
Abstract
Study Design
A meta-analysis.
Objective
Anterior cervical discectomy and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF) are widely used in the treatment of cervical spondylotic myelopathy (CSM). However, the clinical outcomes and complications between ACDF and ACCF treating multi-level CSM remain poorly understood. Thus, we performed a meta-analysis to compare the clinical outcomes and complications of the two procedures in the treatment of 3-level and 4-level CSM.
Methods
An extensive search of the literature was performed in the English databases of PubMed, Embase, and Cochrane Library and the Chinese databases of CNKI and WANFANG. We collected factors, including demographic data, surgical factors, and complications. Data analysis was conducted with RevMan 5.3 and STATA 12.0.
Results
Finally, 14 articles (5429 patients) were included in our study. No significant difference was found in preoperative and 3-month follow-up Japanese Orthopedic Association (JOA) scores, neck disability index, preoperative C2-C7, segmental angle, operation time, as well as the number of dysphagia, hoarseness, cerebral fluid leakage, infection, epidural hematoma, axial pain, hardware breakage, and pseudarthrosis between ACDF and ACCF. However, our findings showed that blood loss (P < 0.00001), the number of total complications (P < 0 .00001), C5 palsy (P = 0.0004), graft dislodgement (P = 0.02), graft subsidence (P = 0.0003), and revision surgery (P = 0.0008) in ACDF were significantly less than in ACCF. Additionally, postoperative and change of C2-C7 (P < 0.00001), segment angle (P < 0.00001), and fusion rate (P = 0.001) in ACDF were significantly higher than in ACCF. Post-operative JOA in ACDF was significantly higher than in ACCF (P = 0.02).
Conclusions
Although the clinical efficacy of both surgeries was similar, ACDF was superior to ACCF in the reconstruction of cervical lordosis and the number of complications in the treatment of 3-level and 4-level CSM.
Keywords
Introduction
Cervical spondylotic myelopathy (CSM) is a common cervical disease, ranging from 10% to 15% of cervical spondylosis.1-3 CSM, especially multilevel CSM, is the major cause of spinal cord injury and neurological dysfunction, posing a great social and economic burden on individuals due to long-life disability.4-6 Regarding patients with worsening clinical symptoms and indicators, surgical therapy is preferable to conservative treatment.7-10 Anterior surgical interventions such as anterior cervical discectomy and fusion (ACDF)11,12 and anterior cervical corpectomy and fusion (ACCF)13,14 have been routinely used in patients with 3-level and 4-level CSM. ACDF can decompress the anterior spinal cord and maintain spinal column stability, yet it may increase a significant risk of inadequate decompression, restricted visual exposure, or cord damage.15,16 ACCF may provide a more widespread decompression, but it is more difficult to implement and has a higher risk of complications.17,18
Which anterior surgery, ACDF or ACCF, is the better option for 3-level and 4-level CSM, remains controversial. Shamji 19 performed a meta-analysis and demonstrated that ACDF was the better option for multilevel CSM. Wang 20 found that both were good plans for clinical outcomes, but ACDF was better than ACCF in radiographic outcomes and the number of total complications. However, two other authors21,22 came to the opposite conclusion that ACDF and ACCF had similar outcomes in the treatment of multilevel CSM. To our knowledge, previous meta-analyses19-23 had some limitations, such as small samples, mainly studied 2-level or 3-level CSM, few variables, high heterogeneity or included studies from the last two or three decades, which may influence the accuracy of results. Thus, we collected data from the last decade and performed a meta-analysis to compare two anterior procedures in clinical outcomes, radiographic outcomes, surgical outcomes, and the number of complications they caused in treating 3-level and 4-level CSM.
Methods
Search Strategy
The terms “anterior cervical discectomy and fusion,” “anterior cervical corpectomy and fusion,” and “3-level and 4-level cervical spondylotic myelopathy” were used to search for English and Chinese language papers in PubMed, Embase, and the Cochrane Library as well as CNKI and WAN FANG. All research that has already been published as of May 2022 was included in the publication date range.
Eligibility Criteria
The following criteria must be fulfilled by included articles: Adult patients, research comparing ACDF with ACCF, 3 or 4 levels of cervical spondylotic myelopathy, and publications from the past 10 years are all prerequisites. Studies were excluded if they met the following criteria: (1) they were abstracts, letters, reviews, or case reports; (2) they contained repeated data; (3) they failed to report outcomes of interest; (4) patients were treated for tumors, infections, spinal cord injuries, or inflammation; (5) they had a history of cervical surgery; (6) they were younger than 18; (7) they underwent posterior surgery; and (8) they had ossification of the posterior longitudinal ligament.
Data Extraction and Outcome Measures
Each study’s general features and the results that were measured were included in the data. The first author, the publishing year, the nation, the number of patients, and the type of article are examples of general features. We only kept the most comprehensive article or study where the same population was mentioned in multiple publications to prevent material from being repeated. Two writers independently extracted the data. Any discrepancies about paper eligibility were settled by discussion and agreement. Check for publication bias risk. The funnel diagram was visually examined for publication bias. If there is a publishing bias, the funnel plot should be asymmetric; if there is no publication bias, it should be symmetric. Egger and Begg tests were conducted to measure the funnel plot asymmetry according to a significance level of P < .10. We used the trim and fill computation to assess the effect of publication bias. We do not calculate sensitive analysis due to the low heterogeneity of every factor.
Statistical Analysis
Odd ratios (OR) and 95% confidence intervals (CI) were calculated for outcomes because our study only referenced continuous outcomes. Statistical significance was defined as a P value < .05. Depending on the degree of heterogeneity among the included studies, either fixed-effects or random-effects models were employed. Heterogeneity was analyzed with both the Chi-squared test I square test, where a P value of < .10 for the Chi-squared and I2 > 50% implied heterogeneity. Review Manager version 5.3 (The Cochrane Collaboration, Oxford, UK) and STATA 12.0 (Stata Corporation, College Station, TX, USA) were used for all statistical analyses.
Results
Study Identification and Selection
Primordially, we collected 91 English articles and 34 Chinese papers from the database search. Due to repetition, 42 English articles and 19 Chinese articles were excluded, and 31 English articles and 12 Chinese articles were removed after reviewing the titles and abstracts. The remaining 18 English articles and 3 Chinese studies were retrieved for inclusion criteria, and 5 English articles and 2 Chinese articles were excluded. Finally, 13 English articles and 1 Chinese article that met our inclusion criteria were included in the present meta-analysis. The selection process that was included in this meta-analysis is shown in Figure 1. Flow diagram of studyselection.
Baseline Characteristics and Quality Assessment
Characteristics of Included Studies.

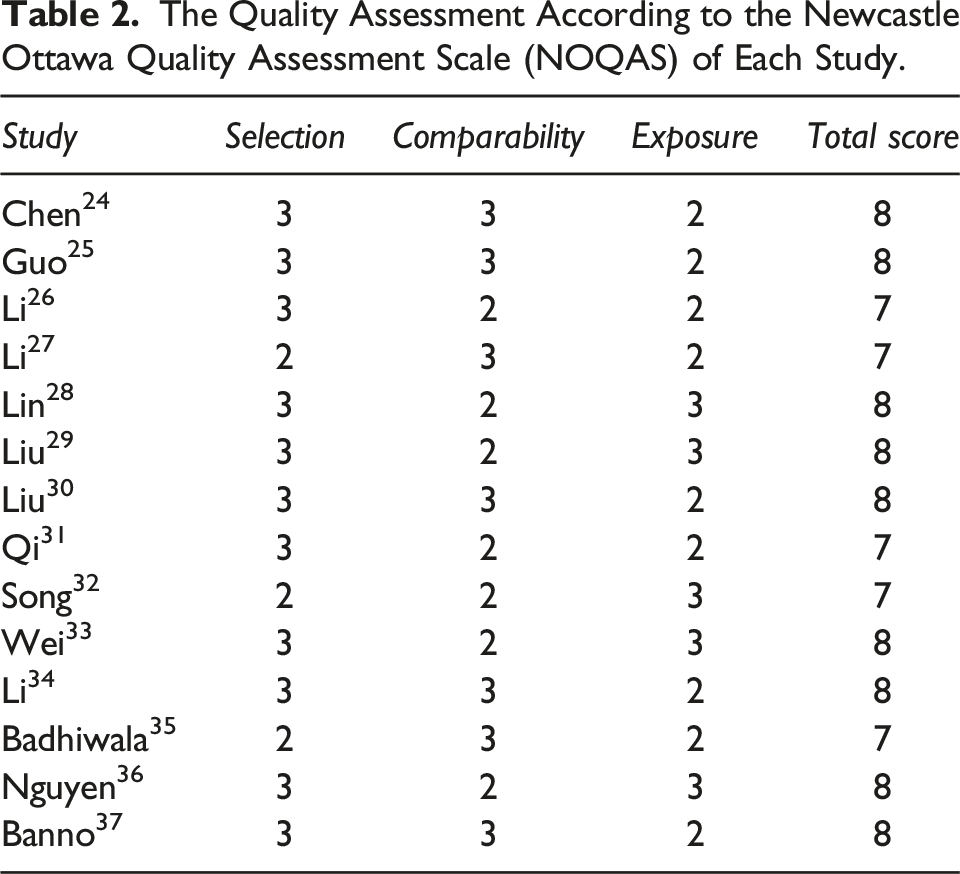
The Quality Assessment According to the Newcastle Ottawa Quality Assessment Scale (NOQAS) of Each Study.
Clinical Outcomes
Japanese Orthopedic Association scores
Ten studies24-33 reported preoperative, postoperative and 3-month follow-upJapanese Orthopedic Association (JOA) scores for ACDF and ACCF. The tests for heterogeneity were not significant and the studies had low heterogeneity (p for heterogeneity = 0.79, I2 = 0%; p for heterogeneity = 0.81, I2 = 0%; p for heterogeneity = 0.31, I2 = 2% respectively, Figure 2A-C). No significant difference was found between ACDF and ACCF in preoperative and 3-month follow-up JOA scores (fixed-effects model, P = 0.50, OR = 0.07, 95% CI [−0.13,0.26]; fixed-effects model, P = 0.84, OR = −0.09, 95% CI [−0.97,0.79], respectively, Figure 2A and C). Post-operative JOA in ACDF was significantly higher than in ACCF (fixed-effects model, P = 0.02, OR = 0.49, 95% CI [0.06,0.91], Figure 2B). Forest plot showing Japanese Orthopedic Association (JOA) in two groups. A. preoperative JOA; B. postoperative JOA; C. 3-month JOA. CI = confifidence interval; df = degrees of freedom, M-H = Mantel–Haenszel, JOA = Japanese Orthopedic Association scores.
Neck Disability Index
Seven studies24-30 reported preoperative and postoperative neck disability index (NDI) for ACDF and ACCF. The tests for heterogeneity were not significant and the studies had low heterogeneity (p for heterogeneity = 0.88, I2 = 0%; p for heterogeneity = 0.38, I2 = 3%, respectively, Figure 3A and B). No significant difference was found between ACDF and ACCF in preoperative and postoperative NDI (fixed-effects model; P = 0.20, OR = 0.34, 95% CI [−0.18, 0.87]; fixed-effects model; P = 0.46, OR = 0.29, 95% CI [−0.47, 1.05], respectively, Figure 3A and b). Forest plot showing neck disability index (NDI) in two groups. A. preoperative NDI; B. postoperative NDI. CI = confifidence interval, df = degrees of freedom, M-H = Mantel–Haenszel, NDI= neck disability index.
Sagittal Alignment
C2-C7 angle
Seven studies24-27,29,33,34 reported preoperative, postoperative, and change in C2-C7 angle for ACDF and ACCF. The tests for heterogeneity were not significant and the studies had low heterogeneity (p for heterogeneity = 0.90, I2 = 0%; p for heterogeneity = 0.30, I2 = 19%; p for heterogeneity = 0.59, I2 = 0%, respectively, Figure 4A-C). No significant difference was found between ACDF and ACCF in preoperative C2-C7 angle (fixed-effects model; P = 0.34, OR = 0.39, 95% CI [−.41, 1.19] Figure 4A). However, the postoperative and change of C2-C7 angle in ACDF were significantly higher than in ACCF (fixed-effects model; P < 0.00001, OR = 5.44, 95% CI [4.25, 6.64]; fixed-effects model; P < 0.00001, OR = 11.65, 95% CI [9.53, 13.78], respectively, Figure 4B and C). Forest plot showing cobb angle of C2-C7 in two groups. A. preoperative cobb angle of C2-C7; B. postoperative cobb angle of C2-C7. C. change of cobb angle of C2-C7. CI = confifidence interval, df = degrees of freedom, M-H = Mantel–Haenszel.
Segmental Angle
Two studies28,30 reported preoperative and postoperative segmental angle for ACDF and ACCF. The tests for heterogeneity were not significant and the studies had low heterogeneity (p for heterogeneity = 0.48, I2 = 0%; p for heterogeneity = 0.82, I2 = 0%, respectively, Figure 5A and B). No significant difference was found between ACDF and ACCF in preoperative segmental angle (fixed-effects model; P = 0.84, OR = 0.12, 95% CI [−0.97, 1.20] Figure 5A). However, postoperative segmental angle in ACDF was significantly higher than in ACCF (fixed-effects model; p < 0.00001, OR=3.23, 95% CI [2.36, 4.09], Figure 5B). Forest plot showing segmental angle in two groups. A. preoperative segmental angle; B. postoperative segmental angle. CI = confifidence interval, df = degrees of freedom, M-H = Mantel–Haenszel.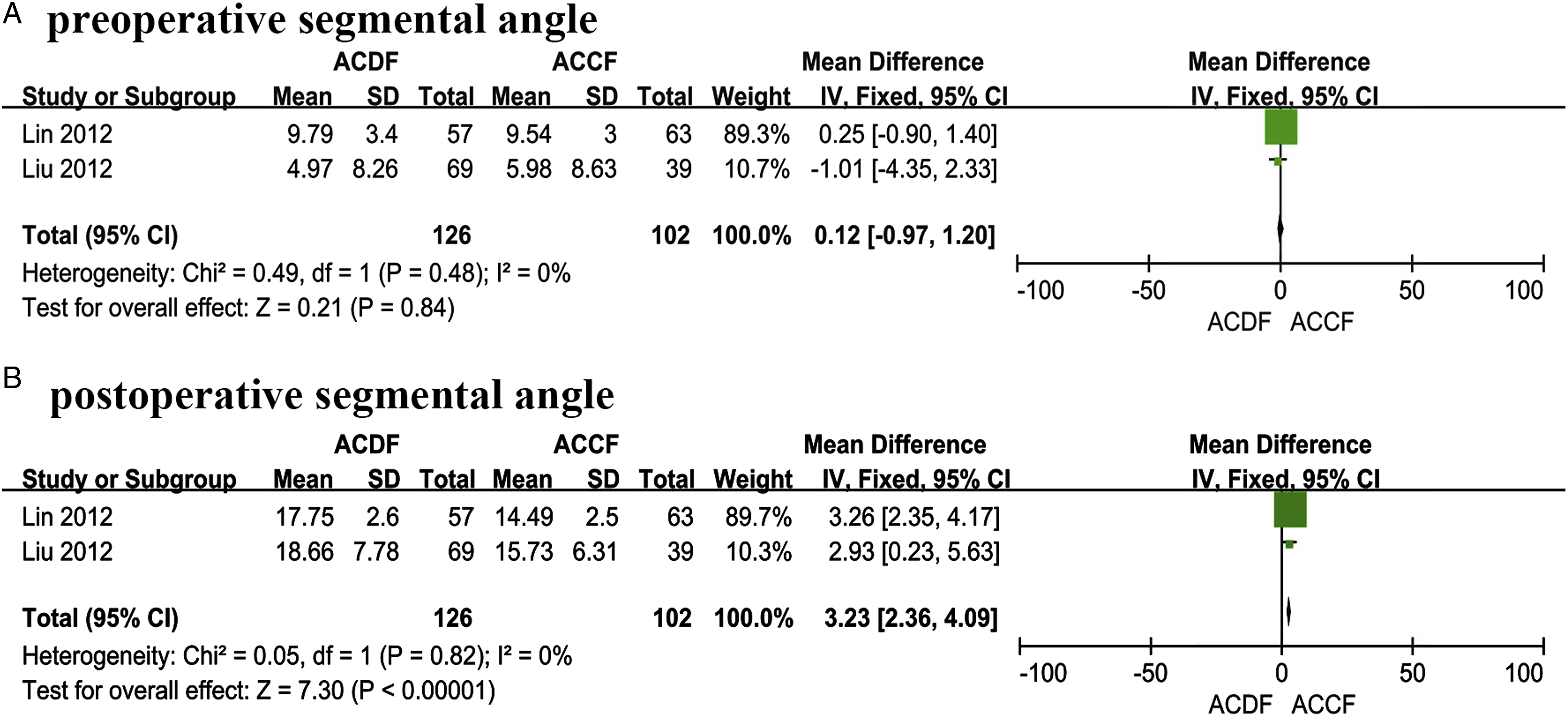
Surgical Factors
Operation time
Three studies26,27,35 reported operation time for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity=0.99, I2 = 0%, Figure 6). No significant difference was found between ACDF and ACCF in operation time (fixed-effects model; P = 0.26, OR = 4.45, 95% CI [−3.23, 12.13], Figure 6). Forest plot showing operation time in two groups. CI = confifidence interval, df = degrees of freedom, M-H = Mantel–Haenszel.
Blood Loss
Two studies24,32 reported blood loss for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.31, I2 = 2%, Figure 7). Blood loss in ACDF was significantly less than in ACCF (fixed-effects model; P < 0.00001, OR = −528.63, 95% CI [−586.86, −470.39], Figure 7). Forest plot showing blood loss in two groups. CI = confifidence interval, df = degrees of freedom, M-H = Mantel–Haenszel.
Complications
Total complications
Twelve studies25-36 reported the number of total complications for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.17, I2 = 28%, Figure 8). The number of total complications in ACDF were significantly less than in ACCF (fixed-effects model; p < 0.00001, OR=0.56, 95% CI [0.48,0.65], Figure 8). Forest plot showing the total number of complications in two groups. CI = confifidence interval, df = degrees of freedom, M-H = Mantel–Haenszel.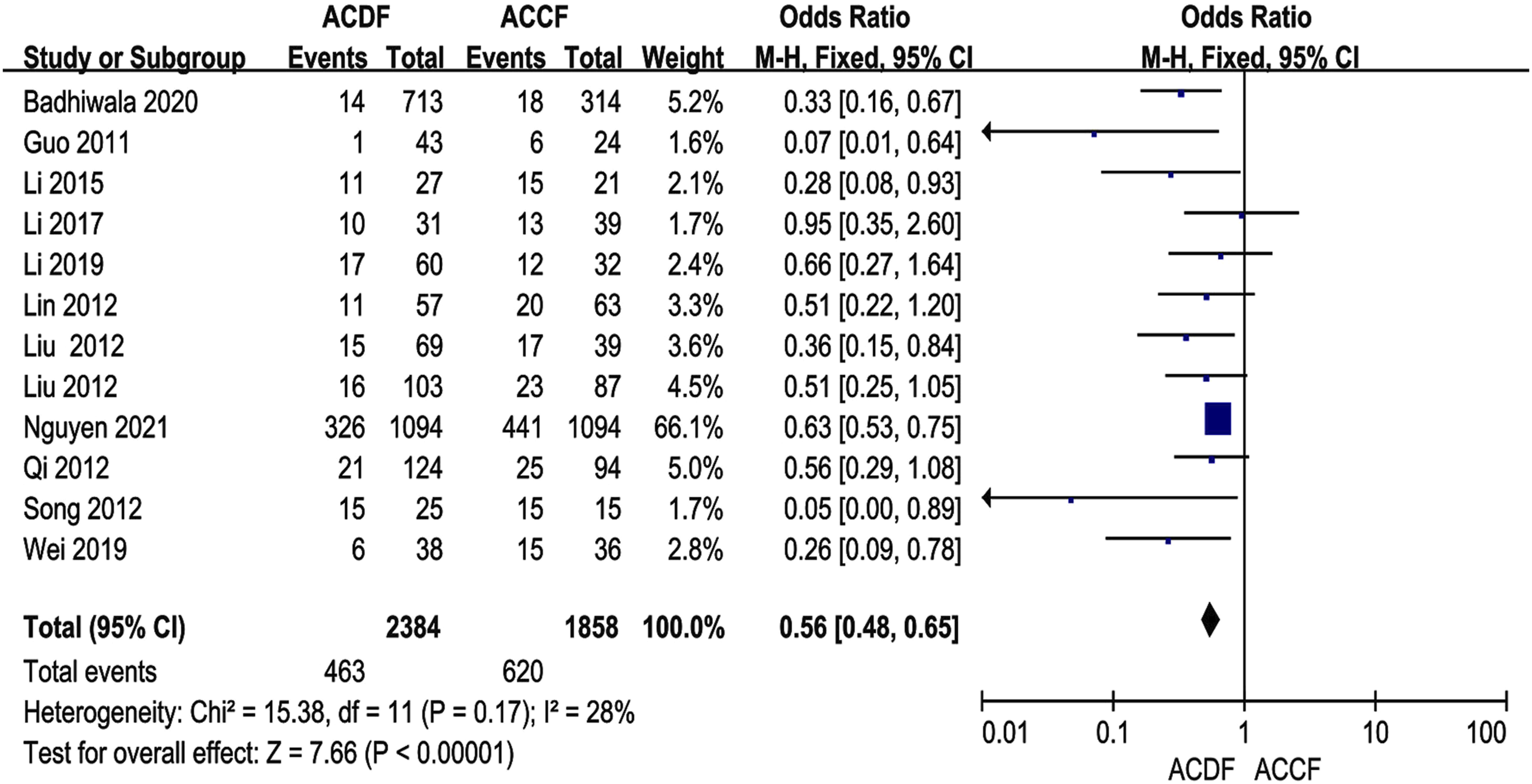
Dysphagia
Ten studies26-34,36 reported the number of dysphagia for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.77, I2 = 0%, Figure 9A). No significant difference was found between ACDF and ACCF in the number of dysphagia (fixed-effects model; P = 0.28, OR = 0.87, 95% CI [0.67, 1.12], Figure 9A). Forest plot showing the number of subgroups of complications in two groups. A. dysphagia; B. hoarseness; C. C5 palsy; D. cerebral fluid leakage; E. infection; F. fusion rate; G. hematoma; H. axial pain; I. hardware breakage; j. pseudoarthrosis; K. graft dislodgement; L. graft subsidence, m. revision surgery. CI = confifidence interval, df = degrees of freedom, M-H = Mantel–Haenszel.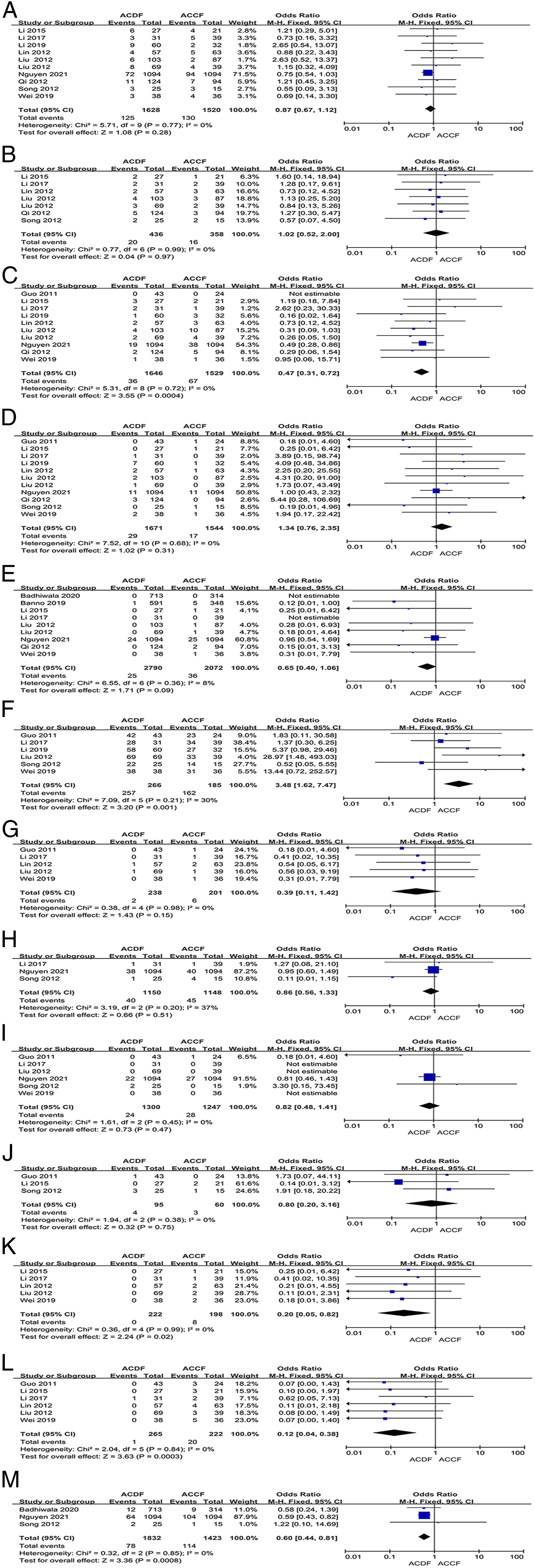
Hoarseness
Seven studies26-32 reported the number of hoarseness for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.99, I2 = 0%, Figure 9B). No significant difference was found between ACDF and ACCF in the number of hoarseness (fixed-effects model; P = 0.97, OR = 1.02, 95% CI [0.52, 2.00], Figure 9B).
C5 Palsy
Ten studies25-31,33,34,36 reported the number of C5 palsy for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.72, I2 = 0%, Figure 9C). The number of C5 palsy in ACDF were significantly less than in ACCF (fixed-effects model; P = 0.0004, OR = 0.47, 95% CI [0.31,0.72], Figure 9C).
Cerebral Fluid Leakage
Eleven studies25-34,36 reported the number of cerebral fluid leakage (CFL) for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.68, I2 = 0%, Figure 9D). No significant difference was found between ACDF and ACCF in the number of CFL (fixed-effects model; P = 0.31, OR = 1.34, 95% CI [0.76,2.35], Figure 9D).
Infection
Nine studies26,27,29-31,33,35-37 reported the number of infection for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.36, I2 = 8%, Figure 9E). No significant difference was found between ACDF and ACCF in the number of infection (fixed-effects model; P = .09, OR = 0.65, 95% CI [0.40, 1.06], Figure 9E).
Fusion Rate
Six studies25,27,30,32-34 reported the number of fusion rate for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.21, I2 = 30%, Figure 9F). Fusion rate in ACDF were significantly higher than in ACCF (fixed-effects model; P = 0.001, OR = 3.84, 95% CI [1.62,7.47], Figure 9F).
Epidural Hematoma
Five studies25,27,28,30,33 reported the number of epidural hematoma for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.98, I2=0%, Figure 9G). No significant difference was found between ACDF and ACCF in the number of epidural hematoma (fixed-effects model; P = 0.15, OR = 0.39, 95% CI [0.11, 1.42], Figure 9G).
Axial Pain
Three studies27,32,36 reported the number of axial pain for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.20, I2 = 37%, Figure 9H). No significant difference was found between ACDF and ACCF in the number of axial pain (fixed-effects model; P = 0.51, OR = 0.86, 95% CI [0.56, 1.33], Figure 9H).
Hardware Breakage
Six studies25,27,30,32,33,36 reported the number of hardware breakage for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.45, I2 = 0%, Figure 9I). No significant difference was found between ACDF and ACCF in the number of hardware breakage (fixed-effects model; P = 0.47, OR = 0.82, 95% CI [0.48, 1.41], Figure 9I).
Pseudarthrosis
Three studies25,26,32 reported the number of pseudarthrosis for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.38, I2 = 0%, Figure 9J). No significant difference was found between ACDF and ACCF in the number of pseudarthrosis (fixed-effects model; P = 0.75, OR = 0.80, 95% CI [0.20, 3.16], Figure 9J).
Graft Dislodgement
Five studies26-28,30,33 reported the number of graft dislodgement for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.99, I2 = 0%, Figure 9K). The number of graft dislodgement in ACDF were significantly less than in ACCF (fixed-effects model; P = 0.02, OR = 0.20, 95% CI [0.05,0.82], Figure 9K).
Graft Subsidence
Six studies25-28,30,33 reported the number of graft subsidence for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.84, I2 = 0%, Figure 9L). The number of graft subsidence in ACDF were significantly less than in ACCF (fixed-effects model; P = 0.0003, OR = 0.12, 95% CI [0.04,0.38], Figure 9L).
Revision Surgery
Three studies32,35,36 reported the number of revision surgery for ACDF and ACCF. The test for heterogeneity was not significant and the studies had low heterogeneity (p for heterogeneity = 0.85, I2 = 0%, Figure 9M). The number of revision surgery in ACDF were significantly less than in ACCF (fixed-effects model; P = 0.0008, OR = 0.60, 95% CI [0.44,0.81], Figure 9M).
Publication Bias
After detection of publication bias by STATA 12.0, there was no publication bias found for all included studies (all P > .05).
Discussion
Surgical therapies for CSM have been dated back to the 1950s, yet the optimal plans for CSM, especially multilevel CSM, remain inconsistent. 38 Historically, three main elements affect the choice between ACDF and ACCF, including the identity and location of the stenotic pathology, cervical sagittal alignment, and the number of pathological segments. 39 Certainly, complication rates have been found to depend on the selected surgical approach, both in all cervical procedures and specifications for more extensive diseases. 40 Lately, the anterior approaches are extensively utilized in the operative management of multilevel CSM because they directly decompress the spinal cord and nerve roots. 41 Meanwhile, complications related to anterior surgeries, such as graft-related complications, hoarseness, dysphagia, C5 palsy, and CFL, are troublesome.
Although increasing articles have compared the clinical efficacy and complications between ACDF and ACCF, the superior method is unclear. Furthermore, some meta-analysis19-23 focused on this topic, but they failed to reach a consensus, which may be associated with their drawbacks, such as small samples, 2-level or 3-level CSM, few variables, high heterogeneity, or old-age included studies. Therefore, we tried our best to collect as much data as possible and conducted this meta-analysis to compare clinical outcomes, radiographic outcomes, surgical outcomes, and the number of complications between ACDF and ACCF in treating 3-level and 4-level CSM. Finally, 5429 patients with 3-level or 4-level CSM were included in our study. Our findings showed that blood loss, and the number of total complications, C5 palsy, graft dislodgement, graft subsidence, and revision surgery in ACDF were significantly less than in ACCF. Moreover, postoperative C2-C7 and segment angle, change of C2-C7, and fusion rate in ACDF were significantly higher than in ACCF.
As we know, JOA and NDI are crucial scales to assess the improvement of nerve function. In the current study, preoperative and 3-month follow-up JOA were consistent with previous meta-analysis,19-22 while the postoperative JOA in ACDF was markedly higher than in ACCF, which indicated that ACDF may more adequately decompress compared with ACCF. However, pre-and post-operative NDI were similar in the two groups. The findings suggest that both operations not only adequately decompress the nerves but also enhance their prognosis. Regarding sagittal alignment, although two methods significantly increased the postoperative Cobb angle of C2-C7 and segmental angle, ACDF was better than ACCF because ACDF not only provided multiple points of distraction and fixation together with the graft and interbody space shaping but also pulled the involved vertebral bodies toward the lordotic ventral plate to restore alignment, while ACCF grafts may straighten the cervical spinal column between the remaining vertebral bodies. 28
Operation time and blood loss are important factors for assessing surgical trauma. Three meta-analyses20-22 suggested no obvious difference between the two groups, while Xiao 23 implied that ACDF spent less operation time than ACCF. However, large heterogeneity should be considered in these four research outcomes, which indicated the low quality of evidence for this outcome. Notably, our data with low heterogeneity (I2 = 0%) from the last decade demonstrated no significant discrepancy in operation time between the two techniques. Additionally, our findings showed that blood loss in ACCF was dramatically higher than in ACDF, implying ACCF with more surgical trauma, which was in line with prior meta-analysis.20-23 It is easy to understand that more blood loss is caused by vertebral resection during ACCF.
Similar to a recent meta-analysis, we also found that the total number of complications in ACCF was significantly higher than in ACCF. What’s more, there was a higher rate of revision surgery after ACCF compared with ACDF, indicating a lower rate of complications. However, the subgroup of complications was different from prior studies.19-23 C5 palsy is a crucial complication following cervical surgery, varying from 0% to 30%, caused by the drift of the spinal cord after multilevel surgery. 42 Han 21 discovered no statistical difference in C5 palsy in the two groups, while both Shamji 19 and Wang 20 proved that C5 palsy was markedly less in ACDF than in ACCF, which was the same as our findings.
Regarding the fusion rate, three studies21-23 supported no remarkable discrepancy between the two groups. Whereas, Shamji 19 found that ACDF had a lower rate of fusion rate in comparison with ACCF. Because some authors43,44 claimed that ACCF not only resolved retrovertebral compressive pathology but also reduced the graft-host interface. Interestingly, Wang 20 suggested that ACDF had a higher fusion rate than ACCF, which was similar to our results. Considering the high heterogeneity in the four meta-analyses,19,21-23 we believed our results would have more accuracy. Regarding graft-related complications, Han 21 and Xiao 23 just identified a higher rate of graft-related complications in ACCF, while Han did not perform a subgroup analysis. Wang 20 mentioned no difference in graft dislodgment but found that ACCF had a higher rate of graft subsidence. In the present study, compared with ACCF, ACDF produced more satisfactory results in the incidence of graft dislodgment and graft subsidence. The reason may account for the results because ACDF was able to provide a more stable biomechanics environment for bone healing, 45 which increases the fusion rate46,47 and lower the incidence of graft dislodgment and graft subsidence.
There were several limitations to this study. First, there was no randomized controlled trial article focused on this topic; we need RCT to perform the further study. Second, the statistical power could be improved in the future by including more studies. Due to the limited studies, some parameters like cervical lordosis and subgroup analysis could not be analyzed. But we tried our best to collect as much data as possible, and a total of 5429 patients, which was far more than the previous meta-analysis, were included in this meta-analysis. Third, the search strategy was restricted to articles published in English and Chinese languages. Articles with potentially high-quality data that were published in other languages were not included because of anticipated difficulties in obtaining accurate medical translations. Fourth, although ten of fourteen included articles were from China, this meta-analysis has high quality and no publication bias.
In summary, two anterior surgeries could achieve clinical efficacy in the treatment of 3-level and 4-level CSM. In addition, ACDF offers more radiographic outcomes. Furthermore, ACDF had more satisfactory results in terms of the rate of complications. We hope our findings could guide the surgeon in selecting among procedures when faced with patients with 3-level and 4-level CSM.
Footnotes
Authors’ Contributions
TW and JFG were responsible for study concept and writing the article. JFG and YBL were responsible for screened the abstracts and reviewed the article. ZYH was responsible for reviewing and writing the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Science and technology project and Intellectual Property Bureau of Baoding City (2041ZF260).
Ethics Approval
The study was approved by the Institutional Review Board of the third hospital of Hebei Medical University before data collection and analysis.there is no need to write informed consent forms from patients because this is a meta-analysis study.