
Abstract
Study Design
Prospective multicenter database post-hoc analysis.
Objectives
Opioids are frequently prescribed for painful spinal conditions to provide pain relief and to allow for functional improvement, both before and after spine surgery. Amidst a current opioid epidemic, it is important for providers to understand the impact of opioid use and its relationship with patient-reported outcomes. The purpose of this study was to evaluate pre-/postoperative opioid consumption surrounding ASD and assess patient-reported pain outcomes in older patients undergoing surgery for spinal deformity.
Methods
Patients ≥60 years of age from 12 international centers undergoing spinal fusion of at least 5 levels and a minimum 2-year follow-up were included. Patient-reported outcome scores were collected using the Numeric Rating Scale for back and leg pain (NRS-B; NRS-L) at baseline and at 2 years following surgery. Opioid use, defined based on a specific question on case report forms and question 11 from the SRS-22r questionnaire, was assessed at baseline and at 2-year follow-up.
Result
Of the 219 patients who met inclusion criteria, 179 (81.7%) had 2-year data on opioid use. The percentages of patients reporting opioid use at baseline (n = 75, 34.2%) and 2 years after surgery (n = 55, 30.7%) were similar (P = .23). However, at last follow-up 39% of baseline opioid users (Opi) were no longer taking opioids, while 14% of initial non-users (No-Opi) reported opioid use. Regional pre- and postoperative opioid use was 5.8% and 7.7% in the Asian population, 58.3% and 53.1% in the European, and 50.5% and 40.2% in North American patients, respectively. Baseline opioid users reported more preoperative back pain than the No-Opi group (7.0 vs 5.7, P = .001), while NRS-Leg pain scores were comparable (4.8 vs 4, P = .159). Similarly, at last follow-up, patients in the Opi group had greater NRS-B scores than Non-Opi patients (3.2 vs 2.3, P = .012), but no differences in NRS-Leg pain scores (2.2 vs 2.4, P = .632) were observed.
Conclusions
In this study, almost one-third of surgical ASD patients were consuming opioids both pre- and postoperatively world-wide. There were marked international variations, with patients from Asia having a much lower usage rate, suggesting a cultural influence. Despite both opioid users and nonusers benefitting from surgery, preoperative opioid use was strongly associated with significantly more back pain at baseline that persisted at 2-year follow up, as well as persistent postoperative opioid needs.
Keywords
Introduction
Over the last decades, the use of medical opioids has increased by a factor of 10 and opioid-related deaths have nearly quadrupled.1-3 Insurance data suggest that opioids are the most commonly prescribed drugs for back pain and more than half of routine opioid users report back pain.4-6 The aging of the global population has led to an increased prevalence of adult spinal deformity (ASD), with reports as high as 68% among older adults.7,8 Pain is the hallmark presenting symptom of ASD, it causes significant disability and has a negative impact on patient-reported quality of life. With pain manifesting in nearly 90% of these patients, most of them will eventually take opioids as part of either their initial non-operative treatment or after surgery, or both.6,9 Moreover, substantial advances in surgical approaches, instrumentation, technology and critical care have helped broaden surgical indications, thus allowing for older and more frail patients to be considered for deformity correction surgery. 10 This growing number of elderly adults with painful spinal conditions and the parallel rise in surgical interventions have led to an over 600% increase in spine-related pain opioid expenditure over the past 20 years.6,11-14
It is known that in the acute postoperative setting opioids provide efficacious analgesia, which translates into faster rehabilitation and functional recovery.15-17 However, optimal opioid utilization for subacute or chronic non-cancer pain is still debated, and non-scientific formulations have been shown to increase the risk of side effects and misuse.3,18,19 Furthermore, marketing campaigns such as “Pain is the 5 th vital sign” have pushed a cultural perception demanding opioids, thus resulting in an on-going public health emergency.20,21 This has allowed for increasing recognition of the risks of perioperative opioids including tolerance, respiratory depression, persistent opioid use and dependence. Therefore, strategies to mitigate opioid consumption, in conjunction with their deleterious side-effects and costs, are being sought.
There is particular interest in establishing ideal preoperative opioid usage since despite a growing cognizance of higher morbidity and worse surgical outcomes associated with their use, these medications are still widely prescribed.22,23 Additionally, there are inherent cultural differences regarding the perception of opioid utilization regardless of indication. The purpose of this study was to evaluate pre- and postoperative opioid consumption surrounding ASD and assess the effects of pre-operative opioid use on patient-reported pain scores at 2 years following multi-level spinal deformity surgery in older patients.
Materials and Methods
Study Design and Inclusion Criteria
Patient records were obtained from a prospective, multicenter, international cohort of patients (Prospective Evaluation of Elderly Deformity Surgery -PEEDS database), an AO-Spine funded study to assess operative treatment and outcomes of elderly patients undergoing spine deformity surgery. 24 The original prospective, randomized trial received institutional review/ethics board approval at all 12 participating sites across North America, Asia and Europe and was then registered at clinicaltrials.gov (Identifier: NCT02035280). Written informed consent was obtained upon enrollment for all patients in the original study; however, the present study was approved for a Waiver of Consent, granting exemption from informed consent requirement, due to the retrospective nature of data collection. All cases were patients aged ≥60 years undergoing primary spinal fusion surgery of ≥5 levels for a coronal, sagittal or combined deformity who were capable and willing to sign the consent (No objective values to define deformity were given). Patients meeting inclusion criteria had outcome forms completed at baseline, 10 weeks, 12 months and 24 months.
Data Collection and Statistical Analysis
We retrospectively extracted data that were prospectively collected to gather patient demographic data, surgical information, and clinical characteristics. Reported outcome scores included the Numeric Rating Scale for back and leg pain (NRS-B; NRS-L; range from 0 to 10, with 0 being no pain and 10 corresponding to the most severe pain) and opioid use was collected from standardized case report forms that queried medication use and question 11 from the SRS 22r questionnaire: “Which one of the following best describes your pain medication use for back pain?” Possible choices were: (1) none; (2) non-narcotics weekly or less; (3) non-narcotics daily; (4) narcotics weekly or less; or (5) narcotics daily. 25 Patients were categorized dichotomously as any opioid use (Opi) or no-opioid use (No-Opi) and surgical centers were divided into North America, Europe and Asia.
The primary objectives of this study were to assess the effects of pre-operative opioid use on patient-reported pain scores at baseline and at 2 years after spine deformity correction surgery, as well as to assess international differences regarding pre- and post-operative opioid consumption. We compared reported outcome scores of patients receiving preoperative opioids to those who were not receiving opioids both at baseline and at 2-year follow-up. We also assessed changes in pain scores after surgery among these same groups and calculated least square differences with 95% confidence interval. Finally, we compared opioid use at baseline and at 2 years among patients from North America, Europe, and Asia, and used the NRS leg and back pain as well as the SRS 22-r satisfaction domain scores to assess for any significant regional differences. To detect significant differences between the groups and to compare pre/post-op results, Wilcoxon rank-sum test was performed. Means with standard deviations and medians with IQRs were used to describe continuous and ordinal variables, and frequencies with percentages were used for categorical variables. Differences were considered statistically significant for P < .05. All statistical analyses were performed using SAS (version 9.4, SAS Institute Inc., Cary, NC, USA).
Results
Baseline Demographic Variables of Patients Undergoing Spine Deformity Correction Surgery.
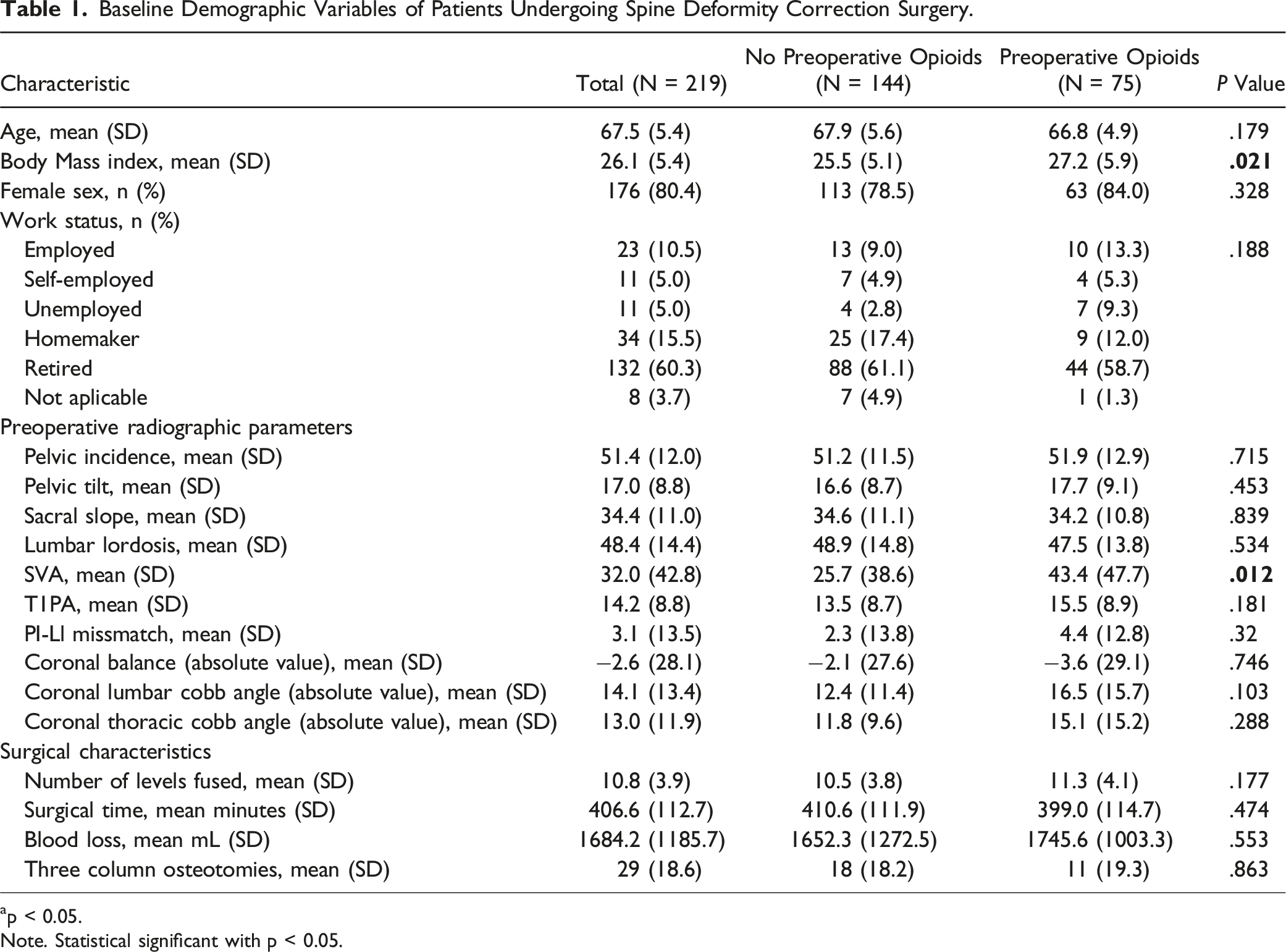
ap < 0.05.
Note. Statistical significant with p < 0.05.
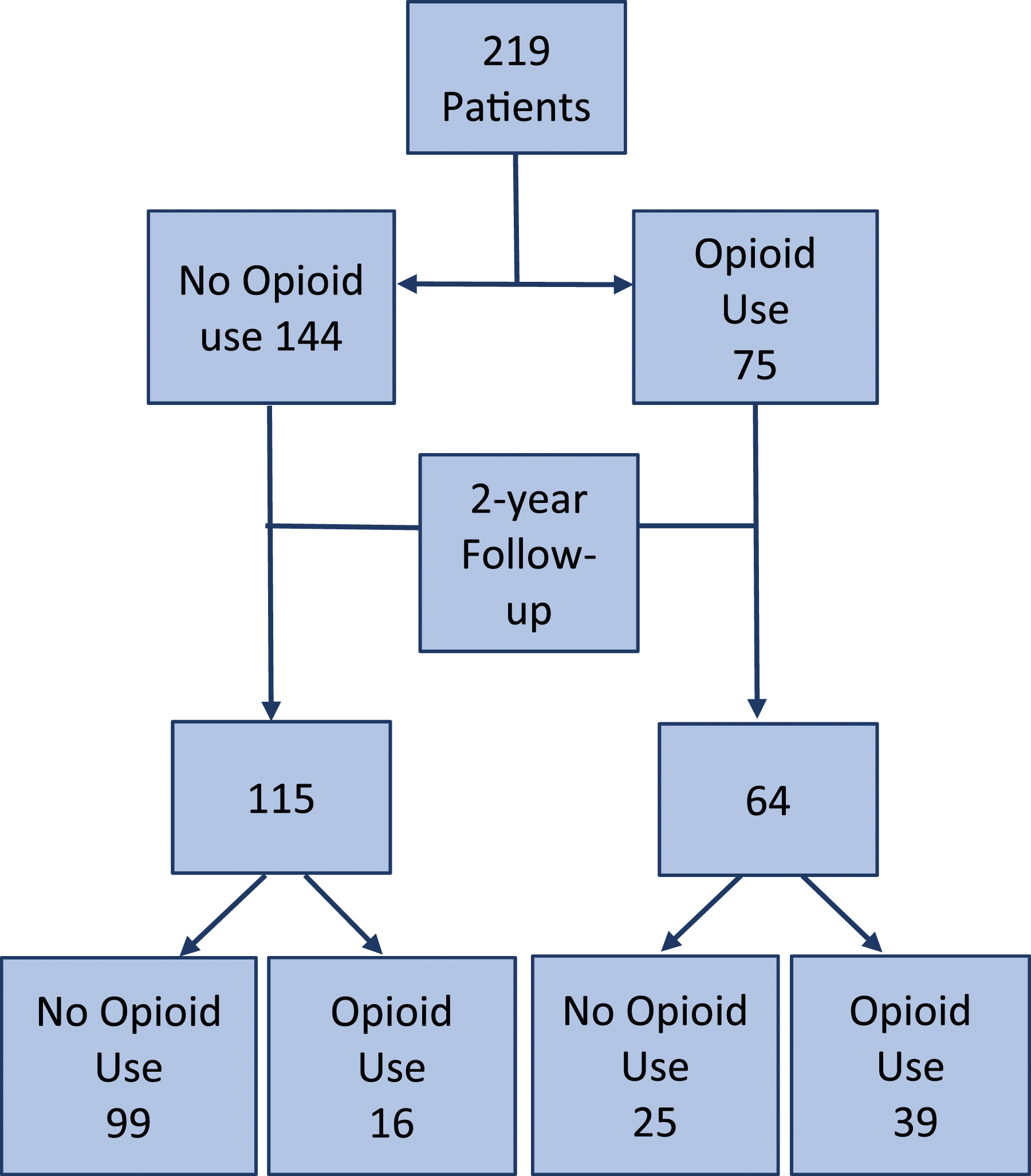
Distribution of patients reporting opioid intake at baseline and at 2-year follow-up.
Pain NRS Data at Baseline by Opioid Use Derived From SRS-22r Questionnaire and Prescribed Drugs Statement.
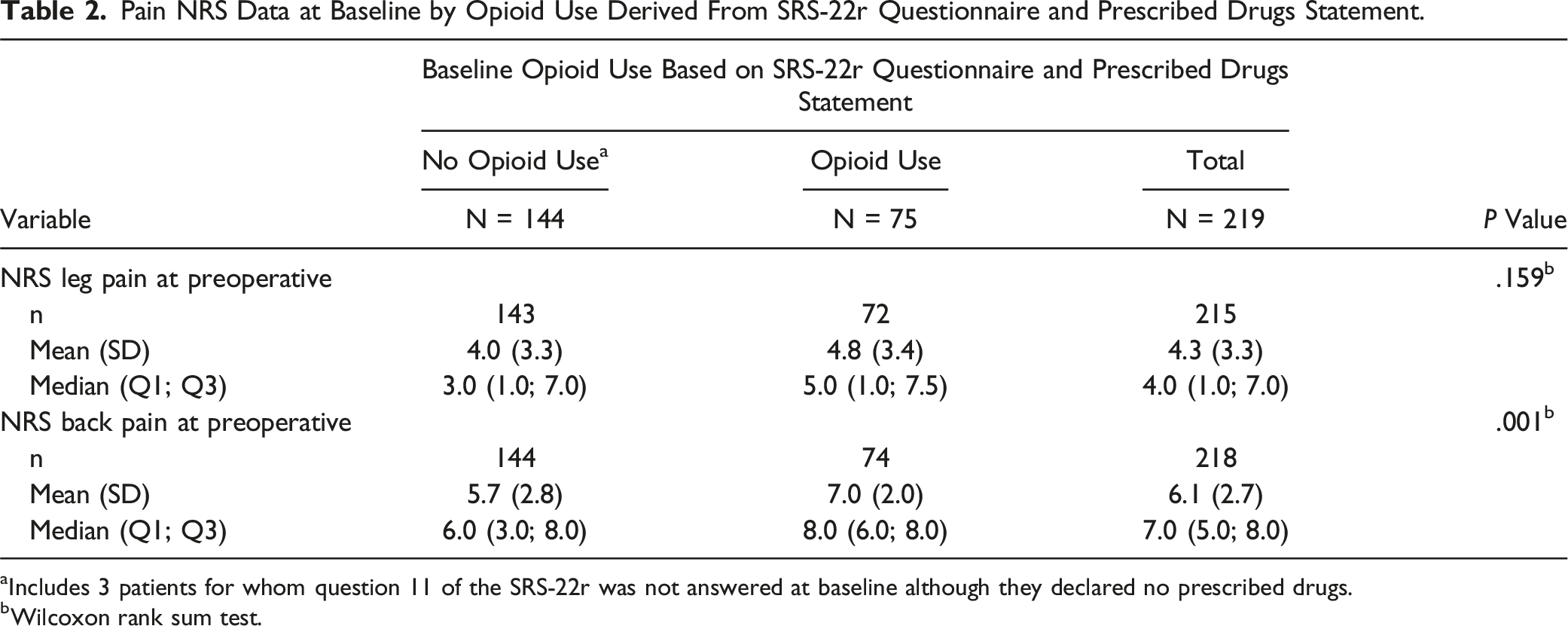
aIncludes 3 patients for whom question 11 of the SRS-22r was not answered at baseline although they declared no prescribed drugs.
bWilcoxon rank sum test.
Pain NRS Data at 2-Year Follow-Up by Opioid Use Derived From SRS-22r Questionnaire and Prescribed Drugs Statement.
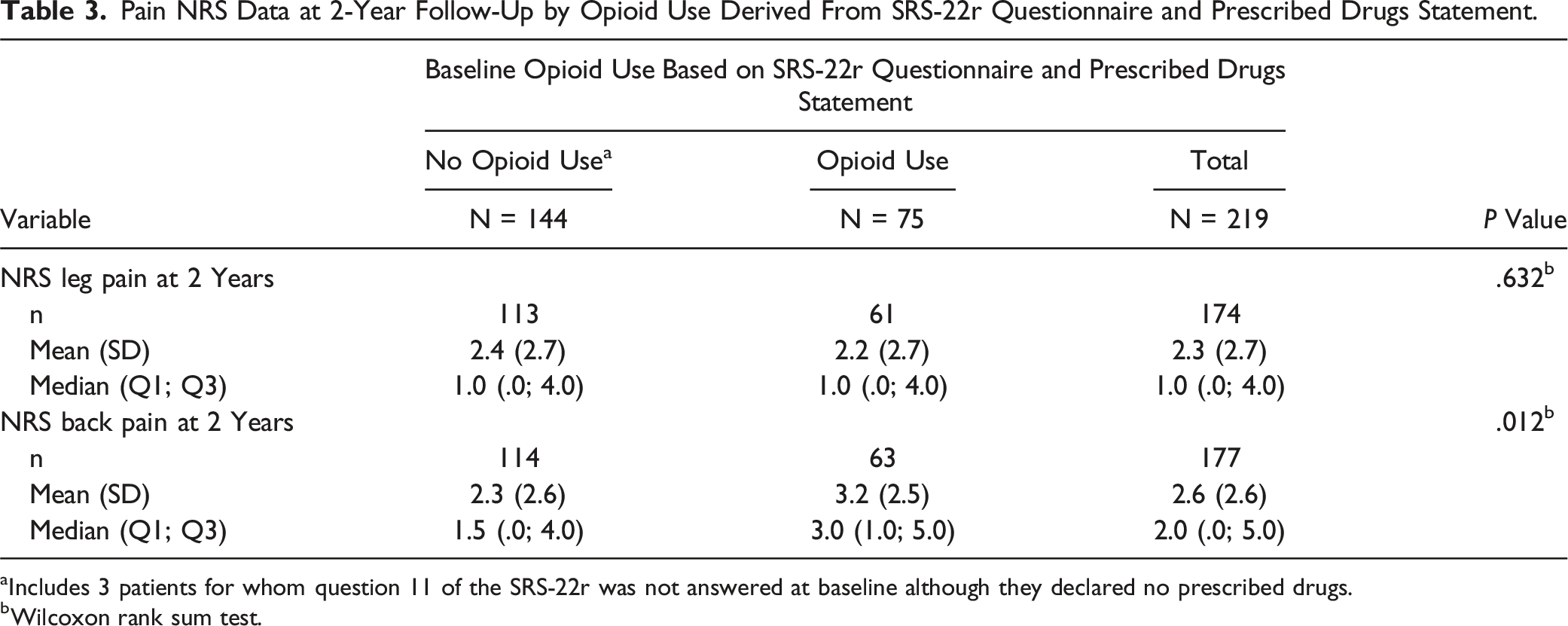
aIncludes 3 patients for whom question 11 of the SRS-22r was not answered at baseline although they declared no prescribed drugs.
bWilcoxon rank sum test.
Change in Pain NRS Scores at 2-Year Follow-Up by Opioid Use Derived From SRS-22r Questionnaire and Prescribed Drugs Statement.
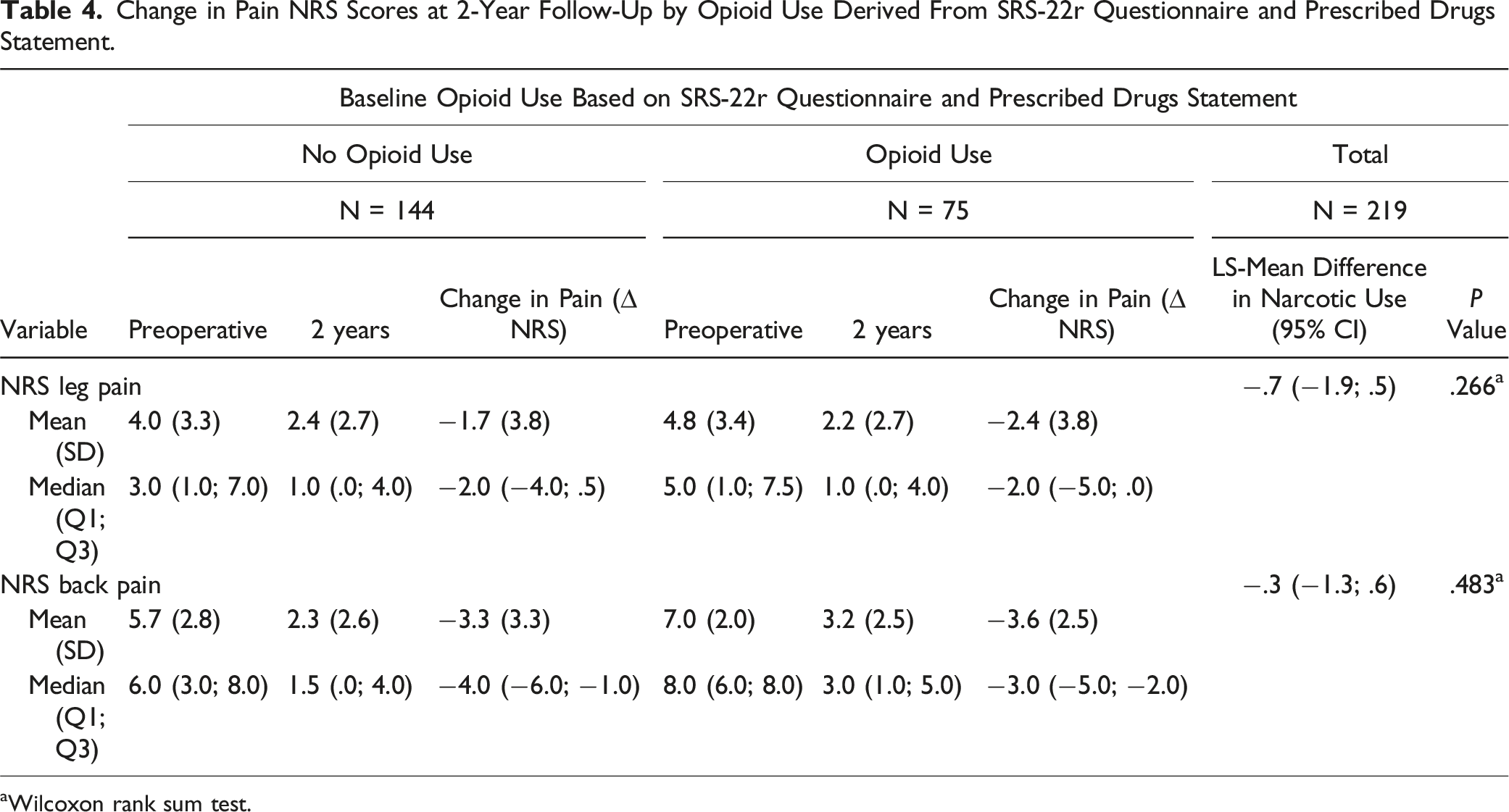
aWilcoxon rank sum test.
Opioid Use With Patient Satisfaction and Pain by Region Derived From SRS-22r Questionnaire and Prescribed Drugs Statement.
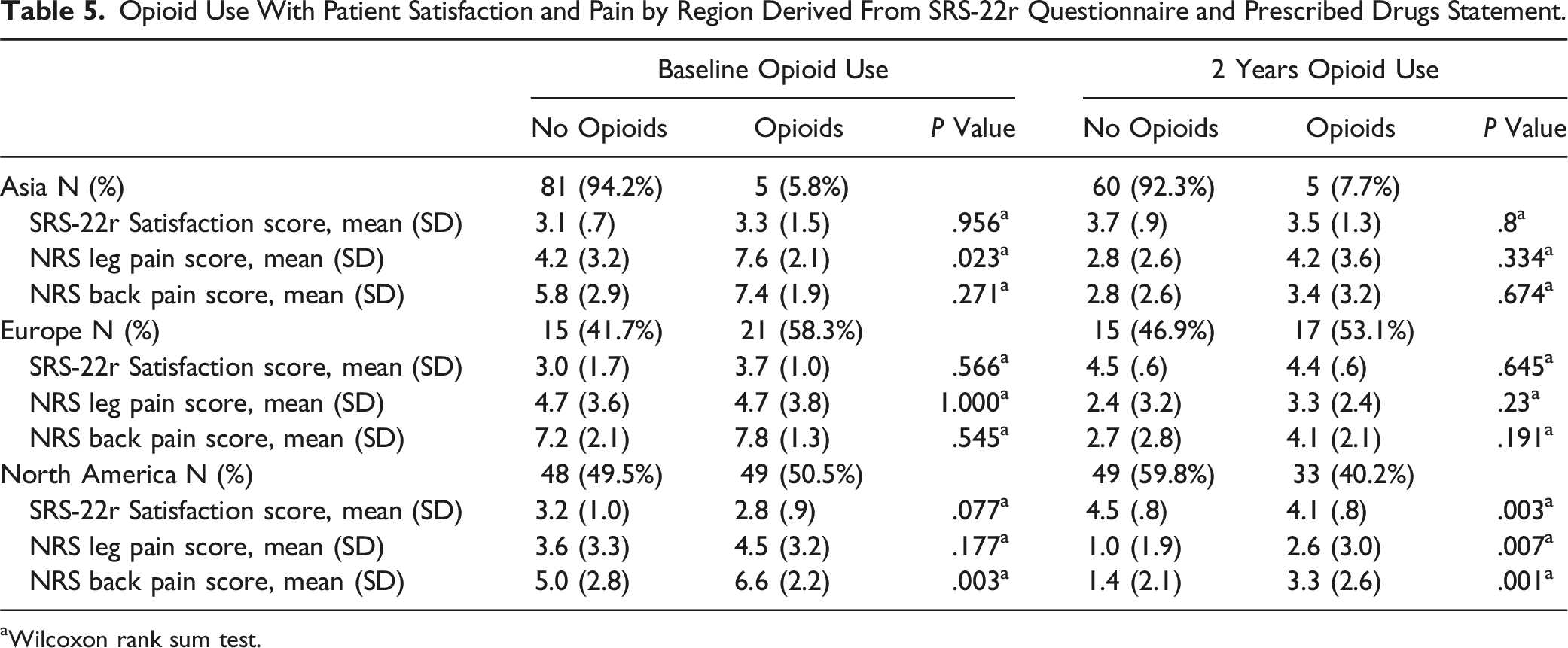
aWilcoxon rank sum test.
Discussion
Impact of Opioid Use on Clinical Outcomes
In this multicentric, multicontinental study of patients ≥60 years undergoing elective spine deformity correction surgery, we found that nearly one-third of patients were consuming opioids pre- and postoperatively world-wide. This is consistent with opioid prescription data in national registries, where 38% of adult patients are found to use opioids at some point during the 12 months prior to any surgical intervention. 26 Previous reports have shown that regular opioid use before surgery is one of the strongest predictors for poorly controlled postoperative pain and is the single most influential predictive factor for opioid refills.27,28 When compared to opioid naïve patients, even minimal preoperative opioid use has been reported to increase the likelihood of requiring prescription refills after surgery (OR 1.49, 95% CI 1.45 – 1.53; P < .001) and an even stronger association is seen if these medications are taken chronically (OR 60.79, 95% CI 27.81–132.92, P < .001). 26 Furthermore, given that nearly 20% of opioid users undergoing spine surgery may be opioid-dependent, high rates of chronic postoperative opioid use are to be expected after these interventions.29-31
Our results indicated that odds ratio for continued opioid use at 2 years postoperative was 9.65 (95% confidence interval = 4.65-20.00, P < .001) for opioid vs non-opioid users. These findings are supported by previous reports also demonstrating the strong association between opioid use prior to spine surgery and their continuation in the postoperative period.3,22,23,29,31-34 However, we observed, that despite 33.3% (25 patients) of baseline opioid users being able to stop taking opioids by the last follow-up, the percentage of patients overall still depending on them 2 years after surgery was considerably high (30.7%). Since only 16 of the initial non-opioid users were taking these medications long after surgery, nearly 70% of the sustained postoperative opioid use observed in our study largely resulted from the high incidence of preoperative use itself (34.2%) (Figure 1). Unlike most ASD studies that usually include revision surgeries, all our patients underwent primary interventions, which makes the incidence of preoperative opioid use strikingly high.
Prolonged postoperative opioid use might suggest surgery failed to provide the expected results in terms of symptomatic relief. However, we observed that pain scores significantly improved after surgery in both opioid users (∆ NRS back pain score: −3.6 and ∆ NRS Leg pain score of −2.4) and non-users (∆ NRS back pain score: −3.3 and ∆ NRS Leg pain score of −1.7) (Table 4). Pain and disability are characteristically what lead patients with ASD to seek surgical treatment and there is substantial evidence supporting significant improvement in pain, HRQoL outcomes, patient function and satisfaction after surgery.7,12,13,24,35 Nevertheless, the majority of these patients have struggled with chronic pain long before surgery and have likely exhausted non-operative interventions, including conventional analgesics and opioids. These chronic painful conditions and their subsequent opioid exposure have been shown to alter pain perception pathways with unintended consequences like allodynia, opioid-induced hyperalgesia (OIH), opioid tolerance and withdrawal-associated hyperalgesia (WAH). 36 Therefore, despite successful surgical interventions, it is possible that these patients may experience higher levels of postoperative pain, increased opioid demands and pose a considerable challenge when trying to wean them off opioids, when postoperative pain should theoretically be controlled.
This distorted nociceptive sensitization may potentially explain why patients in the opioid group, who were presumably receiving “stronger” opioid-based preoperative pain regimes, had significantly more back pain at baseline compared to patients who were not using opioids (NRS Back pain 7.0 [SD 2.0] vs 5.7 [SD 2.8], P = .001). However, while leg pain scores were similar in those with and without preoperative opioid use (NRS Leg pain 4.8 [SD 3.4] vs 4.0 [SD 3.3], P = .159), ASD can present with both back and radicular pain, but there is usually a predominant and most debilitating symptom that directs the invasiveness of the procedure.37-39 Since our patients consisted of coronal and sagittal deformities requiring multilevel instrumentation, their main concern was axial mechanical back pain, thus reflected in the substantial difference between back- and leg pain intensity scores across all patients. Except for the SVA, all spinopelvic parameters were similar among both groups, indicating comparable magnitudes of sagittal and coronal deformities between users and non-users (Table 1). Similar results were reported by Line et al 40 where a propensity score matched analysis of 262 operatively treated ASD patients demonstrated greater baseline NRS back- (7.7 vs 6.8) and leg pain (2.5 vs 2.3) in patients using opioids before surgery as compared to non-opioid users. In their study, both groups of patients had comparable deformity magnitudes, comorbidity burden, history of mental illness and surgical invasiveness.
Interestingly, despite substantial symptomatic relief indicating both groups benefitted from surgery, at last follow-up there was still a statistically significant difference in NRS back pain scores between the Opioid- and No-Opioid groups (3.2 [SD 2.5] vs 2.3 [SD 2.6], P = .012). These findings are consistent with those by Hills et al 34 where preoperative opioid therapy was associated with significantly higher odds of not achieving a clinically meaningful improvement at 1 year in extremity pain (aOR, 1.55; 95% CI, 1.21-1.99; P = .001) and axial pain (aOR, 1.73; 95% CI, 1.37-2.18; P < .001). However, unlike our study where opioid use encompassed any opioid consumption, they only included chronic users (having an active prescription >50% of the days in each month for 3 consecutive months prior to surgery) of which 73% were on high opioid doses (daily morphine milligram equivalents >30). This might suggest that chronicity and dosage have an impact on outcomes and should also be considered prior to surgery. There are also numerous publications involving smaller spine surgeries, including decompressions, cervical and lumbar short-segment fusions and even minimally invasive techniques, in which opioids also were shown to have a negative effect on outcomes.3,21,30,33,41,42 Our results add to the growing body of literature suggesting a negative impact of preoperative opioid use on postoperative outcomes that seems to exists regardless of the invasiveness of the procedure.
Furthermore, preoperative opioid use has been shown to impact other outcome measures besides pain scores. In a systematic review by Yerneni et al 31 that included 45 studies, opioid use was a negative predictor of return to work status, hospital stay, healthcare costs, wound complications and risk of revision surgery. Other studies have also shown a negative impact over ICU length of stay, overall postoperative complications, the 12-item Short Form Health Survey, Oswestry Disability Index and Neck Disability index.23,28,43 There are no definitive explanations as to why preoperative opioid use is associated with worse clinical outcomes, and though it is probably multifactorial, the intrinsic hyperalgesia induced by opioids likely plays a critical role. In light of our results, one could make the argument that preoperative opioid use might be one of the most prevalent modifiable risk factors and that discontinuing or reducing opioid medications prior to ASD correction surgery could lead to better clinical outcomes. Potentially, detoxification and interdisciplinary collaborations could allow for a safe and tolerable transition to non-opioid alternatives and improved preoperative management. However, further research is warranted to recognize if reversing opioid use could lead to better outcomes after spine surgery and if so, establishing proper pathways to achieve this goal.
Our results also highlight the impact of sustained postoperative opioid use. Similar to our findings in which 14% of opioid naïve patients reported still using opioids at last follow-up, a study by Deyo et al 44 that included nearly 2500 patients undergoing spine surgery found that 12.8% of preoperative non-opioid users were also utilizing long-term opioids for pain control. Effective perioperative pain management can significantly improve functional recovery and rehabilitation after spine surgery, hence pain control is a fundamental aspect of the postoperative care.15-17 However, though opioids are effective analgesics in the acute setting, subacute and chronic use remain controversial and have not been shown to be superior to non-opioid formulations in terms of pain relief, safety and functional outcomes.15-17,28,45 Bearing in mind indiscriminate use of opioids and long-term consumption increases the risks of side effects, misuse, dependence, abuse and health-related costs, numerous clinical practice guidelines are now recommending against their use and suggest that alternate strategies for pain control should be considered.3,18,19,46 Multimodal pain management should target reduced opioid use in the perioperative period, ideally reserving opioids only as rescue analgesia; and in cases of opioid-dependent or opioid-tolerant patients, medications like gabapentin, pregabalin and intraoperative ketamine infusions show promising opioid-sparing effects with significant reduced postoperative opioid consumption after spine surgery.47-51
Regional Differences in Perioperative Opioid Use
To our knowledge, this is the first report comparing regional differences in opioid use before- and after spine surgery, between North American, European, and Asian populations. While out of the 3 patient groups Asians reported significantly less pre- and postoperative opioid use, the percentage of opioid users seemed to slightly increase after surgery (5.8% vs 7.7%). However, the total number of opioid users in the Asian patients remained unchanged (5) and this increase resulted from 21 nonusers being lost during follow-up. In contrast, postoperative opioid use in the North American and European patients decreased after surgery from 50.5% to 40.2% and 58.3% to 53.1% respectively, which suggests that surgery provided enough symptomatic improvement that allowed for opioid discontinuation. Much like the results of our data, and consistent with previous publications, subgroup analysis revealed that the vast majority of postoperative opioid users result from persistent preoperative use.
There are few reports in the literature addressing opioid use in spine surgery among European patients, but the high proportion of opioid users observed in our study contrasts significantly with previous published data. An observational study of by Holmberg et al 52 that included over 30 000 patients with degenerative lumbar spine disorders from 2 Norwegian registries found that only 8.7% of patients were using opioids in the year previous to their surgery, however similar to our results nearly two-thirds of these patients continued to use opioids 2 years postoperatively. In 2 other multicentric studies published by the European Spine Study Group, preoperative opioid use was reported to be 18% and 24.2%.53,54 We believe these reports may underrepresent the true prevalence of opioid use in European patients undergoing spine surgery mainly because of how opioid consumption was defined. In the Norwegian paper opioid use was defined as 180 Defined Daily Doses (DDDs) or >4500 oral morphine equivalents (OMEQ) for 365 days, with prescriptions dispensed in 3 of 4 quarters of the year; while Bourghli et al 54 defined opioid use as daily narcotic consumption and patients using opioids on a weekly basis or less were included within the No-painkiller/Minor user group. Even minimal opioid consumption impacts postoperative opioid use and “minor” use should not be overlooked when a patients is deemed candidate for any spine surgical intervention.
Interestingly, despite having the highest percentage of baseline users, there was no difference in NRS-B or NRS-L scores for European patients at baseline or at 2 years following surgery, regardless of opioid use. Asian patients taking opioids at baseline did have worse mean NRS-L scores (7.6 vs 4.2, P = .023) but otherwise there was no difference in baseline NRS-B or 2-year NRS-B or NRS-L scores. These regional results differ from our pooled data and from previous publications in which baseline opioid use is associated with worse baseline and postoperative pain scores. We believe this might be secondary to variations in intake chronicity, dosage and opioid potency among populations. In a study by Lee et al 43 multivariate analyses demonstrated that increased preoperative opioid use was a significant predictor of decreased SF-12 PCS and MCS and increased ODI scores postoperatively; in fact, every increase in 10-mg morphine equivalent amount taken preoperatively predicted a .3 decrease in SF-12 and a .6 increase in ODI postoperatively (P < .05). This is consistent with findings by Holmberg et al 52 where European patients receiving homogenously high opioid doses reported larger mean ODI scores at baseline than nonusers (51.0 points vs 41.9 points, P < 0.001) and larger mean NRS scores for both back pain and leg pain in the year following surgery. Local regulations and health system demands likely cause significant differences in opioid prescriptions between regions which were not discerned by the questionnaires used in our study.
Though prescription and intake dosages in our study were not specified, opioid formulation trends in Europe appear to be more conservative than in North America. Abul et al 53 reported that 96% of opioid users from 5 cites across Europe were found to be receiving weak opioids prior to spine deformity correction surgery, while in a North American based study, Hills et al 34 identified high-preoperative opioid dosage (>30 MME/d) in 73% of patients. These differences might explain why opioid use in North American patients was associated with worse baseline NRS-B (6.6 vs 5.0, P = .003) and 2-yr NRS-B (3.3 vs 1.4, P = .001) and NRS-L (2.6 vs 1.0, P = .007). Also, this might explain why there was no statistically significant difference in satisfaction between nonusers and opioid users in the European (4.4 vs 4.5, P = .8) and Asian (3.5 vs 3.7, P = .645) populations, while North American nonusers were more satisfied after surgery than opioid users (4.5 vs 4.1, P = .003). The amount, potency and chronicity of opioid consumption that leads to chronic postoperative use and significant changes in clinical outcomes remain unknown and further studies will be needed to assess this.
Limitations
Since our study was a post-hoc analysis, the definition of “spine deformity” relied on the inclusion criteria used by the authors of the original paper. Unfortunately, Nielsen et al 24 did not specify the objective coronal nor sagittal values used to define deformity, but rather included patients who underwent multilevel lumbar fusion >5 levels. Furthermore, one of the major limitations we encountered was the lack of specific data regarding opioid dosing before and after surgery. This limited the ability to evaluate dose reduction after surgery, considered an indirect marker of success; and from properly assessing the impact of chronicity and the dose-dependent effect over clinical outcomes and postoperative opioid dependence. Since this was a multicentric transcontinental study, regional differences between pre- and postoperative pain management likely resulted in heterogeneous formulations that were reflected in our results among the different populations. Studies with structured protocols are needed to adequately interpret these variations. Also, the retrospective nature of the design does not allow us to draw conclusions about causality, despite the evident association between preoperative opioid use and dependence as well as over clinical outcomes. Finally, since our study relied on patient questionnaires there was a potential for recall bias that in future research can be addressed using prescription data which will also add granularity to the amounts and time of consumption.
Conclusions
The present study indicates that almost one-third of surgical ASD patients were consuming opioids both pre- and postoperatively world-wide; there is a drastic international variation, with Asia having a much lower usage rate, suggesting a cultural influence. Despite both users and nonusers benefitting from surgery and experiencing significant improvement in pain scores, our results support the growing evidence that preoperative opioid use is strongly associated with persistent postoperative opioid consumption. Furthermore, preoperative opioid users present with significantly more back pain at baseline that persists to at least 2 years following surgery compared to non-opioid users, highlighting the concerning difficulty of discontinuing opioid analgesics in patients who have been using them prior to their intervention. Preoperative opioid consumption may be a potentially modifiable risk factor to promote improved clinical outcomes for ASD surgery. Further studies are needed to determine if individualized preventative approaches and opioid-sparing perioperative management may lead to reduced postoperative opioid utilization and improved clinical outcomes.
Footnotes
Acknowledgements
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international spine deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department.
Authors Contribution
All authors listed contributed sufficiently to the project to be included as authors, and all those who are qualified to be authors are listed in the author byline.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.