
Abstract
Study Design
Systematic Review
Objective
3DP technology use has become increasingly more common in the field of medicine and is notable for its growing utility in spine surgery applications. Many studies have evaluated the use of pedicle screw placement guides and spine models in adult spine patients, but there is little evidence assessing its efficacy in pediatric spine patient populations. This systematic review identifies and evaluates the current applications and surgical outcomes of 3-Dimensional Printing (3DP) technology in pediatric spinal surgery.
Methods
A search of publications was conducted using literature databases and relevant keywords in concordance with PRISMA guidelines. Inclusion criteria consisted of original studies, and studies focusing on the use of 3DP technology in pediatric spinal surgery. Studies with a focus on adult populations, non-deformity surgery, animal subjects, systematic or literature reviews, editorials, or non-English studies were excluded from further analysis.
Results
After application of inclusion/exclusion criteria, we identified 25 studies with 3DP applications in pediatric spinal surgery. Overall, the studies found significantly improved screw placement accuracy using 3DP pedicle screw placement guides but did not identify significant differences in operative time or blood loss. All studies that utilized 3D spine models in preoperative planning found it helpful and noted an increased screw placement accuracy rate of 89.9%.
Conclusions
3DP applications and techniques are currently used in pre-operative planning using pedicle screw drill guides and spine models to improve patient outcomes in pediatric spinal deformity patients.
Keywords
Introduction
As advances in both 2D and 3D imaging technology have rapidly evolved in the field of medicine, there are still many limitations in anatomical visualization abilities that hinder the pre-operative planning process. The emergence of novel 3-dimensional printing (3DP) technology has been expanding its applications in the field of healthcare. Since the 1990s, 3DP, also commonly known as rapid prototyping, additive manufacturing, or solid free form technology, has been used for pre-operative planning, patient, and resident education, manufacturing surgical guides, as well as patient specific implants.1,2
3DP utilizes 3D digital imaging data (eg from computerized tomography or magnetic resonance imaging) which is subsequently sliced into 2D cross sections that are 3D printed in layers. These slices are layered on top of each other and fused into a full prototype.1,3–5 This method of additive manufacturing is more efficient in terms of both cost and material use compared to other methods such as subtractive manufacturing, which consists of the removal of excess material in order to fabricate the final product. 5 While there are various techniques within the realm of 3DP, there are 3 main techniques that are most popular in medical applications.1,5 Stereolithography (SLA) involves a light curable resin which is cured prior to the addition of successive layers via photopolymerization to create a final polymerized prototype. Selective Laser Sintering (SLS) utilizes an electron beam or laser focused energy source to sinter a fine powder bed. The powder may consist of nylon, stainless steel, and titanium alloys, which may make it suitable for implantation in patients. Lastly, Fused Deposition Modeling (FDM) involves heated polymer layered with a computer-controlled extrusion nozzle. While FDM is more economically effective and have more ease of use, SLA and SLS are more commonly used in medical applications due to the ability of the material to withstand sterilization without damaging the models. The low melting point of FDM material makes it more challenging to be used in a surgical environment.1,3–5
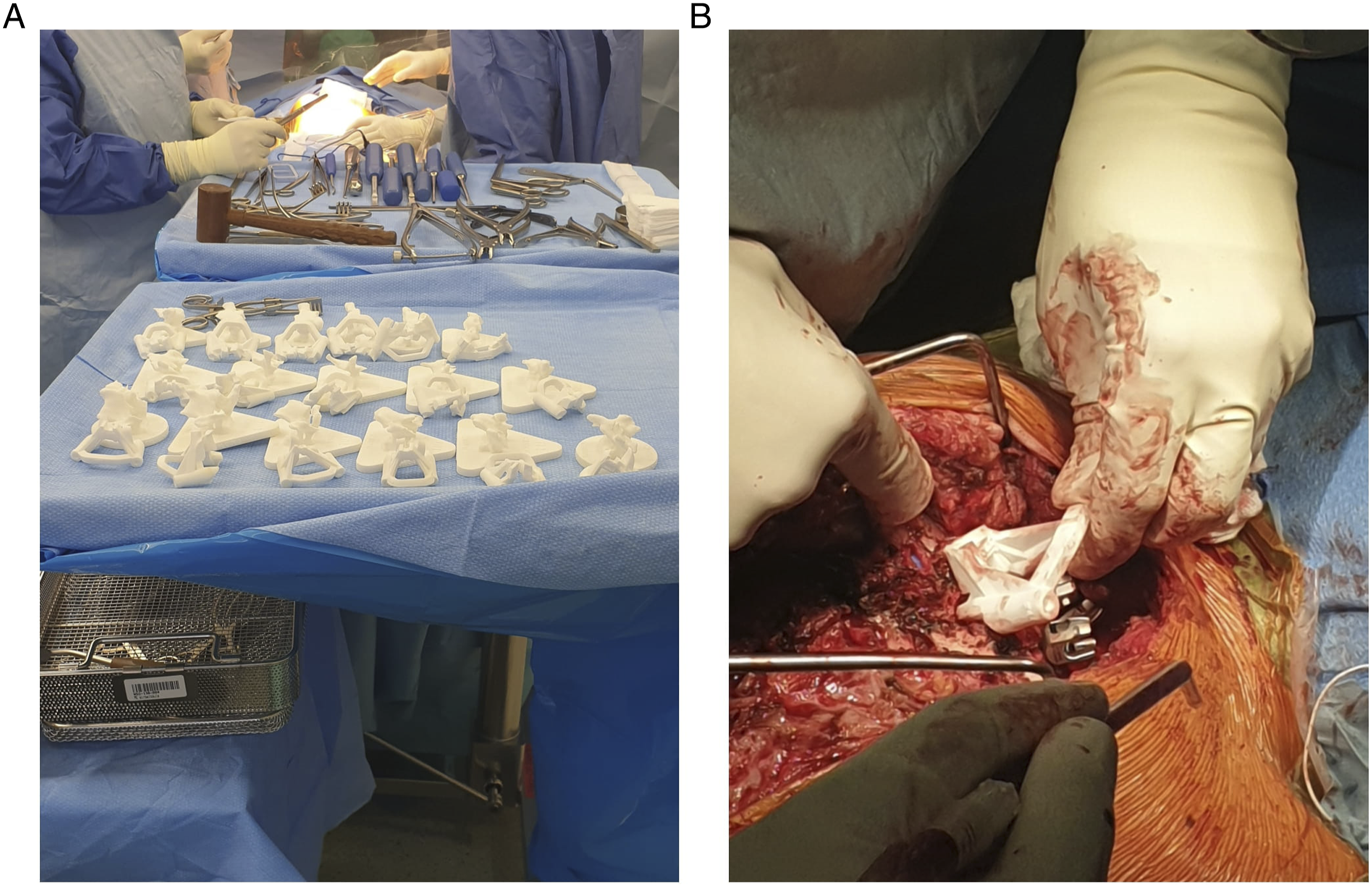
3DP applications have been particularly emphasized in spine surgery due to the complex anatomy and variable anatomy in deformity patients
6
(Figure 1, Figure 2). A 3D model can help spine surgeons to visualize anatomy such as pedicle morphology and neurovascular structures, resulting in improved patient outcomes
3
While the application of 3DP templates to guide pedicle screw placement and pre-operative planning have been described and evaluated in the literature for adult populations, there have been limited reviews examining the efficacy of 3DP applications in pediatric populations.2,3,6 Given the rapid advent of 3DP, increasing surgical applications, and adaptation of this novel technology, the purpose of this current systematic review is to identify all applications as well as the effectiveness of 3DP applications specifically in pediatric patients with spinal pathology. 3-dimensional spine models utilized for preoperative planning. (A) Posterior view of pediatric 3D printed spine model. (B) Lateral view of pediatric 3D printed spine model. 3-dimensional pedicle drill guides for intraoperative planning. (A) 22 3D printed pedicle screw guides for each vertebral level requiring correction. (B) Application of pedicle screw guide in vivo for pedicle screw placement and guidance. Photos courtesy of Medacta International.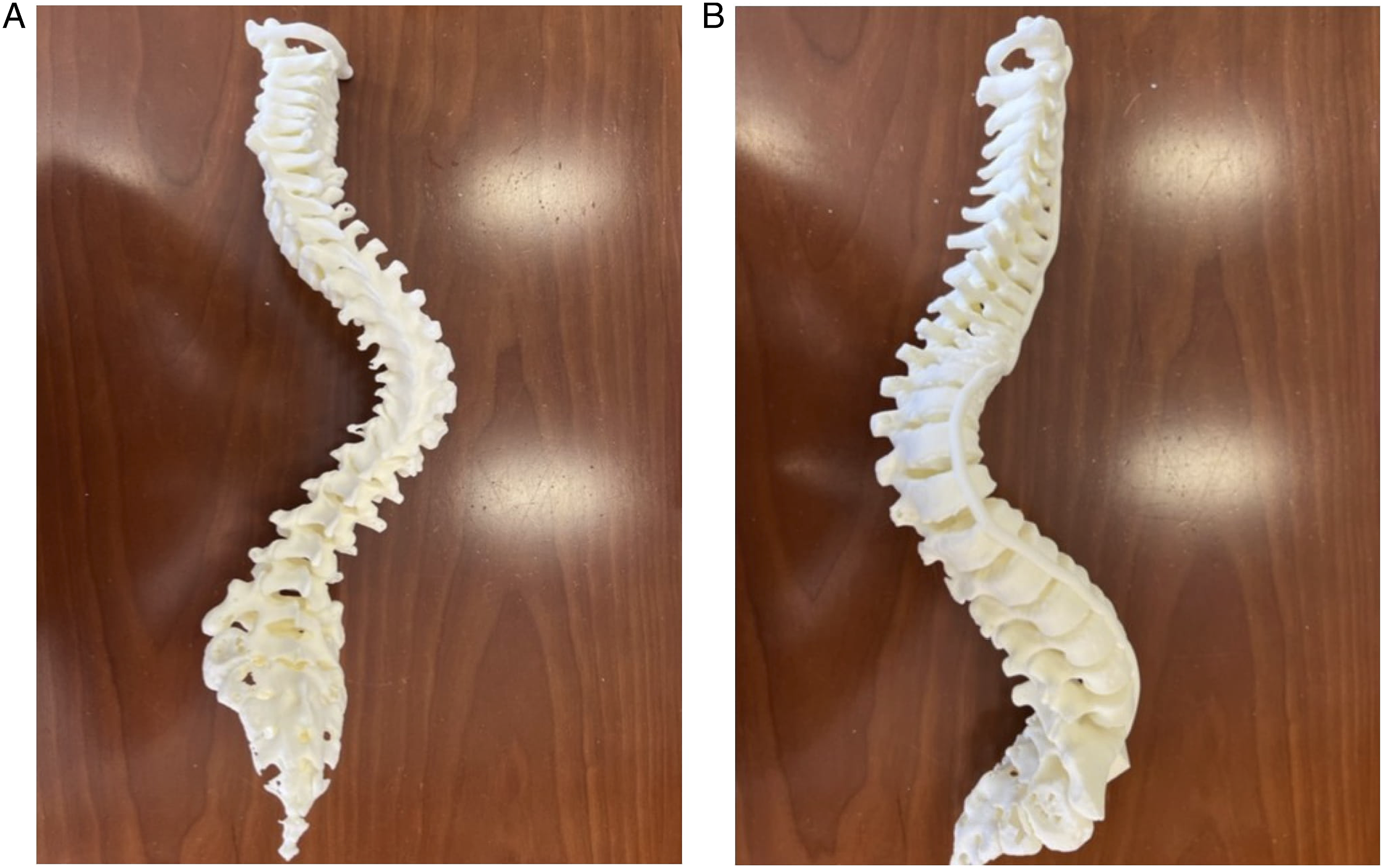
Methods
Search Strategy and Information Sources
A search of publications through August 2022 was conducted using EMBASE, PubMed, Ovid Medline, and World of Science databases in compliance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Search terms included the following keywords along with Boolean operators (OR, AND) to maximize relevance and sensitivity of the searches: “adolescent,” “pediatric,” “3D printing,” “three-dimensional printing,” “rapid prototyping,” “additive manufacturing,” “scoliosis,” “idiopathic scoliosis,” “kyphosis,” “spinal deformity,” “spine malformation,” “spine surgery,” “spondylolysis,” and “spondylolisthesis.”
Eligibility Criteria
Inclusion criteria included all studies evaluating the utility and efficacy of 3DP technologies in the pre-operative planning and treatment of pediatric (defined as ≤ 18 years old) spinal pathology (eg scoliosis, kyphosis, spondylolisthesis, etc.). Studies were excluded if they did not utilize 3-Dimensional Printing for treatment of spinal pathology, studies with adult patient populations or samples with a mean age >18 years old, animal studies, non-English studies, systematic reviews, and editorials. There were no strict parameters on the level of evidence for each study and timing of the study.
Study Selection
Article titles and abstracts were screened initially by 2 reviewers. After exclusions based off titles and abstracts, potential full-text journal articles were screened further based on the inclusion criteria. References for included articles were also reviewed and evaluated to ensure all eligible articles were included in the analysis. Each included article was given a level of evidence rating based off the Oxford Center for Evidence-Based Medicine Levels of Evidence. 7
Data Extraction
A database of the studies analyzed was compiled with the following information: author, publication year, country of origin, study design, level of evidence, study duration, blinding of the study, number of involved institutions, 3DP method, production materials, production cost and time, pathology being treated, 3DP clinical application, primary and secondary outcome measures, result, sample size, average patient age, percent male patients, and when applicable: number of screws used, screw accuracy rate, operative duration, blood loss, fluoroscopy utilization/exposure, percent deformity correction, and reported intraoperative or postoperative complications. Articles were sorted into 2 different non-mutually exclusive categories based on application of 3DP: pedicle screw drill guides and pre-operative planning using models. Descriptive statistics were used to summarize relevant important results, trends, and findings from the reviewed articles. Surgical treatment outcomes were analyzed using weighted averages of the patient groups with and without the use of 3DP across all relevant studies. 3DP costs and materials and production type were both qualitatively and quantitatively assessed.
Results
Search Results and Study Selection
Our search parameters resulted in 609 articles, of which 87 articles were duplicates and subsequently removed. The remaining 522 articles were screened using the inclusion and exclusion criteria based on the article titles and abstracts. 37 articles were fully reviewed, of which 25 satisfied the full inclusion and exclusion criteria set, totaling in a data set inclusive of 596 patients with a mean age of 12.7 years. (Figure 3.) The 11 articles were excluded due to non-3DP applications, or an adult population (mean age >18 years.) PRISMA flow diagram of included studies.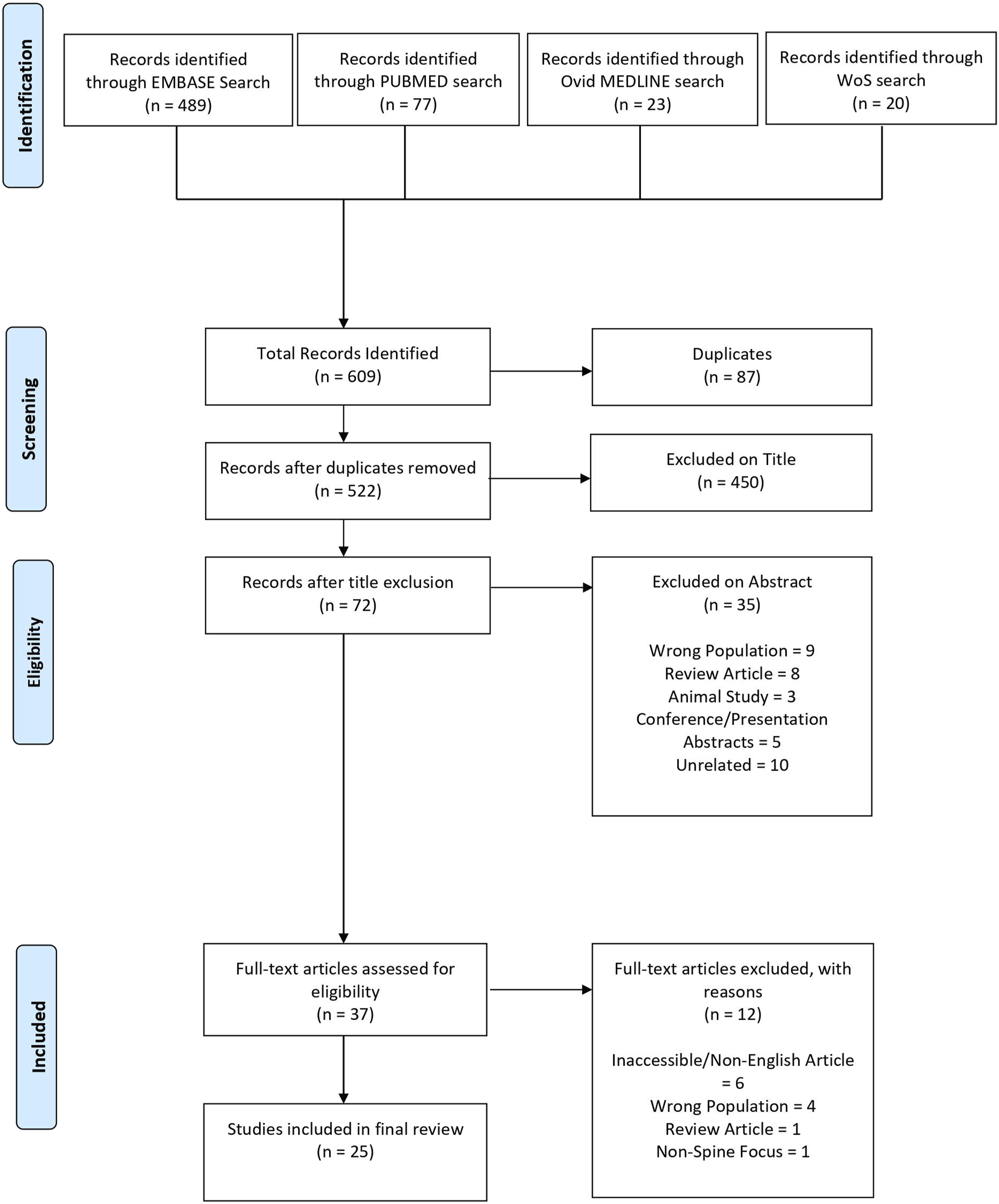
Applications
Screw Drill Guides
Summary of 3DP Screw Drill Template Studies.
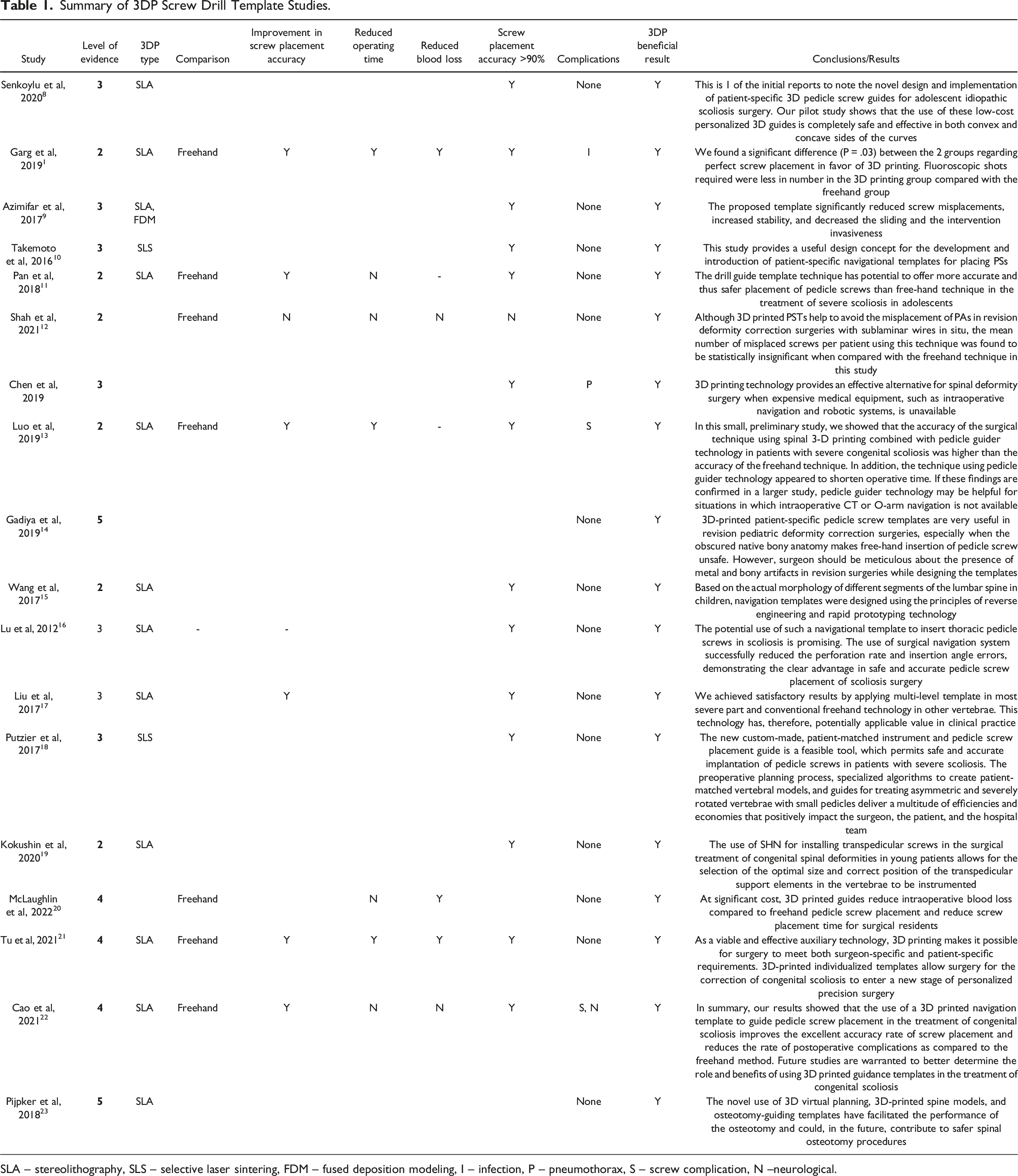
SLA – stereolithography, SLS – selective laser sintering, FDM – fused deposition modeling, I – infection, P – pneumothorax, S – screw complication, N --neurological.
Pedicle screw placement accuracy was assessed in 15 studies. In these studies, 2,125 pedicle screws were placed using 3DP in 222 patients with an average accuracy rate of 93.9%. Eight of these studies compared the screw placement accuracy rate with 3DP screw drill guides against the freehand technique, and 7 of these studies found a significant improvement in screw accuracy in the 3DP drill guide vs the freehand cohorts.11–13,15,17,21,22,24 Across these studies, the average pedicle screw placement accuracy in the 3DP drill guide cohort was 92.7% (991 screws across 105 patients) and significantly higher compared to the free-hand control cohort of 80.8% (1014 screws across 94 patients) (P = .03).
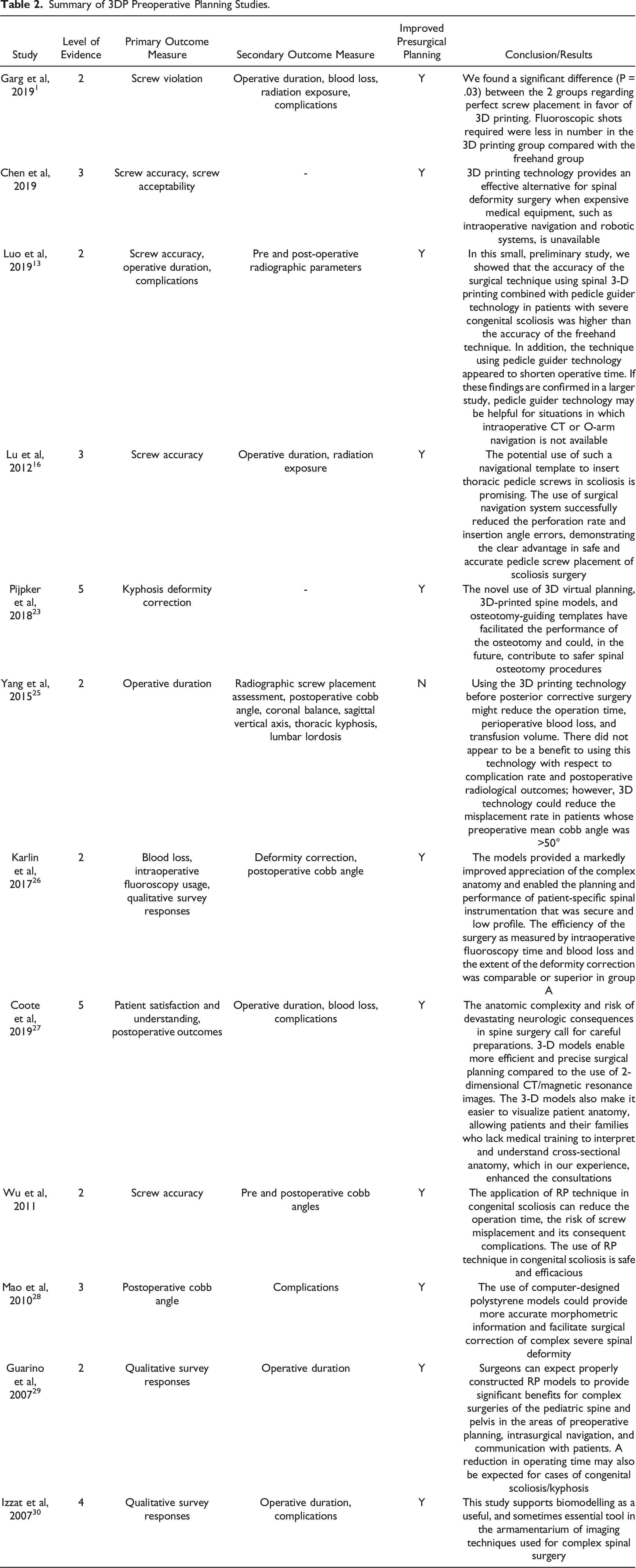
Preoperative Planning
Summary of 3DP Preoperative Planning Studies.
3-Dimensional Printing Process
Summary of 3DP Production Type, Materials, Time, and Cost.
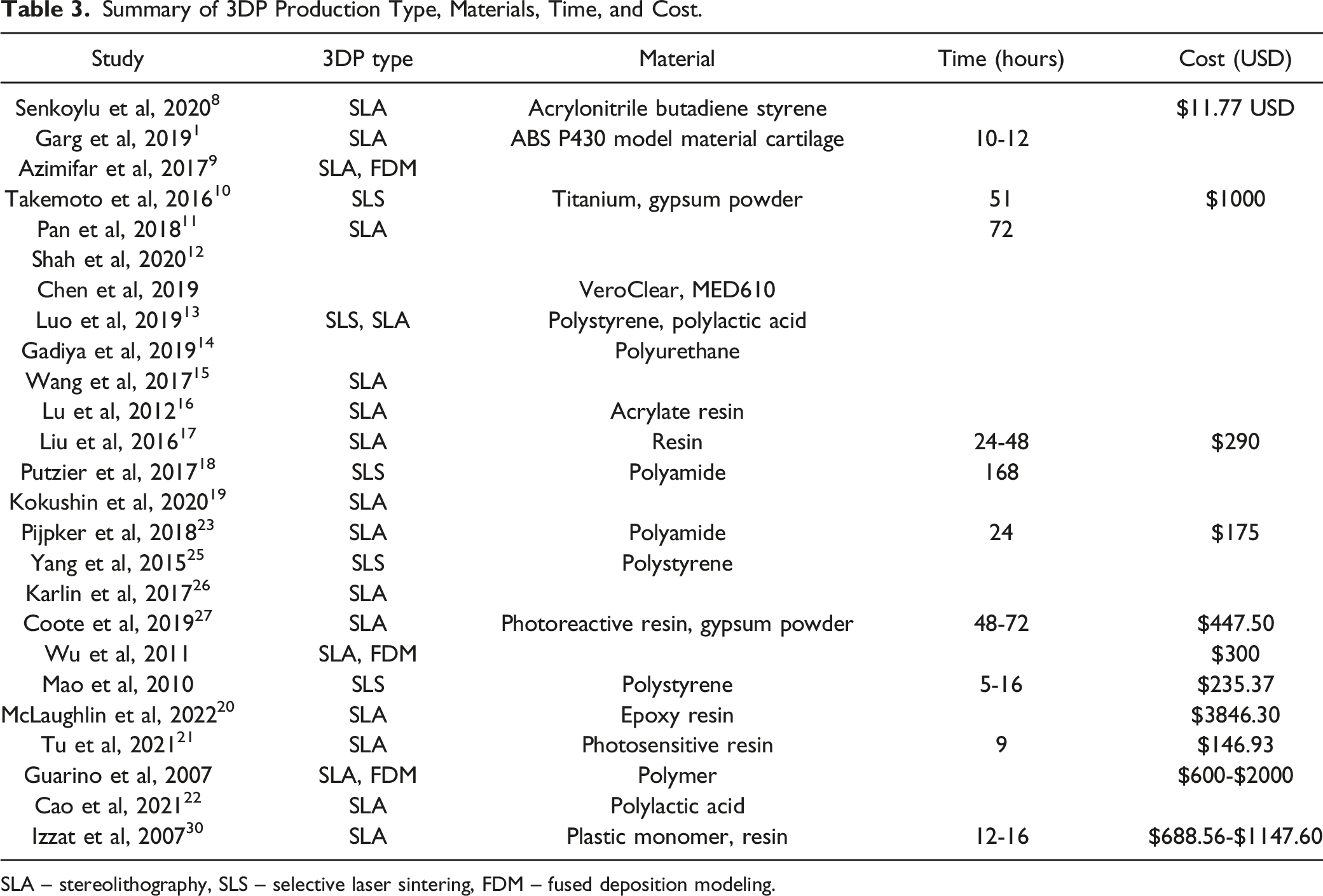
SLA – stereolithography, SLS – selective laser sintering, FDM – fused deposition modeling.
Discussion
This systematic review evaluated all current global studies that utilized 3DP applications in the surgical treatment of pediatric spinal pathology. Across the 25 reviewed studies, 596 patients with a mean age of 12.7 years were evaluated internationally across various countries, including India, China, EU, and USA. The spinal deformities evaluated included kyphosis, cervical stenosis, and various types of scoliosis (congenital scoliosis, adolescent idiopathic scoliosis, neuromuscular scoliosis) among other pathologies. The most common applications of 3DP in this pediatric spinal cohort included 3DP pedicle screw drill guides and preoperative models.3,6
In these studies, free hand pedicle screws are noted to have a fairly high breach rate, especially in patients with significant deformity.3,24 While various navigation techniques have emerged to aid in improved screw placement accuracy, they require extensive training and knowledge to maneuver and have increased costs for the equipment.6,16,24,25 Thus, customizable 3DP pedicle screw drill guides offer a novel approach to improve screw placement accuracy that is tailored to the patient’s unique anatomy, especially in pediatric patients with severe spinal deformities, such as congenital scoliosis or adolescent idiopathic scoliosis. Furthermore, they may also decrease intraoperative radiation exposure, which is particularly important in a pediatric population.8,16,31
The majority of studies reviewed showed that 3DP pedicle screw template use in pediatric patients significantly increased screw placement accuracy compared to the free-hand technique. 3PD pedicle screw templates are also reported to decrease operative time as well as intraoperative and postoperative complications in these procedures, but this was not significant across the cohort of all studies. The use of 3DP guide templates resulted in favorable outcomes, such as increased accuracy and decreased complications, blood loss and operative time.11,16–18 This was attributed to increased accuracy in first time placement of the pedicle screws and decreased need of intraoperative fluoroscopy and adjustment of the screw tract.11,13 Luo et al also suggested that the decreased operative time most likely led to reduced risk of infection and postoperative complications since operative duration itself is an independent risk factor for postoperative complications in patients who have recently undergone spine surgery.6,13
The biggest limitations cited for use of the drill guides were having to facilitate direct bone contact with the template. For this, surgeons had to strip the soft tissue and fat surrounding the start point on the vertebra in order to prepare a clean bone surface to ensure proper stability and fit with the template.16,24 Azimifar et al drafted a medium invasive protocol that suggested utilizing transparent templates for real time verification of accuracy that were fit to the patient’s vertebrae at the anterior and posterior articular processes, which would require less soft tissue removal as opposed to the traditional fixation at spinous and transverse processes. They also utilized multi-level vertebral templates, as opposed to templates for each individual vertebrae, and demonstrated a screw accuracy placement rate of 94%. 9
Preoperative Planning
More than 50% of the reviewed studies utilized 3DP spine models during pre-operative planning. These models provided great utility in visualization of the anatomical and bony landmarks necessary to predict pedicle screw lengths, positioning, and placement13,23,28,31,32 Additionally, Chen et al discussed how 3DP spine models were an effective alternative when intraoperative and robotic navigation methods are unavailable. Luo et al also concurred, citing limitations such as increased radiation risks for both the physician and patient, increased economic burdens, and longer, more complicated operative durations with CT navigation, O-arm navigation, and even robotic navigation26,32 Most of these studies also reported that there were benefits of increased screw accuracy placement rates and decreased operative times, costs, and fluoroscopy time resulting in overall improved outcomes.13,24,26,32 The optimization of the surgical process was attributed to a clearer understanding of pathology, detailed preoperative planning with less references to other imaging resources, and more efficient screw implantation and positioning.26,30,32 1 study led by Yang et al demonstrated that while the 3DP spine models resulted in decreased operative times and blood loss, there was no significant difference in screw placement accuracy rates unless the preoperative Cobb angle was >50°. However, they attribute this difference to the increased complexity of the larger deformity cases, for which the 3DP spine model provided more utility as compared to cases where the deformity was not as severe (<50°). 25 In pediatric patients with severe spinal deformities that illustrate a preoperative Cobb angle >50°, 3DP spine models can help guide preoperative planning by optimizing intraoperative approach, decreased radiation in pediatric patients, as well as reducing the need for revision surgeries or complications in these populations.24,25
3-Dimensional Printing Process
Reports of production costs and times were limited in the reviewed studies, where only a fraction of the studies had included a complete breakdown of these variables. 3DP production ranged from 5 hours to 168 hours and the material cost ranged from $11.77 to $2000 USD. The materials used also varied across studies: titanium, gypsum powder, polystyrene, polyurethane, polyamide, resins, polylactic acid and may have contributed to the wide range in production costs. While the material may not have as much impact in certain 3DP applications (ie spine models), the choice of materials may be pertinent in intraoperative applications. Takemoto et al noted that typical nonmetallic 3DP material is approved for use in the human body for approximately 24 hours, but that when these materials are used intraoperatively that residual debris may accumulate from drilling and other maneuvers. 10 Hence, titanium would be safer for more long-term use and is also more stable, allowing for better guided pedicle screw insertion. Their accuracy rate was 98.6%, 1 of the highest out of all reviewed studies. However, their costs were also 5 times the cost of guides fabricated with polyamide. 10 There are limits with plastic monomers and polymers though as well. For example, these guides may be warped upon intraoperative use, or sterilization prior to surgery.3,10
Limitations
Despite its growing popularity, there are still limitations regarding the data presented on the efficacy and use of 3DP models and screw guides. As most 3DP studies have been performed in adult populations, there were few studies with large sample sizes and high level of evidence study designs that focused on primarily pediatric populations. Most studies reviewed were smaller scale studies with no control group comparisons, or case reports utilizing 3DP applications as experimental technology. In order to receive a broader understanding of the scope of 3DP applications, larger scale, controlled studies are needed.
In terms of the challenges surrounding the expansion of 3DP models and guides in preoperative surgical planning, some of the largest barriers include time and cost. As discussed earlier, the time to print the 3D guide or model depended heavily on the available resources at the institution, and the variability in production methodology (Table 3). Likewise, costs varied widely, and the burden of the cost was sometimes the responsibility of the patient.25,32 This cost was offset in most cases by a decrease in operative costs due to the preoperative planning, which lessened operative durations and decreased intraoperative and postoperative complications.6,30 Another limitation that studies noted was the steep learning curve and necessary training required to master the technology. In a survey among surgeons from Guarino et al, many noted that a hindrance to using 3DP techniques was the training needed to master the equipment and software, which could be time consuming and challenging.6,15,29
Future Directions
Overall, as there is increased expansion, affordability, and evolution of 3DP technology, there is potential for its applications to grow in medicine and healthcare. In both spine surgery and pediatric orthopedic surgery, routine use of 3DP technology will allow for optimization of the preoperative planning process and provide accurate and tailored surgical care. Applications may also expand to include increased use of 3DP implants, especially those with more biocompatibility as development of and access to novel 3DP materials becomes more readily available. 6
Conclusions
3-Dimensional Printing applications and techniques are becoming more commonly used in the treatment of pediatric spinal deformities, with the majority of applications being pre-operative planning using pedicle screw drill guides and spine models. Most of the studies reviewed have shown that the use of 3DP screw guide templates and 3DP spine models have shown to significantly improve screw placement accuracy rates compared to non-3DP control patient cohorts. While costs and production times remain variable, the growing accessibility of 3DP has the potential to streamline these factors and create a broad scope of applications for the future as the field continues to evolve.
Supplemental Material
Supplemental Material - Three-Dimensional Printing Applications in Pediatric Spinal Surgery: A Systematic Review
Supplemental Material for Three-Dimensional Printing Applications in Pediatric Spinal Surgery: A Systematic Review by Prerana Katiyar, Venkat Boddapati, Josephine Coury, Benjamin Roye, Michael Vitale, and Lawrence Lenke in Global Spine Journal
Footnotes
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Prerana Katiyar. The first draft of the manuscript was written by Prerana Katiyar and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prerana Katiyar, Venkat Boddapati, Josephine Coury, and Benjamine Roye have no financial interests. Michael Vitale receives royalties from Zimmer Biomet, is a consultant for NuVasive and Stryker, is on the board of directors for Children’s Spine Foundation and Pediatric Orthopedic Society of North America, and has current grant/research support from Scoliosis Research Society, Children’s Spine Foundation and Pediatric Orthopedic Society of North America, and the Orthopedic Scientific Research Foundation. Lawrence Lenke has received royalties from Medtronic, consulting fees from Medtronic and Acuity Surgical, and is a reviewer for the following journals: Spine, The Spine Journal, European Spine Journal, AO Spine Deformity Knowledge Forum, JBJS, GSJ, ISSG, Spine Deformity.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Submission Statement
This study does not have any prior or duplicate submissions or publications elsewhere of any part of the work. No funding sources, including from the National Institutes of Health; Wellcome Trust; or Howard Hughes Medical Institute, were utilized to complete this study.
Ethics Statement
This study utilized national, de-identified data and is exempt from IRB review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.