
Abstract
Study Design
Systematic review
Objective
The role of limited fusions compared with extensive reconstructions of the spine has not been well defined. The objective of this study is to review the current literature and provide evidence-based recommendations regarding the magnitude of surgery for patients with adult scoliosis, including indications and limitations of short-segment (≤3 levels) fusions.
Methods
A systematic review of the literature was conducted using PubMed/MEDLINE, Cochrane Library, Ovid and Google-Scholar using the following terms: “adult spinal deformity”, “adult scoliosis”, “degenerative scoliosis”, “scoliosis” together with “spinal fusion”, “spinal instrumentation” and “fusion”. Inclusion criteria were comparative studies comprised of thoraco-lumbar or lumbo-sacral adult scoliosis treated with short- or long-segment fusion. Other types of deformities were excluded.
Results
Of the 1736 articles identified from initial query, 9 studies comprised of 660 patients with adult scoliosis who underwent a short-segment fusion (SSF, n = 366) or a long-segment fusion (LSF, n = 294) were included and analyzed for clinical and radiographic outcomes. Summative results indicate that patients undergoing SSF have lower complication rates (.21 vs .36 complications/patient), lower revision rates (9% vs 28%), and though LSF patients had greater scoliotic curvatures and sagittal imbalance at baseline, both groups had significant clinical improvement after surgery. However, the heterogeneous nature of the published data calls into question the reliability of these summative results.
Conclusions
Judicious use of SSF can achieve satisfactory clinical outcomes in carefully-selected patients with adult scoliosis. Factors to consider when selecting patients for SSF include predominant symptoms, patient expectations, comorbidities and spino-pelvic parameters.
Keywords
Introduction
Adult spinal deformity (ASD) continues to be 1 of the most challenging and controversial pathologies for spine surgeons. Structural degenerative changes are hallmark of ASD and account for the majority of symptoms and disability in both well-aligned and malaligned patients. 1 Pain is the most common presenting symptom of ASD with a reported incidence of nearly 90% and first-line treatment usually starts with non-operative interventions.2–4 However, when the desired improvement is not attained or durably maintained, patients tend to seek surgical treatment options.5–7
Determining the optimal surgical management in patients with symptomatic spinal deformity is complex, and appropriate treatment should be individualized and planned according to both clinical and radiologic findings. Although general spino-pelvic targets and surgical goals have been reported in the literature, the number of levels to be fused and the optimal surgical approach for patients with adult scoliosis remains a topic of ongoing debate. Thus, 1 of the first questions spinal surgeons face when contemplating surgery is whether or not to fuse, and if so, how many and which levels should be included in the construct. The purpose of this article is to review the spectrum of surgical management of patients with adult scoliosis and provide guidance for an evidence-based approach based on current literature to determine which patients may benefit from limited fusion and decompression rather than extensive fusion and realignment procedures.
Methods
The authors performed a systematic review of the literature following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (www.prisma-statement.org) to identify reports focused on the magnitude of surgical interventions for patients with thoracolumbar adult scoliosis. A search was conducted in PubMed/MEDLINE, Ovid, Cochrane Library and Google Scholar databases for relevant publications written in English from January 1, 2006 to December 1, 2020, using the following search terms: “adult spinal deformity”, “adult scoliosis”, “degenerative scoliosis”, “scoliosis” together with “spinal fusion”, “spinal instrumentation” and “fusion”. For some queried articles, further assessment of the reference lists as well as the “similar article” and “cited by” features of PubMed were used to screen for other qualifying studies. Titles and abstracts of all the relevant literatures were screened by a single author based on the inclusion and exclusion criteria.
Result of Literature Review on Adult Scoliosis: Review of Articles Included Comparing Short Vs Long-Segment Fusion a .
aASD = adult spinal deformity; LL = lumbar lordosis; CVA = coronal vertical axis; SVA = sagittal vertical axis; ODI = Oswestry Disability Index; FC = fractional curve; PI = pelvic incidence; PT = pelvic tilt; LOHS = length of hospital stay; RMDQ = Roland Morris Disability Questionnaire; VAS = visual analog scale; JOA = Japanese Orthopaedic Association; LSDI = Lumbar Stiffness Disability Index; PSI = Patient Satisfaction Index; COMI = Core Outcomes Measurement Index.
Results
Results of the Literature Review
Initial query produced 1736 articles from the searched databases. After excluding duplicates, 1017 records were screened based on title and abstract and 998 records were discarded due to type of study (biomechanical, experimental, single arm studies, literature reviews or meta-analysis), those not written in English and those that did not address outcomes of patients with adult scoliosis treated with both long- and short-segment fusions. The remaining 19 articles deemed potentially relevant were then subjected to a full-text review and assessed using the inclusion and exclusion criteria defined previously, resulting in exclusion of an additional 10 articles. Finally, 9 studies were included for data extraction and analysis (Table 1).8–16 2 of these were considered of moderate quality with a NOS score of 6 and 7 were considered of high quality with a NOS score ≥7 (Supplemental Table 1). Details of the selection process are shown in Figure 1. Details of the literature search and article selection process.
Patient Population and Surgical Characteristics
Overall, the 9 studies included 660 patients, all with adult scoliosis (coronal Cobb angle ≥10°) who underwent either a short-segment fusion (SSF, n = 366) or a long-segment fusion (LSF, n = 294). The definition for short- and long-segment fusion was variable across studies and in 3 of them the number of levels fused was not clearly specified.9–11 However, none of the SSF patients had a reported arthrodesis of more than 3 segments. The mean number of vertebrae fused was 3.3 in the SSF group and 7.3 in the LSF group based on the data extracted from articles that specifically indicated the number of fusion levels.8,12–16
Most of the procedures for both SSF and LSF were posterior approaches utilizing transpedicular screw fixation, autograft or allograft, and interbody cages. Two studies noted use of anterolateral interbody fusions; however, neither the exact number of patients nor the type of surgery was disclosed.9,13 The study by Transfeldt et al 1110 did not describe the type of procedure in detail and was the only study with no information regarding the use of interbody fusions. All other papers stated whether interbody grafts were used, but only 2 studies discriminated the percentage of cases with cages in each group. Although only 1 study (Wang et al 1116) explicitly mentioned the use of pedicle subtraction osteotomies and Ponte osteotomies when more lordosis was necessary, all of them noted the use of decompressions and bone work to achieve adequate sagittal correction.
Quantitative Results of Studies Comparing Short vs Long-Segment Fusions a .
aODI = Oswestry Disability Index.
Surgical Outcomes and Complications
Across all studies included, the major indications for surgery were low back pain associated with radiculopathy. All but 1 of the studies used at least 1 outcome scale to determine clinical improvement after surgery. 9 Of these 8 papers, only 1 of them, in which the main objective was to compare sagittal alignment changes, did not specify if there were significant differences in pain and disability scores between the SSF and LSF groups. 10 The most common outcome scale used was the Oswestry Disability Index (ODI) which was included in 6 studies and most of them revealed that patients in both groups (SSF and LSF) had statistically significant improvement after surgery.
Complications and Reoperations Associated With Short vs Long-Segment Fusions a .
aASD = Adjacent Segment Disease; PJK = Proximal Junction Kyphosis; PJF = Proximal Junction Failure.
Baseline and Postoperative Spinopelvic Parameters of Studies Comparing Short vs Long-Segment Fusions a .
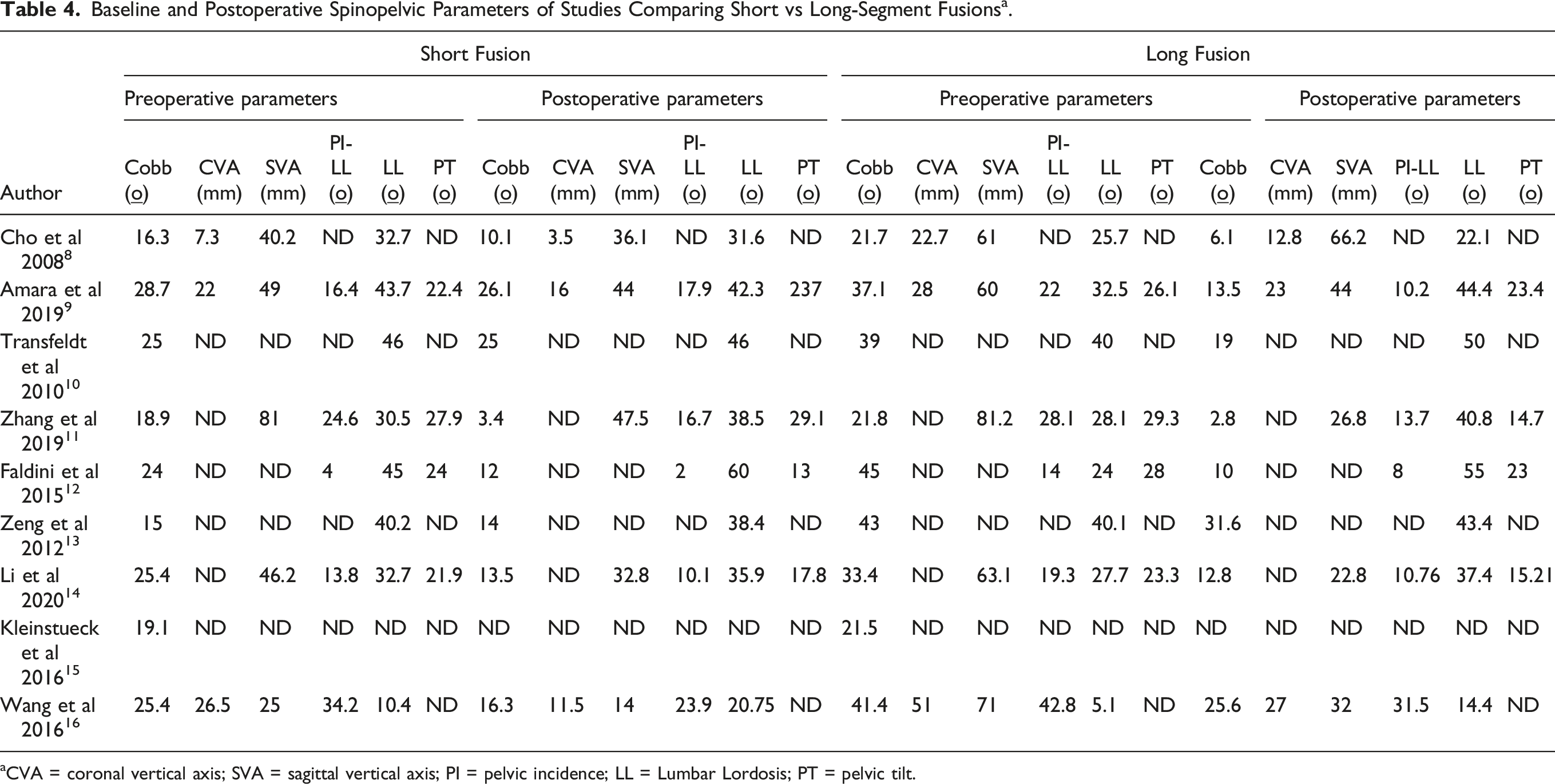
aCVA = coronal vertical axis; SVA = sagittal vertical axis; PI = pelvic incidence; LL = Lumbar Lordosis; PT = pelvic tilt.
Discussion
Objectives and Determinants of Surgery
There is broad agreement on the goals of ASD surgery: improvement of pain, HRQoL outcomes and patient function, low rate of reinterventions, and, most importantly, patient satisfaction. In order to achieve these objectives, the ideal surgery would entail a thorough decompression of neural elements, maintenance or restoration of global alignment, ultimate achievement of solid fusion, with minimal complications and risks.3,4,17 Even though there is a general consensus regarding indications for surgery in patients with adult scoliosis including intractable pain, progressive deformity, spinal instability, loss of function, and neurological deficit, a monolithic approach for optimal management is not well supported by the literature. Consideration of clinical symptoms, structural factors, patient comorbidities, and patient preference should help determine whether a patient is an appropriate candidate for surgery and tailor the extent of the recommended intervention as well.
Although ASD can present with both back and radicular pain, the predominant or most debilitating symptom should be considered in helping to define how much decompression or correction should be planned.18–20 Postacchini proposed that patients with neurogenic claudication and mild LBP could be treated with decompression only, however if axial pain was the predominant symptom or if there was significant deformity a fusion was recommended.21,22 Nevertheless, although decompression alone has been shown to produce symptomatic relief for selected patients with neurogenic claudication and radicular symptoms, there is considerable literature documenting the risk of deformity progression and need for revision surgery due to the potential destabilizing nature of decompressive surgery alone.7,17,22–25 Hence, this type of procedure should be reserved ideally for very select cases in which there is moderate to severe single- or two-level stenosis, highly comorbid patients who may not tolerate more invasive procedures and those with minimal or no global sagittal or coronal malalignment. 26
When determining the magnitude of fusion that will accompany decompressions, we found there was a consistent factor across all 9 articles included in this review: all of them strongly considered patient symptoms in order to define the appropriate surgical intervention. There were only 2 prospective studies and in both, the surgical decision was based on patient symptoms, with those having predominantly radicular symptoms or neurogenic claudication receiving a short-segment fusion and decompression, while patients with predominant low back pain or evidence of progressive deformity were treated with long-segment fusions.13,16 The other 7 studies, though retrospective, also reported a similar tendency in which presence of axial back pain, taken as an indirect reflection of malalignment and deformity, favored larger procedures. This symptom-guided orientation is comparable to that proposed by Lenke-Silva, in which patients with predominantly stenosis symptomatology (Treatment Level II in their study) are considered for more limited interventions, especially if curves are <30° and in the setting of limited or no back pain. 27
Most of the studies revealed that patients in both short- and long-segment fusions groups had statistically significant improvement of symptoms after surgery. In 1 study, patients in the SSF group had significantly better ODI scores at the last follow-up than did patients in the LSF group (P < .005). 16 However, baseline ODI scores were also much higher in the LSF group which could account for the postoperative difference, but no comparison was made regarding the change in ODI between groups. In the study by Transfeldt et al 1110 the LSF group had no significant improvement in their postoperative ODI scores and both SSF and LSF groups had insignificant changes in Roland Morris scores (RM). Nevertheless, there were no reports of spino-pelvic parameters to assess if there was any relation between correction and clinical improvement. Furthermore, patient satisfaction questionnaires revealed that most patients in both SSF and LSF cohorts considered surgery a success and the majority would have the same surgery again.
Evidence Supporting Short-Segment Fusions
Disc collapse, facet hypertrophy with instability and listhesis can produce foraminal stenosis with subsequent compression of the exiting nerve root; specially at the L4-L5 and L5-S1 levels which are the segments of maximum stress and mechanical loading.9,28 Patients with mainly stenotic symptoms at these levels tend to be better candidates for smaller surgical treatments, and a limited decompression with fusion of the affected segment may be sufficient to alleviate pain and improve function, especially if the patient is sagitally aligned. Nonetheless, though the “symptom-based approach” seems to be crucial in determining optimal candidates for short fusions, the degree of desired correction needed to obtain “ideal” spinopelvic parameters should also be taken into consideration. Unfortunately, the heterogeneity of the included studies did not allow for statistically significant coronal or sagittal malalignment cut-off values to define which patients would ultimately benefit from shorter fusions. However, we did observe that the maximum ∆Cobb and ∆LL (baseline – postoperative) across the studies was nearly 15°. Furthermore, in the studies that did report baseline values, we observed a mean Cobb angle <30°, mean coronal vertical axis (CVA) < 30 mm, mean SVA <50 mm and mean PI-LL <35° (Table 4). These values are similar to previous reports in the literature supporting smaller constructs and could serve as the starting point for future matched cohort studies.
None of the studies included in the present review reported significant differences between the SSF and LSF groups with regard to patient comorbidities or overall health. Although this was not an explicit factor in determining the magnitude of surgery, since most of the studies included were retrospective, it is possible that patient health could still have impacted the decision at the point of care. Patient-related variables for risk assessment including age, BMI, cardiopulmonary conditions, smoking and osteoporosis have all been associated with perioperative complications, readmissions and mortality in patients undergoing surgery for adult scoliosis and should be considered prior to any intervention.29–33
Of the 184 complications collectively reported in the included papers, 77 occurred in the SSF population (21% complication rate) and 107 in the LSF group (36% complication rate). All studies reported a tendency for higher complication rates with LSF constructs, and in 3 of them this difference was statistically significant.9,14,15 5 studies reported significantly lower operative times for SSF,8,11,14–16 and all 6 studies that included data regarding blood loss found that SSF was associated with less blood loss.8,9,11,14–16 2 of the 4 studies that reported average length of hospital stay found SSF had a significant shorter stay after surgery.9,11 This is supported by previous studies in the literature in which LSFs have been associated with lengthier operative times and greater blood loss, thus potentially increasing the incidence of morbidity and post-operative complications.34–37 The association of blood loss and hospital stay with complications was also reported in a multicenter study by Schwab et al 3338 in which patients with reported complications had significantly greater blood loss (2.4 vs 1.6 L, P = .004) and longer hospital stay (14.4 vs 7.9 days, P = .001) than patients without complications. Considering that many patients with degenerative spinal disease are elderly and frequently afflicted by comorbidities, limited fusions could present an advantage over larger instrumentations in terms of lower blood loss, shorter hospital stay and fewer complications.
The potential benefits of short-segment decompression and fusion open a window of opportunity for minimally invasive surgery (MIS) which has been studied as an alternative to open interventions. There has been increasing evidence that MIS can be effective for the management of selected patients with ASD.39–41 However, a limitation for MIS procedures remains the amount of correction that can be obtained. To help address the issue of under-correction of sagittal alignment, more recent MIS techniques including release of the anterior longitudinal ligament and use of hyperlordotic or expandable cages have been shown to obtain corrections of up to 17° per level.42–44 Even though some studies comparing MIS and open surgery have shown no significant difference in terms of postoperative SVA between them, the mean correction was significantly greater for the latter group.45,46 Anand and colleagues described the so called “ceiling effect” of MIS surgery and they found these interventions can be used in patients with an SVA of up to 89 mm, a PI-LL missmatch of 38° or less and a Cobb angle of up to 42°. 47 These results suggest that MIS may be a suitable option when patient selection is appropriate and only limited correction in terms of sagittal or coronal alignment is needed, which may be particularly relevant for SSFs.
Revision surgery and progression of scoliosis with SSF continue to be major concerns, especially if fixation stops at or near the scoliosis apex or in patients with adjacent segments that display early signs of degeneration and stenosis. A total of 114 revision surgeries were performed across the 9 studies (in some cases more than 1 per patient), 32 of them in the limited fusion group (revision rate of 8.7%) and mainly due to adjacent segment disease or pseudarthrosis; while patients in the long construct group (revision rate of 27.8%) usually required reinterventions due to proximal junction problems (PJK/PJF) and pseudarthrosis. Interestingly, Amara et al 999 found that even though SSF patients had a higher rate of extension surgery (26% [FC] vs 13% [LT] vs 4% [UT], P = .068), mostly related to progression of deformity and adjacent segment disease, the overall revision rate was similar and the non-extension revision rate was significantly lower than for LSF patients (P < .01).
The incidence of PJK and PJF was considerably higher in the population with longer constructs. Considering that the reported incidence of PJK is as high as 68% with revision rates as high as 55%, the rates of PJK in the present study are consistent with previously published data.9,38,48–50 From a biomechanical stand point, longer fusions are more prone to develop this condition due to more extensive paraspinal muscle dissection, greater curvature corrections, increased posterior spinal ligament disruption, fusions that often extend to sacrum/pelvis and the sudden change in rigidity between instrumented and non-instrumented levels.51,52 Only 1 paper analyzed the impact of constructs on stiffness using the lumbar stiffness disability index (LSDI) and found a mean score of 3.5 ± .5 in the LSF group, which was significantly higher than 1.4 ± .7 in the SSF group (P < .001). 11 This is consistent with findings by Hart and colleagues who found stiffness secondary to long fusions (≥3 levels) has been associated with limitations in daily activities and negative effects over range of motion; oddly enough, small fusions have been reported to produce an improvement in perception of mobility secondary to pain improvement. 53 Hence, smaller fusions may also be considered for active patients in whom their activity levels could be negatively affected by a longer and more rigid construct.
The flexibility of the spine above a fusion is a factor that affects not only deformity progression, but the risk of proximal junction complications as well, hence when thoracolumbar curves show stiffness (eg, bends to less than 30°) SSF may be considered as a viable option. However, even though this value and other factors including bone quality and the presence of kyphosis above the fused levels may qualitatively affect decision making, objective evidence is lacking and warrants further study to inform future recommendations.
In Favor of Long Fusion
There is now good evidence that patient-reported outcome measures correlate with sagittal alignment, thus pursuit of appropriate spino-pelvic parameters is considered 1 of the more important objectives in adult scoliosis surgery.54–59 In particular, PI-LL mismatch, PT, and SVA are among the strongest radiographic predictors that correlate with surgical outcomes, disability and quality of life.54,56,60 Bearing in mind their widely recognized influence, there are concerns regarding short fusions and their limitations for obtaining desired parameter goals. When examining the baseline parameters reported in the papers included in the present study, it is evident that in most of them, patients in the LSF group had significantly greater Cobb angles, PT, PI-LL missmatch and SVA, indicating these patients were substantially more coronally and sagitally malaligned than their SSF counterparts. Since most of the included studies were retrospective, 1 could conclude that the need for spinopelvic restoration likely impacted the extent of fusion, with more malaligned patients treated with more extensive surgeries, causing a selection bias for comparison purposes.
When axial mechanical pain is the main cause of concern for the patient, spinopelvic measures should be carefully assessed to determine if sagittal malalignment is a source of symptoms. Only 2 papers separately assessed improvement of radicular leg pain and low back pain after surgery and in both studies, patients had significant improvement of both leg and back pain after the procedure.14,15 However, Li et al. found greater low back pain relief in the LSF group compared with the SSF population, which may be related to the improvement of spinopelvic parameters since there was a statistically significant difference in PT improvement between both groups. 14 This is consistent with the Lenke-Silva classification in which greater back pain tends to be associated with greater malalignment and favors a more extensive procedure to obtain better global realignment. 27
Four studies reported significant increase between pre and postoperative lumbar lordosis angles in the LSF population,10–12,14 and only 2 observed this change in the SSF patients.11,12 3 papers documented postoperative PT being significantly lower with more extensive fusions,11,12,14 and the 1 paper that compared PI-LL missmatch also favored longer constructs for its correction. 9 These differences between the 2 groups of patients in both preoperative global alignment and the feasible correction that can be obtained with each type of intervention are critical factors when determining whether a patient may be a candidate for a SSF. In a study by Liu et al. 61 LL was shown to significantly increase after long fusion surgeries with no significant change found if only 1 level was decompressed and fused. Other studies have also consistently reported this trend of correction, in which greater improvements in LL, PT, SVA have all been associated with multilevel decompression and fusion.62–64 This is probably why longer fusions have been traditionally used for patients who present with SVA greater than 6 cm, if more than 30° of PI-LL missmatch needs to be corrected or Cobb angles >45° need to be addressed.24,27,65,66 With regard to coronal radiographic changes, we found that across all included studies, longer fusions tended to provide greater corrections in terms of Cobb angle and CVA. Difference was statistically significant in 4 of the studies for the first (P < .05),8–10,13 and in 2 for the latter (P < .03).10,11
Degenerative curves seem to progress more rapidly than their adult idiopathic counterparts.19,27 Furthermore, Cobb angles >30°, lateral subluxation >6 mm and apical rotation greater than Grade II, all often present in this population, are predictors of a more rapid curve progression. 19 This may partly explain why patients treated with SSF tend to have a higher rate of extension surgery and reinterventions due to ASD while longer constructs avoid or at least slow down the progression by stabilizing the deformity. Considering short-segment fusions as the equivalent of Lenke-Silva Level II treatment population, we observed a relatively low adjacent segment stenosis rate compared with what was presented by Cheh and colleagues at the Scoliosis Research Society Annual Meeting in 2006, in which 14 (36%) out of the 39 level II patients developed adjacent segment stenosis after surgery. However, even if our observed ASD rate was low, it accounted for nearly 50% of the reoperation rate in this population and it is a frequently reported complication in the literature. Consequently, we believe patients presenting with major scoliotic curves and significant global malalignment, especially those showing signs of degeneration, stenosis or instability higher in the curve, should be considered for longer constructs in order to better achieve both age-adjusted sagittal alignment goals and help avoid progressive deformity and stenosis. 59
We observed that patients in the LSF cohort presented with greater baseline deformities, and had greater corrections in terms of SVA and postoperative lordosis, all of which have been associated with PJK.67,68 However, proximal junction complications should not necessarily discourage extensive reconstructions for adult scoliosis since these have shown significant improvement in patient-reported outcomes, despite the high complication rates.22,69,70 Furthermore, strategies to help reduce these complications are currently available including age-adjusted parameter corrections and the use of tethers, neither of which were reported in the studies in the present analysis.51,52,59 Also, the key to alignment research lie in the spinopelvic parameters and they were not consistently reported across all papers, which is 1 of the main limitations of our study.
Future Research
One of the main limitations of the present literature review was the lack of matched cohorts in terms of spinopelvic parameters, which precludes true direct comparison of the effectiveness of short-vs long-segment fusions in patients with adult scoliosis and conclusions can only be made regarding efficacy for the specific groups of patients that were ultimately selected for each procedure. Also, there was no consistent mention as to which levels were fused and emphasis was made only on the number of vertebrae included in the constructs. This lack of comparability between patient populations indicates a possible bias in patient selection which hampers objective recommendations. Furthermore, although there is evidence that patients with significant global malalignment would benefit from longer constructs, the cut-off values and parameters to select the intervention are yet to be determined.
Conclusion
Short- and long-segment fusions can achieve satisfactory clinical outcomes in patients with adult scoliosis as long as appropriate criteria, including patient symptoms, comorbidities and spinopelvic parameters, are used to carefully individualize the magnitude of surgery. Short-segment fusions have been shown to have less blood loss, shorter hospital stay and can significantly improve pain and functionality scores, but the amount of correction that can be achieved remains limited. The heterogeneous nature of the published data calls into question the reliability of these summative results, however ideal candidates for SSF may include patients with predominantly radicular or stenotic symptoms who lack significant coronal or sagittal malalignment, but the threshold spinopelvic baseline values are yet to be determined.
Supplemental Material
Supplemental Material - Determining the Magnitude of Surgery in Patients With Adult Scoliosis: A Systematic Review of the Role of Limited Fusions
Supplemental Material for Determining the Magnitude of Surgery in Patients With Adult Scoliosis: A Systematic Review of the Role of Limited Fusions by Juan Pablo Sardi, Bruno Lazaro, Thomas J. Buell, Chun Po Yen, Christopher Shaffrey, Sigurd Berven, and Justin S. Smith in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.
Supplemental Material
Supplemental material for this article is available online