
Abstract
Study Design
Systematic Review.
Objectives
To evaluate which cervical deformity correction technique between anterior cervical discectomy and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF) produces better clinical, radiographic, and operative outcomes.
Methods
We conducted a meta-analysis comparing studies involving ACDF and ACCF. Adult patients with either original or previously treated cervical spine deformities were included. Two independent reviewers categorized extracted data into clinical, radiographic, and operative outcomes, including complications. Clinical assessments included patient-reported outcomes; radiographic evaluations examined C2-C7 Cobb angle, T1 slope, T1-CL, C2-7 SVA, and graft stability. Surgical measures included surgery duration, blood loss, hospital stay, and complications.
Results
26 studies (25727 patients) met inclusion criteria and were extracted. Of these, 14 studies (19077 patients) with low risk of bias were included in meta-analysis. ACDF and ACCF similarly improve clinical outcomes in terms of JOA and NDI, but ACDF is significantly better at achieving lower VAS neck scores. ACDF is also more advantageous for improving cervical lordosis and minimizing the incidence of graft complications. While there is no significant difference between approaches for most surgical complications, ACDF is favorable for reducing operative time, intraoperative blood loss, and length of hospital stay.
Conclusions
While both techniques benefit cervical deformity patients, when both techniques are feasible, ACDF may be superior with respect to VAS neck scores, cervical lordosis, graft complications and certain perioperative outcomes. Further studies are recommended to address outcome variability and refine surgical approach selection.
Keywords
Introduction
Cervical spine deformity (CSD) represents a severely debilitating condition that is becoming increasingly clinically relevant as the elderly population grows. 1 Both static and dynamic factors play into the pathophysiology of CSD. Static players include osteophyte formation and degenerative changes along uncovertebral and facet joints. 2 Dynamically, repetitive movements of the neck, such as cervical flexion or extension, aggravate spinal cord compression. 2 CSD alters the sagittal alignment of the spine over time; gradual cord compression typically manifests as an insidious onset of cervical myelopathy +/− motor and sensory deficits. 2 When the condition is refractory to conservative management, surgical intervention is indicated. 3 Surgical approaches vary significantly due to various etiologies and distant drivers of deformity. 4 Anterior spinal surgical procedures, including multi-level anterior cervical discectomy and fusion (ACDF) and single-/multilevel anterior cervical corpectomy and fusion (ACCF), are safe and effective in treating deformities in the cervical spine. 5 However, it is still unclear as to which procedure produces better clinical and/or radiological outcomes, even for the same type of disease condition.5-7 Some overlapping indications for each approach exist, regardless of the patient’s clinical phenotype. 8 Factors considered by surgeons when selecting between ACDF or ACCF are: open disc spaces, sagittal alignment, degree of instability, location of spinal cord compression, number of cervical levels involved, contributing axial pain, and risk factors for pseudoarthrosis such as poor bone quality. 9 No serious consensus exists about the superiority of each procedure when patient is candidate for both. 10 Different cohort studies have described outcomes of patients with either ACDF or ACCF,3,10-13 but conclusive recommendations for these techniques are still lacking, especially regarding future reoperation or neurological deterioration. Previous meta-analyses have also compared ACDF and ACCF for CSD correction, but not without limitations.14-17 While Guan et al 14 compares studies with a high level of evidence by including only RCTs, it does not extract complication rates for ACDF and ACCF. Han et al explores ACDF and ACCF for treatment of only adjacent two-level cervical spondylotic myelopathy. 15 Collectively, the number of studies and cohorts included in these prior meta-analyses are small, ranging from 8 to 15 and 631 to 1372, respectively; even fewer studies are captured for less frequently reported outcomes.14-17 Most importantly, while these previous meta-analyses share certain generalizations, their results vary considerably, and the efficacy and risks of ACDF compared to ACCF still remain in question. We believe that a critical qualitative synthesis for a large, pooled cohort will provide more insight into the true effects of both techniques and be useful for surgical approach selection for CSD correction.
Anterior Cervical Discectomy and Fusion (ACDF)
ACDF is 1 of the most common techniques performed for cervical deformity; about >50,000 ACDF procedures are conducted in the US alone. 18 There are several key indications for ACDF. Patients presenting with cervical radiculopathy, disc herniation causing myelopathy, anterior osteophytes, or bony spurs with subsequent spinal canal stenosis or nerve root compression have the most benefit with this technique. 19 ACDF allows the surgeon direct vision to address anterior pathology and the ability to perform a complete discectomy which favors a better fusion rate. 20 Multilevel ACDF is favored over ACCF if the compression is confined to the disc space. 18 However, multilevel ACDF is associated with an increased risk of pseudarthrosis, as high as 54% in three-level fusions. 11 Adjacent segment disease after ACDF is reported in 25% to 92% of the cases, 21 which possibly indicates that other variables are involved in the variance registered in different studies. In multiple studies,9,13,22-24 overall complication rates for ACDF varied from 13.2% to 19.3%, including dysphagia, hematoma, lesion of recurrent laryngeal nerve, respiratory insufficiency, esophageal perforation, instrumentation failure to mention a few. These complications that both ACDF and ACCF are susceptible to due to iatrogenic mishaps with anterior exposure and surgical plane, such as compression or damage to swallowing/vocal muscles, nerves, or tracheo-esophageal structures secondary to retraction, traumatic intubation, direct intraoperative contact injury, prevertebral swelling or hematoma formation. Therefore, complication rates have not differed between these 2 approaches, and it is not well defined which is more specific to each.9,13,22,23
Anterior Cervical Corpectomy and Fusion (ACCF)
Corpectomy is commonly preferred over multilevel ACDF in cases retrovertebral pathology such as traumatic disruption of the vertebral body, osteomyelitis, neoplasms and ossification of the posterior longitudinal ligament (OPLL). 25 These conditions require expanded decompression or removal of the vertebral body in order to obtain the desired clinical outcome. 25 Corpectomy is thought to have the ability to provide an entire decompression, particularly when there is important stenosis in the spinal canal behind the vertebral body. 9 Corpectomy also permits improved visualization, serves as source for autografting which facilitates fusion, and requires less donor grafts from other bones different from the spine.
ACCF is believed to have greater morbidity per level since it is more technically demanding than ACDF. 7 Increased rates of lesions to the vertebral artery, increased spinal cord exposure with more risk of iatrogenic injury, and higher rate of implant malfunction are among the additional complications reported for this procedure, but they have not been constant in large series of patients.7,8,11 Some authors consider there is potential risk for significant graft extrusion and implant failure when multilevel corpectomies are conducted, and ACCF accompanied by posterior instrumentation is recommended in such cases. 26 However, results from different series have debated the need for additional instrumentation as well.10,27,28 As shown above, previous studies have compared the clinical and radiological effects of ACDF and ACCF for the treatment of cervical deformity, and the data vary dramatically. It is uncertain what intervention is safer and more effective. In addition, the definitive and relative recommendations for each procedure have not been clearly defined. The objective of this study is to compare the clinical, radiographic, and surgical outcomes achieved by ACDF and ACCF in the treatment for cervical deformity in adult patients.
Methods
Search Strategy
We performed a systematic review of the literature, following the Cochrane Handbook of Systematic Reviews of interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for study selection. This study was registered in PROSPERO: International prospective registry of systematic reviews (CRD42021256069) The search strategy was created by a trained librarian (AH) using a combination of controlled vocabulary terms and keywords, and it was executed on April 16 2024 in MEDLINE (1946 to April 16 2024), Embase (1947 to April 16 2024), Scopus (1823 to April 16 2024), Cochrane Library (all available dates up to April 16 2024), Epistemonikos (all available dates up to April 16 2024), and ClinicalTrial.gov (all available dates up April 16 2024). Search was restricted to articles in English, Spanish and Portuguese, no time-date filters were used. Articles collected from the literature were downloaded into Endnote X20® for duplicate removal with subsequent study selection using Covidence®. The full search strategy is provided in Supplemental File, Complete Search Strategy.
Study Eligibility
Studies conducted in humans older than 18 years old with cervical deformity who underwent correction using an anterior technique (ACDF or ACCF). Studies investigating pediatric patients or only 1 of the 2 techniques were excluded. The bibliographies of the search results were independently reviewed by 2 authors (KB, MRC) to identify relevant articles that met the inclusion criteria (full text or abstract).
Data Extraction and Management
Articles collected from literature search were downloaded into Endnote X20® for duplicate removal with subsequent study selection using Covidence®. Data extraction was performed by 5 reviewers (KB, MRC, GT, MK, SS). 29 The data extracted included the following categories: (I) Study characteristics: Authors, Title, Journal, Year of publication, Country of origin. (II) Study design: Type of study. (III) Patient characteristics: Number of patients, age, gender. Characteristics of the intervention procedures: Indication for surgery, level. Outcomes as defined in the PICO strategy: Hospital Stay, Blood loss, Operation Time, JOA, NDI, VAS neck, radicular palsy, Fusion rates, Cobb angle, Graft subsidence/collapse, Graft dislodgement/migration, Dysphagia, Hoarseness, Infection, Epidural hematoma, Axial pain, T1 slope (T1S), T1 slope – C2-7 angle (T1-CL), and C2-7 SVA (cSVA).
Risk of Bias Assessment and Statistical Analysis
The “Cochrane Risk-of-Bias Tool for Randomized Trials” (ROB-2) 30 and the “Risk of Bias in Non-Randomized Studies of Interventions” (ROBINS-I) 31 were used to evaluate the quality of the studies included. The robvis web app was used for visualizing risk of bias assessment performed as part of the systematic review. 31 Meta-analysis was restricted to studies with low risk of bias. The data from each study was aggregated into a digital table using Microsoft Excel (Microsoft Office, Redmond, Washington). Subsequently, statistical analysis, including descriptive statistics for participant demographics and evaluations mean difference for outcome and complication, was carried out using Review Manager software version 5.4.1 (The Cochrane Collaboration, London, United Kingdom). This involved applying a random effects model for proportions in cases of heterogeneity and a fixed-effects model in instances of homogeneity. For the purpose of our analysis if a study did not reported an outcome measure, that study was not included in the model.
Results
Search results: 1625 relevant citations were selected for initial review according to the search strategies and provided data regarding anterior cervical discectomy and corpectomy in patients with cervical deformity. Of these, 1499 were initially excluded after reading the abstracts and 100 additional citations were excluded after full-text review (Figure 1). Finally, the systematic literature search generated 26 articles totaling 25,727 patients. PRISMA flowchart of literature search and article selection.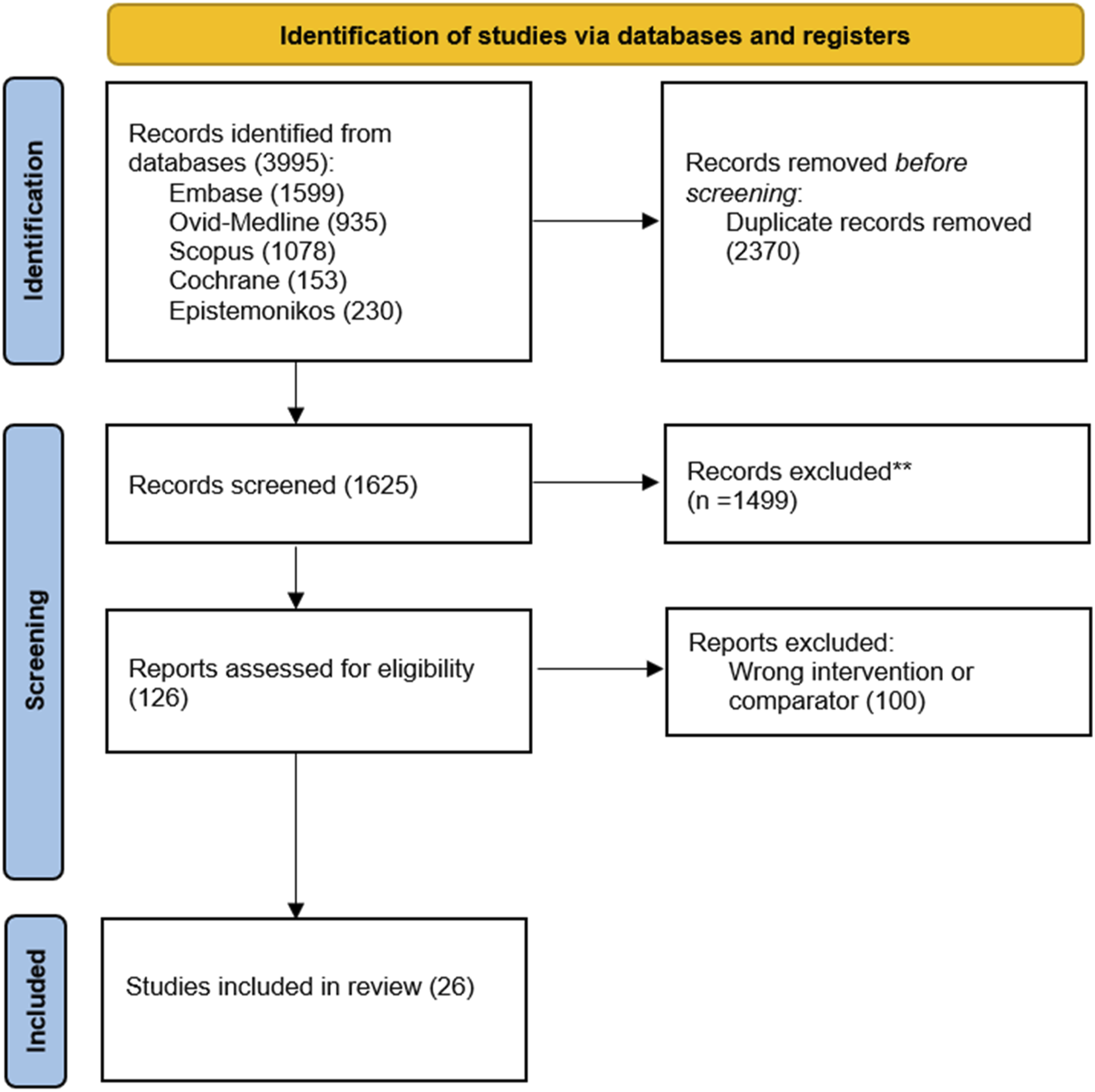
Baseline Characteristics and Quality Assessment
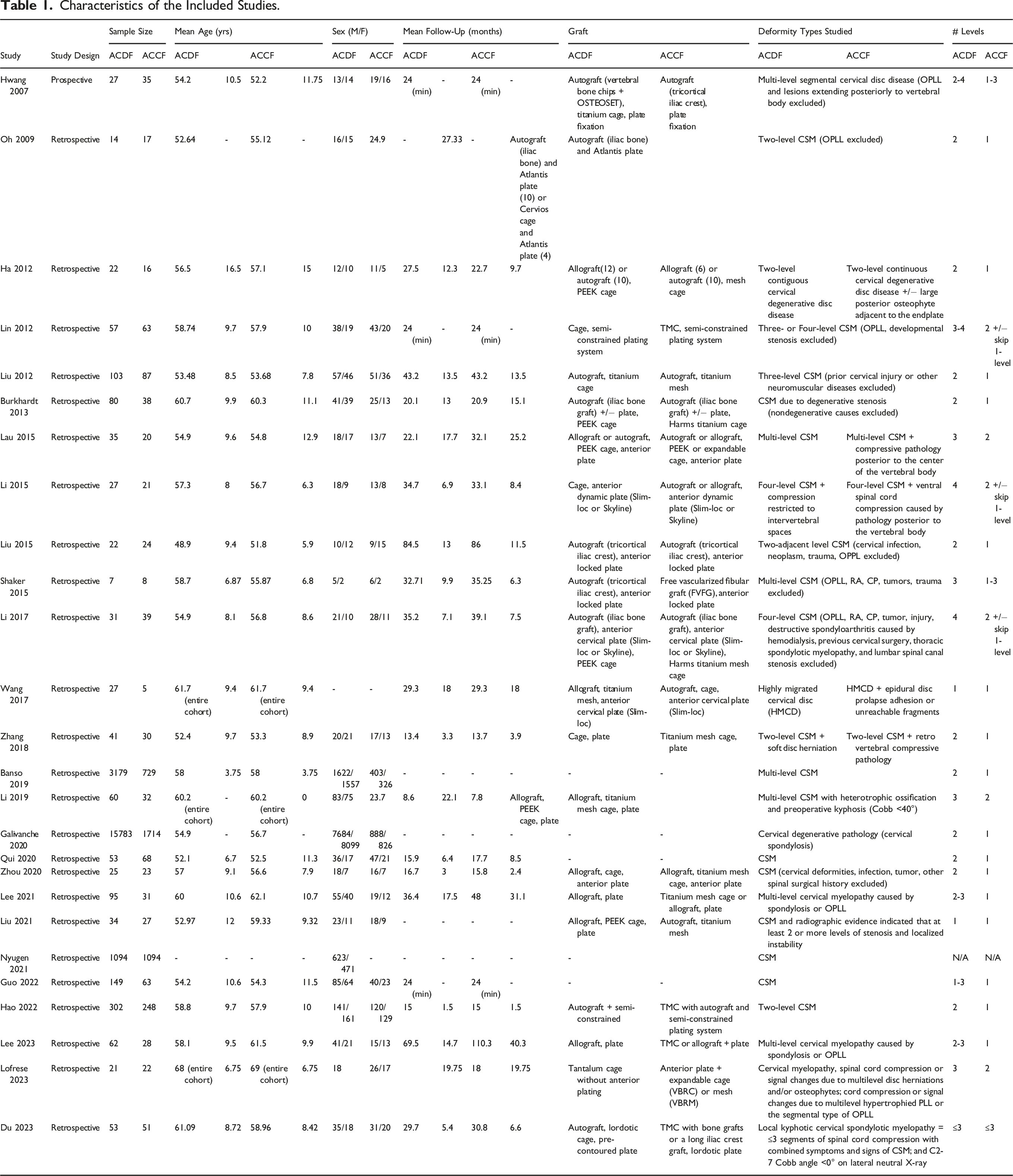
From the 26 studies included,7,32-56 21,194 ACDF patients and 4533 ACCF patients were identified. Mean age of patients was 55.5 years in the ACDF cohort and 54.5 years in the ACCF cohort. Mean follow-up was 27.2 months for both ACDF and ACCF cohorts. The risk of bias was assessed in accordance with the ROBINS-1, and a traffic light and summary of bias plot is shown in Figure 2. The overall risk of bias for 26 studies ranged from low to moderate; of these, 14 studies were deemed low risk of bias and considered for meta-analysis. The demographic data from the studies that met protocol inclusion criteria are displayed in Table 1. Summary and traffic light risk of bias in non-randomized studies. Characteristics of the Included Studies.
Clinical Outcomes
Japanese Orthopedic Association (JOA) Score
Eleven studies (1428 patients) reported preoperative (Supplemental file, Figure 1) and final follow-up (Supplemental file, Figure 2) JOA scores for ACDF and ACCF. This physician-oriented metric evaluates the neurological status of a patient using 6 domains and operates as a surrogate of patient satisfaction and level of functional recovery after surgical intervention. This meta-analysis showed no significant difference in preoperative JOA scores between ACDF and ACCF (OR [95% CI]: 0.06 [-0.14, 0.25], P = 0.57), with low heterogeneity (P = 0.40, I2 = 5%), as well as no significant difference in the final follow-up JOA scores (OR [95% CI]: −0.09 [-0.39, 0.20], P = 0.53), with moderate heterogeneity (P = 0.008, I2 = 58%). Compared to preoperative JOA scores, both ACDF and ACCF correlated with an upward trend in JOA scores at final follow up.
Neck Disability Index (NDI) Score
Seven studies (729 patients) reported preoperative (Supplemental file, Figure 3) and final follow-up (Supplemental file, Figure 4) NDI scores for ACDF and ACCF. This meta-analysis demonstrated no significant difference between ACDF and ACCF regarding either preoperative NDI scores (OR [95% CI]: −0.38 [-1.23, 0.47], P = 0.38), with moderate heterogeneity (P = 0.06, I2 = 50%), or final follow-up NDI scores (OR [95% CI]: 0.86 [-0.29, 2.00], P = 0.14), with high heterogeneity (P < 0.0001, I2 = 80%). Compared to preoperative NDI scores, both ACDF and ACCF showed lower NDI scores at final follow-up.
Visual Analog Scale (VAS) Neck Pain Score
Four studies (781 patients) reported preoperative (Supplemental file, Figure 5) and final follow-up (Supplemental file, Figure 6) VAS neck scores for ACDF and ACCF. This meta-analysis showed no significant difference between ACDF and ACCF for preoperative VAS neck scores (OR [95% CI]: −0.02 [-0.78, 0.74], P = 0.95), with moderate heterogeneity (P = 0.02, I2 = 69%). Although both surgical approaches yielded decreased pain scores postoperatively, final follow-up VAS neck scores favored ACDF (OR [95% CI]: 0.28 [0.05, 0.51], P = 0.02), with no heterogeneity (P = 0.50, I2 = 0%).
Radiographic Outcomes
C2-C7 Cobb Angle
Nine studies (682 patients) reported preoperative (Supplemental file, Figure 7) and final follow-up (Supplemental file, Figure 8) C2-C7 Cobb angle values for ACDF and ACCF. The C2-C7 Cobb angle is measured as the angle between 2 crossed perpendicular lines extended parallel to the inferior endplates of C2 and C7 on a standing lateral cervical spine radiograph. It is accepted as the gold standard for assessing cervical sagittal alignment, a key consideration in deformity correction. There was no significant difference between ACDF and ACCF in the preoperative C2-C7 Cobb angle (OR [95% CI]: −0.03 [-0.62, 0.55], P = 0.91), with low heterogeneity (P = 0.22, I2 = 25%), and ACDF yielded a better absolute C2-C7 Cobb angle than ACCF in the final follow-up (OR [95% CI]: −1.99 [-3.63, −0.34], P = 0.02), with high heterogeneity (P < 0.00001, I2 = 93%).
T1 Slope
Two studies (175 patients) reported pre-operative (Supplemental file, Figure 9) and final follow-up (Supplemental file, Figure 10) T1 slope values for ACDF and ACCF. This meta-analysis showed no significant difference between ACDF and ACCF for preoperative T1 slope (OR [95% CI]: −0.83 [-2.36, 0.69], P = 0.28), with no heterogeneity (P = 0.38, I2 = 0%). T1 slope was greater with ACDF than ACCF at final follow-up (OR [95% CI]: −3.29 [-5.21, −1.37], P = 0.0008), with low heterogeneity (P = 0.20, I2 = 38%).
C2-7 SVA
Two studies (161 patients) reported pre-operative (Supplemental file, Figure 11) and final follow-up (Supplemental file, Figure 12) C2-7 sagittal vertical axis (cSVA) values for ACDF and ACCF. This meta-analysis showed no significant difference between ACDF and ACCF for preoperative cSVA (OR [95% CI]: −0.89 [-3.03, 1.25], P = 0.41), with no heterogeneity (P = 0.51, I2 = 0%), or final follow-up cSVA (OR [95% CI]: −2.31 [-4.64, 0.03], P = 0.05), with low heterogeneity (P = 0.25, I2 = 24%).
T1 Slope – C2-7 Angle (T1-CL)
Two studies (175 patients) reported T1 slope and C2-7 angle at pre-operative (Supplemental file, Figure 13) and final follow-up (Supplemental file, Figure 14). From the raw data, the T1-CL was calculated as the difference between the T1 and C2-7 angle, and the standard deviation as the variance of the sum of their standard deviations. 57 In this meta-analysis, there was no significant difference between ACDF and ACCF with respect to TL-CL pre-operatively (OR [95% CI]: 0.13 [-0.81, 1.07], P = 0.79), with low heterogeneity (P = 0.61, I2 = 0%), or at final follow-up (OR [95% CI]: 0.98 [-1.64, 3.60], P = 0.46) with high heterogeneity (P = 0.009, I2 = 85%). Postoperatively, T1-CL increased for both techniques in 2 studies, decreased for both techniques in 2 studies, and decreased for ACDF but increased for ACCF in 1 study.
Fusion Failure
Nine studies (1298 patients) reported fusion failure rates (Supplemental file, Figure 15) for ACDF and ACCF. The criteria for fusion vary, but generally, include the following features: (i) no motion or instability across the fusion site on flexion-extension X-rays,32-34,36-39,41,42,49 (ii) the presence of bony bridging trabeculae across the fusion interface,33,34,36-39,41,42,47,49 or (iii) no lucency across the fusion site or around any of the screw sites.33,34,39,41,42,47 This meta-analysis demonstrated that ACDF is associated with a lower rate of fusion failure than ACCF, though not significantly (OR [95% CI]: 1.42 [0.68, 2.98], P = 0.35, with low heterogeneity (P = 0.32, I2 = 14%).
Graft Dislodgement
Seven studies (1166 patients) reported graft dislodgement rates (Supplemental file, Figure 16) for ACDF and ACCF. Graft dislodgement is used interchangeably with migration, extrusion, and dislocation. It is defined as the displacement of the graft beyond the leading edge of the upper had lower vertebral bodies by a distance greater than 2 mm on lateral radiographs . 35 In this meta-analysis, ACDF shows significantly lower graft dislodgement/migration rates than ACCF (OR [95% CI]: 4.74 [1.70, 13.22], P = 0.003), with no heterogeneity: P = 0.76, I2 = 0%).
Graft Subsidence
Four studies (794 patients) reported the incidence of graft subsidence (Supplemental file, Figure 17) for ACDF and ACCF. Graft subsidence refers to a loss of height of the fusion segments on lateral plain radiographs. The specific criteria for diagnosing graft subsidence varies with respect to how and when the loss of height is measured. A commonly used criterion is a >3 mm decrease in the height of the fused segments on imaging taken 1-2 days postoperatively and at bony fusion.34,35,39,49 This study found that ACDF procedures have lower graft subsidence rates (OR [95% CI]: 3.20 [1.45, 7.05], P = 0.004), with no heterogeneity: P = 0.67, I2 = 0%).
Operative/Surgical Outcomes
Operative Time
Ten studies (18656 patients) reported operative time (Supplemental file, Figure 18) for ACDF and ACCF. This meta-analysis showed that ACDF is associated with significantly lower operative time compared to ACCF (OR [95% CI]: 12.68 [0.71, 24.65], P = 0.04), with high heterogeneity (P < 0.00001, I2 = 95%).
Intraoperative Blood Loss
Eight studies (1041 patients) reported intraoperative blood loss (Supplemental file, Figure 19) for ACDF and ACCF. ACDF is significantly associated with less intraoperative blood loss than ACCF (OR [95% CI]: 114.08 [76.84, 151.23], P = 0.06), with high heterogeneity (P < 0.00001, I2 = 97%).
Length of Hospital Stay
Six studies (18376 patients) reported length of hospital stay (Supplemental file, Figure 20) for ACDF and ACCF. This meta-analysis showed that ACDF has a shorter length of hospital stay than ACCF (OR [95% CI] 1.25 [0.14, 2.36], P = 0.03, with high heterogeneity (P < 0.00001, I2 = 93%).
C5 Palsy
Five studies (474 patients) reported the incidence of C5 palsy (Supplemental file, Figure 21) for ACDF and ACCF. ACDF has a lower incidence of C5 palsy than ACCF, but not to a significant degree (OR [95% CI]: 1.44 [0.63, 3.27], P = 0.38), with low heterogeneity (P = 0.39, I2 = 2%).
Dysphagia
Nine studies (1222 patients) reported the incidence of dysphagia (Supplemental file, Figure 22) for ACDF and ACCF. In this meta-analysis, no significant difference exists in dysphagia rates for ACDF and ACCF (OR [95% CI]: 1.12 [0.71, 1.78], P = 0.62), with no heterogeneity: P = 0.91, I2 = 0%).
Hoarseness
Seven studies (1144 patients) reported the incidence of hoarseness (Supplemental file, Figure 23) for ACDF and ACCF. There is no significant difference between ACDF and ACCF for the incidence of hoarseness (OR [95% CI]: 1.01 [0.50, 2.02], P = 0.99), with no heterogeneity: P = 0.87, I2 = 0%).
Epidural Hematoma
Four studies (866 patients) reported the rate of epidural hematoma (Supplemental file, Figure 24) for ACDF and ACCF. No significant difference is found between ACDF and ACCF in the incidence of epidural hematoma (OR [95% CI]: 1.78 [0.24, 13.05], P = 0.57), with moderate heterogeneity: P = 0.08, I2 = 56%).
Axial Pain
Two studies (260 patients) reported the incidence of axial pain (Supplemental file, Figure 25) for ACDF and ACCF. This meta-analysis demonstrated no significant difference in the rate of post-operative axial pain for ACDF and ACCF (OR [95% CI]: 2.47 [0.23, 26.61], P = 0.45), with low heterogeneity: P = 0.25, I2 = 26%).
Infection
Seven studies (18009 patients) reported the infection rate (Supplemental file, Figure 26) for ACDF and ACCF. No significant difference exists between ACDF and ACCF with respect to infection rate (OR [95% CI]: 1.37 [0.73, 2.57], P = 0.33), with no heterogeneity (P = 0.84, I2 = 0%).
Discussion
Clinical outcomes are arguably the most considerable factor in spine surgery decision-making because they represent how an intervention directly affects patients’ neurological status and quality of life. Assessing improvement after cervical deformity reconstruction requires considering nerve function. The Japanese Orthopedic Association (JOA) is a disease-specific scoring measure for cervical myelopathy, whereas Neck Disability Index (NDI) and Visual Analog Scale (VAS) are patient-reported outcome measures. Our study provides evidence that the total gain in JOA and NDI varies consistently between the 2 surgical approaches, but ACDF is modestly advantageous in reducing VAS scores for neck pain. Notably, all 3 clinical measures improved for both cohorts from the preoperative to final follow-up timepoint. These findings are consistent with previous meta-analyses.14-17 They indicate that, while there may not be a strong difference in the clinical efficacy between ACDF and ACCF, both anterior cervical surgical approaches effectively decompress the spinal cord and nerve roots while returning cervical lordosis to ultimately improve patients’ nerve function and quality of life. Where clinical benefits are comparable between both ACDF and ACCF, it may be valuable to determine the optimal surgical approach by considering which yields better radiographic results and minimizes complications, given a patient’s unique cervical spine deformity.
Radiographic outcomes reflect biomechanical changes that carry clinical and functional implications, such as persistent pain or ability to maintain horizontal gaze. Besides decompression, correction of sagittal alignment is a critical goal of ACDF or ACCF. Cervical sagittal balance has been shown to correlate with health-related quality of life (HRQOL),58-61 and C2-C7 Cobb angle, T1 slope – Cobb angle mismatch, and C2-7 SVA are key players. This meta-analysis indicates that ACDF is significantly more effective than ACCF in yielding a lordotic C2-C7 Cobb angle at final follow-up. Previous reviews15-17 share this trend, suggesting that ACDF may be a preferred surgical approach for restoring cervical sagittal alignment in the setting of cervical spine deformity for the following reasons: i) The shape of the interbody graft/spacer in ACDF allows superior control for restoring cervical lordosis than meshes/grafts used in ACCF. 62 Interbody grafts in ACDF can be adjusted in ways to promote lordotic angle, whereas meshes/grafts in ACCF may straighten the cervical spinal column between the remaining vertebral bodies, resulting in loss of Cobb. 17 (ii) ACCF only provides 2 points of fixation; whereas ACDF affords more fixation points that pull the involved vertebral bodies toward the lordotic anterior plate to restore alignment.17,35 (iii) The magnitude of removal and reconstruction is larger in ACCF. ACDF only replaces the vulnerable intervertebral disc with graft/spacer that enables an almost normal cervical spinal column postoperatively. In comparison, ACCF removes 1 or more vertebral bodies to create a larger defect, which requires more intervention and greater room for error in recovering cervical lordosis.32,63
In addition to C2-7 Cobb angle, T1-slope-CL mismatch and C2-7 SVA are markers of cervical alignment that reflect severity of cervical deformity. 64 In this meta-analysis, there was no clear trend for either cohort with respect to C2-7 SVA, but studies showed that T1 slope increased at final follow-up with both anterior techniques. However, changes at the T1 level are a result of spinopelvic changes inferior to the level, rather than a result of cervical deformity correction. Instead, the Ames classification for cervical spine deformity highlights T1-CL mismatch as a cervical deformity modifier. This parameter has been considered the cervical counterpart of the thoracolumbar relationship of PI-LL. Just as an increase in PI requires a greater LL to compensate, greater T1 slope requires more cervical lordosis to maintain cervical sagittal alignment. 65 In our meta-analysis, 5 studies with either low or moderate risk-of-bias included both T1 slope and CL values. While no significant difference in T1-CL was found between approaches, postoperative T1-CL was <15°, corresponding to a score of zero in the Ames classification, in all studies, except for Du 2023. Though the Ames classification does not correlate its scores with HRQOL, studies, like Lan et al, have demonstrated that, as T1-CL mismatch increases, there is more strain on posterior neck muscles to maintain horizontal gaze, worsening neck pain and disability. 66 Therefore, in as much as anterior approaches restore cervical lordosis, and thereby lower T1-CL, they are associated with better clinical prognosis. More studies are required to characterize cutoffs regarding this parameter and its correlation to clinical phenotypes of cervical deformity.67-69
ACDF fusion failure rates showed a lower trend than ACCF in this meta-analysis, though it did not significantly differ between the 2 procedures. This is consistent with previous meta-analyses14-16 and challenges studies that argue multi-level ACDF has a high rate of non-union due to more graft-host interface (7, 22). The lack of significant difference in fusion shown here can be attributed to several factors. One explanation is the heterogeneity in the types of graft material and fixation devices used in the studies included in this analysis (Table 1). This can impact the rates of fusion failure in both procedures. Varying criteria for successful fusion across studies can also contribute to differences in observed rates of fusion failure. It is worth noting that 1 previous meta-analysis 17 reported a significant decrease in the rate of fusion failure with ACDF. The degree of segmental motion permitted with the 2 ventral decompression techniques may be a factor, as a longer fused segment with less points of fixation in ACCF may result in greater motion at the fused level, increasing the risk of fusion failure. 70 While Wang et al suggest that ACDF is associated with a lower incidence of fusion failure than ACCF, it is crucial to consider individual patient characteristics when selecting the appropriate surgical approach, since the lack of a statistically significant difference in this larger, pooled cohort highlights the importance of careful deliberation in clinical practice.
This meta-analysis shows that ACDF has significantly lower rates of graft dislodgement. Graft dislodgement is a complication that can lead to poor clinical outcomes and the need for revision surgery. Wang et al, 2016 shows a pattern of lower graft dislodgement rates in ACDF compared to ACCF, providing more evidence to support the validity of the trend observed in this current meta-analysis. One potential reason why ACDF may have lower rates of graft dislodgement is that it provides more points of fixation to hold the implant in place and better resistance to displacement, whereas ACCF has only 2 points of fixation.17,71,72 The size of the defect and corresponding graft may also play a role. ACCF creates a larger defect that requires a larger graft or cage to be placed. 73 The lower incidence of graft dislodgement in this meta-analysis argues in favor of ACDF as the more stable fixation technique in the long-term.
According to our study, as with graft dislodgment rates, ACDF also produces better results than ACCF with respect to graft subsidence. This adds to existing evidence in favor of ACDF over ACCF regarding graft subsidence. Indeed, consistency with previous meta-analyses16,17 strengthens the robustness of our findings, although factors such as bone graft material, device size and shape, and placement and fixation technique may influence the risk of graft subsidence. The lower graft subsidence rates in ACDF may be due to various factors. A main reason is the load of the construct in ACDF is shared by the screws in the intervening segment and 2 terminal segments. In ACCF, the screws are only present at the cranial and caudal vertebral segments, and of the 2, the caudal end plate of the corpectomy bears the full load. 74 The contact area of the graft is also smaller for ACCF than for ACDF, generating higher shear stress in ACCF. 16 These factors may accelerate graft absorption into the end plate of the adjacent vertebral body, causing the treated segment to subside. It is worth noting that since only 3 studies reported extractable subsidence rates, more studies are necessary to determine the validity of mechanisms put forth here. Nevertheless, according to the available data, this meta-analysis shows that ACDF has a significantly lower incidence of graft subsidence than ACCF.
Operative outcomes are valuable insofar as they reflect surgical morbidity to the patient and potential drivers of health care cost. According to our meta-analysis, ACDF is significantly better than ACCF at reducing operative time, intraoperative blood loss, and length of hospital stay. Intuitively, ACDF is a faster surgical procedure that results in less bleeding. 16 Guan et al shared the superiority of ACDF regarding operative time, blood loss, and length of stay, while Wang et al and Han et al also found less blood loss with ACDF.14,15,17 The consistency of these findings suggests ACCF is associated with more surgical morbidity than ACDF. Removing a vertebral body is a more invasive surgical approach than removing an intervertebral disc. ACCF involves performing a 15-19 mm anterior midline trough in the vertebral body, extending down to the posterior longitudinal ligament, plus excising the upper and lower discs adjacent to the affected area.33,63,75 This requires more time for the removal stage and preparation of the graft to fit the trough. Meanwhile, ACDF is only associated with removing the affected intervertebral disc tissue and plugging the graft.63,75 Compared to ACDF, ACCF involves greater exposure of the spinal cord, increasing the risk for spinal cord injury. This, along with the fact that ACCF is more time consuming and surgically traumatic, may explain why ACDF patients recover faster, whereas ACCF patients tend to experience a longer hospital stay.
No significant difference between techniques was found in this meta-analysis regarding dysphagia, hoarseness, epidural hematoma, axial pain, infection rates. This held true when all 26 included studies were analyzed as well as when only the 14 high-quality studies were. Previous meta-analyses share these findings.15-17 Contrary to these studies, our meta-analysis showed ACDF to be significantly better at reducing the incidence of C5 palsy when analyzing both low- and moderate-risk studies, a gain that became modest with only low-risk studies. Nevertheless, as a clinically difficult complication, C5 palsy warrants some attention. C5 nerve root palsy is defined as a “mostly unilateral severe weakness of the deltoid and a concomitant mild to moderate weakness of the biceps muscle with additional sensory loss and pain in the C5 dermatome.76,77 Even though postoperative C5 palsy typically has a good prognosis with spontaneous full recovery in most cases, it seriously affects patients’ function during rehabilitation. Multiple explanations have been proposed as to the pathophysiology of postoperative C5 nerve root palsy, including stretching and tethering of the C5 nerve root following dorsal decompression, a pre-existing subclinical C5 nerve root compression due to a tight C4/5 foramen, excessive intraoperative traction, unique anatomical course of the C5 nerve root, lack of myotome supply redundancy, spinal cord ischemia due to decreased blood supply from radicular arteries, reperfusion injury of the spinal cord, or iatrogenic injury. 78 The exact contribution of these factors varies according to technique and surgeon expertise and is still not exactly understood. However, considering the shift of the spinal cord in the setting of ventral decompression and its impact on the unique trajectory of the C5 nerve roots offers a unique biomechanical perspective into pathogenesis of this phenomenon. Anterior approaches decompress the spinal cord in a way that ventrally shifts the cord and can potentially kink the C5 nerve as it exits the neuroforamen. 78 Since a corpectomy involves removing the vulnerable vertebral body, adjacent discs, and the posterior longitudinal ligament, as opposed to only the vulnerable intervertebral discs, it yields a more drastic forward shifting of the spinal cord. Additionally, cadaver studies have demonstrated that C5 ventral rootlets are shorter and exit more obtusely from the spinal cord than lower rootlets, while C5 upper dorsal rootlets angle much less inferiorly from the cervical cord than other dorsal cervical rootlets.79,80 These distinct anatomic features increase the vulnerability of the C5 nerve root with more extensive decompression. This explanation is shared by other studies that observe a trend increasing C5 palsy rates as the number of levels operated increased. The difference in the magnitude of this ventral shift between ACDF and ACCF procedures plus the unique anatomy of C5 rootlets are biomechanical players for the significantly lower rates of C5 nerve root palsy with ACDF than ACCF observed in this meta-analysis.
Limitations and Future Direction
Assessing methodological quality reveals several key limitations of this meta-analysis. First, this study does not offer a complete quantitative synthesis culminating in a surgical algorithm due to the difficulty in finding an appropriate method to transform the different summary metrics found in the included studies. This can be accounted for by various factors. First, 6 key outcomes (JOA, NDI, C2-C7 Cobb angle, operative time, blood loss, and length of stay) all displayed a moderate-to-high degree of heterogeneity, which could have an unstable impact on the consistency of the results. Whether this heterogeneity is methodological or clinical requires further analysis, such as subgrouping by levels operated. We aimed to minimize the methodological heterogeneity by analyzing only high-quality studies in the meta-analysis. However, as it is, certain outcomes were measured by very few studies, and studies rarely reported results by number of levels operated, making this very difficult. Second, there was no RCT comparing the results of ACDF and ACCF; this is necessary for generating evidence with a strong causative effect. That said, our study echoes the superior safety profile of ACDF with respect to operative time, blood loss, and length of stay found in Guan et al, a meta-analysis of only RCTs. Third, the search method was limited to articles in English, Spanish and Portuguese. Due to the difficulty in acquiring precise medical translations, articles with potentially high-quality data that were published in other languages were excluded.
Conclusions
The sustainability or longevity of improvement following anterior cervical spine surgery approaches has only seldom been explored. This is 1 of the largest pooled meta-analyses comparing the effectiveness and safety of 2 prevalent ventral decompression and realignment techniques. Both ACDF and ACCF procedures similarly improve clinical outcomes in cervical spine deformity patients. However, according to this pooled meta-analysis, ACDF is significantly more efficacious at recovering cervical lordosis while minimizing graft-related complications, surgical trauma (ie, operative time, length of hospital stay), and the incidence of postoperative C5 palsy. Future sub-group analyses by number of levels operated are encouraged to clarify the heterogeneity apparent in this meta-analysis in an effort to produce a more granular surgical approach selection algorithm.
Supplemental Material
Supplemental Material - A Meta-Analysis of Surgical Outcomes in 25727 Patients Undergoing ACDF or ACCF for Cervical Deformity
Supplemental Material for A Meta-Analysis of Surgical Outcomes in 25727 Patients Undergoing ACDF or ACCF for Cervical Deformity by Karma Barot, Miguel A. Ruiz-Cardozo, Som Singh, Gabriel Trevino Michael Ryan Kann, Samuel Brehm, Tim Bui, Karan Joseph, Rujvee Patel, Angela Hardi, Alexander T. Yahanda, Julio J. Jauregui, Magalie Cadieux, Brenton Pennicooke, and Camilo A Molina in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author JJJ is an editorial board member for Children. Editor in Chief, Acra SA. Author CAM reports being a consultant for Stryker, Augmedics, DePuy Synthes, and Kuros Biosciences. Author BP consults for Pacira Biosciences and is an external advisor for McKinsey & Company. The remaining authors have no conflicts of interests or disclosures. All authors declare that this report was conducted in the absence of any commercial or financial relationships.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.