
Abstract
Study Design:
A narrative review of the literature.
Objective:
This article reviews the general principles of treatment and investigation for primary bone tumors of the spine. Furthermore, it explores the emerging alternatives.
Methods:
A review was performed using Medline, Embase, and Cochrane databases.
Results:
Primary bone tumors of the spine are rare entities that general spine surgeons may encounter only a few times in their career. The treatment algorithm of these complex tumors is filled with nuances and is evolving constantly. For these reasons, patients should be referred to experienced tertiary or quaternary centers who can offer a comprehensive multidisciplinary approach. For most malignant spinal bone tumors, surgery remains the cornerstone of treatment. Respecting oncologic principles has been associated with improved survival and decreased local recurrence in multiple settings. However, even in experienced centers, these surgeries carry a significant risk of adverse events and possible long-term neurologic impairment. The associated morbidity of these procedures and the challenges of local recurrence have encouraged professionals caring for these patients to explore alternatives or adjuncts to surgical treatment.
Conclusions:
Over the past few years, several advances have occurred in medical oncology, radiation oncology and interventional radiology, changing the treatment paradigm for some tumors. Other advances still need to be refined before being applied in a clinical setting.
Keywords
Introduction
Primary bone tumors of the spine are far less common than metastatic spine disease. According to the Surveillance, Epidemiology and End Results (SEER), the overall incidence of primary bone tumors in the United States is 0.9 per 100 000 men and women per year, including both axial and appendicular lesions. 1 An estimated 3450 new cases will be declared this year in the United States. These lesions can harbor different patterns of behavior and represent a heterogeneous group; from benign and latent to malignant and aggressive. Chordoma, chondrosarcoma, osteosarcoma, and Ewing’s sarcomas represent the most frequent malignant bone tumors. 1 Some lesions, such as aneurysmal bone cyst (ABC), giant cell tumor (GCT) of the bone, and osteoblastoma are histologically benign but can have aggressive behaviors and recur if not treated properly.
Identifying the rare primary bone tumor of the spine is of paramount importance as their management may differ tremendously from a metastatic spinal lesion. Undergoing inappropriate treatment can negatively affect these patient outcomes and even transform a curable disease to a lethal one. It cannot be overemphasized that vigilant recognition of these lesions is key, and prompt referral to experienced spine tumor centers for investigation and definitive management should be sought. Primary bone tumors of the spine should be treated in dedicated centers with experienced multidisciplinary teams. Although surgery remains a critical part of the treatment for most primary bone tumors, it is only a component of a comprehensive management plan. In this era of rapid medical advances, a multidisciplinary approach is mandatory to optimize these patient outcomes.
This article will review general management principles of primary bone tumors of the spine and will focus on recent advances in the treatment of these unique lesions.
General Principles
Staging
In the presence of a solitary spinal lesion, local and systemic staging should be undertaken. More than 85% of the time, the origin of a lesion can be determined with systematic systemic staging. Investigations include a computed tomography (CT) scan of the chest, abdomen, and pelvis and a bone scan. Positron emission tomography (PET)-CT is also increasingly used for staging. 2 After appropriate local and systemic staging a well-planned biopsy to confirm the diagnosis should be done. When a primary bone tumor is suspected, the biopsy should be coordinated by the center where the patient will undergo definitive treatment. Proper biopsy orientation is a key aspect in the management of primary bone tumors. This is highlighted by reports confirming that biopsy performed outside the definitive treating center as well as intralesional resection are associated with greater rates of tumor recurrence. 3,4 As a multidisciplinary group of experts caring for patients with spinal tumors, the Spine Oncology Study Group (SOSG) published recommendations that stipulate that the surgeon who will perform the definitive surgery should do or direct the biopsy. 5 This ensures suitable orientation of the biopsy allowing resection of its tract within the surgical specimen where feasible.
Classifications
Over the past decades, recognition of the uniqueness of primary bone tumors has led to the acceptance of Enneking’s principles. This classification originated from the appendicular musculoskeletal oncology world. 6 A recommended surgical margin is proposed for each stage of this oncological staging system. Tumors are divided into benign and malignant. Benign lesions are classified as S1, latent; S2, active; and S3, aggressive. For benign lesion, observation is suggested for latent lesions and an aggressive curettage or wide/marginal resection is suggested for active or more aggressive lesions. Malignant tumors are classified based on the grade (low vs high), local extension (intra- vs extracompartmental), and the presence of metastasis. For malignant lesions, in the absence of metastases, a wide resection is advocated.
Surgical Management
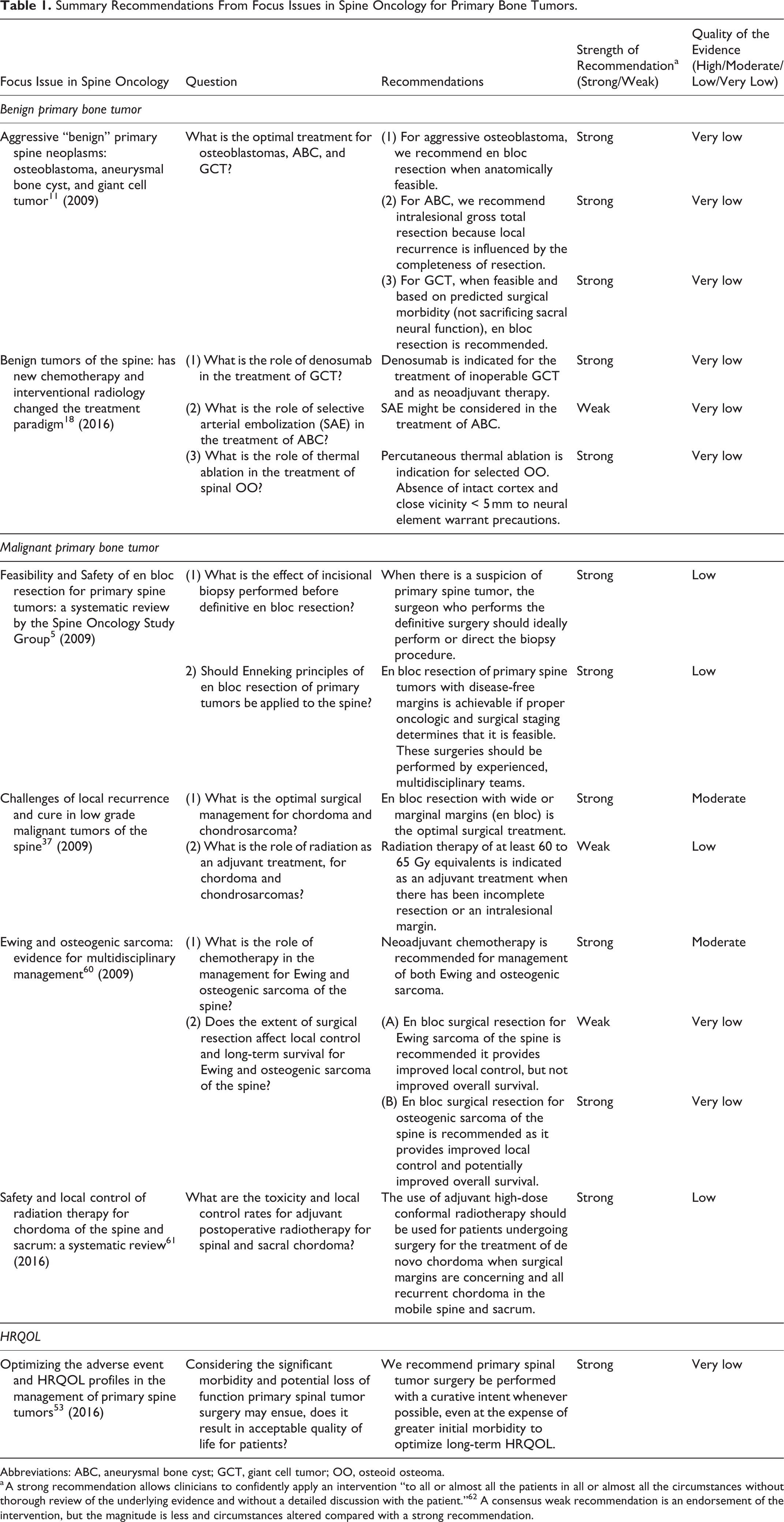
An en bloc resection is a surgical resection where the tumor is excised as a single piece as opposed to piecemeal resection. However, in terms of local control and survival, an en bloc resection is meaningless if not accompanied by the pathological description of the margins. Depending on the histological appearance of the margins, they can be classified as intralesional, marginal, or wide. Intralesional means that the tumor capsule has been violated. Wide margins refer to the removal of the tumor along with a shell of healthy tissue contiguous to it. Marginal margins signify that the plane of dissection is in the reactive layer surrounding the tumor or its pseudocapsule. As dura is not excised with the specimen for most cases, margins at the dura are often marginal if the tumor is extending to the epidural space. In 2009, the SOSG issued a strong recommendation based on moderate quality evidence and consensus expert opinion that en bloc resection with wide or marginal margins should be undertaken for surgical treatment of primary malignant bone tumors 5 (Table 1). Because of the morbidity especially regarding neural sacrifice controversy remains within some areas of the spinal community. Modern evidence supports en bloc resection with wide/marginal margins as the cornerstone of management for most primary malignant bone tumors and confirms that adhering to evidenced-based oncologic principle results in lower recurrence and mortality rates. 7 -10 Furthermore, en bloc resection after an Enneking inappropriate surgery (ie, an intralesional procedure for a malignant bone tumor) has been demonstrated to yield inferior outcomes in terms of local recurrence and survival, reinforcing that the first surgery is the best attempt for cure and that these patients should be promptly referred to experienced centres even in a setting of neurological deficit 3,4 (Figure 1).
Summary Recommendations From Focus Issues in Spine Oncology for Primary Bone Tumors.
Abbreviations: ABC, aneurysmal bone cyst; GCT, giant cell tumor; OO, osteoid osteoma.
a A strong recommendation allows clinicians to confidently apply an intervention “to all or almost all the patients in all or almost all the circumstances without thorough review of the underlying evidence and without a detailed discussion with the patient.” 62 A consensus weak recommendation is an endorsement of the intervention, but the magnitude is less and circumstances altered compared with a strong recommendation.
En bloc resection of a L5 chordoma after inappropriate intralesional resection. (A) L5 chordoma at initial presentation. This patient underwent a decompressive laminectomy and intralesional resection. (B) Pathological specimen. Because of inappropriate intralesional resection, a skin ellipse was removed to excised tumor contaminated tissue when the Enneking appropriate en bloc resection was performed. This required a complex plastic closure. (C) Specimen x-ray.
In the appendicular skeleton, benign aggressive lesions such as ABC, GCT, and osteoblastoma are usually treated with intralesional curettage with or without local adjuvant such as phenol and liquid nitrogen. However, intralesional resection carries a significant risk of local recurrence, which can be challenging in the spine. Furthermore, local adjuvants usually cannot be used around the spine due to the risk of thermal injury. The SOSG issued strong recommendation with a very-low-quality evidence to perform en bloc resection for stage 3 osteoblastoma and GCT when feasible based on the staging and predicted surgical morbidity. For ABC, a gross total intralesional resection (very-low-quality evidence) is recommended. 11 More recently, data favoring en bloc resection over intralesional resection for GCT of the spine with regard to local recurrence have been published. 12
As surgical treatment of primary bone tumors is associated with significant morbidity and mortality, alternative therapies and adjuvant treatments have emerged with the goal of facilitating the surgery or, in some cases, replacing surgery altogether while achieving similar outcomes. This evolving field involves medical treatment, percutaneous techniques, radiation therapy, and the emergence of precision medicine with molecular sequencing. Furthermore, interest in patient reported outcomes has come to the forefront, acknowledging that local recurrence and survival are not the only outcomes that need consideration.
Medical Oncology and Interventional Radiology
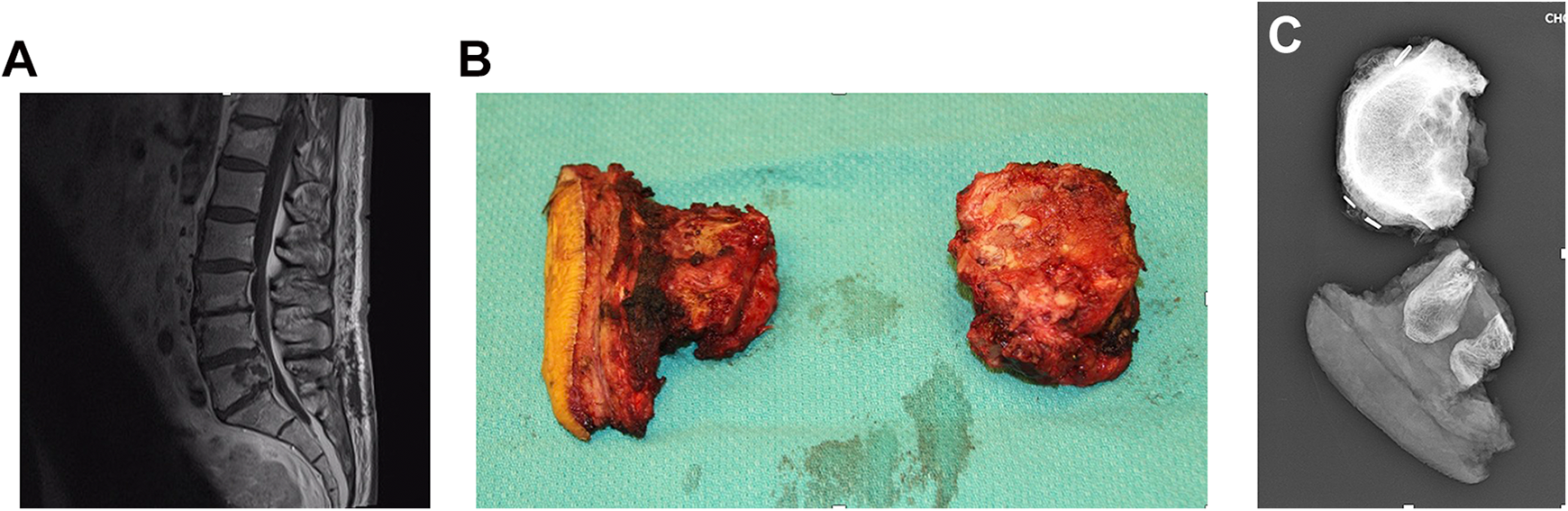
Giant cell tumors harbor 3 types of cells: the multinucleated giant cell, the stromal cell and the mononuclear monocyte. The hallmark of GCT is the multinucleated giant cells, which express high levels of the receptor of activator nuclear factor κ-B ligand (RANKL). Activation of the RANKL leads to bony resorption. Denosumab is a monoclonal antibody that inhibits RANKL and it was postulated that this medication could halt progression in inoperable GCT. The first clinical trial funded by industry yield promising results with clinical response in more than 85% of the patients at 6 months (37 patients). 13 On histopathological analysis of that same cohort, a marked reduction of the multinucleated giant cells was observed (>90%). 14 The second clinical trial (282 patients) results were in line with the first one: an overall 75% objective tumor response, however, mostly partial responses. 15 Of note, these clinical trials included axial and appendicular GCT. This led to the Food and Drug Administration approval of denosumab for the treatment of inoperable GCT in 2013. Specific to the spine, in 2015, Goldschlager et al 16 published the first case-series of neoadjuvant denosumab with all patients presenting a favorable clinical and radiological response to denosumab. One patient out of 5 presented with histopathological failure to treatment. 16 Decreased epidural disease as well as tumor calcification was reported with this treatment (Figure 2). Tumor angiogenesis has been shown to be reduced with denosumab. 17 In 2016, the AOSpine Knowledge Forum Tumor (AOSKFT) recommended denosumab either as a stand-alone for treatment of inoperable GCT or as an adjuvant prior to surgical resection. 18 Preoperative treatment duration recommendation was either 6 months or to maximal calcification/tumor reduction. However, uncertainty regarding long-term response and side effects remains. Concerns regarding rate of recurrence after discontinuation have been reported, especially after intralesional procedure. 19,20 This can be explained by the findings of Mak et al 21 that although the multinucleated giant cells are effectively eliminated with denosumab, the true neoplastic cells (the stromal cells) persist. Short-term treatment is associated with mild toxicities, but prolonged treatment is associated with a 9% risk of osteonecrosis of the jaw as well as a 4% risk of atypical femoral fracture in the most recent series. 19 Furthermore, case reports of malignant transformation following this treatment have been published although causal relationship cannot be made. 22 -24 Denosumab is definitely a valuable treatment, but as with any newer treatment, vigilance is mandatory.
Denosumab response in a L1-L2 giant cell tumor after 6 months of treatment. (A) Axial computed tomography (CT) pretreatment. (B) Coronal CT pretreatment. (C) Axial CT after 6 months of denosumab. (D) Coronal CT after 6 months of denosumab.
Selective arterial embolization as a stand-alone treatment has been reported with ABC. Initially, promising results were observed with tumor calcification and regression. 25,26 The main problematic issue with this technique was that up to 35% of the patients in these series required more than 6 treatments, which is a concern from a radiation exposure standpoint. 26 The most recent series published by the same group tempered the initial enthusiasm with a rate of failure approaching 30%. 27 Nonetheless, their results showed a reasonable safety profile and this technique can be considered as an option when the morbidity of other procedures appears to be too high. As an alternative, exploratory research on denosumab use for ABC has been published with a handful of case reports. 28 -31 As of now, evidences to support its use in ABC are lacking.
Thermal ablation for osteoid osteoma (OO) is currently the gold standard treatment in the appendicular skeleton with a failure rate of 5%. 32 The potential proximity of the OO to the spinal cord has naturally raised concerns about the safety of thermal ablation in the spine. With radiofrequency ablation, a temperature of 90°C is usually applied for 6 minutes to achieve a satisfactory ablation of the nidus. Generally, lesions with an absent cortex or located within 5 mm of a neural structure are considered at risk of thermal injury. 18 Nonetheless, Yu et al 33 have performed radiofrequency ablation successfully with only 1 mm of cerebrospinal fluid space between the lesion and the neural element. Techniques with either air or saline insufflation have been proposed to reduce the risk of injury. 34,35
Radiation Therapy
Even in experienced hands, achieving en bloc resection with marginal or wide margins is challenging with a failure rate of 21% to be Enneking appropriate. 36 Consequently, radiation therapy has been recommended to increase local control. Chordoma and chondrosarcoma are known to be radioresistant, necessitating doses of approximately 70 Gy. 37 A recent survey by the AOKFT revealed large variations across some of the world’s most experienced cancer centers in the use of radiation modalities in the setting of newly diagnosed spinal chordomas. 38 For tumors with which en bloc resection is feasible with acceptable morbidity, some centers are giving neoadjuvant radiation as a standard of care, other centers are administering routine postoperative radiation regardless of the surgical margins, and some centers are not pursuing any radiation treatment when wide/marginal margins are obtained. On the other hand, when en bloc resection would result in significant morbidity, some centers rely more heavily on neoadjuvant and adjuvant therapies with variation in the surgical procedure. These findings highlight that the optimal radiation therapy regimen remains unsolved.
Radiation oncology has undergone a major transformation over the past decade as a consequence of on-board image-guidance systems, incorporation of multimodal imaging, sophisticated treatment planning software, and delivery hardware that permits millimetric precision. These technical developments have also resulted in a new technique known as spine stereotactic body radiotherapy (SBRT), which refers to the delivery of tumor ablative doses within the diseased vertebral segment, in a single or few high dose fractions, while sparing the surrounding organs-at-risk (primarily the spinal cord). The intent is to maximize local control. 39 Although the main application has been in the treatment of metastatic spine disease, spine SBRT is evolving into the management of primary spinal tumors. For spinal chordoma, treatment with high-dose SBRT has been reported with encouraging local tumor control results 40 ; however, it represents a major departure from established practice of protracted radiation delivery with intensity modulated photon radiotherapy or proton particle–based radiation (eg, 78 Gy in 39 fractions). 41 At present the use of spine SBRT remains investigational for chordoma and should be performed on clinical trial.
In principle, proton therapy offers a substantial clinical advantage over conventional photon therapy with regard to limiting dosage to surrounding tissues. Using a combination of photons and protons, 5-year local control rate as high as 94% has been published for primary spinal sarcomas. 42 -44 Combination of neoadjuvant radiation therapy, en bloc resection, and a postoperative radiation course has been postulated to result in the highest rate of local tumor control. 43 However, Houdek et al 45 recently challenged this concept. In their retrospective study of 239 patients, neoadjuvant radiation therapy did not reduce mortality, local recurrence or metastasis. 45 Furthermore, it was associated with significant wound complications and sacral fracture.
A disruptive technology that has been reported for resistant tumors like chordoma is carbon ion particle radiation. This particle is biologically distinct from protons, represents a potential for a greater biologic effect, and has inherent unique radiobiological characteristics that may explain the high rates of local tumor control reported for sacral chordoma. 46 For example, one of the largest series for sacral chordoma outcomes with carbon ion was reported by Imai et al. 46 They reported a 5-year local control rate of 77%, which is impressive as compared with historic data. The technique is still experimental and evolving with only few installations globally.
Mobile spine chordoma is a separate entity and the optimal technology is debatable especially as the precision afforded by modern image-guided photon therapy may allow less uncertainty in margins compared to proton or carbon ion therapy. The high precision allows for tighter and more reproducible dose gradients at the spinal cord–tumor interface, which may provide an advantage in this clinical scenario. Ultimately, we need comparative data for these radiation modalities to understand what is best and cost-effective, given the far greater costs associated with particles as compared with photons and the greater availability for photon therapy globally.
Molecular Sequencing
Precision medicine with molecular sequencing is changing the face of oncology. Knowing the molecular signature of a specific tumor for a specific patient opens the horizon for potential treatment that could never have been envisioned before. This area of translational medicine is still in its infancy but is definitely promising. Given the rarity of primary bone tumors, collaborative approaches have to be advocated. An example of this is that through the AOSKFT, Bettegowda et al 47 were able to extract DNA from 109 paraffin-embedded chordoma specimens. They were able to demonstrate association with the single nucleotide polymorphism (SNP) rs2305089 in the T gene and survival. 47 Overexpression of the T (brachyury) gene is known to be the hallmark of chordoma. Other collaborative networks are expanding our knowledge on the genetic landscape of chordoma. 48
Tumor surveillance would benefit from new methods to allow early detection of tumor recurrence and/or metastasis. Liquid biopsy, taken from a blood sample, are potentially prognostic or predictive marker in multiple cancers. 49 Liquid biopsies inform on circulating tumor cells as well as tumor-derived cell-free nucleic acids, exosomes, and platelets. Because of the rarity of primary bone tumor and the absence of specific markers expressed by most primary bone tumors, the characterization of primary bone tumor circulating tumor cells has to date been relatively limited. 50 Recently, techniques have been described to monitor Ewing sarcoma through liquid biopsy. 51,52
Health-Related Quality of Life
En bloc resection is associated with significant morbidity (13%-73.7%) and mortality (0%-7.7%), even in the most experienced centres. Because of their unique anatomical relation and because of the potential bowel and bladder dysfunction, sacral resection are considered highly morbid procedure with a complication rate approaching 100%. 53 The impact of these extensive and potentially impairment-producing procedures on health-related quality of life (HRQOL) is definitely a critically valuable piece of information.
At the present time, there is paucity of published data regarding HRQOL following these surgeries. 54 -58 Nonetheless, when combining the available literature, HRQOL after surgery for primary bone tumor of the spine is acceptable with HRQOL reaching close to normative values over time. 53 Furthermore, tumor recurrence seems to be correlated with worse HRQOL, reinforcing the application of oncologic principles. 57
Clinical Resources
Guidelines have been developed in the management of appendicular sarcomas. Although spine has its own specificities, the overall management shares similarities. The American National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines (www.nccn.org) and its European counterpart, the ESMO/European Network Working Group, Clinical Practice Guidelines for Bone Sarcomas 59 are available tools that provide guidance for diagnosis, treatment, and surveillance for most common primary bone tumors.
The Chordoma Foundation (www.chordomafoundation.org) is a nonprofit organization that promote research and provide counseling for patients with diagnosed chordoma. Patient educational vignettes and peer support are offered through the chordoma foundation. Furthermore, their website provides comprehensive information regarding diagnosis, management and offers a list of centers in Europe and North America with recognized expertise in primary bone tumors.
Conclusion
Treating primary bone tumors of the spine is challenging and this field has been evolving rapidly over the past few years, especially due to international and local collaborative networks. Respecting oncologic principles is the foundation of the treatment of these tumors. However, new advances in medical oncology, radiation therapy and interventional radiology are now emerging and may be changing the treatment paradigm. Some of these advances are very promising and might one day become standard of care. Until then, these patients should be treated according to the best available evidence. For the primary bone tumor population, this means referral to an experienced center where they will be treated according to the latest standard of care and hopefully, will be able to contribute to scientific advances.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AOSpine International through the AOSpine Knowledge Forum Tumor, a focused group of international spine oncology experts acting on behalf of AOSpine. Study support was provided directly through the AOSpine Research Department.