
Abstract
Study Design
Survey study.
Objectives
The purpose of this study was to characterize the utility of 3D printed patient specific anatomic models for the planning of complex primary spine tumor surgeries.
Methods
A survey of individual members of an international study group of spinal oncology surgeons was performed. Participants were provided a clinical vignette, pathologic diagnosis, and pre-operative imaging for three primary spinal oncology cases. Study participants provided a free text surgical plan for resection and were then presented an associated 3D printed model for each case and asked to re-evaluate their surgical plan.
Results
Ten spinal oncology surgeons participated in the study, representing nine institutions across five countries. Four of the surgeons (40%) made significant changes to their surgical plan after reviewing the 3D models, including sacrifice of an additional nerve root to obtain negative margins, sparing an SI joint that was originally planned for inclusion in the en bloc resection, adjusting the location of osteotomy cuts, changes to the number of surgical stages and/or staging order, and preservation of neurology that was originally planned for sacrifice. The overall impression of the 3D models was positive, with 90% of the participants stating they found the 3D model useful in developing a surgical plan.
Conclusions
Surgical planning for resection of primary spinal column tumors is challenging and time intensive. 3D printed patient specific surgical models may be an additional tool that can augment surgical planning and execution by improving the chance of accomplishing surgical resection goals and minimizing morbidity.
Introduction
Spinal column tumors can be technically challenging to resect given the complex surrounding anatomy. In addition, appropriate surgical management for primary spine tumors often calls for en bloc resection to provide the highest rate of disease-free and overall survival.1-5 This is difficult even for the most experienced spinal oncology surgeons, as evident by prior work showing planned surgical margins were achieved only 75% of the time among surgeons at high volume cancer centers. 6
A number of tools have been developed to assist with pre-operative planning and the successful execution of primary spinal column tumor surgery. Frameless stereotactic image guidance has been described for sacral and cervicothoracic chordomas to identify the appropriate location for osteotomy cuts and tumor-free dissection planes.7-9 Robotic guidance has been described for assistance with osteotomy cuts for en bloc resection of a sacral osteosarcoma. 10 3D-printed anatomic models are increasingly available for utilization in clinical practice, with production from raw materials (often plastics) of a highly precise, multicolor physical object constructed from patient specific CT and MRI images. 11 3D models have been found to reduce complication rates and OR times among craniofacial reconstruction procedures and have improved the planning for repair of complex congenital heart defects.12,13 In spinal deformity surgery, prior work has shown 3D models can decrease the duration of surgery, decrease estimated blood loss, improve the accuracy of pedicle screw placement, and decrease intraoperative x-ray exposure for the patient.14,15 In primary spinal column tumor surgery, models detailing the tumor location and surrounding anatomy have been described in limited case reports and case series, but further evaluation of the technology’s potential benefits is needed.8,11 The purpose of this study was to further explore the utility of a patient specific 3D-printed model for planning the surgical resection of primary spinal column tumor cases by surveying a group of international spinal oncology experts.
Methods
Data Source
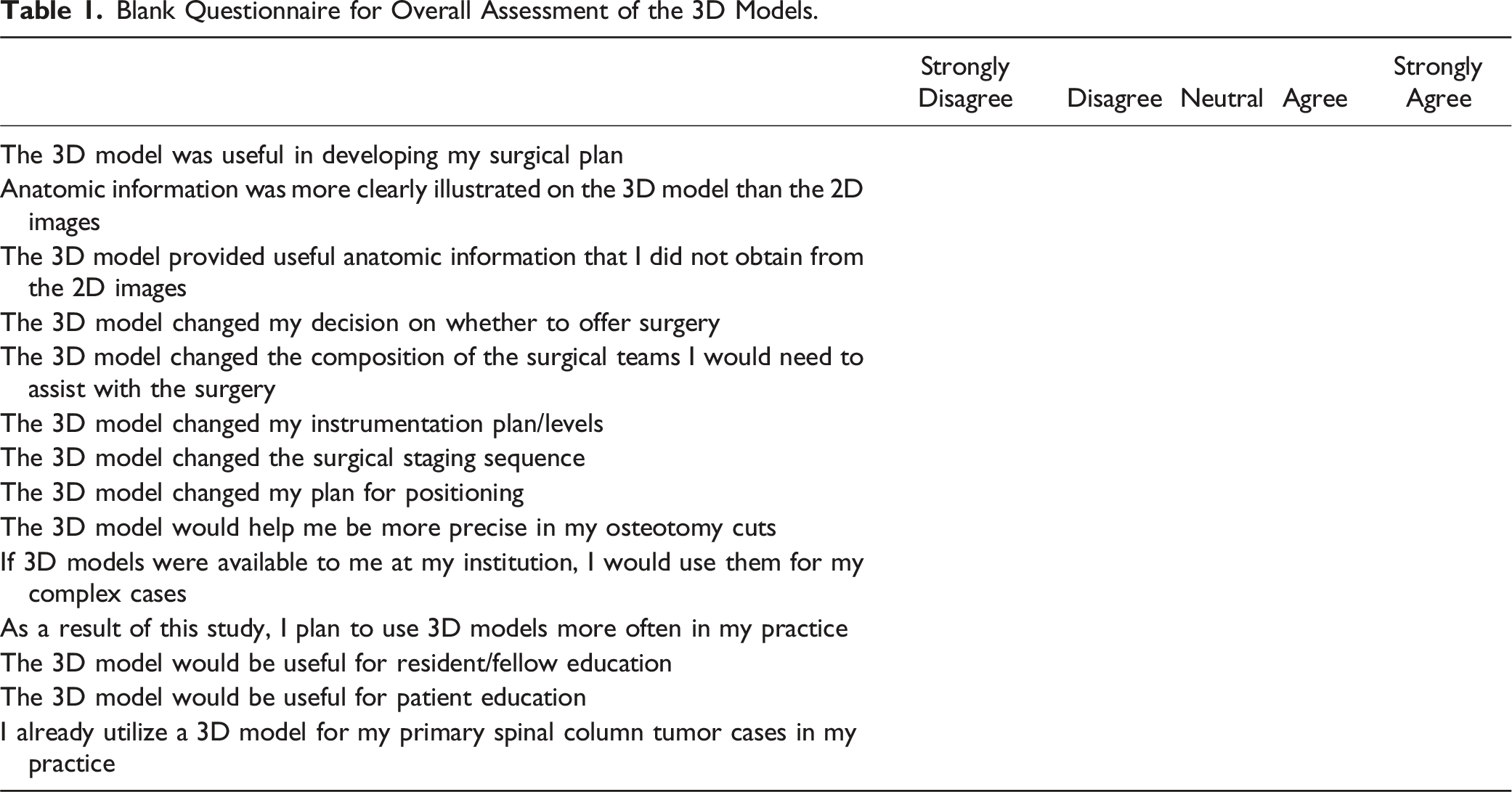
Blank Questionnaire for Overall Assessment of the 3D Models.
3D Models
CT and MRI images were used to segment the patient’s tumor and surrounding osseous anatomy utilizing the Materialise Mimics Innovation Suite software, version 26.0 (Leuven, Belgium). This software contains presets including bone, vasculature, muscle, and others, to segment required anatomy. These presets were used to threshold the ROIs and then manually corrected for accuracy. CT images are used to segment bony aspects of the tumor and MR images are used for soft-tissue components of the tumor. After the mask of regions of interest were created, tumor segmentation was reviewed by radiologists, computer-aided design (CAD) models were generated by a 3D printing engineer (KT) and reviewed by two senior surgeons (LDR, JEB). Approved CAD models were 3D printed using a Stratasys Objet350 Connex 3D printer which uses PolyJet technology (Stratasys Units, Eden Prairie, MN, USA). GrabCAD’s auto-orientation and print optimization tools were used to align the CAD models on the print bed. Clear materials were selected to 3D print bone and color materials for tumor, for better visualization of tumor extent in the bone.
Cases Presented to Participants
Case 1
A 50-year-old male presented with nine years of progressive left back and hip pain. He developed left L5 distribution numbness over the preceding two years. On exam he had decreased sensation to light touch in the left leg in an L4 and L5 distribution but was otherwise neurologically intact. Imaging and the associated 3D model demonstrated a large left sided spinopelvic mass with a cartilaginous cap involving the left SI joint and extending cephalad to the L3 spinal level (Figures 1 and 2). Biopsy proved this to be a grade 1 chondrosarcoma, likely arising from osteochondroma.
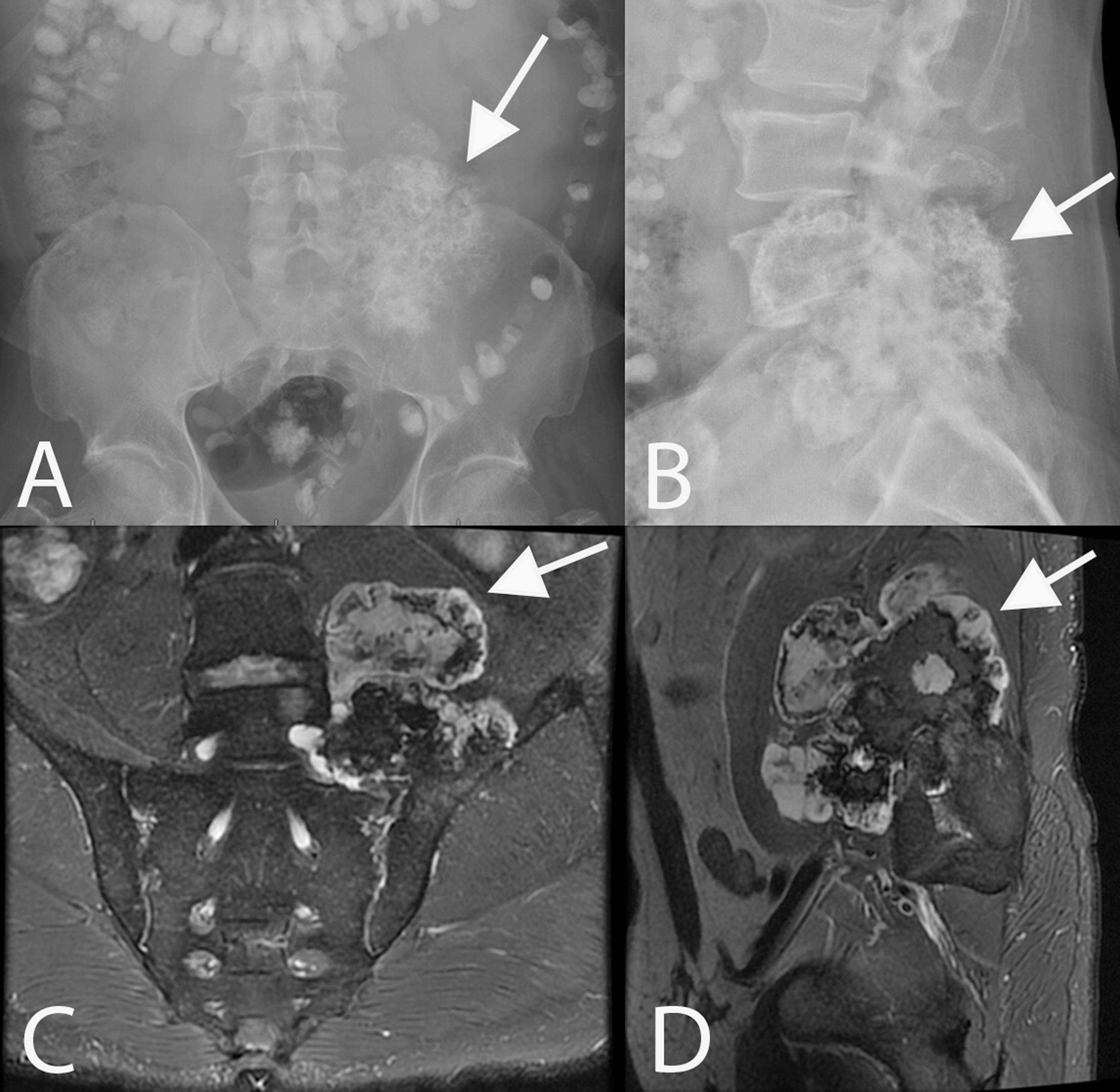
AP (A) and lateral (B) x-rays of the lumbar spine depicting a left sided spinopelvic chondrosarcoma involving the left sided sacrum, SI joint, pelvis, and extending cephalad to L3 (arrows). T2 fat-saturated MRI demonstrates the T2 hypointense mass with a T2 hyperintense cartilaginous cap on coronal (C) and sagittal (D) images.
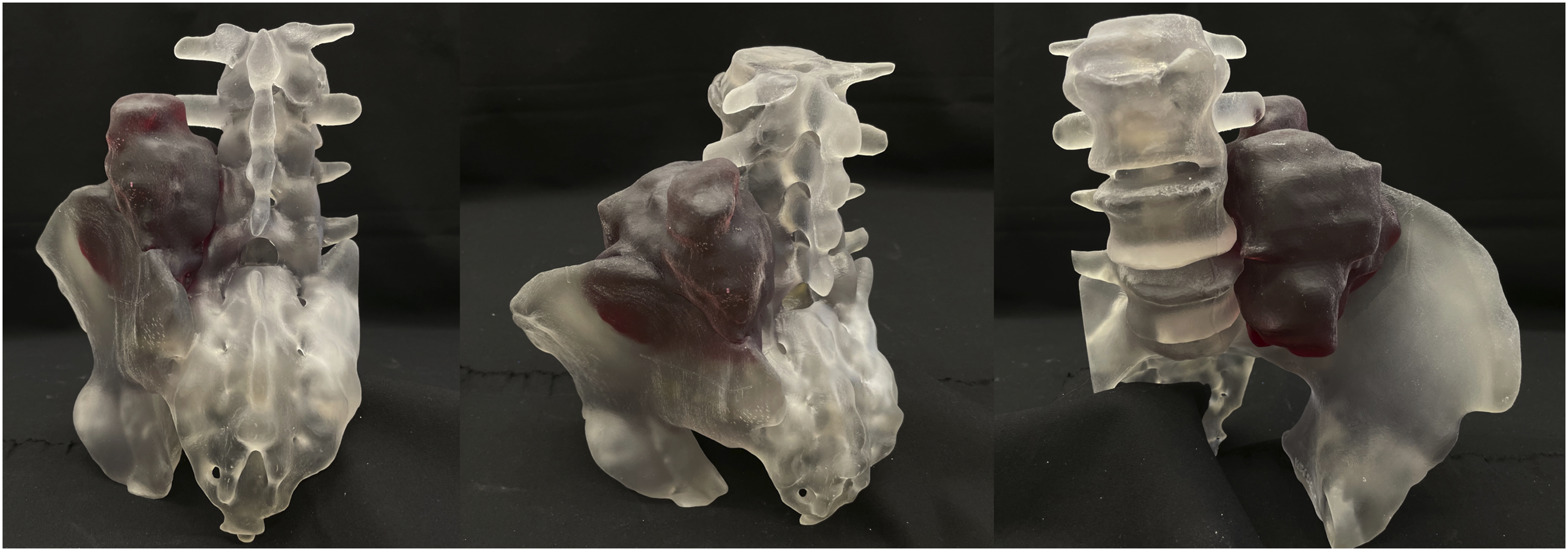
3D model provided to study participants depicting a left sided spinopelvic chondrosarcoma.
Case 2
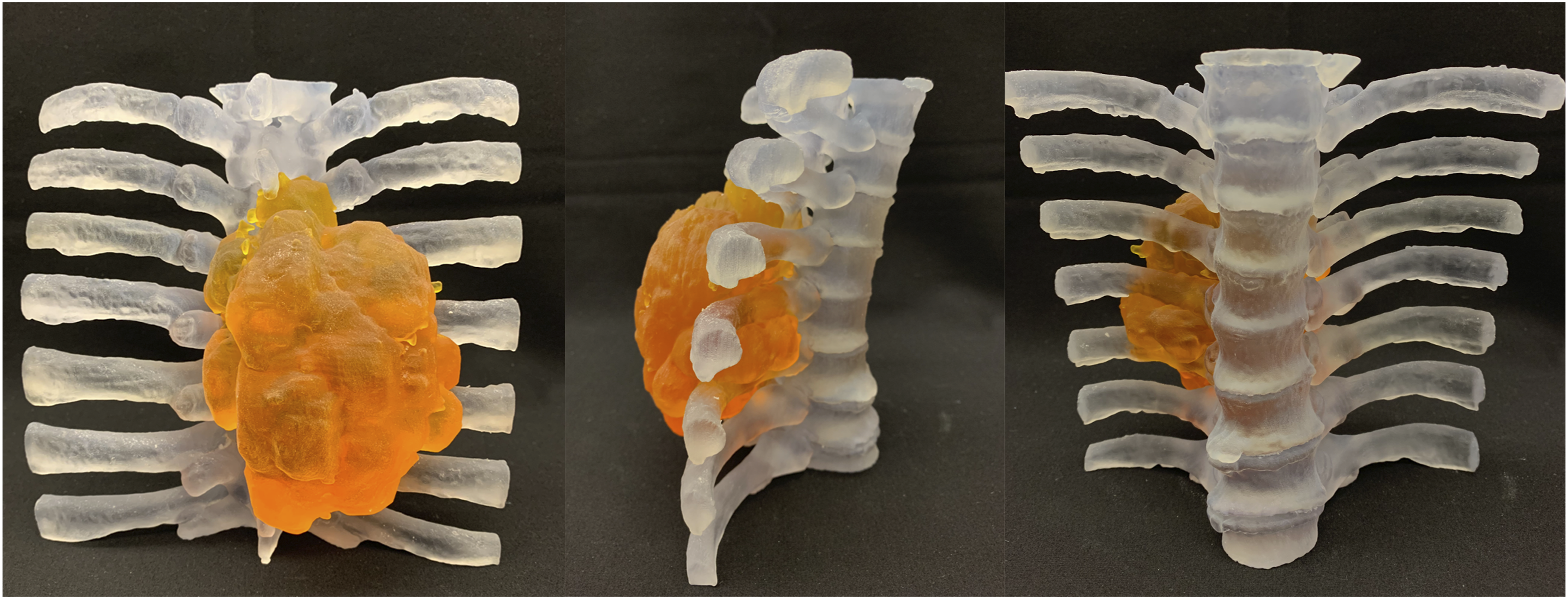
A 42-year-old male presented with 1 year of an enlarging posterior spinal mass with increasing discomfort. He denied any neurologic complaints and on exam he was neurologically intact. Imaging and the associated 3D model depicted a large posterior right sided cartilaginous capped lesion from T4-T8 with extension into the right chest wall through the 6th and 7th ribs (Figures 3 and 4). Biopsy proved this to be a grade 1 chondrosarcoma with a small focus of grade 2 present. Sagittal CT (A, B), sagittal fat-saturated MRI (C), and axial T2-weighted MRI (D) demonstrate a right sided calcified mass with a cartilaginous cap extending from T4 to T8 with extension through the 6th and 7th ribs into the chest wall (arrows) consistent with a chondrosarcoma. 3D model provided to study participants depicting a right sided thoracic chondrosarcoma.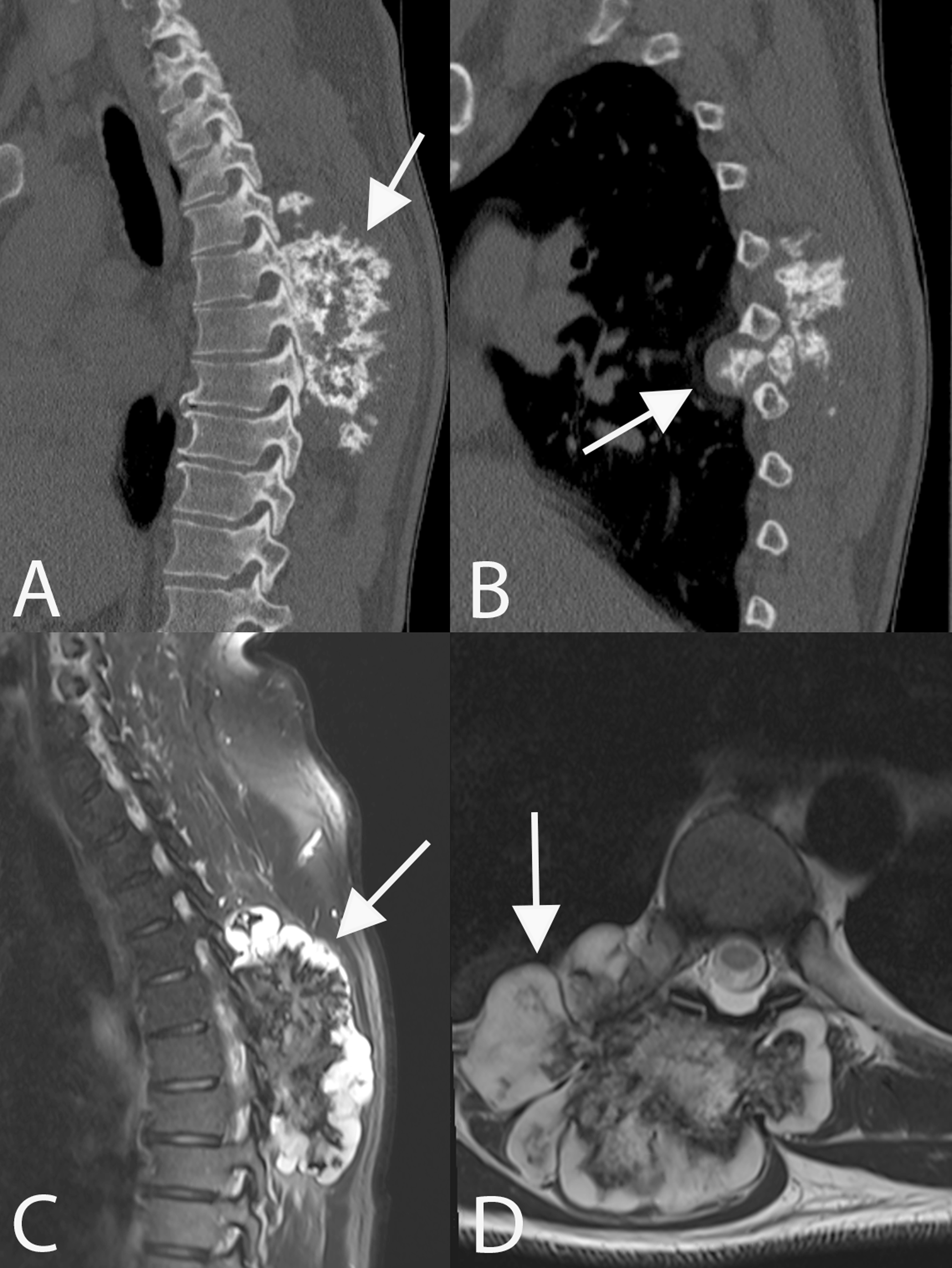
Case 3
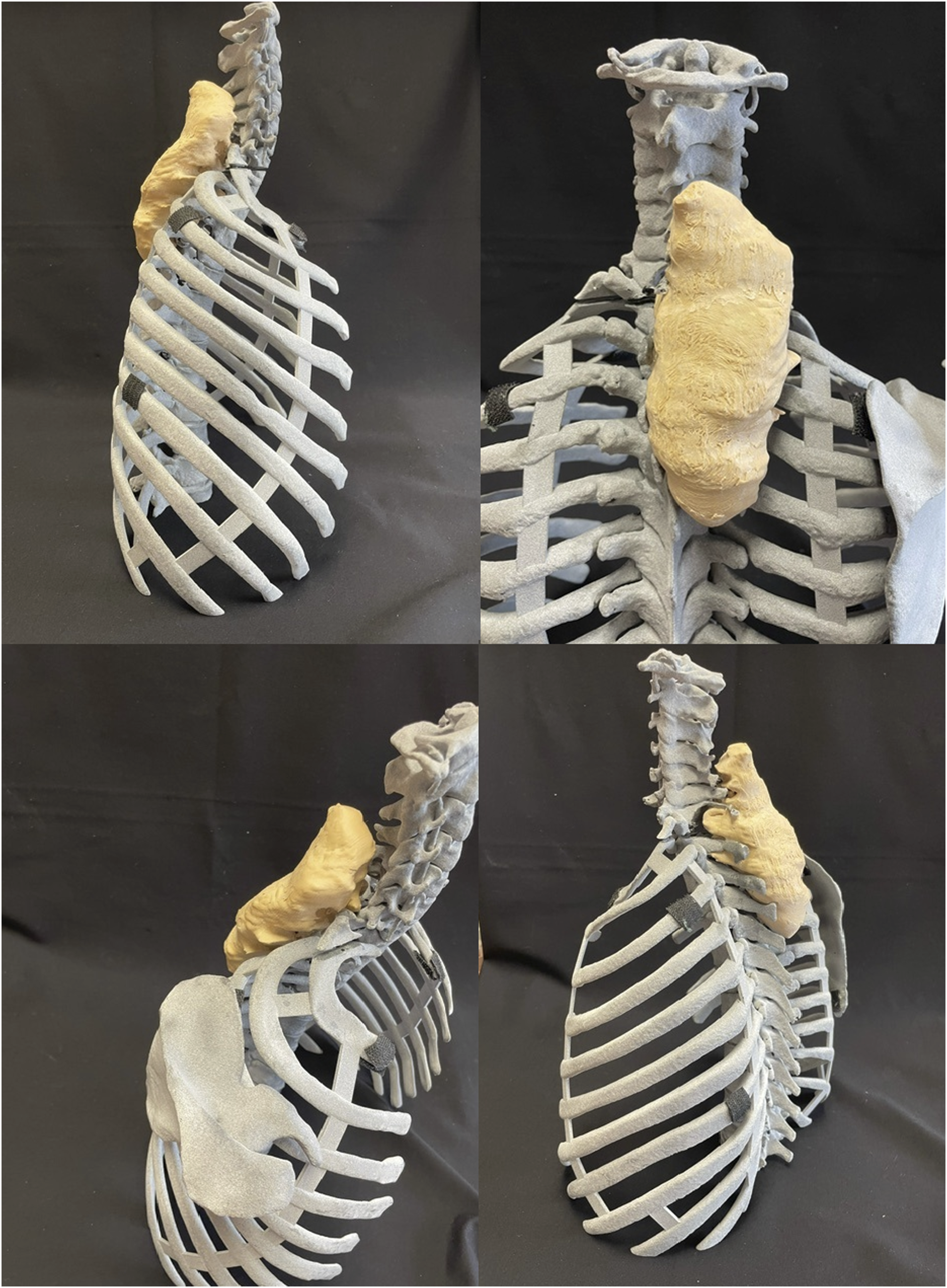
A 20-year-old male presented with 6 months of right sided upper thoracic back pain. He did not have any neurologic complaints and on exam he was neurologically intact. Imaging and the associated 3D model demonstrated a large right sided posterior spinal enhancing mass spanning C5 to T4 with extension into the pedicles and facets on the right side (Figures 5 and 6). Biopsy was consisted with a malignant peripheral nerve sheath tumor. Sagittal (A) and axial (B) CT demonstrate a non-calcified destructive lytic mass from C5 to T4 (arrows) with posterior element involvement and extension into the right sided pedicles and facets. Contrast enhanced sagittal (C) and axial (D) MRI images demonstrate the soft tissue mass (arrows) eccentric to the right side with posterior element involvement. Biopsy was consistent with a malignant peripheral nerve sheath tumor. 3D model provided to study participants depicting a right sided cervicothoracic malignant peripheral nerve sheath tumor.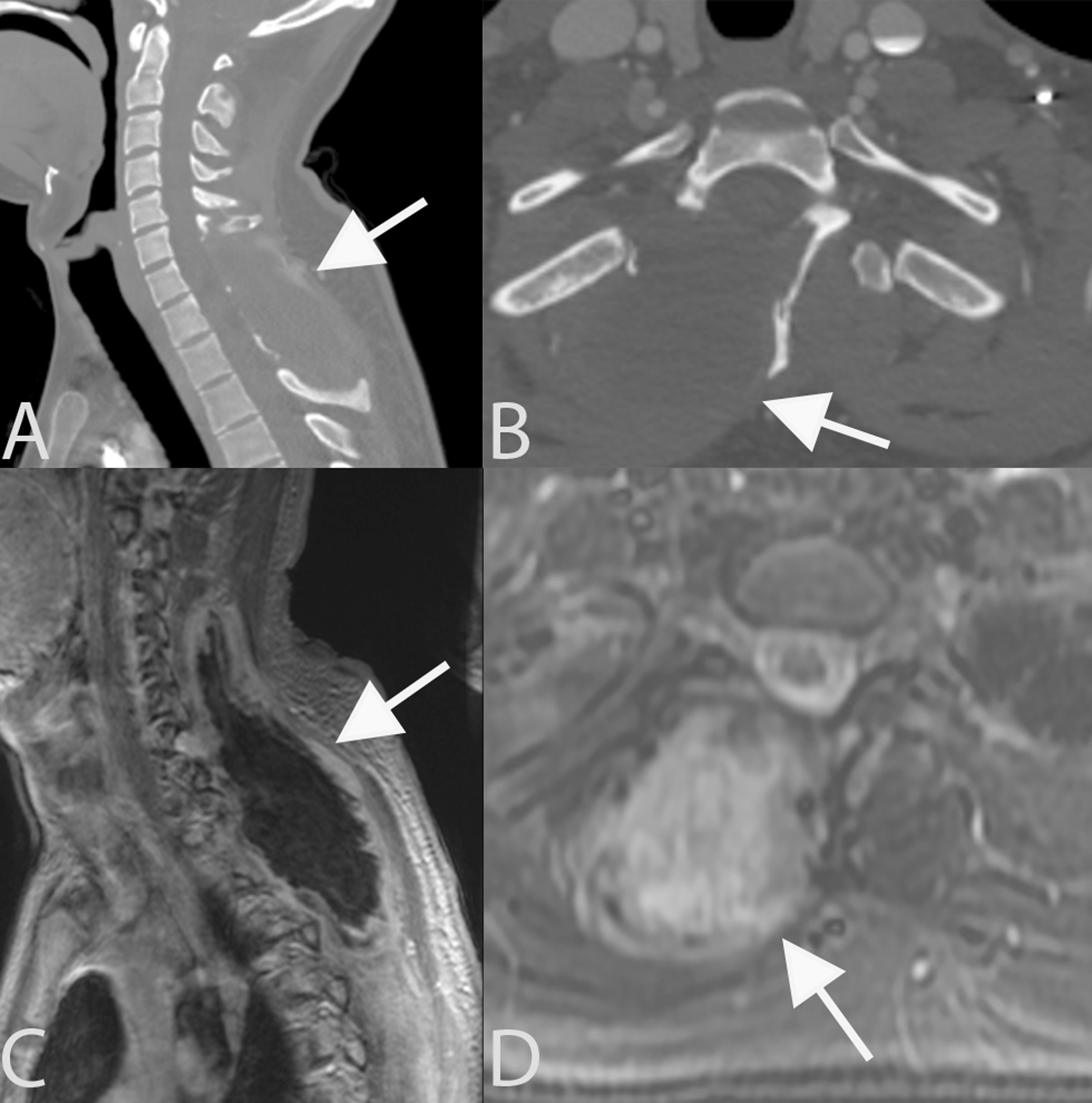
Results
Ten spinal oncology surgeons participated in the study, all with recognition as experts in the field. Participants provided international perspective, representing nine institutions across five countries. Years of experience ranged from <5 years (n = 2), 5-10 years (n = 2), 11-15 years (n = 4), 16-20 years (n = 1), and >20 years (n = 1). All the participants filled out 100% of the survey questions.
For case one, four participants (40%) changed their operative plan after studying the 3D model. Adjustments to the surgical plan included sacrifice of an additional nerve root to obtain negative margins and sparing an SI joint they originally planned to include in the en bloc resection. The case two questionnaire revealed three participants (30%) who changed their operative plan after analyzing the model. This included changes to the staging order (posterior followed by anterior), adjusting the location of the osteotomy cuts on 1 side of the tumor, and preservation of a nerve root that was originally planned for sacrifice. For case three, three participants (30%) changed their operative plan after studying the model. Adjustments to the plan included the number of stages from a two-stage anterior-posterior approach to a single all-posterior approach, and sacrifice of an additional nerve root to obtain negative margins.
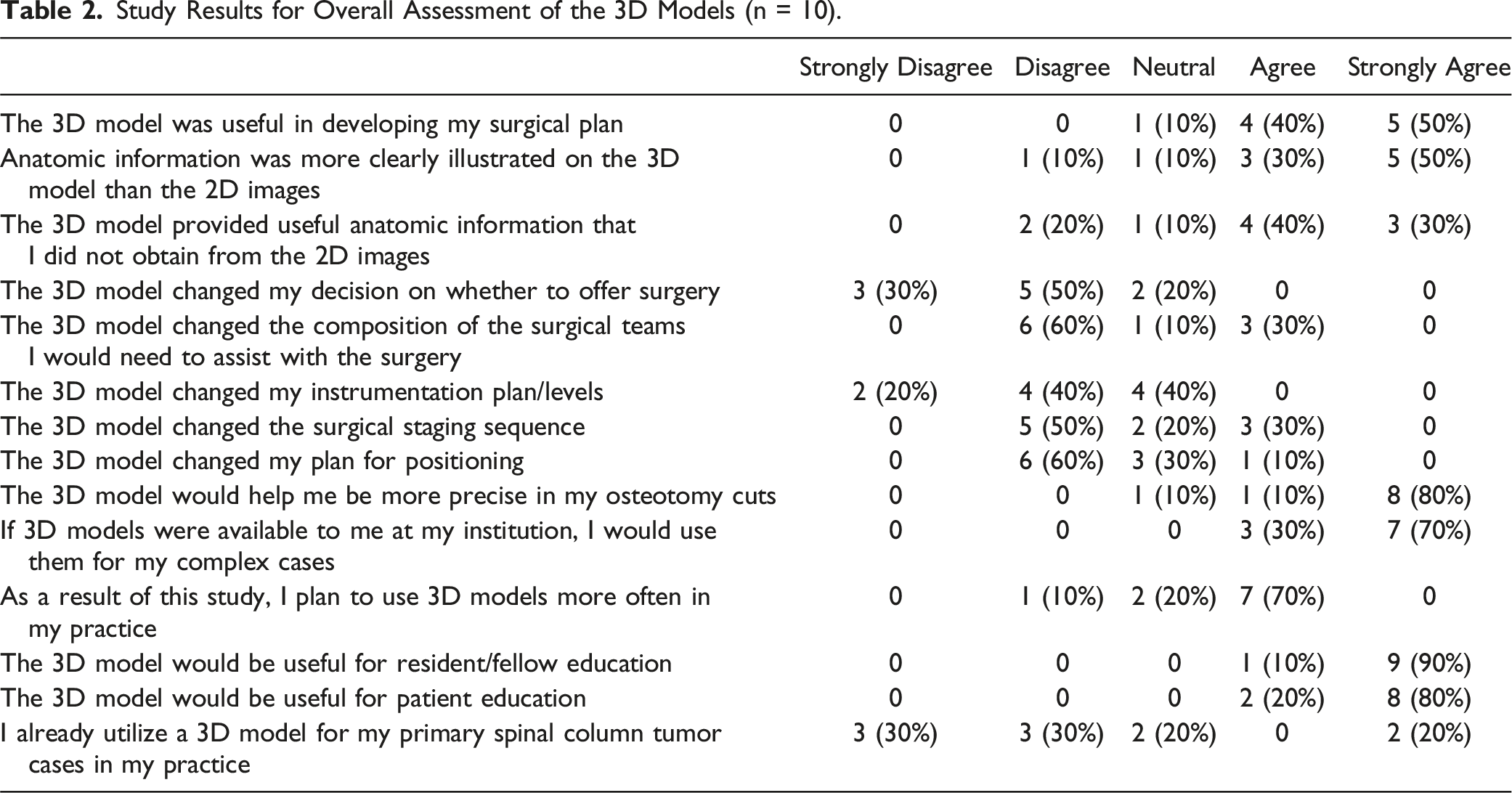
Study Results for Overall Assessment of the 3D Models (n = 10).
Discussion
Surgical resection of primary spinal column tumors can be a daunting task that involves a very time intensive planning process for every case. The surgical goals often entail negative margin en bloc resection while attempting to minimize neurologic consequences and maximize stability with a biomechanically durable construct. Given the high stakes for these patients, surgeons should employ every tool in their armamentarium to achieve the goals of surgery while minimizing morbidity. 3D printed anatomic models may be of value during this planning process, as evident by the vast majority (90%) of spinal oncology surgeons surveyed in this study stating they found the 3D model useful in their surgical planning. The potential for an increase in the utilization of 3D models was evident by the survey respondents stating they would all utilize the models if available at their institution despite only a minority (20%) currently doing so. The survey results also support the use of the 3D models not only to potentially improve patient care, but also to improve trainee and patient education.
Prior studies reporting the use of 3D printed anatomic models for spinal oncology cases is limited to case reports and small case series.8,11,16-19 Wang et al analyzed 41 total en bloc spondylectomy cases, for which 19 cases had a 3D printed model utilized and 22 did not. They found a higher rate of negative margin resection among the 3D anatomic model group (79%) compared to the non-3D model group (55%). 18 Leary et al reported a case series of nine patients where a 3D printed model was utilized pre-operatively for surgical planning and patient education, and seven were also referenced intra-operatively. The surgical teams found the 3D models helpful for surgical planning pre-operatively and intra-operatively for creating appropriate osteotomy cuts and appreciating the relationships between the tumor and key anatomic structures. 11 Jug et al had a 3D model printed pre-operatively in a four year old patient with post-laminectomy kyphosis following medulloblastoma resection to practice fixation strategies “in vitro” before the surgery, resulting in a successful operation. 19 Rogers-Vizena et al reported 20 patients who underwent craniofacial reconstruction procedures without a 3D model and nine who had a patient-specific 3D model printed. They found 3D model patients had a lower rate of complications, a reduction in OR time, and an associated cost savings that may offset the cost of 3D model production. 12 In a prospective international multicenter study on the utility of 3D models for planning the repair of 40 complex congenital heart defects, 48% of planned surgeries were significantly changed after reviewing the 3D model, including converting four of the cases that were originally deemed non-operative to operative cases with successful biventricular repair in all four cases. 13 In our own study, 40% of surgeons made significant changes to their surgical plan after reviewing the 3D models, including the number of surgical stages, neurology to be sacrificed or preserved, preservation of an SI joint, and/or osteotomy cut locations.
In addition to the clinical advantages, prior studies have investigated the educational utility of patient-specific 3D models for patients and trainees. Patients from Leary et al. reported improved understanding of the extent of tumor involvement and what was to be accomplished during surgery when allowed to visualize the 3D models pre-operatively. 11 Hu et al analyzed trainee understanding of spinal tumor cases by randomizing 36 residents or fellows to a group with or without a 3D model in addition to typical 2D images for surgical planning. They were then examined on their surgical plan and the anatomy relevant to the tumor. The students who had access to the 3D model had improved ability to describe tumor involvement with paraspinal structures, including the surrounding vasculature (P < 0.05). Most participants also reported favorable responses in regard to the 3D printed model’s ability to improve the trainees understanding of anatomic structures, surgical planning, and enhancement of interest and confidence. 20 A similar study assessed residents and the utility of a 3D model in assisting the planning of solid organ cancer surgery. They found the 3D model provided a statistically significant benefit in terms of identifying tumor location, tumor invasion, tumor-vessel relationships, and ability to collaborate with multidisciplinary colleagues. 21
Limitations of this study include self-selection bias in that not all participants of the study group participated and potentially those who participated were more likely to find the 3D models useful due to pre-existing interest. We also did not make the study results anonymous, potentially leading to social desirability bias where respondents were more likely to respond favorably. We also cannot prove that 3D models will improve patient care based on the results of this survey study. Future studies are warranted that evaluate clinical outcomes tied to the use of 3D printed anatomic models, which may require collaboration across disciplines and medical centers. Two potential barriers to implementing 3D models into clinical practice include cost and availability, which could be overcome by evidence that supports 3D models as an important tool for improving patient care in certain complex circumstances.
Conclusions
Planning and executing a surgical strategy for primary spine tumors can be a challenging task given the complex anatomy surrounding spinal column tumors in combination with, often, a goal for negative margin en bloc resection. 3D models can be a valuable tool when planning these surgeries, as evident by responses from the experts in spinal oncology surgeons surveyed in this study. When adjusting surgical boundaries for en bloc resection, the potential to impact patient care is significant, including the preservation of uninvolved neurology and important biomechanical structures while avoiding inadvertent tumor transgression. Future studies are warranted to determine if implementation of 3D models in a spinal oncology practice translates to improved clinical patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.