
Abstract
Study Design:
Systematic review.
Objectives:
This current systematic review seeks to identify current applications and surgical outcomes for 3-dimensional printing (3DP) in the treatment of adult spinal deformity.
Methods:
A comprehensive search of publications was conducted through literature databases using relevant keywords. Inclusion criteria consisted of original studies, studies with patients with adult spinal deformities, and studies focusing on the feasibility and/or utility of 3DP technologies in the planning or treatment of scoliosis and other spinal deformities. Exclusion criteria included studies with patients without adult spinal deformity, animal subjects, pediatric patients, reviews, and editorials.
Results:
Studies evaluating the effect of 3DP drill guide templates found higher screw placement accuracy in the 3DP cohort (96.9%), compared with non-3DP cohorts (81.5%, P < .001). Operative duration was significant decreased in 3DP cases (378 patients, 258 minutes) relative to non-3DP cases (301 patients,272 minutes, P < .05). The average deformity correction rate was 72.5% in 3DP cases (245 patients). There was no significant difference in perioperative blood loss between 3DP (924.6 mL, 252 patients) and non-3DP cases (935.6 mL, 177 patients, P = .058).
Conclusions:
Three-dimensional printing is currently used for presurgical planning, patient and trainee communication and education, pre- and intraoperative guides, and screw drill guides in the treatment of scoliosis and other adult spinal deformities. In adult spinal deformity, the usage of 3DP guides is associated with increased screw accuracy and favorable deformity correction outcomes; however, average costs and production lead time are highly variable between studies.
Keywords
Introduction
The use of 3-dimensional printing (3DP) technology, also known as additive manufacturing or rapid prototyping, is rapidly expanding in health care and has the potential to improve patient care and reduce costs. It offers the ability to create prototypes of customizable shapes from 3D software renderings using a variety of different materials. Across surgical specialties, 3DP technology has been shown to be beneficial in aiding surgical planning, enhancing patient education and resident training, improving intraoperative navigation, and reducing operative durations. 1,2
Three-dimensional printing technology involves using computed tomography (CT) or magnetic resonance imaging (MRI) to create a digital 3D model that is then sliced into 2D sections, which are physically produced in layers by a 3D printer and eventually fused into a final model. 3 Different materials are used in the printing process—stereolithography (SLA) most commonly involves the use of polystyrene or resin, whereas selective laser sintering (SLS) employs a focused energy source on various materials such as nylon, titanium, or stainless steel to sculpt a final model. 3 Another 3DP type, fused deposition modeling (FDM), creates layers using a heat-softened polymer. For complex surgical procedures such as spinal surgery, 3DP offers valuable preoperative planning and close anatomic guidance to avoid damaging nerves and vessels, which may improve patient outcomes. 4 Three-dimensional printing has shown utility across various surgical specialties, including spine surgery, in preoperative planning, anatomic visualization, custom prosthetic design, procedural rehearsal, and even as an educational tool for training and doctor-patient communication. 1,2,5 -15
New applications of 3DP in spine surgery have been described in the literature and their efficacy has been studied, but many studies are often single-institution and underpowered and questions remain about variable costs, production times, materials, and patient outcomes, especially in applications for treating adult spinal deformity. 7,16 The purpose of this review is to identify and evaluate all current applications of 3DP in the literature for the treatment of adult spinal deformity and to assess surgical outcomes with and without the utilization of 3DP.
Methods
Search Strategy and Information Sources
A comprehensive search of publications (up to November 2019) was conducted using the EMBASE, Medline, and PubMed databases in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Search terms included the following keywords or MeSH terms: “3D printing,” “three-dimensional printing,” “rapid prototyping,” “additive manufacturing,” “scoliosis,” “idiopathic scoliosis,” “degenerative scoliosis,” “kyphosis,” “spinal deformity,” “spine malformation,” and “spine surgery” Boolean operators (OR, AND) were also used to maximize the sensitivity of the search.
Eligibility Criteria
Inclusion criteria consisted of original clinical studies, including studies that evaluated the feasibility and utility of 3DP technologies in the planning and/or treatment of adult scoliosis and other spinal deformities, studies evaluating the use of 3DP implants in spinal surgery, and studies with patients who present with scoliosis or other spinal deformities such as kyphosis in adult patients (>18 years old). Exclusion criteria consisted of studies that do not evaluate the use of 3DP technology in spine surgery, studies with nonscoliosis or nonkyphosis patients, animal subjects, or pediatric patients, non-English studies, inaccessible articles, reviews, and editorials. No limits were placed on level of evidence or timing of the study, since the majority of the reviewed studies were published within the past 10 years.
Study Selection
Article titles and abstracts were screened initially by 2 reviewers, and full-text articles were subsequently screened based on the selection criteria. The studies were rated by their level of evidence, based on the Oxford Centre for Evidence-based Medicine Levels of Evidence. 17 The reference list of all articles included in the study was also carefully assessed to identify any potential studies that may have been missed by our initial search strategy. Discrepancies in inclusion studies were discussed and resolved by consensus.
Data Extraction
A database was collected from all included studies with the following information: publication author and publication year, country of origin, study design, level of evidence, study duration, blinding of the study, number of involved institutions, 3DP technology type, production materials, production cost and time, pathology being treated, 3DP clinical application, primary and secondary outcome measures, result, sample size, average patient age, percent male patients, number of screws used (if applicable), screw accuracy rate, operative duration, blood loss, fluoroscopy utilization/exposure, preoperative and postoperative Cobb angles, percent deformity correction, reported intraoperative or postoperative complications, and any additional pertinent findings from the study. Articles were sorted into 3 different, non–mutually exclusive categories based on 3DP use/application (screw drill guides, presurgical planning, and training/education). Descriptive statistics were employed to summarize important findings and results from the selected articles and to describe trends in 3DP technology applications, materials, costs, and clinical outcomes. Post-surgical outcomes with and without the use of 3DP technology were assessed using weighted averages of patient cohorts across different studies, and with the use of Student’s t test or Fisher’s exact test for statistical significance testing. Significance was defined as P < .05. Data summarizing 3DP technology types, materials, costs, and production times were presented using simple averages, frequencies, and proportions.
Results
Search Results and Study Selection:
Using our predefined search terms resulted in 204 articles, of which 92 duplicate articles were removed. The remaining 112 articles were screened by title and abstract according to inclusion and exclusion criteria. Ultimately, there were 39 articles included for full review, of which 32 studies (with a total of 703 patients) met full inclusion and exclusion criteria (Figure 1). Seven articles were excluded during the full-review process because they either violated exclusion criteria or did not have a focus on 3DP or spine surgery.
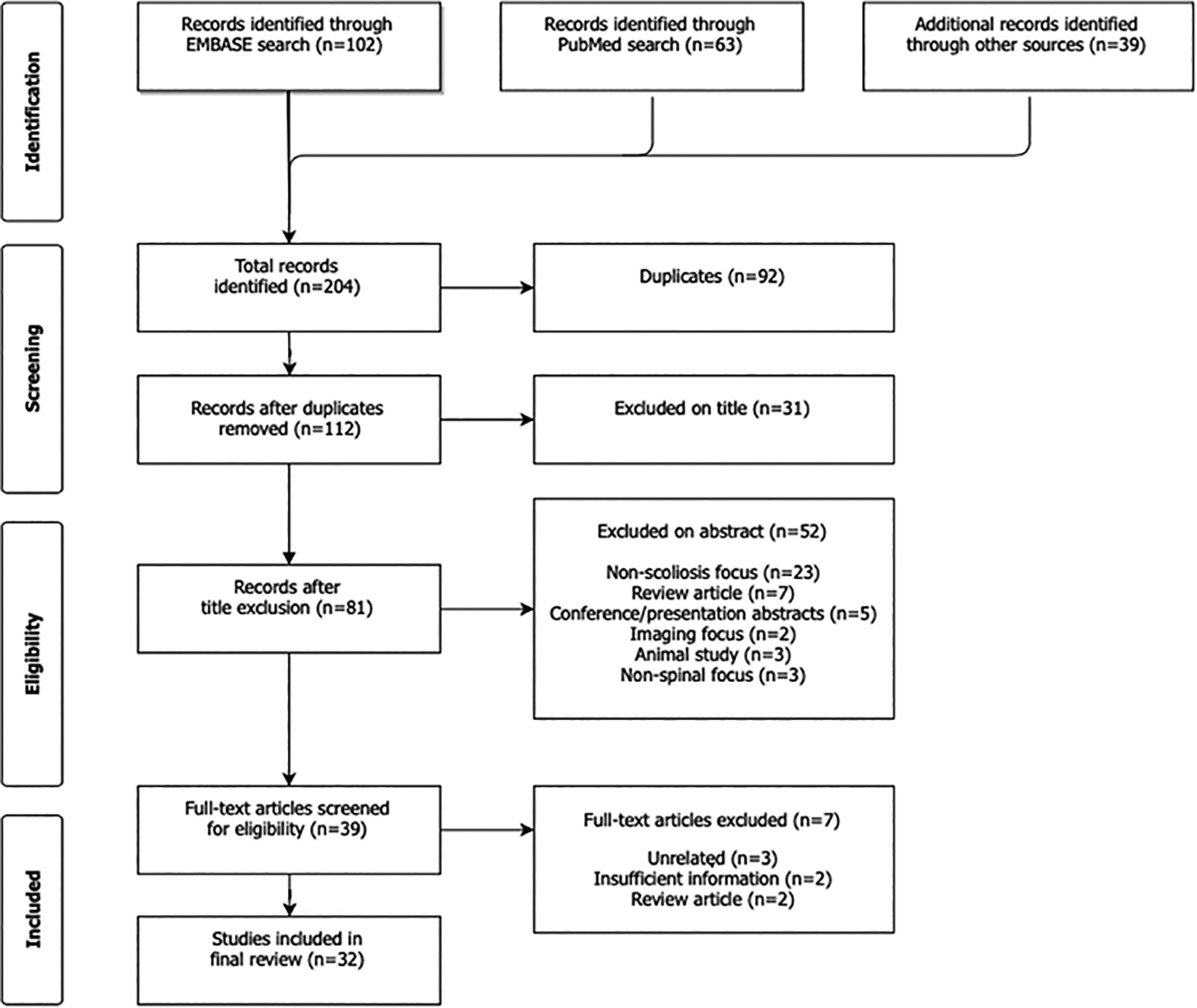
PRISMA flow diagram of included studies.
Applications
Screw Drill Guides
A total of 22 out of 32 reviewed studies (68.8%) evaluated the efficacy of 3DP drill guide templates in surgical treatment of spinal deformities (Table 1, Figure 2) Nine of eleven studies that assessed operative duration as an outcome variable found significantly decreased operative durations when 3DP screw drill guides were used, compared with cases in which no 3DP guides were used (free-hand, navigation-based, or imaging-based screw placement). Six studies compared 3DP guides with free-hand screw placement, 3 studies compared with navigation-based, and 2 studies compared with fluoroscopic guidance. Ten studies did not specify a comparison technique. Across these studies, the average operative duration decreased from 272 minutes in cases without a 3DP screw guide (301 patients) to 258 minutes with a 3DP screw guide (378 patients), which was statistically significant (P < .05). Three studies also reported significantly reduced intraoperative blood loss when using 3DP drill guides, compared to cases without 3DP. However, across 10 studies measuring blood loss, there was no significant difference in intraoperative blood loss between 3DP (177 patients, 925 mL) and non-3DP spine cases, after controlling for operating time and procedure type (252 patients, 936 mL, P = .058). Screw placement accuracy, confirmed with imaging, was also a commonly assessed outcome in studies assessing 3DP screw drill guides and preoperative surgical models. In 17 studies using 3DP screw drill guides or planning models, there was a significant increase in screw placement accuracy in the 3DP cohorts (96.9% of total screws placed), compared with non-3DP cohorts (81.5% of total screws placed; P < 0.001), including freehand placement (81.6%) and nonspecified techniques (81.3%). Screw placement accuracy was not reported for fluoroscopic-guided or navigation-based techniques.
Summary of 3DP Screw Drill Template Studies.
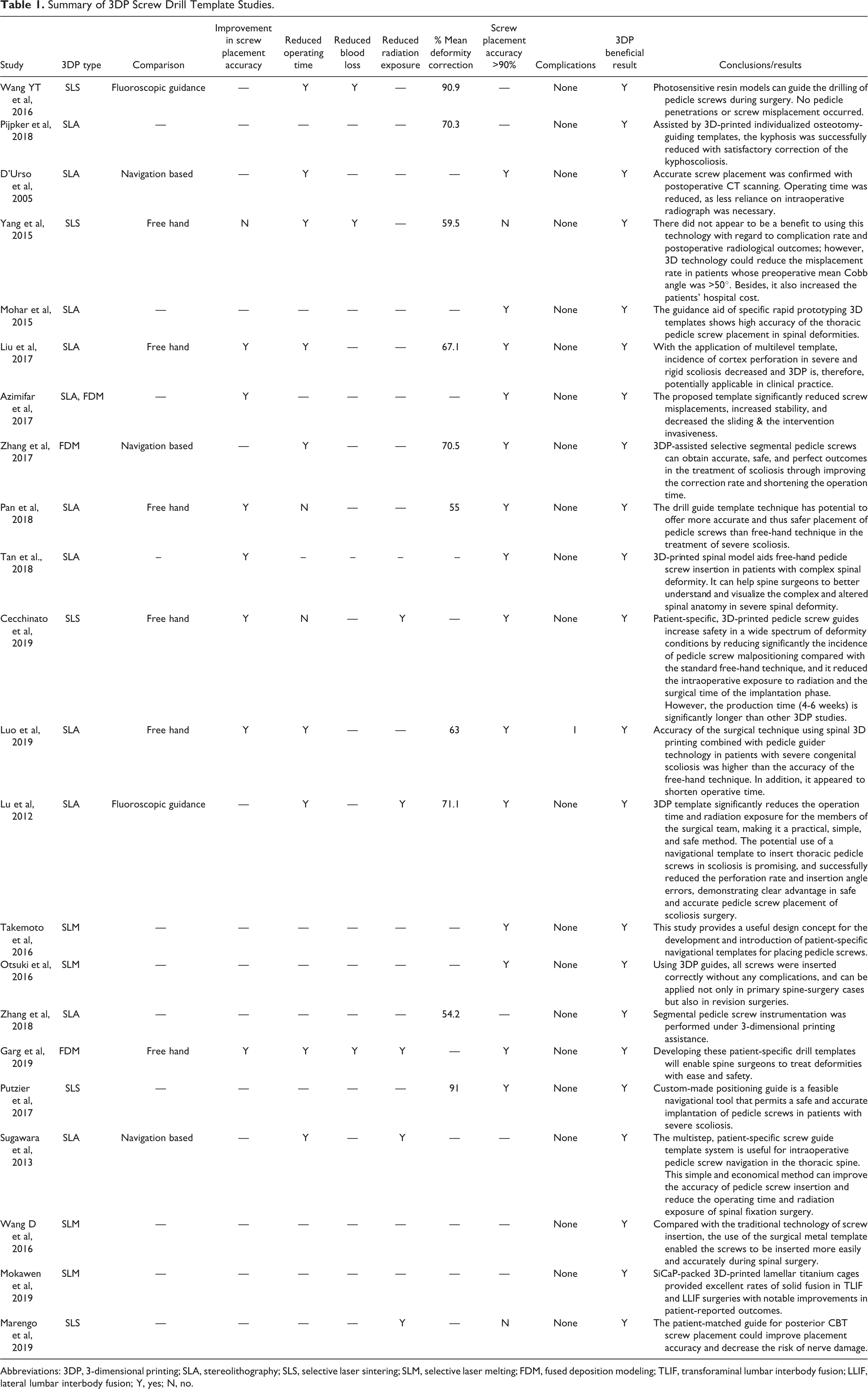
Abbreviations: 3DP, 3-dimensional printing; SLA, stereolithography; SLS, selective laser sintering; SLM, selective laser melting; FDM, fused deposition modeling; TLIF, transforaminal lumbar interbody fusion; LLIF, lateral lumbar interbody fusion; Y, yes; N, no.
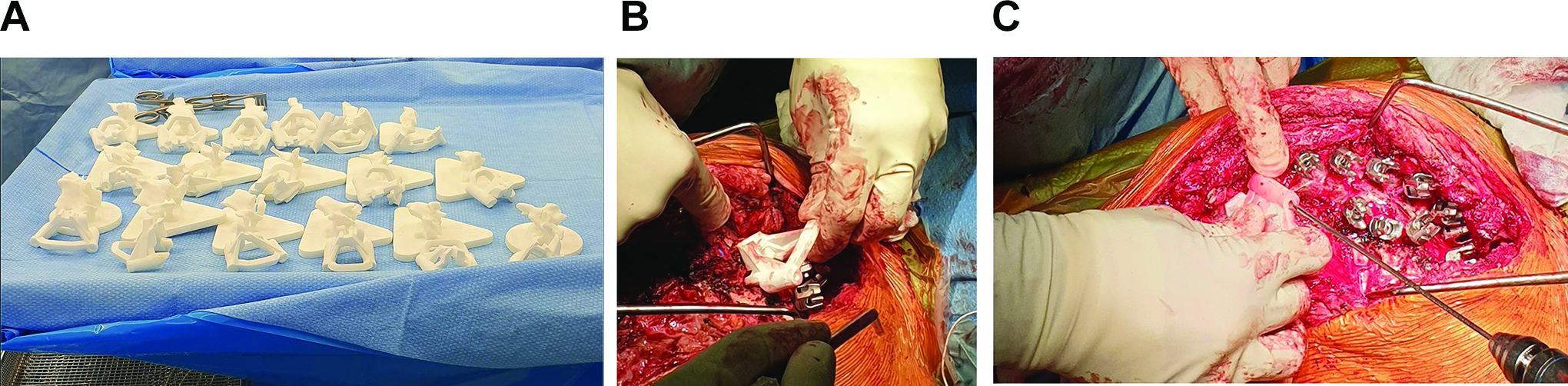
Sample images of custom 3D printed pedicle screw guides. Figure A shows sterile, back table preparation of all 3D printed guides for a specific patient, B shows one specific guide being placed at planned instrumented level, C shows a pedicle tract being drilled with orientation provided by the custom 3D printed guide. All figures were provided courtesy of Medacta International MySpine (Memphis, TN).
Presurgical Planning
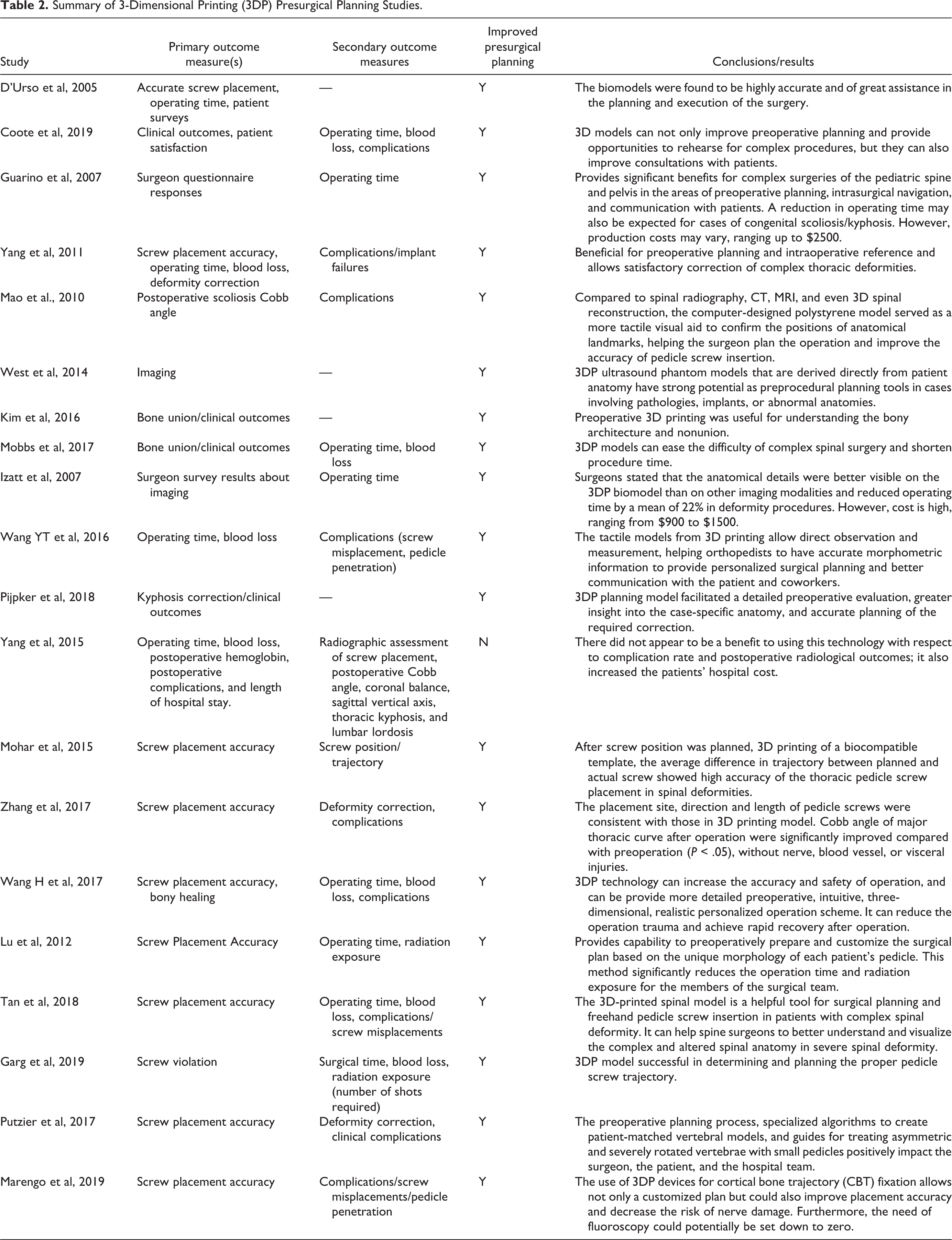
Twenty reviewed studies (62.5%) evaluated the use of 3D printing applications (ie, spine models, anatomical guides) in presurgical planning (Table 2, Figure 3). One of these studies concluded that not only did there not appear to be a benefit to using 3DP, but it also increased hospital costs compared to non-3DP cases (Chinese Yuan to USD conversion: $22 342 + $1415.16 vs $21 701 + $1629, P = .03). 1 However, the other 19 reviewed studies found 3DP planning models to offer benefits to both attending and resident spine surgeons during presurgical planning in terms of enhancing understanding of spinal anatomy and associated bony architecture, especially in preparation for complex surgeries. In one of the studies, attending surgeons remarked that “anatomical details were better visualized on the 3DP models than on any imaging modalities.” 18 Several studies reported favorable clinical outcomes when using 3DP technology—among 12 reviewed studies using 3DP planning models or 3DP drill guides, the reported average deformity correction rate was 72.5% in 3DP cases of 245 patients. Surgical time averaged 236 minutes, which was significantly less than the average surgical time of non-3DP studies (262 minutes; P < .001). Five total studies reported reduction in fluoroscopy exposure in cases using 3DP drill guides and/or planning models with an average radiation exposure decrease of 61.2%, although it was statistically non-significant (P = .109). Two studies measured fluoroscopy doses in cases with 3DP (average 30 unique images) and without 3DP (average 77 unique images). 19,20 One study in the review reported an intraoperative complication after using 3DP for presurgical planning, involving a patient who had a cerebrospinal fluid leak involving the nerve root axilla which was repaired with sutures. 21
Summary of 3-Dimensional Printing (3DP) Presurgical Planning Studies.

3-Dimensional printed model of complex kyphoscoliosis.
Training and Education
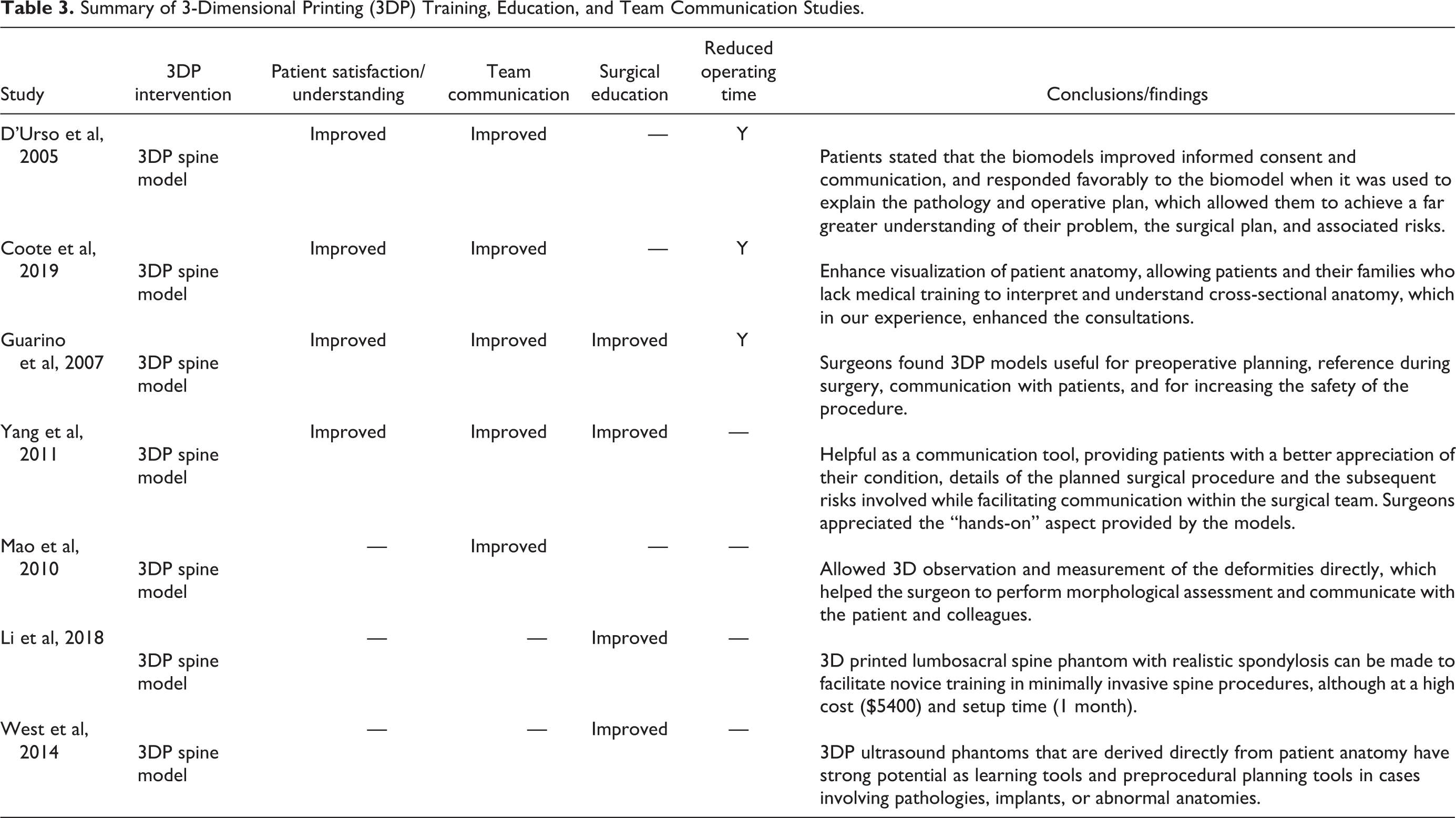
There were 7 reviewed articles (21.9%) which studied the use of 3DP in applications involving surgical training and education, communication between surgical team members, and patient education and communication (Insert Table 3). Surgical time averaged 257 minutes, although surgical time for non-3DP applications were not reported. Authors of studies analyzing 3DP applications in these settings cited enhanced preoperative understanding of patient anatomy by surveyed attending surgeons, resident trainees, and patients, as well as procedural guidance and improved trainee confidence as some of the most significant reasons for supporting the use of 3DP. 21 -27 In addition, several studies reported improved patient communication and satisfaction during presurgical consultations by providing easy-to-understand and tactile 3DP renderings of complex anatomy and imaging. 18,21 -23,28,29 Surgeons cited the benefits of 3DP models as helpful communication tools by “providing patients with a better appreciation of their condition, details of the planned surgical procedure, and the subsequent risks involved.” 18 Surgeons and patients surveyed by Wang et al 28 stated that the tactile 3DP models enhanced intuitive understanding of the complex spinal anatomy and improved patient-surgeon communication.
Summary of 3-Dimensional Printing (3DP) Training, Education, and Team Communication Studies.
3DP Production Process (Production Materials, Costs, and Time)
Numerous 3DP technology types were used in the reviewed articles. However, stereolithography (SLA) was the most commonly used 3DP technology, appearing in 18 out of 32 (56%) studies. Selective laser sintering (SLS), which also included selective laser melting (SLM) and MySpine technologies, was the second most commonly used 3DP technology, with 12 out of 32 studies (37.5%) reporting its use. Only 4 out of 32 studies (12.5%) used fused deposition modeling (FDM), which was the least used 3DP technology.
There are a wide range of reported costs (ranging from $175 for a 3DP template model to $5,400 for sophisticated 3DP spinal phantom training models), production lead time (9 hours to 1 month), and materials (polymers, metals, synthetic bone graft materials, other) (Table 4). The average cost for a set of screw drill guides was $415, without including cost of the 3D model, with an average production lead time of 5.8 days. 3DP planning tools cost an average of $1263, and production time averaged 4.9 days. 3DP applications for training and education purposes had an average cost of $1673 and production time of 8.6 days. Various types of 3DP materials were used in the reviewed studies, with 15 different materials across 4 categories (metals, polymers, synthetic bone graft materials, and other). Polymers were reported as the most commonly used material type in 24 out of the 32 studies (75%). Polystyrene and resin were both reported as the most commonly used polymers; each was used in 5 studies (17%). Titanium or stainless steel for 3DP templates or implants were used in 5 out of 32 (16%) studies.
Summary of 3-Dimensional Printing (3DP) Production Type, Materials, Costs, and Time.
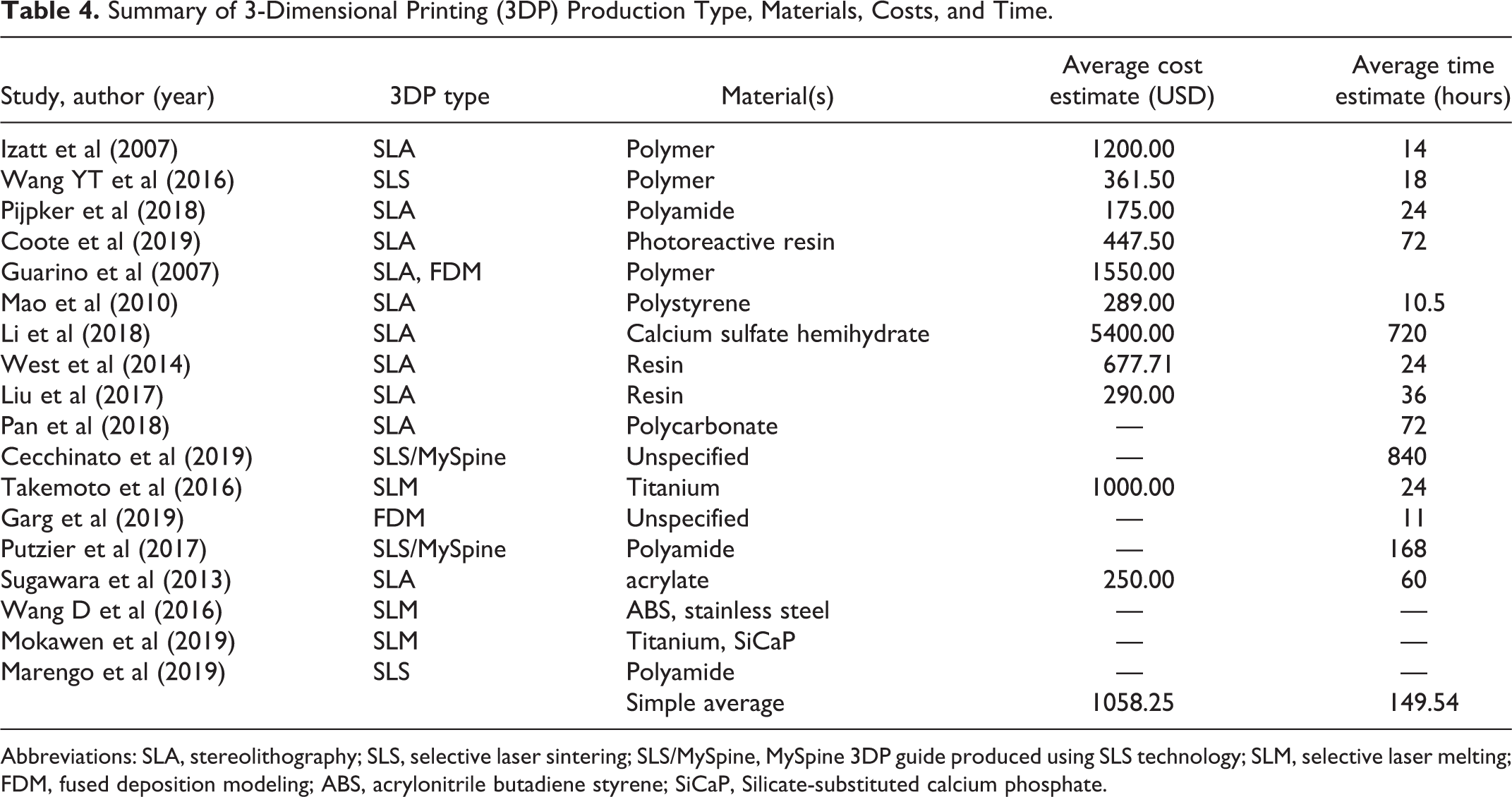
Abbreviations: SLA, stereolithography; SLS, selective laser sintering; SLS/MySpine, MySpine 3DP guide produced using SLS technology; SLM, selective laser melting; FDM, fused deposition modeling; ABS, acrylonitrile butadiene styrene; SiCaP, Silicate-substituted calcium phosphate.
Discussion
This systematic review evaluated current applications of 3DP in the surgical treatment of adult spinal deformities. The surgical treatment of scoliosis and other complex adult spinal deformities involves inherent difficulties such as anatomic anomalies, dysmorphic or absent pedicles, and vertebral rotation. These challenges make it difficult to visualize the scoliotic spine and its anatomical landmarks for pedicle screw insertion. As such, 3DP applications in the surgical planning process can aid spine surgeons in visualizing and understanding spine anatomy, enabling more detailed planning and simulation of the procedure, and instrumentation decisions. 4,18,23 -25,30 Compared with a previous systematic review of 3DP in spine surgery, 4 our review focuses on the use of 3DP in treating adult spinal deformities, which poses unique challenges and opportunities. In addition, an increasing trend in the number of annual 3DP review—over one-third of the articles in this review (11 studies) were published in 2018 or 2019—makes it necessary to provide a more up-to-date review that includes the most current applications.
In our review, 3DP applications, including 3DP screw guides and planning models, have resulted in statistically decreased operative durations and increased pedicle screw placement accuracy. 1,18,19,28,31 Compared with conventional imaging (eg, intraoperative fluoroscopy), 3DP screw placement guides provide improved screw placement accuracy rates, 19,20,31 -35 and models enhance intrateam communication and planning, 21,23 -25,28,36 and reduced fluoroscopy time. 19,20 In one retrospective study of 126 adolescent idiopathic scoliosis patients with a Lenke 1 deformity, Yang et al 1 showed that 3DP models used for surgical planning resulted in reduced operative duration and blood loss. However, there was no effect on the rates of screw placement accuracy, complications, and hospital length of stay. 1 Another study surveyed spine surgeons and found that anatomical details were better visualized on a 3D spine model compared with CT or MRI 3D reconstructions. They reported a 22% reduction in operation duration, which the authors attributed to enhanced anatomical visualization and more detailed preoperative planning which resulted in easier and more accurate implant and screw positioning, less frequent reference to conventional imaging, and increased implant efficiency and reduced cost of surgery. 18 In addition, they reported improved intra-surgical team communication and between surgeons and patients.
3DP technology has also been used for physician training and patient education applications. It provides a physical and tactile anatomical model that serves as an aid in understanding the spine anatomy of each patient and the planned surgical intervention. 3DP models enhance patient understanding of their condition and the surgical plan, which has been shown to increase rates of patient informed consent by as much as 25%. 37 In postoperative patient questionnaires, many patients reported that patient-specific 3D printed spinal models improved anatomical understanding of their condition as well as comprehension of their planned surgical procedure and its associated risks. 18,25,38 3DP spine models may also be able to replace or supplement cadaveric models in resident training and education, as they offer customizability and greater availability, and have none of the health and safety issues associated with cadaveric models. 39 3DP has been shown to be beneficial in improving training in spine surgery, including complex procedures such as open door laminoplasties and needle placement for image-guided spinal procedures. 27,40,41 Li et al 26 showed that training using a 3DP spine model helps increase skills and confidence of surgical trainees.
Radiation exposure from intraoperative fluoroscopy and CT imaging used in navigation systems remains a concern to patients and surgeons as an increase in tumor incidence has been reported in each of these groups in sufficient radiation doses. 42 -44 The use of 3DP spine models in presurgical planning may potentially reduce intraoperative radiation exposure. However, a preoperative CT scan is typically required. Our review identified 2 studies that measured intraoperative radiation exposure from fluoroscopy in adult deformity cases with 3DP technology and without 3DP. 19,20 Although there was a nonsignificant reduction in fluoroscopy exposure by 61.2% in the 3DP cases compared with the non-3DP cases, more studies are needed to elucidate stronger evidence of radiation dose reduction in cases when 3DP is used.
Pedicle screw placement accuracy remains a major concern for spine surgeons, and misplacement has been reported to occur in up to 20% to 30% of cases. 45,46 Free-hand implantation of screws depends heavily on surgeon skill and the occasional utilization of intraoperative fluoroscopy to confirm positioning. However, 3DP screw drill guides and navigational templates, which are customizable and made to be anatomically accurate based on pre-operative imaging, may offer more accurate and safer screw placement during deformity-correcting spine surgery. 47 Some studies in our review have shown that the use of 3DP pedicle screw templates may result in improved screw placement accuracy and precision, reduced operative time, and reduced perioperative complications and radiation exposure, compared to non-3DP (fluoroscopy or CT) guided procedures. 32,48 -50 Our review shows that the use of 3DP may result in favorable deformity correction outcomes, with an average correction rate of 72.5% and a high screw placement average accuracy of 96.5%. It is worth noting, however, that there exists variation in operating time among spine surgeons, which depends on skill level and prior training with screw implantation. Advanced free hand surgeons may not benefit as much from using screw drill guides in their practice as a general spine surgeon would.
Finally, production costs of 3DP surgical planning models vary widely in the reviewed studies, with marginal costs ranging from $175 for a 3DP template model to $5400 for sophisticated 3DP spinal phantom training models. Production lead times also varied widely from 9 hours to 1 month within the reviewed studies. Similar to 3DP in surgical planning, there is a wide range of per-unit manufacturing costs and production time across various types of materials and printers in the application of 3DP in creating screw guides. Costs ranged from $175 to $290 in marginal costs, although reporting was limited among the reviewed articles, and there was no discussion regarding costs and production times. There was also a wide variability in 3D printing materials in the reviewed studies, which included resin, polystyrene, polymer, polyvinyl chloride, polycarbonate, polylactic acid, titanium, stainless steel, polyamide, and acrylate. Few studies discussed comparisons between materials, especially metal. Takemoto et al 48 reported a very high pedicle screw accuracy rate (98.4%) when using 3DP titanium screw templates. Although titanium is 5 times more expensive than plastic polyamide, which is one of the most commonly used material in 3DP, the authors emphasized the superior strength and durability of titanium metal compared with polyamide plastic, which ensures greater accuracy, reduces the risk of warping, flexing, and potential damage to the guide during intraoperative manipulation. 48 The authors also noted that plastic is more likely to produce intraoperative debris when in contact with drills and other surgical tools, posing a potential risk to the safety of nearby neurovascular structures, and which may lead to retained micro-debris. Another study by Wang et al 28 showed that 3DP screw templates made with stainless steel have better screw placement accuracy, are easier to autoclave, and are less prone to perioperative damage and deformation, compared with 3DP resin templates. It is important to note that the reported variation in production costs of polymer-based 3DP models, which can range up to $2500, pales in comparison with the relatively lower costs of other materials that have demonstrated comparable efficacy.
There are still limitations associated with the use of 3DP screw guides and templates. There were 4 studies that disclosed conflict of interest, including 3 studies with authors receiving consulting fees from device manufacturers (Medacta and Medtronic), 20,29,35 and 1 study which was supported by DePuy Acromed, Inc and Medtronic Sofamor Danek. 22 Although various studies have shown reduced operative times when using 3DP screw guides, it is important to also consider the production time which can take several hours and involves collecting and processing imaging data and designing and printing the 3D screw guides. Production costs of 3DP surgical planning models vary widely in the reviewed studies, likely due to lack of standardized manufacturing processes. In addition, a common problem reported in studies involves clean bone preparation, which requires complete removal of soft tissue for optimal template fixation. This is a time-intensive process that has been associated with increased intraoperative blood loss. 4,50,51 Additional time and costs associated with implementing the technology in hospitals and training staff on how to use the technology must also be considered. Future directions in 3DP technology must focus on creating a user-friendly and commercially viable 3DP system that allows for standardization and streamlining of the production process into a more cost-effective and efficient model.
Conclusions
Three-dimensional printing is currently used for presurgical planning, patient and trainee communication and education, pre- and intraoperative guides, and screw drill guides in the treatment of scoliosis and other adult spinal deformities. Studies evaluating the use of 3DP drill guide templates have shown significantly better screw placement accuracy compared to the non-3DP cohort, and favorable deformity correction rates. Utilization of 3DP technology in the treatment of adult spinal deformities has been shown to significantly reduce operative duration, compared to the non-3DP cohorts. However, there are no significant difference in perioperative blood loss between the 3DP and non-3DP cohorts among the reviewed articles. Analysis of 3DP technology types, materials, and manufacturing costs and times yielded variable results. Stereolithography remains the most commonly used 3DP method.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.