
Abstract
Background
The retrospective study was conducted to compare the efficacy of anterior cervical discectomy and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF) for localized ossification of the posterior longitudinal ligament (OPLL) by evaluating clinical and radiologic outcomes.
Methods
We reviewed 151 patients to assess the effects of treatment for one or two levels localized OPLL. Perioperative parameters, such as blood loss, operation time and complications, were recorded. Radiologic outcomes, such as the occupying ratio (OR), fusion status, cervical lordosis angle, segmental angle, disc space height, T1 slope, and C2–C7 sagittal vertical axis (SVA), were assessed. Clinical indices, such as the JOA scores and VAS scores, were investigated to compare the two surgical options.
Results
There were no significant differences in the JOA scores or VAS scores between the two groups (p > 0.05). The operation time, volume of blood loss and incidence of dysphagia were significantly less in the ACDF group than in the ACCF group (p < 0.05). In addition, cervical lordosis, segmental angle and disc space height were significantly different from their preoperative evaluations. No adjacent segment degenerated in the ACDF group. The subsidence rates of implants were 5.2% in the ACDF group and 28.4% in the ACCF group. The degeneration of the ACCF group was 4.1%. The incidence of CSF leaks was 7.8% in the ACDF group and 13.5% in the ACCF group. All the patients ultimately achieved successful fusion.
Conclusion
Although both options achieved satisfactory primary clinical and radiographic efficacies, ACDF was associated with a shorter surgical procedure, less intraoperative blood loss, better radiologic outcomes, and lower incidence of dysphagia than ACCF.
Keywords
Introduction
Since its first reports in 1960 by Tsukimoto, 1 ossification of the posterior longitudinal ligament (OPLL) is a common cause of cervical myelopathy. With the advancement of imaging technology, it has become increasingly common due to improvements in detection, especially in Asian countries. Although the reported prevalence of OPLL in Asians ranges from 1.9% to 4.3%, 2 most patients with OPLL appear to be asymptomatic. 3 It is defined as the lamellar bone deposition at the site of posterior longitudinal ligament. 4 It seems to be a persistent pathological development process which is different from osteophytes which formed from the degenerated disc. When an ossified ligament results in spinal stenosis, clinical symptoms and secondary cervical spondylosis can develop. 5 Operative treatment can block the natural process of OPLL to prevent further deterioration in compression of the spinal cord. 6
OPLL is morphologically classified into localized, segmental, continuous and mixed types. 7 Localized OPLL refers to the ossified masses of the upper corner of lower vertebra and the lower corner of upper vertebra fused at the intervertebral space. 8 Anterior surgery allows resection of the ossified mass to achieve direct decompression because the primary pathological mechanism of OPLL is spinal cord compression. ACDF and ACCF are two practical methods that are used for spinal decompression and cervical lordosis reconstruction for the treatment of severe spinal stenosis. 9 However, the subject of alternative surgical modalities is still controversial. Most surgeons prefer ACCF because it is easier to extirpate ossification. However, many complications frequently occurs in ACCF. 2 Although the small incision in ACDF brings technical demands in decompression, it can avoid the removal of vertebral bodies to reduce the damage. It has also been demonstrated that ACDF leads to lower perioperative complication rates than ACCF. 10 Smith, Robinson and Cloward described ACDF as a safe and efficient strategy for degenerative cervical spondylosis in 1958. 11 However, to date, few studies have compared the clinical efficacy of these two techniques in the treatment of localized OPLL, and little is known about the outcomes of ACDF for localized OPLL. Thus, we analyzed the clinical and radiographic outcomes to compare the efficacy of ACDF and ACCF in this retrospective study.
Materials and methods
Patient enrollment and inclusion criteria
This retrospective and comparative clinical study was from January 2018 to January 2021. We selected a total of 151 consecutive patients based on the timing of presentation who were without lost follow-up. When we confirmed the diagnosis of the localized OPLL by imaging examination, the surgeon considered both ACDF and ACCF to be feasible surgical methods. Patients were informed of the advantages and disadvantages of ACDF and ACCF in detail before surgery. ACDF is more minimally invasive than ACCF while ACCF decompress more thorough than ACDF. Finally, they were subsequently divided into two groups based on their choice (77, ACDF group; 74, ACCF group). The same physician recorded and evaluated the results of the follow-ups. All procedures performed in study were approved by the Institutional Ethics Committee of Soochow University. The surgeries were performed by the same experienced orthopedic surgeon.
The following were inclusion criteria: (1) symptoms such as refractory cervical radiculopathy with or without cervical myelopathy caused by localized OPLL; (2) findings showing localized OPLL by computed tomography (CT), and magnetic resonance imaging (MRI); (3) underwent anterior cervical surgery.
Patients were excluded when (1) no symptoms caused by localized OPLL; (2) other types of OPLL (3) received other cervical spine surgery for tumors, fractures and so on; (4) anterior surgery combined with posterior surgery.
Operative procedure
The ACDF and ACCF techniques were performed via a standard cervical anterior approach. 11 After discectomy or corpectomy, titanium mesh cages (PYRAMESH, Medtronic Inc, USA) with anterior plates (VENTURE, Medtronic Inc, USA) were used for ACCF and zero-profile anchored spacer (ROI-C, LDR, Troyes, France) with clips for ACDF. Excised cancellous osteophytes mixed with 0.25 mg of recombinant human bone morphogenetic protein (rhBMP-2, Pharmaceutical Group Inc, Hangzhou, China) were used as bone grafts for fusion.
Regardless of one-level or two-level localized OPLL, ACCF is used to deal with the corresponding vertebrae with upper and lower intervertebral discs. For one-level and two-level localized OPLL, ACDF is used to deal with the corresponding intervertebral discs.
Clinical evaluation
Bazaz grading system for dysphagia.

Odom criteria.

Radiologic evaluation
Figure 1 shows the measurement of cervical spine parameters on the X-ray. (A)Cervical lordosis was measured by Cobb angle of C2-7 which formed between the inferior endplate of C2 and C7; (B)Segmental angle was the angle between the superior and inferior endplates of the fused vertebral body; (C) Disc space height was the distance between the midlines of the involved cranial and caudal vertebral bodies; (D) C2-7 sagittal vertical axis (SVA) was the length from the postero-superior corner of C7 and the vertical line from the center of the C2 body; T1 slope was the angle between the upper endplate of T1 and the horizontal line. The CT scan can measure the occupying ratio (OR), which was determined by the ratio of the maximum anteroposterior diameter of the OPLL to the anteroposterior diameter of the spinal canal. Implant subsidence was considered when the loss of disc space height was more than 2 mm at the final follow-up compared with measurements taken at 1 month postoperatively. Fusion was considered when there was no activity between the spinous processes, no radiolucent gap between the graft and endplate and continuous bridging of the trabecular bone at the graft and plate interface.
13
Measurement of cervical spine parameters: (a) C2-7 Cobb angle; (b) Segmental angle; (c) Disc space height; (d) C2-7 sagittal vertical axis; T1 slope.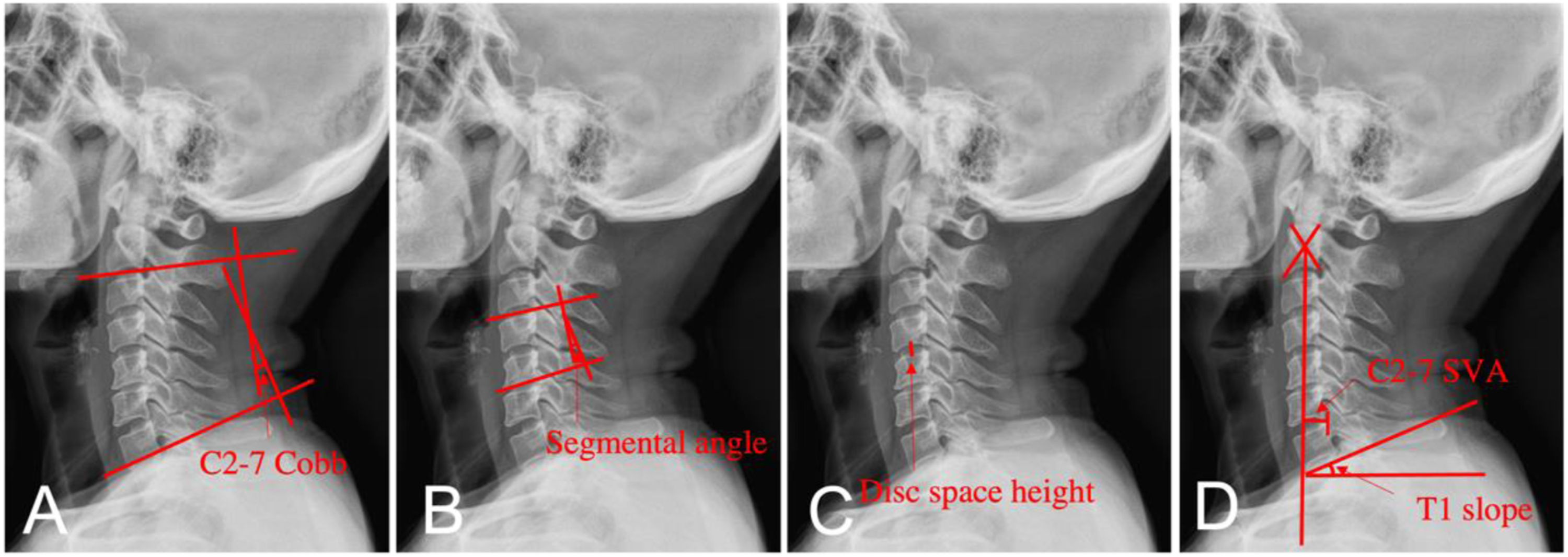
Statistical analysis
We analyze all statistics by performing SPSS version 26.0 (Chicago, IL, USA). Quantitative results are expressed as the mean and standard deviation. We used an independent t test for intergroup comparisons. We performed a paired t test before and after the operation. The chi-square test was used to compare the complications between the groups. When p values were less than 0.05, the results were recognized as significantly different.
Results
Patient demographics
Preoperative patient data and operative details in the two groups undergoing different methods.

ACDF: anterior cervical discectomy and fusion, ACCF: anterior cervical corpectomy and fusion, OR: occupation rate, CSR: cervical spondylotic radiculopathy, CSM: cervical spondylotic myelopathy.
Surgical outcomes
For patients with single localized OPLL, we performed single-level ACDF or single-level ACCF. For patients with dual localized OPLL, we performed two-level ACDF or single-level ACCF. In the ACDF group, the mean operation time for one level was 82.6 ± 6.9 min. In the ACCF group, the mean operation time was 131.9 ± 24.5 min. The corresponding volumes of blood loss were 37.9 ± 15.4 and 129.0 ± 22.5 ml, respectively. The operation times for the two levels were 128.0 ± 11.3 and 176.2 ± 23.1 min, respectively. The corresponding blood loss was 58.3 ± 12.5 and 162.5 ± 26.6 ml, respectively. At either the single or two levels, ACDF significantly reduced the time of the surgical procedure and the volume of intraoperative blood loss when compared with ACCF (p < 0.05).
Clinical outcomes
The mean outcomes of clinical parameters reviewed before operation and during follow-up (mean ± SD).

JOA scores: Japanese orthopedic association scores, RR: recovery rate, VAS scores: visual analogue scale scores.
#p < 0.05 comparing with preoperative value.
Radiologic outcomes
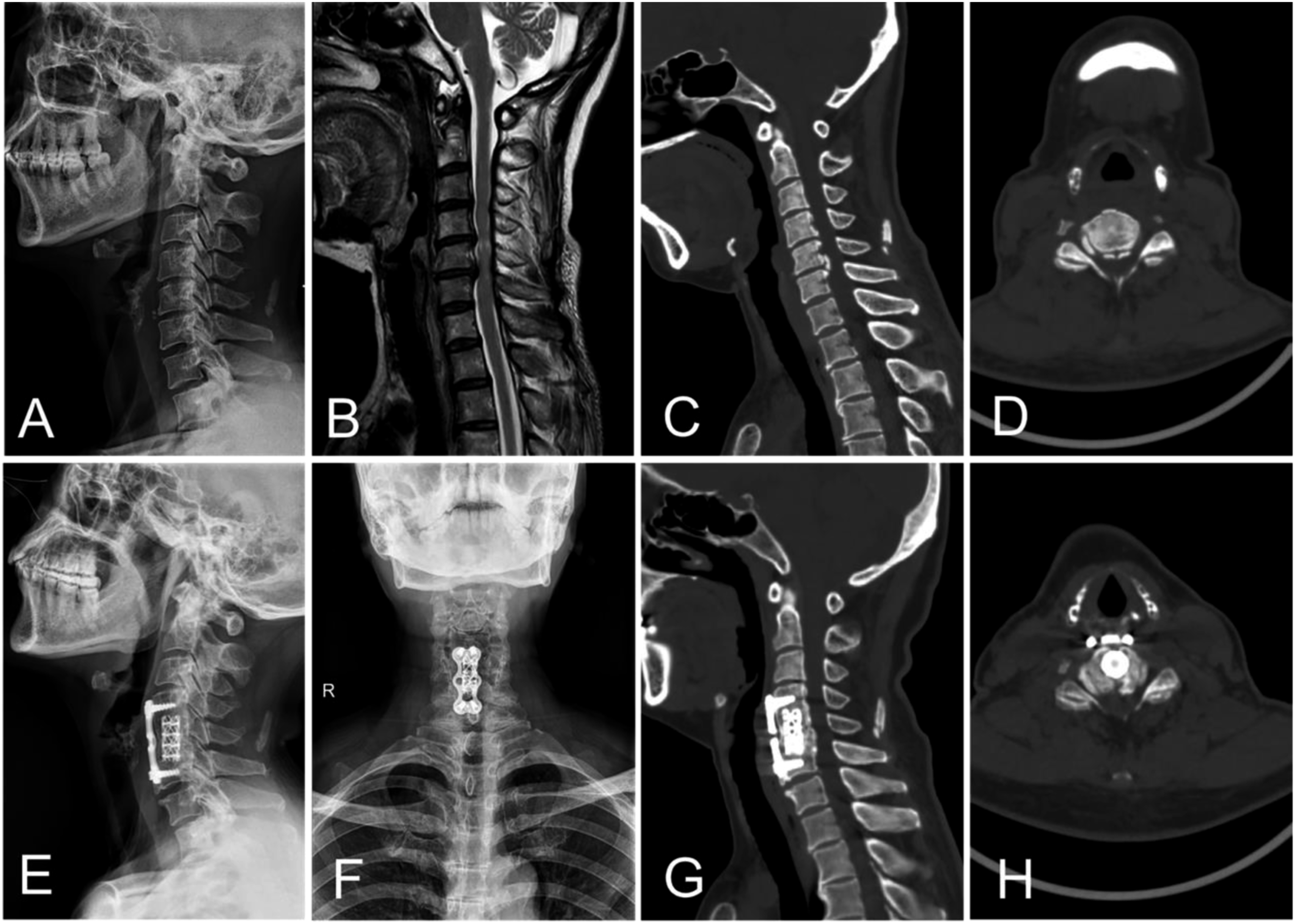
Figures 2 and 3 show representative images for one patient in each group. Table 5 lists a summary of the radiographic outcomes. The two groups showed a similar baseline before surgery (p > 0.05). The occupying rate in both groups were 40.6 ± 6.3% and 39.1 ± 10.1% which showed the similar severity of OPLL. In the ACDF group, the disc space height was 5.1 ± 1.1 mm preoperatively and 7.3 ± 0.8 mm in the final follow-up, the cervical lordosis was 16.4 ± 12.4° preoperative and 24.5 ± 9.2° in the final follow-up. In the ACCF group, the disc space height was 4.9 ± 0.9 mm preoperatively and 6.0 ± 0.8 mm in the final follow-up, the cervical lordosis was 13.8 ± 9.7° preoperative and 18.1 ± 10.5° in the final follow-up. The disc space height, the cervical lordosis angle, and the segmental angle increased in the ACDF group, which was significantly better than the corresponding parameters in the ACCF group (p < 0.05). The T1 slope improved from 20.2 ± 5.0° to 23.8 ± 4.9° in the ACDF group and from 18.9 ± 4.9° to 20.7 ± 4.8° in the ACCF group. ACDF showed more improvement than ACCF (p < 0.05). The C2–C7 SVA increased from 15.4 ± 7.1 mm to 18.6 ± 7.8 mm in the ACDF group and from 14.8 ± 9.6 mm to 18.2 ± 7.8 mm in the ACCF group at the last follow-up. We did not observe a difference (p > 0.05). At six months after the surgery, 66.2% and 40.5% patients in the two groups showed continuous bridging of trabecular bone on the X-ray. In the final follow-up, solid fusion was successfully achieved in all patients. Figure 4 shows a representative case. The preoperative lateral radiograph (a), sagittal T2-weighted magnetic resonance image (b), sagittal CT image (c) and CT scan (d) of 45-year-old female patient showed localized OPLL at C5–C7 levels. The postoperative anteroposterior (e) and lateral (f) radiograph showed anterior cervical discectomy and fusion with the zero-profile anchored spacers (ROI-C). The postoperative sagittal CT image (g) and CT scan (h) showed excellent decompression. The preoperative lateral radiograph (a), sagittal T2-weighted magnetic resonance image (b), sagittal CT image (c) and CT scan (d) of 56-year-old female patient showed localized OPLL at C5-C6 levels. The postoperative anteroposterior (e) and lateral (f) radiographs showed anterior cervical corpectomy and fusion with the Titanium cages and plates. The sagittal CT image (g) and CT scan (h) of 1-year follow-up showed solid fusion and excellent decompression. The mean outcomes of radiological parameters measured before operation and during follow-up (mean ± SD). SVA: sagittal vertical axis. #p < 0.05 comparing with preoperative value. The preoperative lateral radiograph (a), sagittal T2-weighted magnetic resonance image (b), sagittal CT image (c) and CT scan reconstructions (d) of 59-year-old female patient showed at localized OPLL C4–C5 level, in whom the anterior cervical discectomy and fusion (ACDF) was performed with the zero-profile anchored spacers (ROI-C). The postoperative lateral radiographs (e) and sagittal CT image (f) showed a satisfactory improvement of the cervical lordosis. The sagittal CT image (g) and CT scan (h) of 6-months follow-up showed adequate fusion and excellent decompression.


Complications
Complications after operations in the two groups.

ASD: adjacent segment degeneration, CSFL: cerebrospinal fluid leak.
Discussion
OPLL may progress more aggressively and tend to cause various symptoms. Osteophyte compression of nerve roots causes the symptoms of cervical radiculopathy and that of spinal cord causes the symptoms of cervical myelopathy. The occupying rate in both groups were 40.6 ± 6.3% and 39.1 ± 10.1% respectively. In our study, osteophytes at the level of the vertebral space alone were prominent as the cause of neurological symptoms and this degree of OPLL is more suitable for anterior approaches than posterior approaches. Meanwhile, there was no significant difference in types of symptoms between two groups. Although anterior approach is more technically demanding, it allows direct decompression, which may be related to better prognosis and less progression. 14 Usually, ACDF is chosen for milder cases, while ACCF is not done for CSR. Localized OPLL is usually asymptomatic at the very beginning. Patients’ symptoms are aggravated by disc herniation at the same intervertebral space level or due to neurological symptoms caused by disc injury because of recent trauma. For this reason, ACDF may achieve the same efficacy as ACCF by resecting the herniated disc and OPLL at the intervertebral space level with much less surgical injury than ACCF. The limited surgical exposure and the adhesion of the OPLL to the dura make the operation more difficult. Therefore, ACDF was considered to perform only when the preoperative CT scan showed that the OPLL did not extend to the entire posterior margin of the vertebrae.
In this study, we found that the volume of blood loss and duration of surgical procedure were significantly less in patients undergoing ACDF than in patients undergoing ACCF. The majority of previous studies were in accordance with our results. 15 This difference is because ACCF requires resecting the corresponding vertebral body and the adjacent disc, which is more traumatic. However, Lin et al. 16 found that the duration of the ACDF surgical procedure was significantly longer than that of the ACCF procedure, which was contrary to our study. He believed that performing ACDF to remove osteophytes from the intervertebral space is time-consuming and more technically challenging. The reason why many scholars perform ACCF is that the difficulty of ACDF is much greater than that of ACCF. The limited surgical exposure and the adhesion of the OPLL to the dura make it difficult to decompress sufficiently. However, when the technical learning curve of ACDF is mature, it is a more advantageous surgical method.
ACCF and ACDF not only relieves compression in the spinal cord but also reconstructs the physiological parameters of the cervical spine through careful distraction of the intervertebral space. 17 Burkardt et al. 18 showed that ACDF had better maintenance of disc space height and greater improvements in cervical lordosis. Our study corresponded with it. Compared with patients who underwent ACCF, the postoperative disc space height was significantly improved in those who underwent ACDF. However, disc space height dropped slightly in both groups when they came to review and the ACCF group decreased more than the ACDF group. The reduced height of the treated disc space was partly due to postoperative subsidence of implant settling and then migrating to the endplates. The subsidence rate of implant in our study was 5.2% in the ACDF group and 28.4% in the ACCF group. We thought that the difference of subsidence rate was related to the shape of both ends of the implant. The main causes of abnormalities in patients who undergo ACCF may be related to excessive damage to the vertebral endplate and the rigid effect of the titanium cage. The contact surface of the titanium cage is sharper. Under the action of stress, it is more likely to protrude to the cancellous bone to form subsidence. However, the cage used in ACDF has a relatively large effective contact surface, which disperses the stress of adjacent vertebrae and is more advantageous in the maintenance of intervertebral height. The subsidence rate was low in ACDF in our study, but there was still a decrease in the height of the intervertebral space at the last follow-up. We speculated that intraoperative distraction of the intervertebral space and then postoperative gravity on the cervical spine contributed to this condition. In addition, the thickness of the removed endplate also had a significant effect on the subsidence of the cage after fusion surgery. 19 We suggest preserving the bony endplate as much as possible to prevent cage subsidence when scraping the endplate cartilage.
Biomechanically, we believe that multiple points of distraction during ACDF can more effectively correct the cervical curvature. Clinical studies have directly linked postoperative cervical kyphosis to greater neurological deficits. 20 Yukawa et al. 21 found that the average C2-7 Cobb angle was 13.9 ± 12.3° in 1200 asymptomatic patients in Japan. In our study, the C2-7 Cobb angle, and the segmental angle in ACDF significantly showed greater improvement than that in ACCF at each follow-up. However, they were both within normal limit. In radiographic measurements, C2-7 Cobb angle and segment angle were significantly improved at the last follow-up, but the clinical outcomes of the patient in both groups were not statistically significant. Hirai et al. 22 detected that the maintenance of lordosis after ACDF may be better than that after ACCF from a long-term perspective. Thus, we needed longer-time follow-up to explore the differences in clinical efficacy. Other main radiologic factors associated with it were T1 slope and C2–C7 SVA. Zhang et al. 23 suggested that the sagittal balance of ACDF was better than that of ACCF, which was correlated with fewer axial symptoms. Some scholars took the value of T1-CL as the standard to judge cervical deformity. A T1-CL mismatch >20° corresponded to a C2-7 SVA >40 mm, which is considered the threshold of cervical deformity. 24 From our study, we found that the T1 slope had a greater improvement in the ACDF group than in the ACCF group. Thus, two approaches corrected the balance by ameliorating the T1 slope. The values of T1-CL in our study were always at a balance value. This may tell us that the localized OPLL has little effect on cervical deformity and that both procedures prevent cervical misalignment and worsening clinical outcomes. We found that no significant difference was observed in C2–C7 SVA in our research, and the values were at a normal level. This finding indicated that two surgical procedures caused little damage to the neck muscle, could prevent the cervical gravity center from moving forward, better maintained cervical sagittal balance and enhanced the postoperative quality of life of patients.
The patients had similar chief complaint symptoms before surgery. Both clinical outcomes showed no significant difference, which was similar to previous studies. 15 Moreover, postoperative clinical outcomes improved significantly in both groups. This finding indicated that patients improved after surgery, and their condition gradually improved at each follow-up. Since the neurologic symptoms were derived from the ossified posterior longitudinal ligament, the symptoms of all patients improved after the removal of osteophytes. Regardless of CSR with or without CSM, all patients experienced greatly postoperative relief of symptoms and showed significant improvement at the last follow-up. Thus, the effect of the anterior approach is acceptable. Statistics show that reports of improvement in neurological function is approximately between 60% and 70%. 25 The JOA recovery rate in our study improved greatly. Clinical outcomes according to Odom criteria were also showed no significant difference. During the follow-up, almost all patients were satisfied with the curative effect. They obviously felt that the neck pain disappeared, and the upper limb numbness was relieved. Wang et al. 26 reported that either ACCF or ACDF had a highly successful improvement of clinical outcomes and that they are good solutions.
The success of cervical surgery often depends directly on the progress of fusion. 27 From a biomechanical point of view, additional external or internal support should be employed to prevent excessive movement of cervical cages. 28 Qiu et al. 28 reported that corpectomy and discectomy with plate fixation and autograft fusion had similar fusion rates. Several scholars have shown that ACCF has relatively good fusion rates. 29 Pseudarthrosis may occur in multi-segmented ACDF if fusion surfaces are increased. 30 However, in our study, the 6-month fusion rates of patients who underwent ACDF and those who underwent ACCF were 66.2% and 40.5%, respectively. This is statistically significant. This result indicated that ACDF might promote earlier solid fusion in the 6 months. At 1 year, the difference disappeared. In the final follow-up, patients achieved successful solid fusion in each group.
In anterior cervical spine surgery, chronic dysphagia is one of the most common postoperative complications, but the mechanism remains unknown. Esophageal injury, anterior cervical soft tissue edema and postoperative hematoma might contribute to dysphagia. 31 Sixteen (20.8%) patients complained of mild dysphagia postoperatively in the ACDF group and thirty (45.9%) in the ACCF group after surgery. Some of them might be due to recurrent laryngeal nerve injury, and they recovered after we used methylprednisolone. At 1 month postoperatively, we still found a lower incidence of dysphagia in patients who underwent ACDF (10.4%) than in those who underwent ACCF (24.3%). We thought that the plate used in ACCF made the difference and that the presence of a plate caused anterior cervical soft tissue edema. In ACDF, We implanted a special cage into the intervertebral space and insert two anchoring clips to fix the cage into the adjacent vertebra. 32 This method could prevent the implant from contacting the anterior cervical soft tissue. Through our follow-up of patients, only one patient in the ACDF group and five patients in the ACDF group had no apparent relief finally. Thus, we conclude that ACDF is great at ensuring milder anterior soft tissue injury, which results in a lower incidence of dysphagia. Another long-term postoperative complication is ASD, because cervical spine fusion surgery immobilizes the motion segment at the expense of its range of motion. Fewer remaining segments are considered to provide more motion, which accelerates disc degeneration, chronic osteophyte formation and new adjacent segment disease. 32 Another factor is that the edge of the plate approaches the disc. 33 However, the results showed in our current study that no case of ASD was observed in the ACDF group, and the incidence was 4.1% in the ACCF group. Fortunately, the two patients showed only changes in imaging data and no definite clinical symptoms or mild symptoms, so no repeated operations were needed. The low incidence of ASD in this study may be due to the short observation period. Nevertheless, we speculate that the incidence of ASD will increase in those who undergo ACCF in the future because of the inevitable misposition of the plate.
Cerebrospinal fluid leak (CSFL) after cervical spine surgery can be troublesome, as it can cause meningitis, spinocutaneous fistula, or pseudomeningocele. Lee et al. 34 reports that dural tears are relatively common, as they occur in approximately 10.5% of ACCF procedures. The crucial point of our operation is that the herniated disc is completely removed first. Then, we can incise the normal posterior longitudinal ligament so that we can, in turn, expose the dura and remove the OPLL with a rongeur. When a rongeur was used to resect the localized OPLL, it was much more likely to break the dura if the OPLL adhered to the dura. In our study, CSFL occurred in six patients in the ACDF group and in 10 patients in the ACCF group. Although the incidence was not statistically significant, we considered that resection of more structures during ACCF is more likely to cause dural tears. Various techniques have been used to manage dural tears and the consequent CSFL after surgery. Gelatin sponges were successfully used to repair dural tears intraoperatively. These patients completely recovered after 3–5 days of bed rest and management with ceftriaxone, and their wounds healed normally. There was one patient in the ACCF group in which lumbar cistern drainage postoperatively was employed to solve the problem because the size of the dural defect was large. No patient developed further spinal or intracranial infection, cutaneous fistula or required secondary surgery.
This study has some limitations. First, larger sample and longer follow-up time are necessary. Second, a randomized controlled trial study should be carried out to avoid selection bias. The current findings cannot be interpreted as long-term results. Therefore, we require further observation to investigate the issue in prospective randomized trials.
Conclusion
Both ACDF and ACCF achieved satisfactory primary clinical efficacies and fusion rates for patients with localized OPLL. However, ACDF was associated with a shorter surgical procedure, less blood loss, better radiologic outcomes, and lower incidence of dysphagia than ACCF. In most cases, when both surgical approaches are an option, ACDF is a worthwhile alternative to ACCF as a surgical treatment for localized OPLL. When the osteophyte extends to the posterior edge of the vertebral body that cannot be removed or occupies more than 2/3 of the intervertebral space laterally so that rongeur has no space to bite, ACCF is better.
Footnotes
Author contributions
Conception and design: Tangyiheng Chen, Yijie Liu.
Administrative support: Weimin Jiang, Yijie Liu.
Provision of study materials or patients: Weimin Jiang, Xuefeng Li.
Collection and assembly of data: Tangyiheng Chen, Yujie Wang, Hong Zhou, Cheng Lin.
Data analysis and interpretation: Tangyiheng Chen.
Manuscript writing: All authors.
Final approval of manuscript: All authors
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is supported by the Youth Fund for Medical and Health Basic Research of Suzhou (SYS2020096).
Ethical approval
All procedures performed in study were approved by the Institutional Ethics Committee of Soochow University.
Informed consent
All experiments were performed in accordance with relevant named guidelines and regulations. Informed consent was obtained from all individual participants included in the study.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.