
Abstract
Study design
Retrospective, cohort study
Objectives
Hand function can be difficult to objectively assess perioperatively. In patients undergoing cervical spine surgery by a single-surgeon, we sought to: (1) use a hand dynamometer to report pre/postoperative grip strength, (2) distinguish grip strength changes in patients with radiculopathy-only vs myelopathy, and (3) assess predictors of grip strength improvement.
Methods
Demographic and operative data were collected for patients who underwent surgery 2015-2018. Hand dynamometer readings were pre/postoperatively at three follow-up time periods (0-3 m, 3-6 m, 6-12 m).
Results
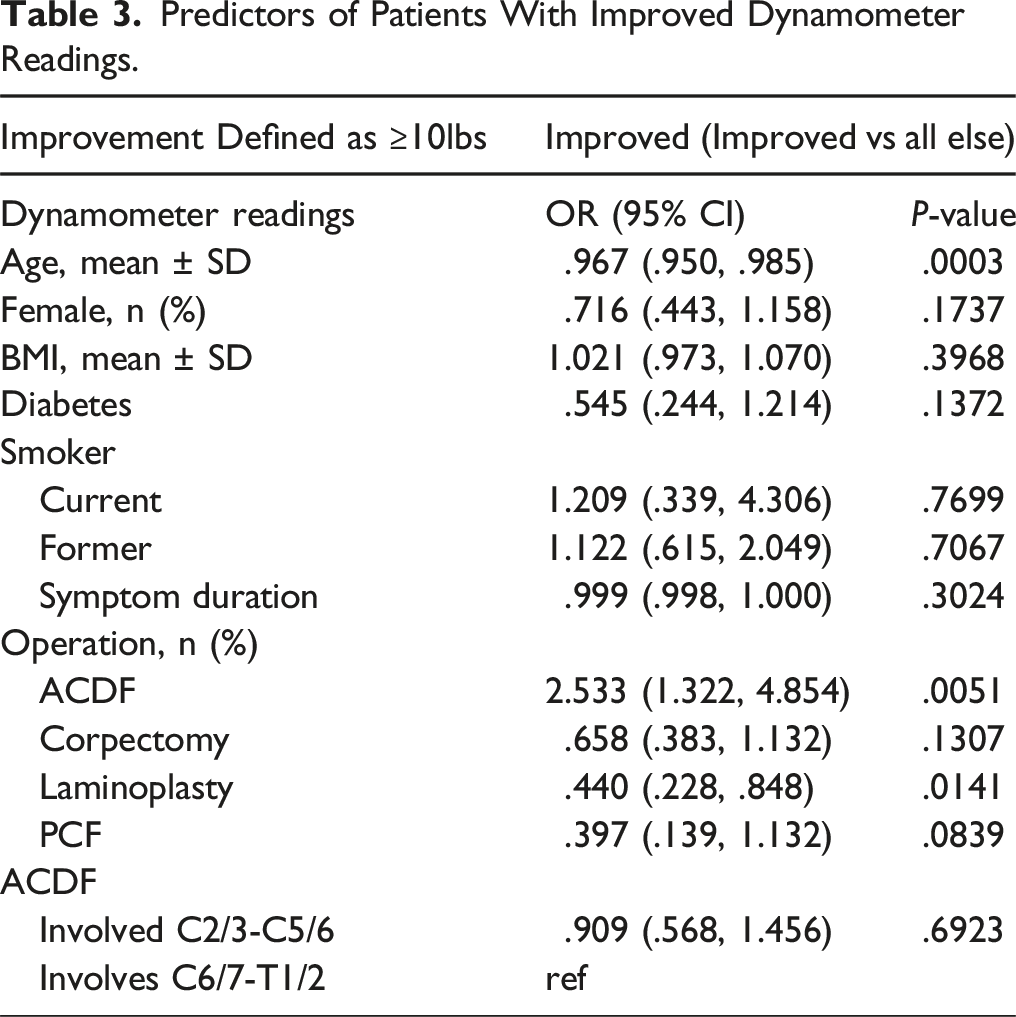
262 patients (mean age of 59 ± 14 years; 37% female) underwent the following operations: ACDF (80%), corpectomy (25%), laminoplasty (19%), and posterior cervical fusion (7%), with 81 (31%) patients undergoing multiple operations in a single anesthetic setting. Radiculopathy-only was seen in 128 (49%) patients, and myelopathy was seen 134 (51%) patients. 110 (42%) had improved grip strength by ≥10-lbs, including 69/128 (54%) in the radiculopathy-only group, and 41/134 (31%) in the myelopathy group. Those most likely to improve grip strength were patients undergoing ACDF (OR 2.53, P = .005). Patients less likely to improve grip strength were older (OR = .97, P = .003) and underwent laminoplasty (OR = .44, 95% CI .23, .85, P = .014). Patients undergoing surgery at the C2/3-C5/6 levels and C6/7-T1/2 levels both experienced improvement during the 0-3-month time range (C2-5: P = .035, C6-T2: P = .015), but only lower cervical patients experienced improvement in the 3-6-month interval (P = .030).
Conclusions
Grip strength significantly improved in 42% of patients. Patients with radiculopathy were more likely to improve than those with myelopathy. Patients undergoing surgery from the C2/3-C5/6 levels and the C6/7-T1/2 levels both significantly improved grip strength at 3-month postoperatively.
Keywords
Introduction
Compression of the cervical spinal cord and/or nerve roots often leads decreased grip strength. Myelopathic patients report hand clumsiness, poor fine motor coordination, and dropping things. 1 Patients with lower cervical and upper thoracic radiculopathies also present with hand motor deficits. Hand weakness can lead to severe disability and compromise one’s ability to live independently. 2 The unique functionality of the human hand is crucial to nearly all aspects of life and evolutionarily separates humans from other species.
Despite the frequency of hand weakness in patients with cervical spine pathology, grip strength can be difficult to localize and quantify. The hand is innervated by five nerve roots, C5 to T1, in addition to three peripheral nerves: median, radial, and ulnar nerve. Isolating specific radicular problems requires a detailed knowledge of the relevant motor/sensory anatomy and hand/finger motor examination techniques. 3 A pre- or post-fixed brachial plexus may also confound hand examination. Moreover, subjective exams between surgeons can obfuscate motor and sensory deficits.
A hand dynamometer is an objective, reproducible method for obtaining grip strength in the clinical setting since the 1970s.4,5 Readings provide maximum measure of grip strength through force, most commonly in pounds (lbs.). Readings vary greatly between sex and age anywhere from approximately 40 to 140 lbs. Large scale studies have revealed associations between hand grip strength and various measures of health including nutritional status, physical function, vertebral fracture risk, and overall mortality.6,7 Comparing baseline preoperative to postoperative dynamometer readings can provide an objective measure of strength improvement for patients and surgeons. Grip strength and hand dexterity, a function of sensory and motor abilities, are both important for quality of life and daily activity independence.
Given the complexity of assessing grip strength for cervical spine surgeons, we aimed to study this topic in a quantifiable, reproducible way. In a cohort of patients undergoing cervical spine surgery by a single-surgeon, we sought to: (1) use a hand dynamometer to report preoperative and postoperative grip strength, (2) distinguish grip strength changes in patients with radiculopathy-only vs myelopathy, and (3) assess predictors for postoperative grip strength improvement.
Methods
Study Design
A retrospective, single-institution, cohort study was performed of prospectively collected data. The study period was 4 years from 2015 to 2018. Institutional review board approval was obtained (IRB# AAAR0656) prior to study initiation. Informed consent was obtained prior to surgery. A waiver of informed consent for retrospective study participation was granted by the IRB. Of note, some patients in the study have been part of other published clinical research projects, yet their grip strength information has never been published before.
Patient Population
All patients undergoing elective, degenerative cervical spine surgery were included. Inclusion criteria were: age ≥18-year-old, minimum follow-up of at least 1-year, anterior and/or posterior cervical spine operation performed by the senior author (BLINDED), and preoperative and postoperative dynamometer readings recorded in the electronic medical record (EMR). Non-degenerative etiologies were excluded, including trauma, infection, and tumor.
Data Collection
All pertinent data was collected through a retrospective EMR review in addition to clinic visits. Demographic, comorbidities, presenting signs/symptoms, and operative data were collected as part of our institutional cervical spine registry. Most relevant to this study, the diagnosis of myelopathy was recorded by the treating surgeon based on symptomatology (impaired balance, spasticity, loss of fine motor coordination), clinical examination (motor weakness, hyperreflexia, balance deficits), and magnetic resonance imaging (MRI) scan findings (spinal cord compression). The cohort was dichotomized into those with myelopathy (myelopathy and/or myeloradiculopathy) compared to those without myelopathy (radiculopathy only). In addition, the patient-reported outcome (PRO) of Neck Disability Index (NDI) was obtained preoperatively and postoperatively prospectively by a research coordinator each clinic visit (MV). Importantly, operations were divided into anterior and posterior approach. If a patient had a combined anterior fusion and posterior fusion, these were counted as two separate operations. Despite the potential drawbacks of dividing anterior-posterior surgery into two operations, it was decided a-priori that it more accurately portrayed the specific type and breadth of surgery being performed to separate anterior-posterior operations into two. Groups were also divided into upper cervical (C2/3-C5/6) and lower cervical (C6/7-T1/2) in order to dichotomize nerve roots primarily involved in grip strength (lower roots C7/C8/T1) vs those roots classically not involved with hand function (C3/C4/C5/C6). With respect to cases involving multiple levels, the lowest level was used for grouping. For example, if the patient underwent a C5-7 ACDF, they were grouped in the lower cervical group.
Grip Strength Assessment
Hand dynamometer data was obtained on all patients preoperatively and postoperatively at three follow-up time periods (0-3 m, 3-6 m, 6-12 m). A commercially available grip strength dynamometer (Constant 200 lbs.) was used to quantify grip strength (Figure 1). For each visit, the average of three dynamometer readings from each hand, obtained by a medical assistant, was calculated. Readings were obtained by the same medical assistant, though there were intermittent staffing changes to clinic based on departmental needs. The same script was used for each patient: “Please squeeze as hard as you can three times with each hand.” All readings were obtained by the assistant prior to the surgeon history and examination to reduce any bias that may be introduced by the surgeon finding weakness or a lack thereof on examination, in either the preoperative or postoperative setting. Anecdotally, some patients were not aware of objective grip weakness, and conversely, some patients believed they had weakness that was not observed on dynamometer testing. Hand dynamometer.
The change in dynamometer reading was considered functionally significant if it was greater than or equal to 10 lbs. The 10 lbs. threshold was chosen based on the following approach. Our preferred option was to select a threshold from prior studies; however, no prior study on cervical spine surgery and dynamometer use with such a threshold existed. In the absence of prior knowledge, we selected 10 lbs. based on two reasons. First, the senior author chose this number based on over 20 years of anecdotal experience that patients considered a clinically meaningful improvement to be approximately 10 lbs. Second, the 10 lbs. threshold was also chosen based on our data, which gave us an appropriate split of the sample for us to further study. In selecting one of the three potential round number thresholds – 5, 10, 15 lbs. – 10 lbs. provided the most even split of patients.
Routine follow up was scheduled for 6 weeks, 6 months, and 1-year. Patients were grouped according to their actual time of follow-up, which led to different numbers of patient seen at each postoperative time point, such that not all patients were seen at each of the 3-time intervals. Follow-up times were grouped into: 0-3 months, 3-6 months, and 6-12 months.
Operative Technique
The senior author’s operative technique for anterior cervical operations has been previously reported. 8 However, herein we included a key aspect of technique related to motor deficit improvement that involves the anterior uncinatectomy. After the central decompression is performed, a posterior foraminal decompression is achieved with a matchstick burr, until all cranial and caudal bony stenosis is removed and only soft tissue remains. A 2-0 curette is then used to dissect and curve around the lateral aspect of the anterior uncinate to clear off any soft tissue, while protecting the vertebral artery. This is done in a counterclockwise fashion on the right, and a clockwise fashion on the left, to stay close to the bony uncus and clear off any soft tissue. A Penfield 2 or 4 is then used to replace the curette, which marks the lateral boundary of the uncinate. The burr is then taken in an anterior to posterior fashion, and the caudal aspect of the uncinate is notched until a thin wafer of bone is left that can be easily broken free with the curette using minimal force. The pedicle of the caudal level is then palpated to ensure the uncinate is removed and root is free.
Statistical Analysis
Descriptive statistics were performed to summarize patient demographics, comorbidities, presenting signs/symptoms, and operative data. Categorical data was presented as frequencies and percentages, whereas continuous data was presented with mean and standard deviations (SD). Based on Shapiro-Wilk tests, all variables were non-parametrically distributed, with the exception of operative time. Chi-square proportion tests were used for count data. Univariate and multivariate logistic regression were used to assess the variables of grip strength improvement of ≥10 lbs. (binary) in addition to reaching the NDI minimal clinically important difference (MCID). The MCID for NDI was defined as reaching a 30% improvement from baseline.9,10 Statistical significance was set at an alpha level of <.05. All statistical analyses were performed in STATA version 14 (StataCorp LP, College Station, TX, USA).
Results
Patient Sample
Demographics and Presenting Information.
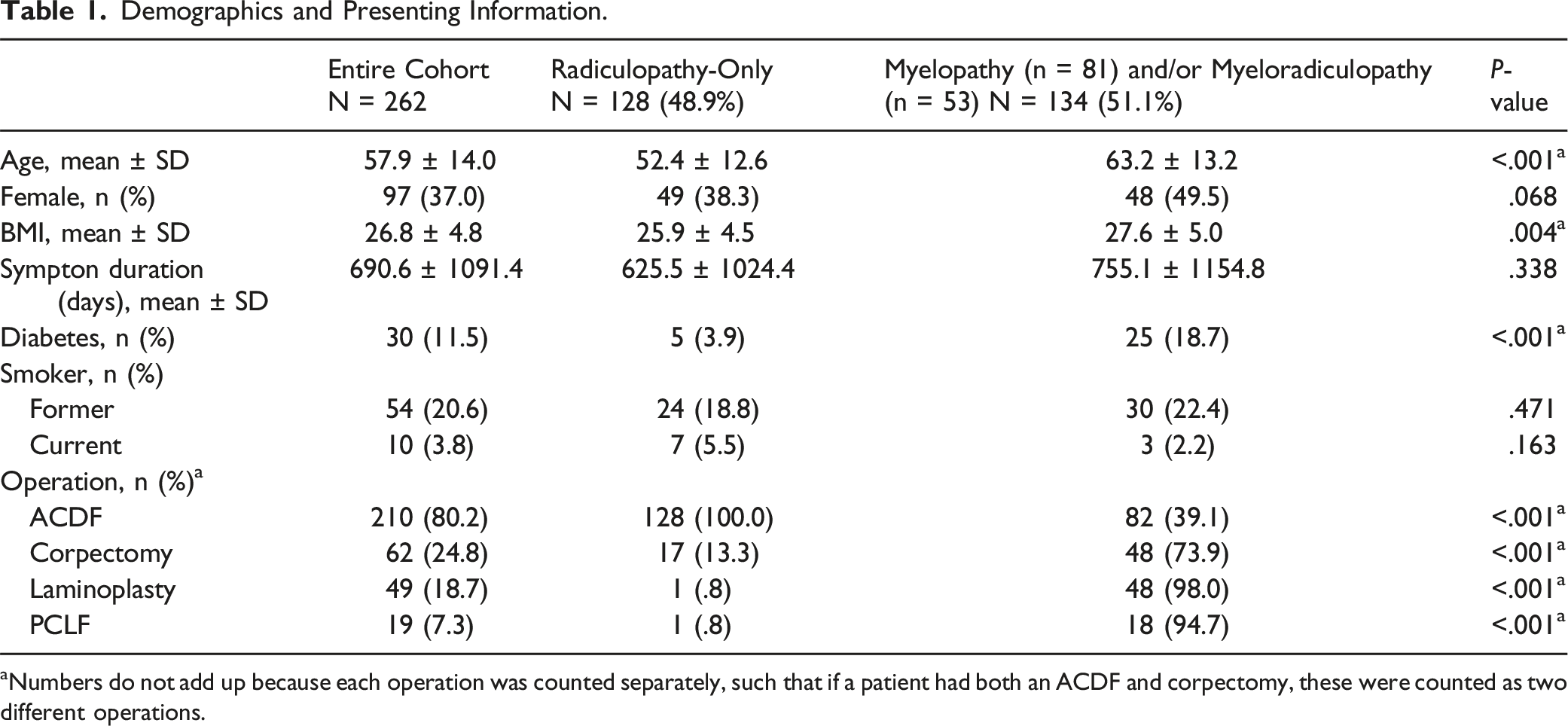
aNumbers do not add up because each operation was counted separately, such that if a patient had both an ACDF and corpectomy, these were counted as two different operations.
Grip Strength Readings
Dynamometer Readings at Each Time Point.
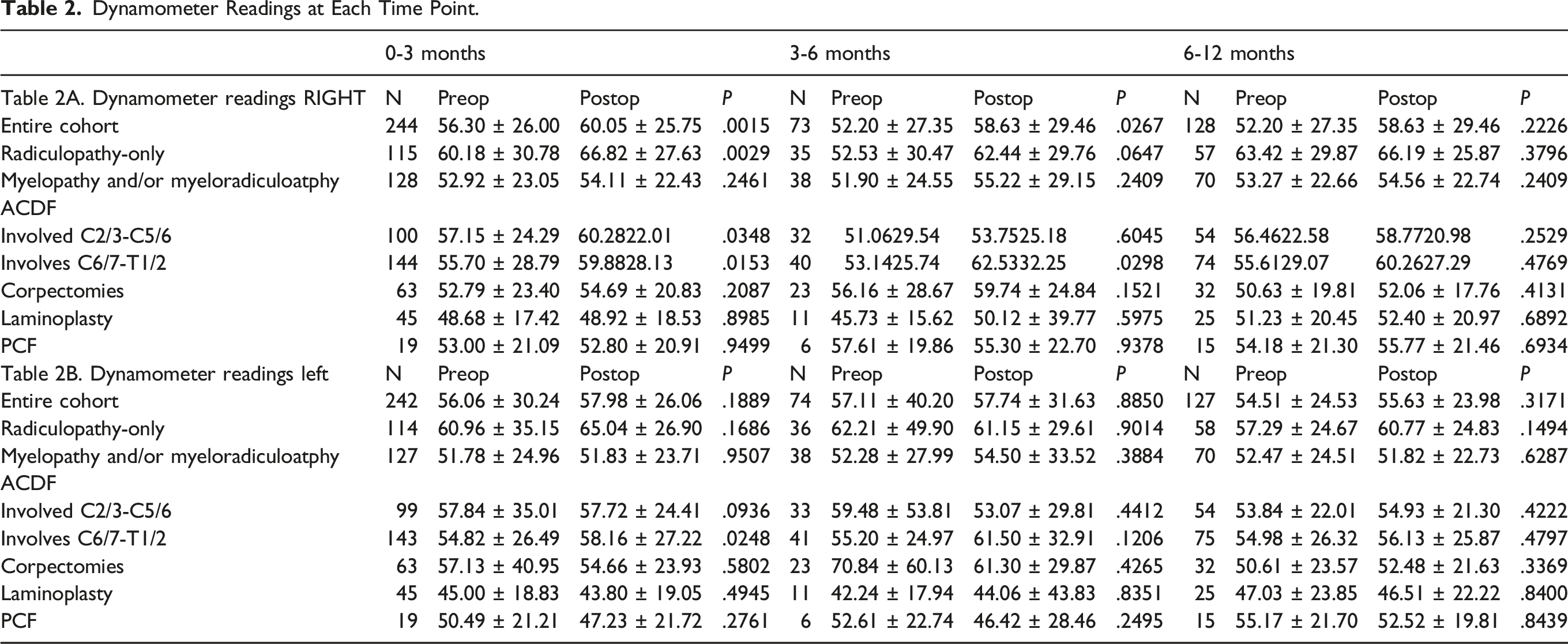
Interestingly, patients undergoing surgery at the C2/3-C5/6 levels and the C6/7-T1/2 levels both significantly improved grip strength by 3 months postoperative: C2/3-C5/6 57.2 lbs. to 60.3 lbs, P = .035; C6/7-T1/2: 55.7 lbs. to 60.0 lbs (P = .015). Correspondingly, a similar percent of improvement was seen in the C2/3-C5/6 group (45/108, 41.7%) vs the C6/7-T1/2 group (65/154, 42.2%) (P = .936). There were no neurologic specific complications. Notably there were no new postoperative neurologic deficits immediately after surgery that would confound grip measurements, such as a compressive hematoma, seroma, pseudomeningocele, or abscess leading to spinal cord or nerve root compression.
Predictors of Grip Strength Improvement
Predictors of Patients With Improved Dynamometer Readings.
Patient-Reported Outcomes
Grip Strength Correlation With Postoperative NDI.

aNDI MCID defined at 30% improvement in NDI.
Discussion
In a large cohort of patients undergoing cervical spine surgery, grip strength improved by ≥10 lbs in 42% of all patients and more commonly occurred in patients with radiculopathy-only (54%) vs myelopathy (31%). Improvement in grip strength was also significantly associated with improved NDI scores. Patients undergoing surgery from C2/3-C5/6 levels and the C6/7-T1/2 levels both significantly improved their grip strength at 3-month postoperatively, yet improvement in the 3-6-month range was only seen in lower cervical patients. Younger patients and those undergoing ACDF were significantly more likely to improve grip strength, whereas those undergoing laminoplasty were less likely to improve grip strength, likely reflecting differences in surgical indication. While the presence of myelopathy, age, and operation impacted postoperative grip strength improvement after cervical spine surgery, levels of surgery appeared to be less important, as patients undergoing surgery in the C2/3-C5/6 region had similar rates of grip strength improvement compared to patients undergoing surgery in the C6/7-T12 region. These results may aid in patient counseling during the early postoperative period.
Several reports of changes in grip strength after cervical spine surgery exist, most in agreement with our findings. Paul et al 11 retrospectively reviewed 40 myelopathic patients undergoing surgery with five different pre- and post-operative quantitative grip strength measurements (maximum, sustained, pinch, key pinch, and sustained key pinch). All five metrics showed significant improvement postoperatively. Interestingly, patients who underwent a posterior approach tended to be weaker pre- and post-operatively, which was also seen in our study. The quantitative metrics used were informative, yet resource intensive, compared to our simple approach of three dynamometer readings obtained by a medical assistant. Yoo et al 12 obtained dynamometer and pinch strength readings in 86 patients undergoing ACDFs. While a postoperative pinch strength increase positively correlated with improved NDI (lower NDI but improved function) in both myelopathy and radiculopathy patients, grip strength increase was only positively correlated with NDI in myelopaths but not radiculopathy patients. These results agree with our current analysis, despite one subtle difference, that we showed a strong correlation between change in grip strength and NDI in all patients.
Conversely, some authors have found conflicting results, that grip strength may not improve after cervical spine surgery. Ylinen et al 13 compared dynamometer readings in 53 ACDF patients compared to 53 matched controls. The authors found no differences between the post-surgical patients and the healthy controls, which may indicate that postoperative patients improve to the point of those not requiring cervical spine surgery. While interesting, this study was limited by the lack of preoperative data. The aforementioned study by Yoo and colleagues 12 did not find any predictors of grip strength, whereas we found multiple, specifically radiculopathy compared to myelopathy, younger age, and undergoing an ACDF.
Several potential reasons exist for our findings, that radiculopathy patients, younger patients, and those undergoing ACDF improve grip strength after surgery. Potential reasons are that younger patients are more physiologically fit and more likely to recover, and that myelopathic patients may have suffered irreversible cord damage that decreases the likelihood of recovery. However, perhaps the most plausible and unifying explanation is the surgical technique employed by the senior author with regards to uncinatectomies performed if patients have a neurological deficit. Though dangerous due to vertebral artery proximity, full uncinate removal can have profound effects on decompressing significant foraminal stenosis. Anecdotally, we sometimes see immediate motor evoked potential improvement in the operating room after the uncinate has been removed. By removing the entire uncinate, and not just opening the posterior foramen, a full decompression is achieved, which we believe significantly improves the chance of strength improvement. The finding that the lower cervical group experienced improvement in the 3-6 month time period may be due to several factors. After surgery at any level, pain may subside that leads to improved grip strength, as patients can use their entire upper extremity when pain free. However, it may take a longer for patients to experience nerve root motor recovery, which is attributable to lower roots C7, C8, or T1. Though these theories may or may not hold weight, the current study was not designed to answer this specific question. Moreover, we must remember that these findings can only be applied to the current small sample, and we withhold sweeping claims about entire surgical procedures due to the lower point and single surgeon nature to our study.
Our study has several notable strengths and limitations. The strengths include the large and diverse patient population and the prospective collection data though this data was analyzed retrospectively. Additionally, a commercially and readily available device was used to collect quantifiable and reproducible strength data. These factors help mitigate the risk of bias. The generalizability of our findings may be limited by the single institution, single surgeon design. Though choosing only one operation to study (eg, ACDF) would have allowed us to focus on one particular type of procedure, such method would not have let us evaluate key differences between each cervical spine operation. Thus, we intentionally kept the sample broad and combined all types of cervical spine surgery in our analyses. Additionally, we did not explicitly account for comorbid conditions that may independently impact grip strength and possibly confound our results such as depression, malnutrition, or double crush peripheral nerve pathology, as this data was not prospectively collected for all study patients. However, we were able to monitor diabetes in our patient population, though within the diabetes population, we were unable to record the presence of neuropathy or not. Of note, the myelopathic patient group also had a higher number of patients with diabetes compared to the radiculopathy group and was also older than the radiculopathy group, which may have biased results. Though these were both controlled for in the multivariate analysis, the unequal proportion of patients with diabetes and ages were major confounding variables that were unequal between groups. We also do not have accurate data regarding the duration of preoperative weakness. This was because many of these patients did not even realize that their grip was weaker than expected, in comparison to the asymptomatic side. Though this information was anecdotal and could not be quantified, it was not an uncommon occurrence for patients to not realize their objective grip deficits, and conversely, patients sometimes thought they had weakness that was not observed on dynamometer testing. Even patients with weakness in their proximal muscles often had a difficult time pinpointing the onset of the weakness. Though every effort was made to elicit a detailed an accurate history, which is an essential part of any cervical spine pathology workup, we therefore felt that it would be inaccurate to attempt to estimate the duration of weakness. Along the lines of a detailed history, two important pieces of information we did not collect were handedness and dominant side of radiculopathy. In an ideal clinical research setting, we would have recorded what handedness the patients were, and also what was their dominant side of radicular presentation. Moreover, though uncinatectomies were performed for neurologic deficits, this was not recorded in our prospective registry. Unfortunately, without this information, our conclusions are limited by these confounding variables. Importantly, each case was divided into individual levels, to most accurately quantify the impact of upper and lower cervical operations. One downside to this approach is that we were not able to capture the number of levels addressed in each procedure, which could reflect the severity of disease.
Conclusions
Grip strength is a functionally meaningful metric to evaluate before and after spine surgery. Conventional methods of grip strength measurements are operator dependent, difficult to reproduce, and challenging to quantify and communicate. The dynamometer objectively quantifies grip strength. This study represents the largest series of patients undergoing cervical spine surgery with preoperative and postoperative dynamometer measurements. Patients with preoperative radiculopathy improved grip strength more often than patients with myelopathy. Patients most likely to see improvement in grip strength were younger and underwent ACDF, whereas those undergoing laminoplasty were less likely to improve. Grip strength improvement was seen in both the C2/3-C5/6 cervical segments as well as C6/7-T1/2 segments during the 0-3-month time period; however, further improvement during the 3-6-month time range was only seen in the lower cervical group.
Footnotes
Acknowledgments
We would like to thank the clinic staff who routinely check patients in and obtain all dynamometer recordings per visit.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.