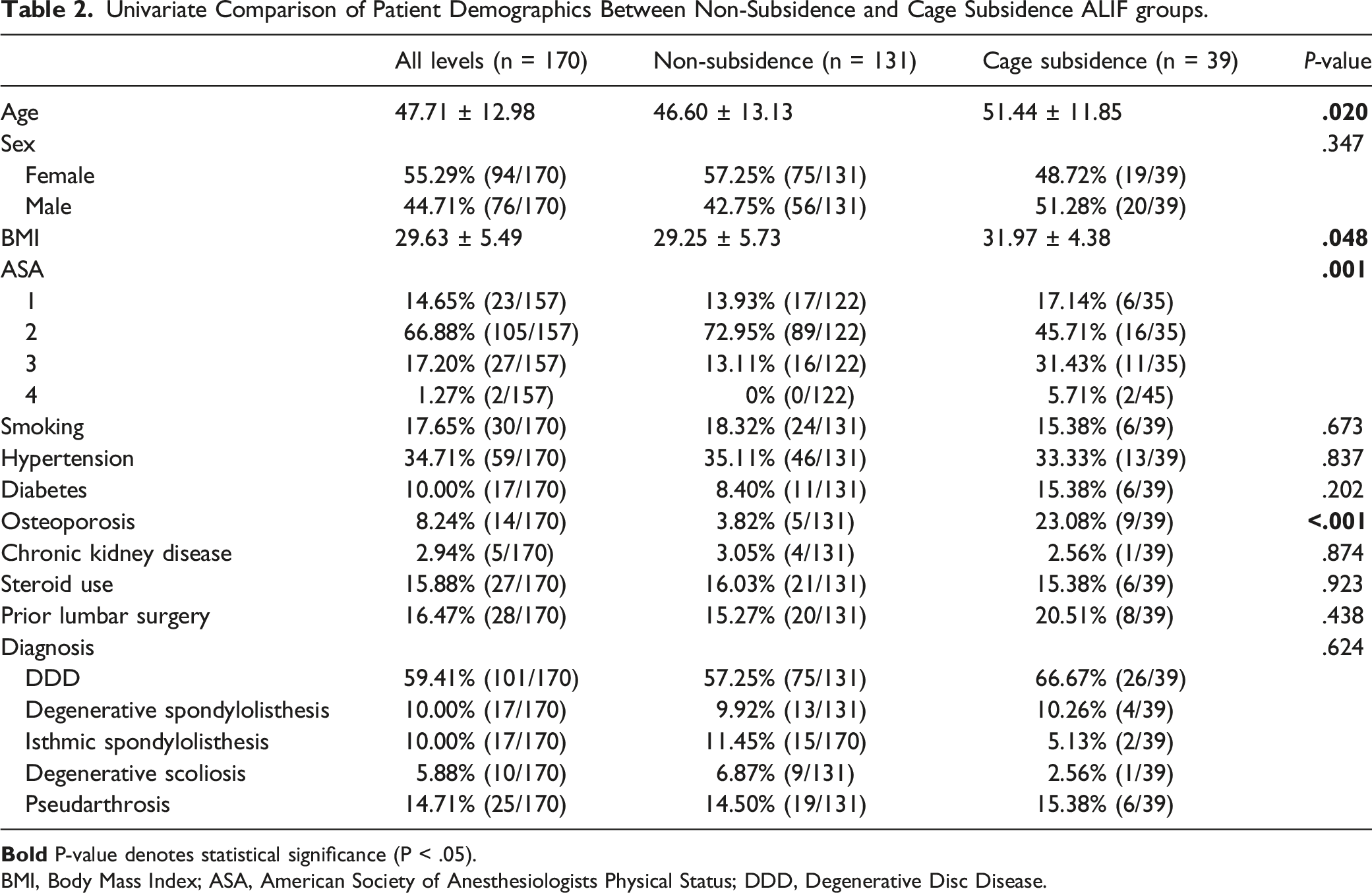
BMI, Body Mass Index; ASA, American Society of Anesthesiologists Physical Status; DDD, Degenerative Disc Disease.
Univariate Comparison of Operative Characteristics and Radiographic Outcomes Between Non-Subsidence and Cage Subsidence ALIF groups.
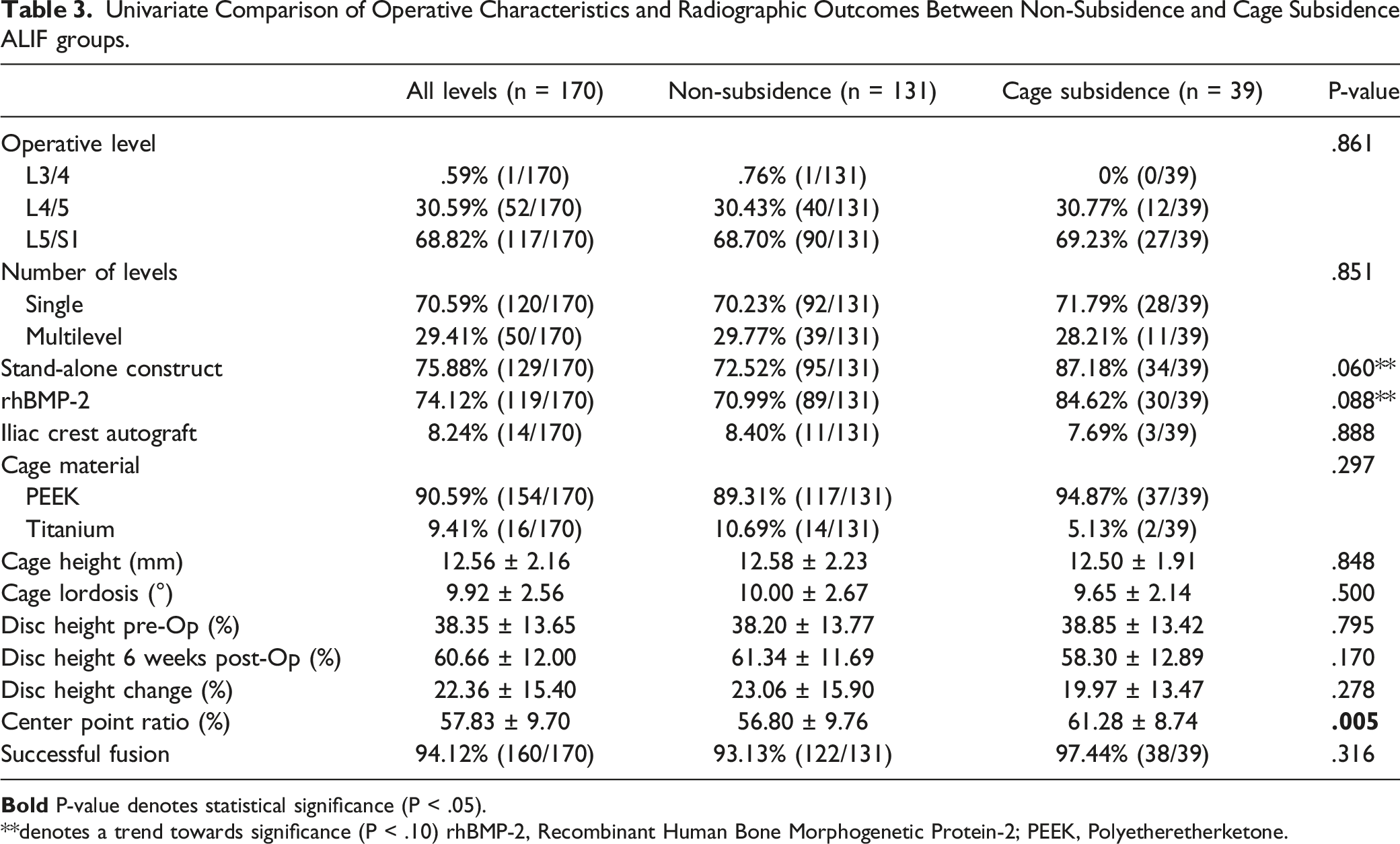
**denotes a trend towards significance (P < .10) rhBMP-2, Recombinant Human Bone Morphogenetic Protein-2; PEEK, Polyetheretherketone.
Radiographically, the interbody device was placed more anteriorly in the disc space among CS-ALIF patients as determined by the CPR (61.28 ± 8.74% vs 56.80 ± 9.76%, P = .005). There were no differences in disc heights at the preoperative (P = .795) or 6 weeks postoperative time periods (P = .170), nor in the magnitude of change (P = .278). Successful fusion was seen among 97.44% (38/39) CS-ALIF and 93.13% (122/131) of NS-ALIF patients, with no statistical difference between cohorts (P = .316).
Multivariate Risk Factors
Multinomial Logistic Regression Model Evaluating Risk Factors Predictive of Interbody Cage Subsidence.
Secondary Surgical Intervention
Overall, 26 of 144 patients (18.06%) underwent subsequent surgery either at the index operative segment or at an adjacent level. There was a higher incidence of subsequent surgical intervention among the CS-ALIF group, although the difference was non-significant (38.46% vs 26.72%, P = .158). Index-level revisions were seen at similar rates between CS-ALIF and NS-ALIF groups (5.26% vs 3.85%, P = .701). When evaluating the development of pathology at adjacent segments, there was a trend towards a higher incidence of ASD among the CS-ALIF group (35.90% vs 22.14%, P = .083) and a significantly higher proportion of the CS-ALIF group underwent subsequent surgery at an adjacent lumbar level (20.51% vs 8.40%, P = .035), while a similar proportion developed pathology at the sacroiliac (SI) joint requiring SI fusion (0% vs 3.82%, P = .216).
Discussion
Subsidence of the intervertebral device following lumbar fusion may present with severe pain, neural compression, malalignment, instability, and vertebral body fracture potentially necessitating revision surgery. This study evaluated patient-specific and procedural risk factors for interbody cage subsidence in 144 patients who underwent ALIF at 170 vertebral levels and followed up postoperatively for a minimum of 2 years (mean 4.23 years) after surgery. Subsidence of 2 mm or more was measured at 22.94% of all operative levels. We found that older age, high ASA, increased BMI, osteoporosis, and anterior cage placement posed a significant risk on univariate analysis. On multivariate analysis, anterior cage placement remained the only significant independent risk factor for subsidence, with a relative contribution of 52.6% to the overall model fit. Additionally, subsidence was associated with a significantly higher incidence of adjacent segment pathology requiring subsequent surgery.
Past studies have demonstrated that the central endplate represent the region of lowest subchondral BMD and is thus less resistant to compressive load than the peripheral endplate.18-21 A biomechanical study evaluating the effect of cage width in a human cadaveric lateral lumbar interbody fusion (LLIF) model found that placement of a larger cage that spans the width of the ring apophysis increased the compressive strength of the construct, thus decreasing the risk of subsidence. 22 Few clinical studies have investigated the relationship between cage placement and subsidence in posterior approaches to lumbar fusion. In all cases, off-center cage placement was associated with a higher risk of subsidence.11,23,24 Our study provides further in vivo evidence to corroborate these findings and is the first to specifically look at cages placed from an anterior approach to the lumbar spine. Among patients who did not experience cage subsidence, the average center point ratio was 56.80%, corresponding to relatively central placement and thus allowing the periphery of the cage to leverage the strong outer ring apophysis. Conversely, patients who experienced cage subsidence had a more anterior average CPR of 61.28%, leading to more involvement the weaker central endplate region in the peripheral cage-bone interface. Additionally, although the degree of disc space distraction did not increase the risk for subsidence in this study, it is possible that attempting to overstuff the disc space with an oversized cage may have led to anterior malpositioning, particularly in patients with more advanced degenerative disease and stiffer anatomy. Based on these findings, surgeons should emphasize optimization of cage placement and sizing to decrease the risk of endplate compromise.
The relationship between BMD and endplate strength has been well established, with several biomechanical studies demonstrating a higher risk of endplate failure with lower BMD due to lower compressive strength under dynamic loading.19-21,25 Clinical studies have also found low BMD and osteoporosis to significantly increase the risk for subsidence in the context of several fusion procedures, including LLIF, posterior lumbar interbody fusion (PLIF), and transforaminal lumbar interbody fusion (TLIF).10,26-28 Recently, a study by Jones et al. used QCT technology to assess how the BMD of the cage footprint affected the risk for subsidence in LLIF, establishing a cutoff for volumetric trabecular BMD of 211.04 kg/m2, below which risk for subsidence was increased. 10 However, past studies did not assess the predictive value of BMD and osteoporosis on subsidence independent of cage positioning. Our findings suggest that off-center cage placement may contribute more significantly to subsidence, especially in osteoporotic endplates.
The results of this analysis demonstrated that age, BMI, and ASA score were all univariate predictors of subsidence following ALIF. These findings corroborate past studies which have suggested that these factors may contribute to subsidence following lumbar fusion procedures.8,10 Both older age and increased ASA status are known to contribute to poor bone structure and mechanical strength, thus resulting in a decline in load-bearing capacity.29,30 Additionally, obesity increases the risk for endplate compromise or even fracture due to an increased compressive axial load on the interbody cage.8,31,32
Patients who experienced subsidence more commonly were implanted with standalone ALIF cages without posterior pedicle screw instrumentation (87.18% vs 72.52%) and had rhBMP-2 added to the fusion construct (84.62% vs 70.99%), although the difference only trended towards significance. The use of pedicle screw instrumentation provides immediate rigid fixation, thus providing immediate stability to the operative segment and mitigating problematic continued motion which may impede successful fusion, lead to cage migration, or compromise the integrity of the endplate.33,34 However, these studies have demonstrated that pedicle screw fixation also increases the strain at adjacent segments, thus increasing the risk for adjacent segment degeneration. Despite the promotion of robust fusion masses with the use of exogenous rhBMP-2, past studies have reported complications of vertebral osteolysis, edema, and bone resorption with its use. This is believed to be the product of increased osteoclastic activity stimulated by rhBMP-2, typically occurring within months of surgery.35,36 This may lead to an associated increased risk for mechanical failure, including interbody device migration, subsidence, or endplate fracture. 36
Fusion of a mobile motion segment to an immobile spinal unit is known to alter the biomechanics of adjacent levels, leading to increased strain and mobility which may accelerate the progression of spondylosis.37,38 The results of this analysis demonstrated that interbody cage subsidence following ALIF may further increase the risk for pathology at adjacent lumbar segments, as the rate of subsequent adjacent level surgeries was significantly higher among patients who experienced subsidence. This may be attributed to subsidence-induced derangement of sagittal alignment, which has been shown to further increase the risk for adjacent segment degeneration.12,39,40 Interestingly, we did not observe any difference in the incidence of index revisions between patients with and without subsidence. However, this may be attributed to the overall low rate of revisions in the cohort, which were performed in only 7 of 144 patients (4.86%).
There are several limitations to this retrospective cohort study that must be considered. First, the surgeries were performed over a 13-year period by multiple surgeons at a single institution, thus increasing the potential for heterogeneity in procedural methods and postoperative protocols. Due to the wide timespan encompassed by this study, we were also unable to assess differences in patient-reported outcomes metrics (PROMs) between patients who did and did not experience interbody cage subsidence. This is attributed to inconsistencies in PROM collection at our Institution early in the study period. Additionally, a larger sized cohort would have increased the granularity of the data and of the significant findings. However, considering the minimum follow-up of 2 years, a sample size of 170 operative levels is sizeable, to our knowledge making this study the most robust analysis of risk factors for subsidence in ALIF to date. Furthermore, while we evaluated for certain patient factors that may have contributed to derangements in bone metabolism such as diabetes, renal dysfunction, and steroid use, we were unable to account for all potential variables that may have affected bony integrity. Moreover, while we considered osteoporosis as a binary surrogate for low bone mineral density (BMD), we were unable to quantitatively assess the relationship between BMD and subsidence. This is because quantitative assessments such as dual-energy X-ray absorptiometry (DXA) are not routinely obtained at our institution, and preoperative protocols for obtaining computed tomography (CT) scans vary by individual surgeons, precluding quantitative CT (QCT) analysis. However, quantitative assessments of BMD such as with QCT or CT osteoabsorbptiometry (CTOAM) and its interaction with cage position to affect subsidence may provide a valuable area for future study.
Conclusion
Subsidence following ALIF occurred at a rate of 22.94% of 170 operative levels evaluated. Significant univariate risk factors for interbody cage subsidence included older age, higher BMI, severe ASA, osteoporosis, and an anteriorly placed cage as measured via the cage center point ratio. On multivariate analysis, increased center point ratio remained the only significant predictor of subsidence, and a threshold of 56.98% was defined, above which there is an increased risk. Subsidence was associated with a significantly higher rate of subsequent surgeries at adjacent segments, although there was no difference in the rate of index-level revisions. Based on these findings, surgical technique should be focused on optimizing placement of the interbody cage and avoiding overstuffing of the disc space. Further investigation should validate these findings in an external cohort.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.