
Abstract
Study Design
Retrospective cohort study.
Objective
The impact of paraspinal sarcopenia following fusions that extend to the upper thoracic spine remain unknown. The purpose of the present study was to assess the impact of sarcopenia on the development of PJK and PJF following spine fusion surgery from the upper thoracic spine to the pelvis.
Methods
We performed a retrospective review of patients who underwent spine fusion surgery that extended caudally to the pelvis and terminated cranially between T1-6. The cohort was divided into 2 groups: (1) patients without PJK or PJF and (2) patients with PJK and/or PJF. Univariate and multivariate analyses were performed to determine risk factors for the development of proximal junctional complications.
Results
We identified 81 patients for inclusion in this study. Mean HU at the UIV was 186.1 ± 47.5 in the cohort of patients without PJK or PJF, which was substantially higher than values recorded in the PJK/PJF subgroup (142.4 ± 40.2) (P < 0.001). Severe multifidus sarcopenia was identified at a higher rate in the subgroup of patients who developed proximal junction pathology (66.7%) than in the subgroup of patients who developed neither PJK nor PJF (7.4%; P < 0.001). Multivariate analysis demonstrated both low HU at the UIV and moderate-severe multifidus sarcopenia to be risk factors for the development of PJK and PJF.
Conclusions
Severe paraspinal sarcopenia and diminished bone density at the UIV impart an increased risk of developing PJK and PJF in following thoracolumbar fusions from the upper thoracic spine to the pelvis.
Keywords
Introduction
Proximal junctional complications, including proximal junctional kyphosis (PJK) and proximal junctional failure (PJF) are common following thoracolumbar spine fusion surgery, occurring in up to 46% of cases.1-3 The development of proximal junctional pathology is frequently associated with pain, disability, neurologic deficit, and the need for reoperation.1,4 Proposed risk factors for the development of PJK and PJF include insufficient correction of sagittal balance, elevated body mass index (BMI), older age, musculoskeletal frailty, construct extension caudally to the pelvis, low bone mineral density on dual energy X-ray absorptiometry (DXA), and low Hounsfield Units (HU) at the upper instrumented vertebra (UIV).1,5-10 Given the morbidity associated with proximal junctional complications, the search for modifiable risk factors to mitigate the risk of these complications continues.4,6,11-14
Sarcopenia is the progressive loss of skeletal muscle mass and is a manifestation of frailty that is not accounted for by other risk stratification methods.15-17 Studies investigating cohorts of patients undergoing posterior cervicothoracic fusions for myelopathy have revealed that severe qualitative sarcopenia is associated with worse patient reported outcomes, cervical sagittal balance, and junctional alignment.18-20 1 recent study reported that patients with severe qualitative paraspinal sarcopenia were at higher risk of developing proximal junctional complications following spine fusions terminating near the thoracolumbar junction. 10 However, the impact of paraspinal sarcopenia on PJK and PJF following long construct thoracolumbar spine fusion surgery terminating in the upper thoracic spine remains unknown. The present study is the first to assess the impact of paraspinal sarcopenia on the development of PJK and PJF following thoracolumbar spine fusion surgery terminating in the upper thoracic spine using opportunistic evaluation of paraspinal fatty degeneration on preoperative magnetic resonance imaging (MRI). The results of this study may help surgeons identify patients at risk for proximal junctional complications and implement perioperative strategies to mitigate this risk.
Methods
Patient Cohort
Following IRB approval, a retrospective review was conducted of all patients who underwent posterior spine fusion surgery that extended caudally to the pelvis and terminated cranially between T1-6 at a single academic institution between 2008 and 2019. To be included in this study, patients were required to have undergone surgery for degenerative or deformity indications and have a preoperative MRI, a preoperative computed tomography (CT) scan that included the UIV and UIV+1, preoperative and postoperative radiographs, and have a minimum clinical follow-up of 2 years. Patients were excluded if they had an ankylosing spine condition, prior instrumentation at the UIV or UIV+1 that precluded HU measurements, or had a fusion construct that extended proximal to T1 to prevent heterogeneity within the cohort given the differences in HU measurements and the paraspinal musculature between regions of the spine. 21
Demographics and Sagittal Alignment Parameters
Basic demographic variables were recorded, and frailty indices including the modified frailty index (mFI) and the Charlson Comorbidity Index (CCI) were calculated for each patient. Sagittal alignment parameters, including C2 sagittal vertical axis (SVA), pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), lumbar lordosis (LL), L2-T10 lordosis, and PI-LL mismatch were measured on preoperative and postoperative radiographs obtained at least 1-year postoperatively. The proximal junctional angle (PJA) was defined as the cobb angle between the caudal end plate of the UIV and the cephalad end plate 2 vertebrae cranial to the UIV. 4 PJA was measured on postoperative radiographs obtained during the index hospitalization and on radiographs obtained greater than 1 year postoperatively or at the earliest identified occurrence of PJK or PJF. Proximal junctional kyphosis (PJK) was defined as a change in PJA of at least 10° between the immediate postoperative and final follow up standing radiographs. 4 Proximal junctional failure (PJF) was defined as proximal junctional fracture, fixation failure, or kyphosis requiring cranial extension of the fusion. 4
Bone Mineral Density
Hounsfield Units (HU) were measured on preoperative CT scans obtained within 6 months prior to surgery by 2 blinded independent reviewers at L3, L4, the UIV, and the UIV+1 using our institution’s standard imaging software, which is a methodology previously validated in the literature. 22 The reviewers’ measurements were averaged to create the final HU measurement at each level. HU at the UIV and UIV+1 was averaged and considered the variable of interest, and the L3 and L4 HU values were averaged to serve as a control within the construct. Preoperative DEXA measurements were recorded, including bone mineral density (BMD) and t-scores in the lumbar spine, hip, and femoral neck. Utilization of preoperative pharmacologic treatments for low bone mineral density was also recorded.
Paraspinal Sarcopenia
Two blinded independent reviewers performed Goutalier classification of the bilateral multifidus muscles at the level of the L3 vertebral body utilizing axial cuts of T2-weighted MRI sequences (Figure 1).
23
Goutalier grading has been shown to have substantial intra- and inter-rater reliability when assessing the paraspinal musculature.
24
The 2 reviewer scores were then averaged to determine the final Goutalier classification. Patients were classified as Goutalier zero if there were no visible fat streaks in the muscle, Goutalier 1 if there were minimal fatty streaks in the muscle, Goutalier 2 if there was more muscle present than fat, Goutalier 3 if fat and muscle were present in equal quantity, and Goutalier 4 if more fat was present than muscle. Patients were then further classified as having either mild (Goutalier 0-1), moderate (Goutalier 1.5-2), or severe sarcopenia (Goutalier 2.5-4.0) based upon the Fuchs Modification of the Goutalier grading system. This qualitative methodology for assessing paraspinal sarcopenia has previously been correlated with patient reported outcomes and complications following spine surgeries in the cervical and thoracolumbar regions of the spine.10,18-20,23,25 Axial cut of a T2-weighted MRI at the level of the L3 vertebral body with the right-sided multifidus muscle outlined.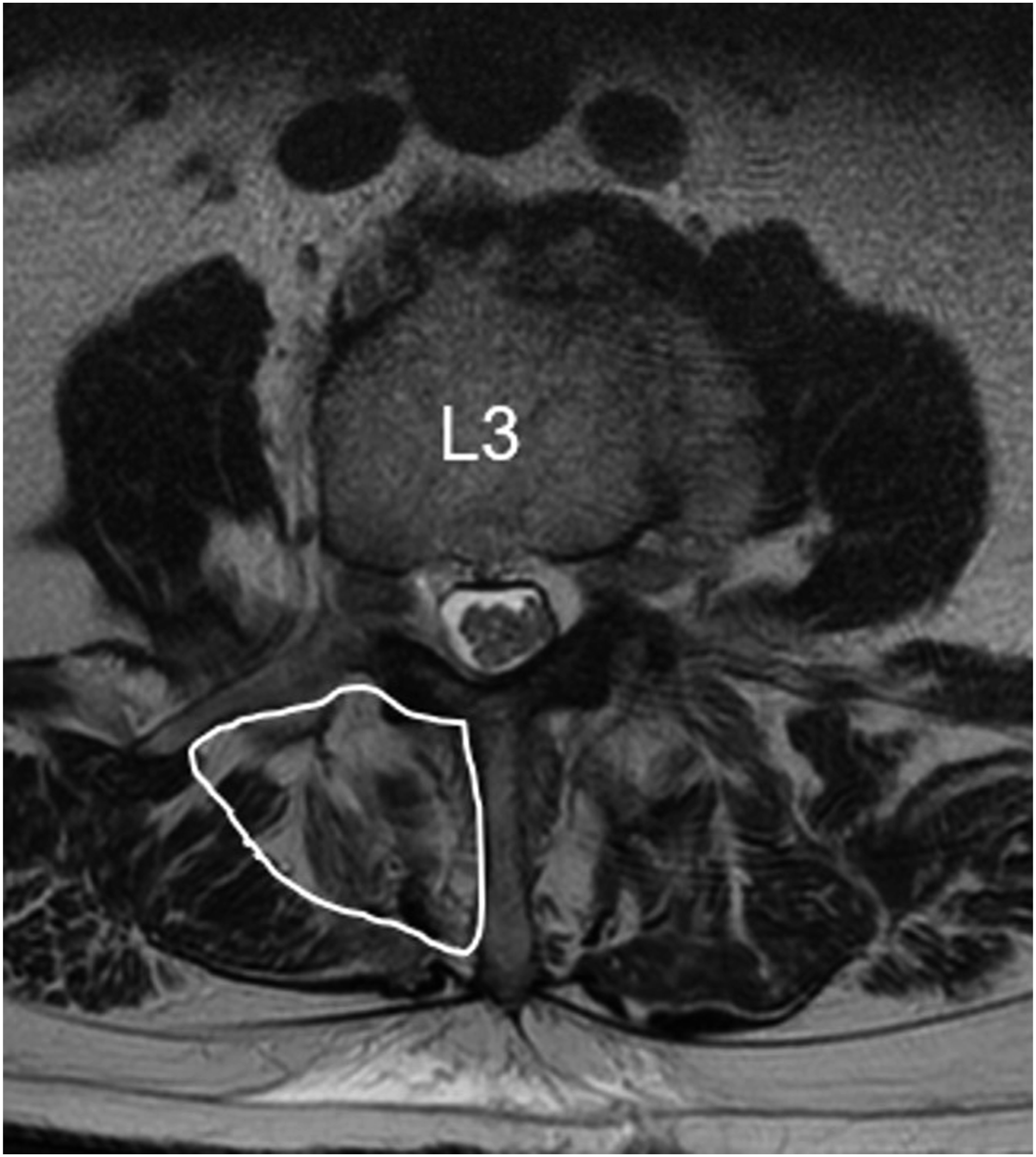
Statistical Analysis
The cohort was divided into 2 groups: (1) patients without PJK or PJF at follow-up and (2) patients who developed a proximal junctional complication, including PJK and/or PJF. Univariate analysis was performed to assess for differences between groups in baseline demographics, sagittal alignment parameters, bone mineral density measurements, and qualitative sarcopenia. Sagittal alignment parameters were compared based upon preoperative values, postoperative values, and the mean difference between preoperative and postoperative values. t test was performed to compare continuous variables between the 2 groups, while Pearson’s chi-squared was performed for categorical variables. In cases that >20% of the cells included <5 observations or if there was a cell with no observations, Fisher’s exact test was utilized in lieu of the chi-squared test.
Multivariable logistic regression analyses were performed to determine risk factors for the development of proximal junctional complications. All statistical analyses were performed in the R environment, version 4.1.0 (R Foundation for Statistical Computing, https://www.R-project.org/), utilizing the “rms” and “arsenal” packages. P-values less than 0.05 were considered statistically significant.
Results
Demographics
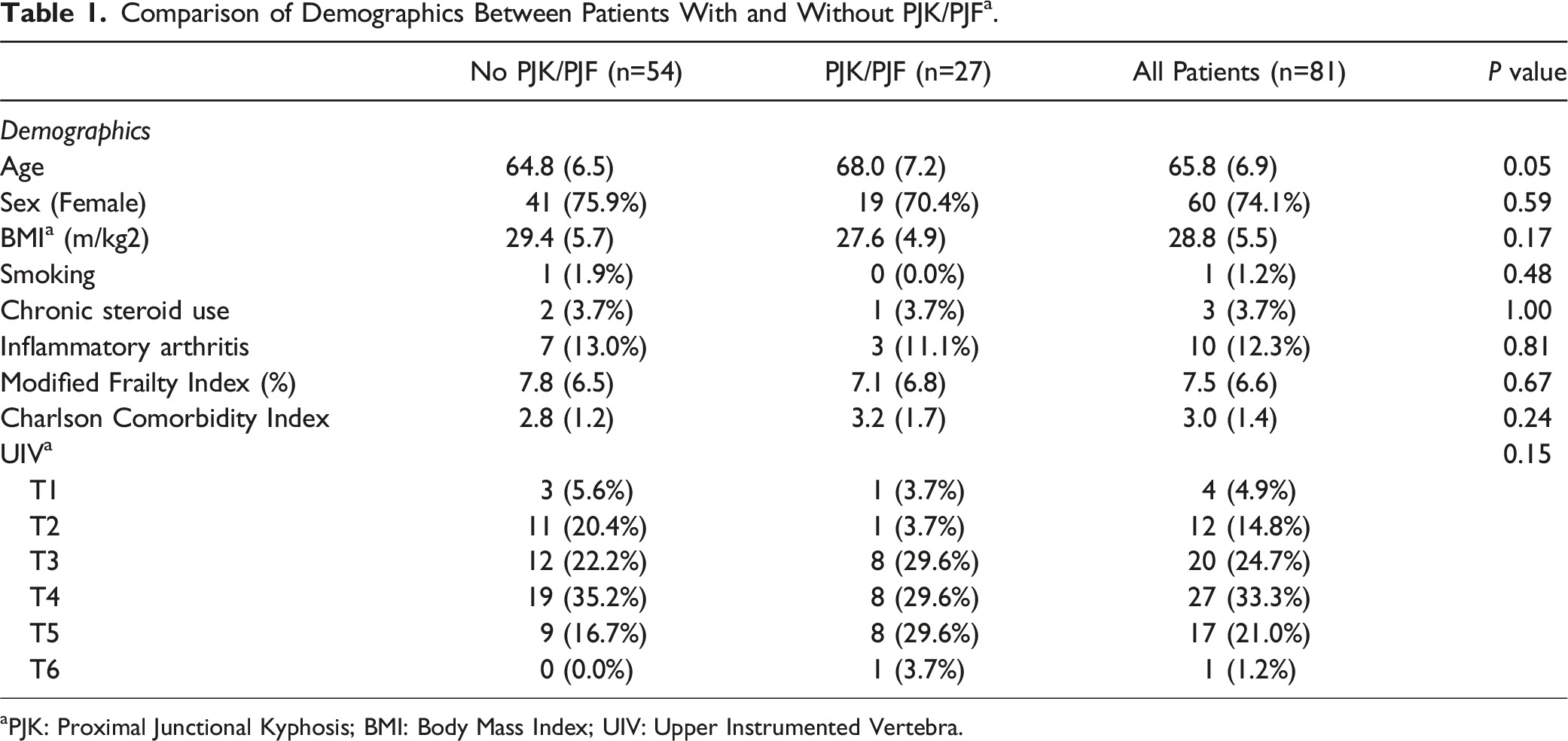
We identified 81 patients for inclusion in this study, including 54 patients without proximal junctional complications and 27 patients who developed a proximal junctional complication (Figure 2). There were no statistically significant differences between these subgroups based upon baseline demographics, mFI, CCI, or location of the UIV (Table 1). (A) Early (PJA 22o) and (B) 2-year (PJA 65o) postoperative lateral standing radiographs of the entire spine demonstrating proximal junctional kyphosis in a patient with severe sarcopenia. This patient subsequently underwent extension of the fusion to C2. Comparison of Demographics Between Patients With and Without PJK/PJF
a
. aPJK: Proximal Junctional Kyphosis; BMI: Body Mass Index; UIV: Upper Instrumented Vertebra.
Sagittal Alignment Parameters
Comparison of Sagittal Alignment between Patients With and Without PJK/PJF a N=81.
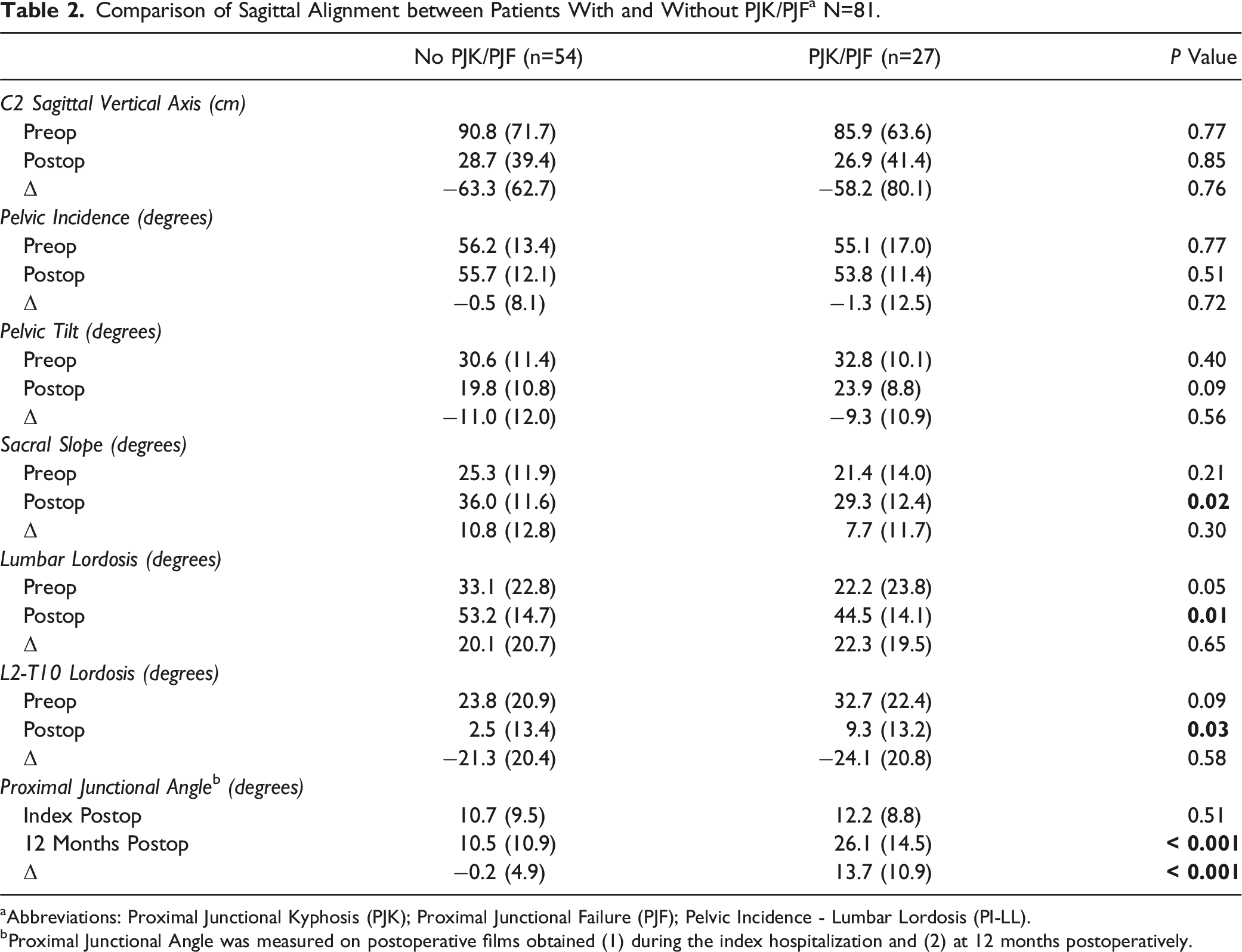
aAbbreviations: Proximal Junctional Kyphosis (PJK); Proximal Junctional Failure (PJF); Pelvic Incidence - Lumbar Lordosis (PI-LL).
bProximal Junctional Angle was measured on postoperative films obtained (1) during the index hospitalization and (2) at 12 months postoperatively.
Bone Mineral Density
Comparison of BMD* between Patients With and Without PJK/PJF* N=81.
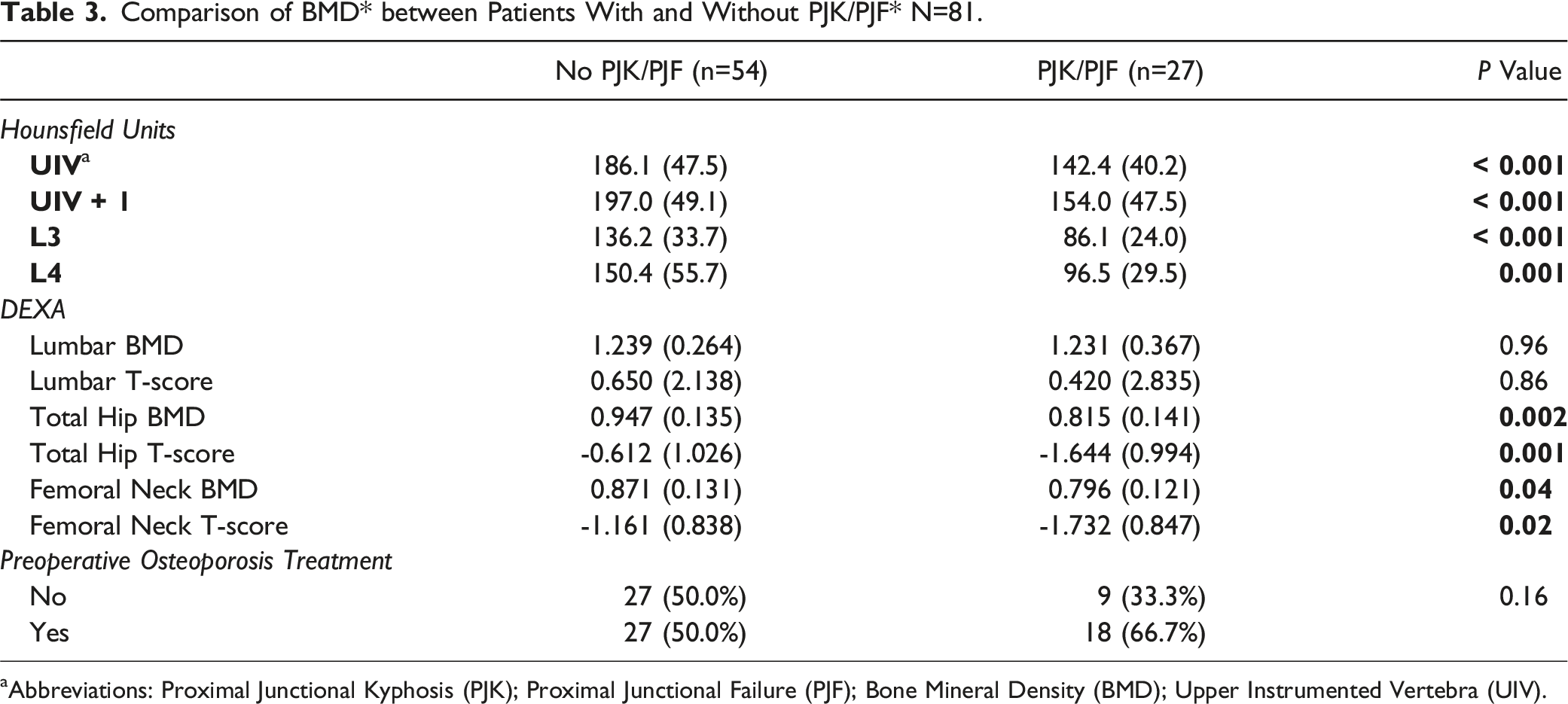
aAbbreviations: Proximal Junctional Kyphosis (PJK); Proximal Junctional Failure (PJF); Bone Mineral Density (BMD); Upper Instrumented Vertebra (UIV).
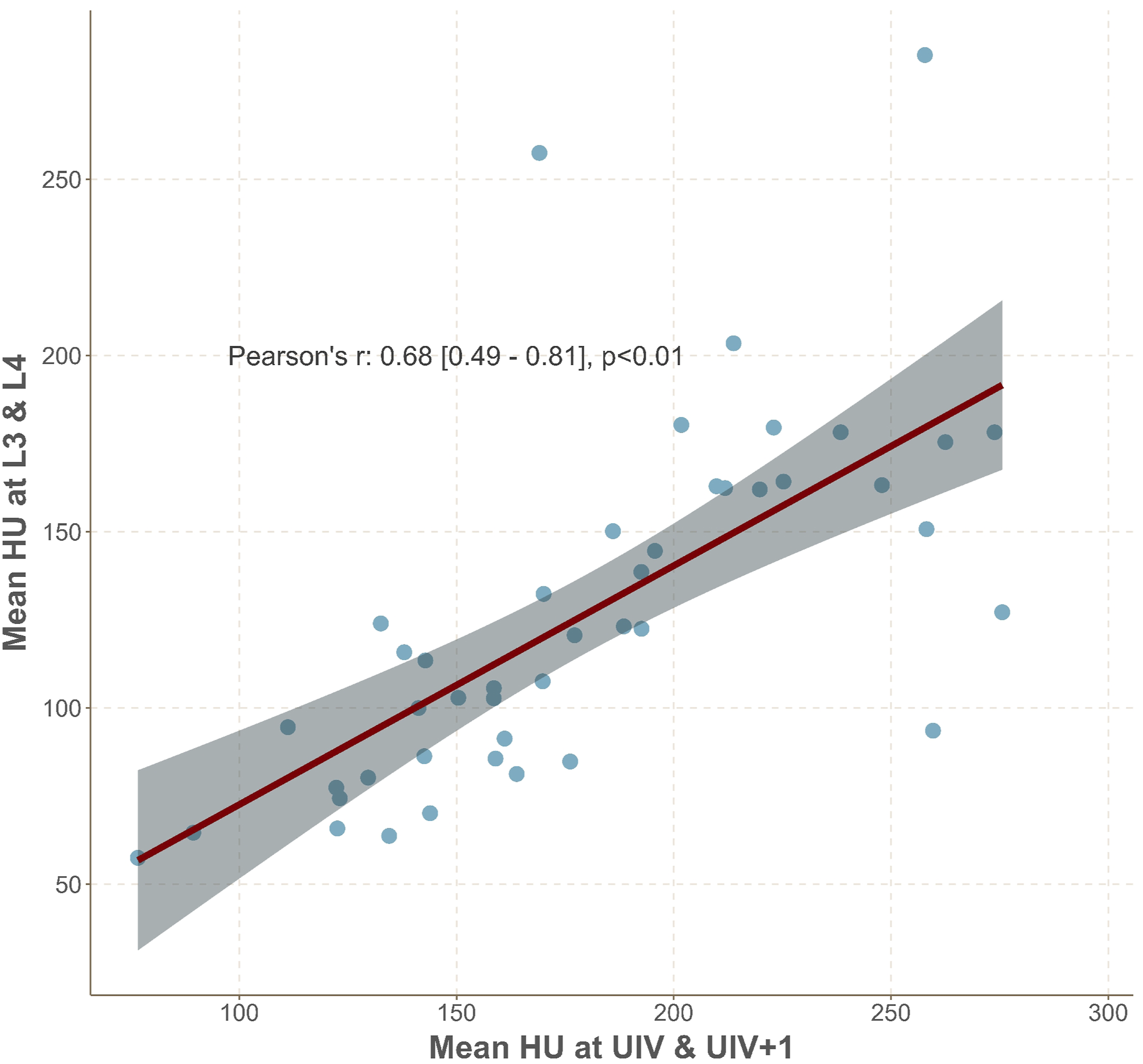
Plot demonstrating the significant correlation between mean vertebral HU at L3 and L4 in comparison to values measured at the UIV and UIV+1 in the upper thoracic spine.
Paraspinal Sarcopenia
Comparison of Paraspinal Sarcopenia between Patients With and Without PJK/PJF a N=81.
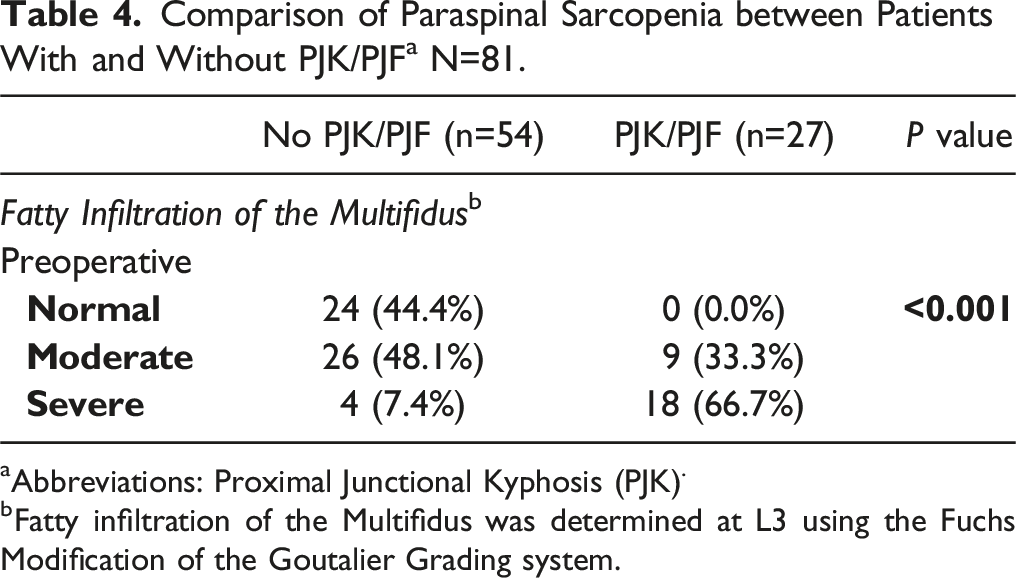
aAbbreviations: Proximal Junctional Kyphosis (PJK).
bFatty infiltration of the Multifidus was determined at L3 using the Fuchs Modification of the Goutalier Grading system.
Comparison of Paraspinal Sarcopenia Based on Age a N=81.
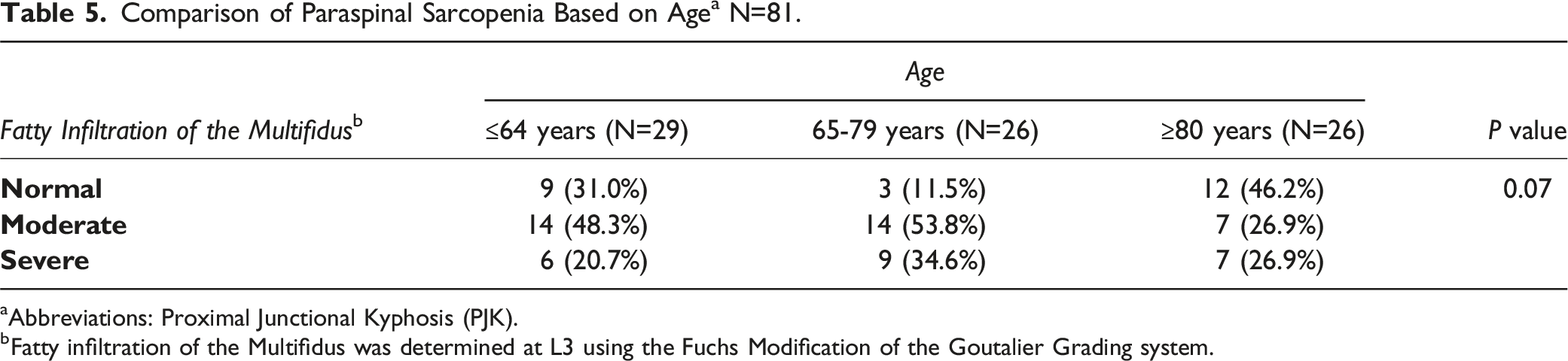
aAbbreviations: Proximal Junctional Kyphosis (PJK).
bFatty infiltration of the Multifidus was determined at L3 using the Fuchs Modification of the Goutalier Grading system.
Multivariable Analysis
Odds Ratios for Development of Proximal Junctional Kyphosis and/or Failure.

*Abbreviations: BMI (Body Mass Index), UIV (upper instrumented vertebra), HU (Hounsfield Units).
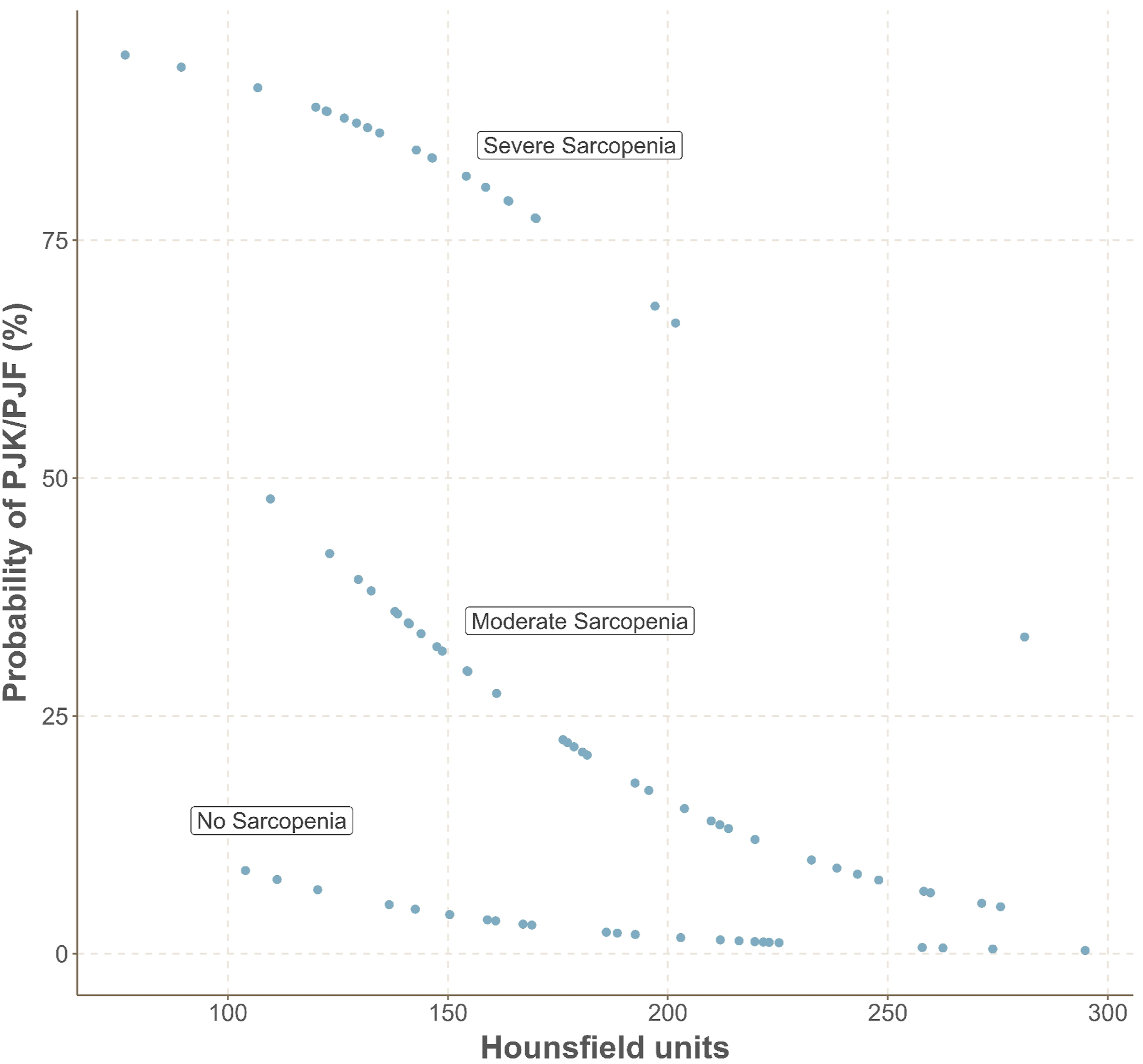
Plot demonstrating the probability of developing proximal junctional complications based upon the combined impact of paraspinal sarcopenia and vertebral Hounsfield Units.
Discussion
Proximal junctional complications following long construct thoracolumbar spine fusions are both common and burdensome to patients and health care systems.1,4 Many studies have sought to identify modifiable risk factors to mitigate the risk of developing these challenging complications.1,5-9 Mikula et al. investigated a cohort of patients undergoing thoracolumbar fusions that terminated near the thoracolumbar junction and reported that decreased HU at the UIV was a risk factor for developing proximal junctional complications. 7 In a subsequent study, the same authors reported that HU at the UIV was also a risk factor for developing proximal junctional complications following long construct thoracolumbar fusions terminating in the upper thoracic spine. 8 However, neither of these studies investigated the impact of sarcopenia on proximal junctional complications. Pinter et al. investigated risk factors for proximal junctional complications following thoracolumbar fusions terminating proximally between T10-L2 and identified that both HU at the UIV and severe paraspinal sarcopenia were significant risk factors for the development of these mechanical complications. 10 The authors postulated that perhaps proximal extension of a spine fusion construct may be 1 modifiable surgical variable to mitigate the risk of PJK and PJF in patients with severe sarcopenia. However, the impact of qualitative paraspinal sarcopenia on proximal junctional complications following long construct thoracolumbar fusions terminating in the upper thoracic spine has remained unknown.
The results of the present study suggest that decreased HU at the UIV and a greater degree of paraspinal sarcopenia are independent risk factors for the development of proximal junctional complications following thoracolumbar fusions extending from the pelvis to the upper thoracic spine. Two-thirds of the patients who developed a proximal junctional complication were moderately or severely sarcopenic, and no patient who developed a proximal junctional complication had normal paraspinal muscle quality. The presence of moderate-severe multifidus sarcopenia as an isolated variable imparted a 23-fold increase in the risk of developing PJK and/or PJF. Mean HU at the UIV was substantially lower in the cohort of patients who developed a proximal junctional complication, which supports the findings by Mikula et al regarding the impact of low bone mineral density, as assessed opportunistically by measuring HU on preoperative CT scans, on the risk of developing PJK and/or PJF.7,8
Ongoing investigations to identify and optimize modifiable patient and surgical variables to mitigate the risk of proximal junctional complications must consider both the cost and ease of application of any new diagnostic test or intervention. In the present study, both HU and paraspinal sarcopenia were assessed opportunistically on routine preoperative imaging, eliminating the need for additional costly diagnostic tests. Furthermore, both the measurement of HU and assessment of paraspinal sarcopenia are simple, rapidly performed, and demonstrate excellent intra- and interrater reliability.7,10,22 Importantly, in both the present study and a previous study by Pinter et al. investigating a cohort of patients with spine fusions terminating near the thoracolumbar junction, HU at the UIV and qualitatively assessed sarcopenia were demonstrated to be independent predictors of proximal junctional complications, while well-known frailty markers such as the mFI and CCI were not predictive of these complications. 10 These findings support the developing theory that paraspinal sarcopenia and vertebral body HU are more spine-specific markers of frailty and may be more strongly correlated with mechanical complications at the junctions of a spine fusion construct than global markers of frailty. The present study adds to the growing body of evidence suggesting that the measurement of HU at the UIV and the qualitative assessment of paraspinal sarcopenia are cost-effective, simple, reproducible, and relevant components of determining a patient’s overall risk profile prior to spine fusion surgery.
Previous studies in both the cervical and thoracolumbar spine have demonstrated an association between qualitative paraspinal sarcopenia and both complications and patient-reported outcomes.10,18-20,23,25 Of particular relevance, Pinter et al. reported that patients with severe paraspinal sarcopenia were at increased risk of PJK and PJF following thoracolumbar fusion surgery terminating near the thoracolumbar junction. 10 The authors postulated that perhaps proximal extension of a spine fusion construct may be 1 modifiable surgical variable to mitigate the risk of PJK and PJF in patients with severe sarcopenia. The present study highlights that a higher degree of paraspinal sarcopenia is similarly associated with proximal junctional complications following thoracolumbar fusion surgeries that terminate in the upper thoracic spine. While the 2 cohorts investigated in these studies are inherently different based upon the length of the fusion constructs for which they were indicated, both studies assessed paraspinal sarcopenia at the level of the L3 vertebral body. Consequently, the present study suggests that qualitative paraspinal sarcopenia likely affects the entire spinal column and, therefore, is unlikely to be bypassed by extending a fusion construct. Future studies may focus on identifying mechanisms for optimizing paraspinal sarcopenia preoperatively, which may include nutrition optimization, preoperative physical therapy, or pharmacologic options to increase skeletal muscle mass.
This study has several limitations. First, this is a retrospective study that may be subject to selection bias. Second, this study assessed only fatty degeneration of the paraspinal muscles, making it impossible for this study to draw conclusions regarding the relationship between quantitative measures of paraspinal degeneration and postoperative outcomes. However, previous studies have demonstrated qualitative measures of assessing paraspinal sarcopenia to be more strongly correlated with outcomes than quantitative measures.10,20 Furthermore, fatty degeneration of the paraspinal muscles was assessed in the mid-lumbar spine, rather than at the proximal junction, which may not represent regional differences in paraspinal sarcopenia. However, this same methodology has been utilized in previous studies given that the paraspinal muscles are robust in the lumbar spine and, therefore, are more readily assessed for evidence of sarcopenia. 10 Third, these surgeries were performed by 8 different surgeons at a single academic institution, introducing the potential for variability in outcomes based upon surgeon technique. However, this cohort was limited to include only patients with pelvic fixation distally and a proximal termination point between T1 and T6, and all of the surgeons follow similar accepted principles with regards to exposure and closure, especially as it pertains to maintaining soft tissue attachments at the proximal junction to mitigate the risk of PJK. Differences may exist between other surgical variables such as the use of interbodies, rod diameter, pedicle screw diameter, angle of pedicle screw insertion at the UIV, and bone graft adjunct, but these differences are unlikely to substantially influence the behavior of the native tissues proximal to the construct. Fourth, while this multivariate analysis attempts to segregate the impact of paraspinal sarcopenia and lower BMD on the development of proximal junctional complications, these 2 variables are likely intertwined markers of frailty, making it difficult to assess the relative influence of each of these variables. Finally, this study only included patients with at least 2 years of clinical follow-up, which is relatively brief when investigating complications such as PJK and PJF that can occur over the course of many years. Future studies may investigate the impact of sarcopenia and diminished BMD on proximal junction complications at longer follow-up.
Conclusions
The present study is the first to assess the relationship between qualitative paraspinal sarcopenia and the development of proximal junctional complications following long construct thoracolumbar fusions extending from the pelvis to the upper thoracic spine. The results of this study add to a growing body of evidence suggesting that both lower HU at the UIV and a greater degree of paraspinal sarcopenia are independent predictors of an increased risk of PJK and PJF. This knowledge may help surgeons identify patients who would benefit from additional preoperative optimization and counsel patients more effectively regarding their risk of perioperative complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Consent was obtained from all study participants prior to inclusion in this study.
IRB Approval
Approval obtained from Mayo Clinic IRB. IRB Approval Number: 18-002622.