
Abstract
Study Design
In-vitro cadaveric biomechanical study.
Objectives
Long posterior spinal fusion is a standard treatment for adult spinal deformity. However, these rigid constructs are known to alter motion and stress to the adjacent non-instrumented vertebrae, increasing the risk of proximal junctional kyphosis (PJK). This study aimed to biomechanically compare a standard rigid construct vs constructs “topped off” with a semi-rigid construct. By understanding semi-rigid constructs’ effect on motion and overall construct stiffness, surgeons and researchers could better optimize fusion constructs to potentially decrease the risk of PJK and the need for revision surgery.
Methods
Nine human cadaveric spines (T1–T12) underwent non-destructive biomechanical range of motion tests in pure bending or torsion and were instrumented with an all-pedicle-screw (APS) construct from T6–T9. The specimens were sequentially instrumented with semi-rigid constructs at T5: (i) APS plus sublaminar bands; (ii) APS plus supralaminar hooks; (iii) APS plus transverse process hooks; and (iv) APS plus short pedicle screws.
Results
APS plus transverse process hooks had a range of motion (ie, relative angle) for T4-T5 and T5-T6, as well as an overall mechanical stiffness for T1-T12, that was more favourable, as it reduced motion at adjacent levels without a stark increase in stiffness. Moreover, APS plus transverse process hooks had the most linear change for range of motion across the entire T3-T7 range.
Conclusions
Present findings suggest that APS plus transverse process hooks has a favourable biomechanical effect that may reduce PJK for long spinal fusions compared to the other constructs examined.
Keywords
Introduction
Adult spinal deformity (ASD) is characterized by deformity in the sagittal plane (ie, >5 cm imbalance) and/or coronal plane (ie, >10° curve), typically in the thoracolumbar spine.1–3 Spinal deformity has a significant impact on quality of life, with patients scoring lower in all 8 domains of the 36-Item Short Form Health Survey (SF-36) compared to the general population. 2 Although spinal deformity incidence was thought to be 8%–13%, it has recently been documented at a higher frequency and is likely to increase as the population ages.4,5 Surgical intervention is recommended for patients with failed non-operative management, curve progression, or neurologic compromise.4,6
At present, long posterior spinal fusion is a standard surgical treatment for ASD, which generally utilizes an all-pedicle-screw (APS) construct.4,7 This allows for intervertebral segmental stability and substantial correction of the deformity. There are satisfactory patient outcomes with this procedure, such as decreased pain, increased function, and improved health-related quality of life scores.6,8
However, APS constructs create a stiff lever arm that places significant mechanical stress at the junction between the instrumented fusion and adjacent non-instrumented spine.9,10 This can lead to proximal junctional kyphosis (PJK), which has a recognized incidence of 6%–69%.11–13 PJK occurs when the vertebrae immediately cephalad to the instrumented segment collapses into a kyphotic deformity with a sagittal Cobb angle ≥10° compared to pre-operative measurements. 11 PJK can have substantial clinical implications, such as proximal junctional failure, leading to vertebral body fracture, subluxation, pain, neurologic deficits, and the need for revision surgery. 9
An alternative surgical approach is to “top off” the standard rigid APS construct with a semi-rigid construct at the vertebral level above the fusion (Upper Instrumented Vertebrae +1 [UIV+1]). This aims to create a more gradual change in motion and decrease mechanical stress between the fusion construct and the non-instrumented spine. Finite element analyses have suggested that this gradual change in motion may decrease stress at the posterior ligamentous complex and nucleus pulposus, depending on the semi-rigid construct utilized. 14 To this end, prior biomechanical studies using mechanical tests and/or computational models have examined various semi-rigid constructs with different amounts of success, such as tethers,15–17 laminar hooks,15,18 sublaminar bands,15,19,20 and transverse process hooks,21–23 but not short pedicle screws. However, few studies have investigated a head-to-head comparison of the commonly cited constructs. Furthermore, vastly different protocols across studies make comparison between constructs challenging. Thus, there is still no consensus in the literature on the optimal semi-rigid construct.
The goal of this biomechanical study was to compare a standard rigid APS construct against 4 different commonly used semi-rigid constructs in human cadaveric thoracic spines. It is hypothesized that a difference in stiffness would be achieved when using semi-rigid constructs, indicating one group may be superior in avoiding PJK and that the metallic constructs would lead to less movement compared to the soft material counterparts. Furthermore, based on previous clinical and biomechanical data, it is expected that transverse process hooks and sublaminar bands will provide the most gradual transition in motion.
Methods
Specimen Preparation
Institutional approval was granted for using nine human cadaveric spines of known sex (7 male, 2 female) and age (average, 63.9 years; range, 33-78 years). CT scanning, medical history review, and visual inspection were completed to rule out bone tumors, fractures, or internal bony abnormalities. The thoracic section (T1-T12) was removed and stored in a −20°C freezer. Specimens were thawed for at least 24 h prior to surgical preparation and biomechanical testing. Musculature was dissected while retaining the facet capsules, posterior ligamentous complex, and costovertebral joints. The most cranial (T1) and caudal (T12) vertebrae had drywall screws inserted to improve potting in cement, so endplates were oriented horizontally.
Instrumentation
Based on a literature review
24
and experience at the authors’ institution, the following constructs were selected and instrumented in a randomized order following a step-up/step-down ladder sequence in each of the nine spines (Figure 1). All nine spines were instrumented with pedicle screws (CD Horizon Legacy Spinal System, Medtronic Canada, Mississauga, Canada) from T6–T9 to create a multi-level instrumented fusion, which represented the all-pedicle-screw (APS) construct. The pedicle screws were inserted free hand using standard anatomical landmarks to reference the starting points.
25
The screw track was examined for breaches by rotating a pedicle probe in a stepwise progression around 360°. The depth of the track was then measured and appropriate screw lengths were chosen, ranging from 35-45 mm. None of the screws breached the anterior cortex, but the longest screw possible was chosen. Finally, a pair of 5.5-mm diameter titanium rods were attached to the screws. Spines were then sequentially instrumented with various semi-rigid constructs at T5. Semi-rigid constructs for long spinal fusion. (A) APS + SB, (B) APS + SH, (C) APS + TH, (D) APS + SS. APS: all-pedicle-screw, SB: sublaminar bands, SH: supralaminar hooks, TH: transverse process hook, SS: short pedicle screws.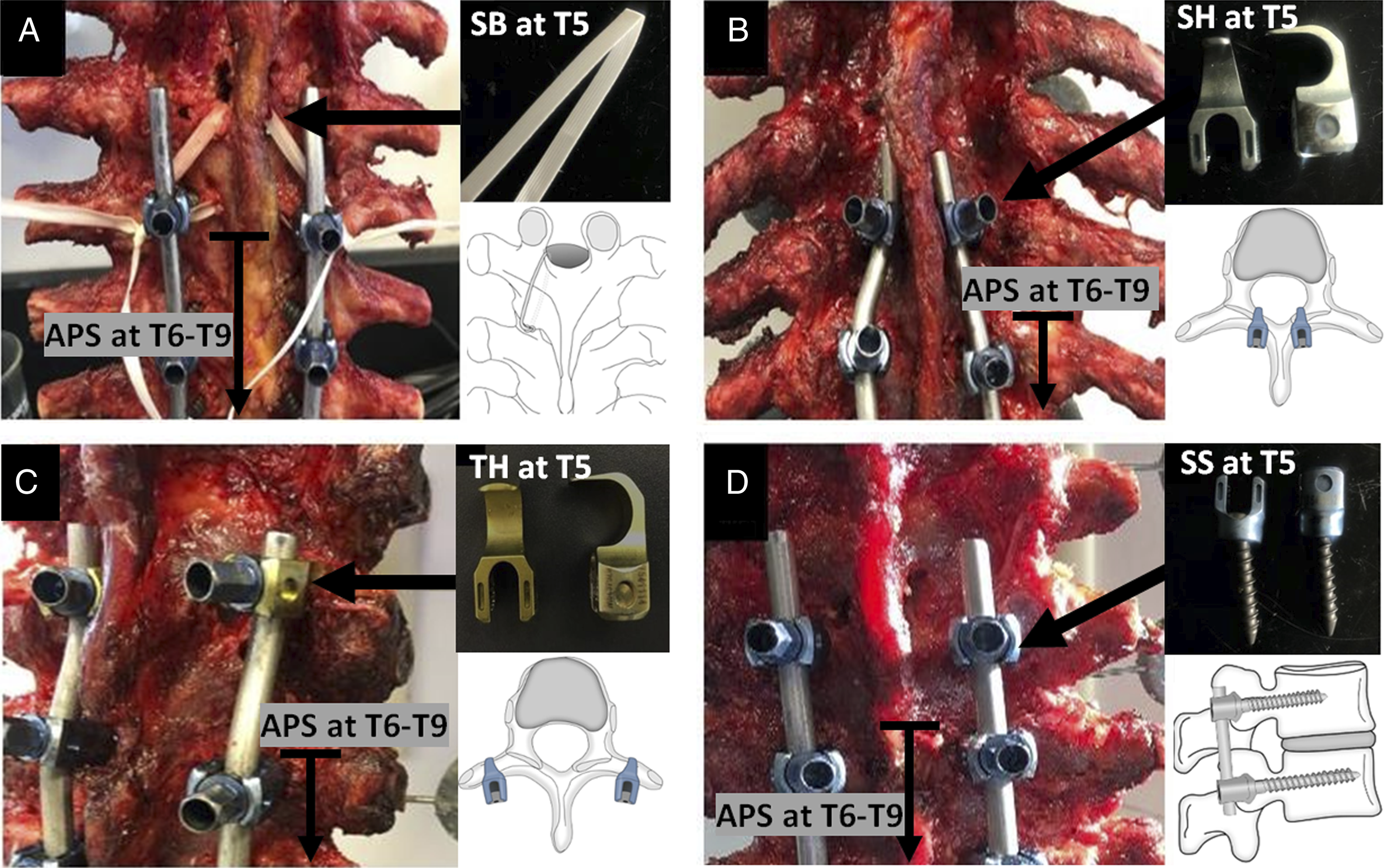
The APS + SB construct included sublaminar bands (SB) at T5. A 5-mm wide Mersilene® tape (Ethicon, Sommerville, NJ, USA) was used.16,17,20 A hemilaminectomy was performed on the superior lamina with a Kerrison bone punch. A suture needle attached to the band was passed under the T5 lamina and retrieved at the cranial edge. The needle was cut off, and the band was looped around the titanium rods. Two square knots were thrown, followed by 3 half-hitches with the final on an alternating post.
The APS + SH construct included supralaminar hooks (SH) at T5 (CD Horizon Legacy Spinal System, Medtronic Canada, Mississauga, Canada). A hemi-laminectomy of the superior lamina was performed using a Kerrison bone punch. The ligamentum flavum was removed from the cranial edge of the T5 lamina. Hooks were then placed over the cranial edge of the lamina bilaterally and attached to the rods.
The APS + TH construct included transverse process hooks (TH) at T5 (CD Horizon Legacy Spinal System, Medtronic Canada, Mississauga, Canada). A scalpel was used to reveal the edge of the transverse process and create space between the transverse process and the rib head. The hooks were then placed at the midpoint on the transverse process bilaterally and attached to the rods.
The APS + SS construct included short pedicle legacy screws (SS) at T5. The screws were placed using the same sequence described for the APS fixation. However, T5 screws were 25 mm in length. The rods were then attached to the screws.
Biomechanical Testing
Established protocols were used as guidelines for all experiments.26,27 Intact spines (ie, no implants) were tested to establish baseline data, followed by instrumented spines. Specimens were equipped with 3-dimensional motion markers, mounted onto a mechanical tester (Instron® 5967, Norwood, MA, USA), and attached to a computer-controlled custom-made spine testing apparatus (Figure 2). After applying a 10-N axial pre-load, three cycles of pure moment (+/− 5 Nm, 1°/s) were applied to generate forward-backward (ie, flexion-extension) bending, left-right (ie, lateral) bending, or clockwise-anticlockwise (ie, axial) torsion. The first two cycles were for pre-conditioning, while the last cycle was for data analysis. During loading, a dual-camera digital image correlation system (ARAMIS Adjustable 12M, GOM Metrology, Braunschweig, Germany) recorded the 3-dimensional motion of markers at 3 images/s to determine inter-vertebral motion. The cameras had a focal length of 24 mm, a 3000 × 4096 pixels viewing window, and a pixel size of 3.45 μm. Images were processed with dedicated computer software (ARAMIS Professional 2019, GOM Metrology, Braunschweig, Germany). Spine testing setup for applying loads and recording motions. Red arrows indicate pure moments applied to the cranial end of the spine to generate bending and torsion. Black arrows denote motions on the bearing table for the caudal end of the spine. Key: 2D, two-dimensional; 3D, three-dimensional; DOF, degree of freedom.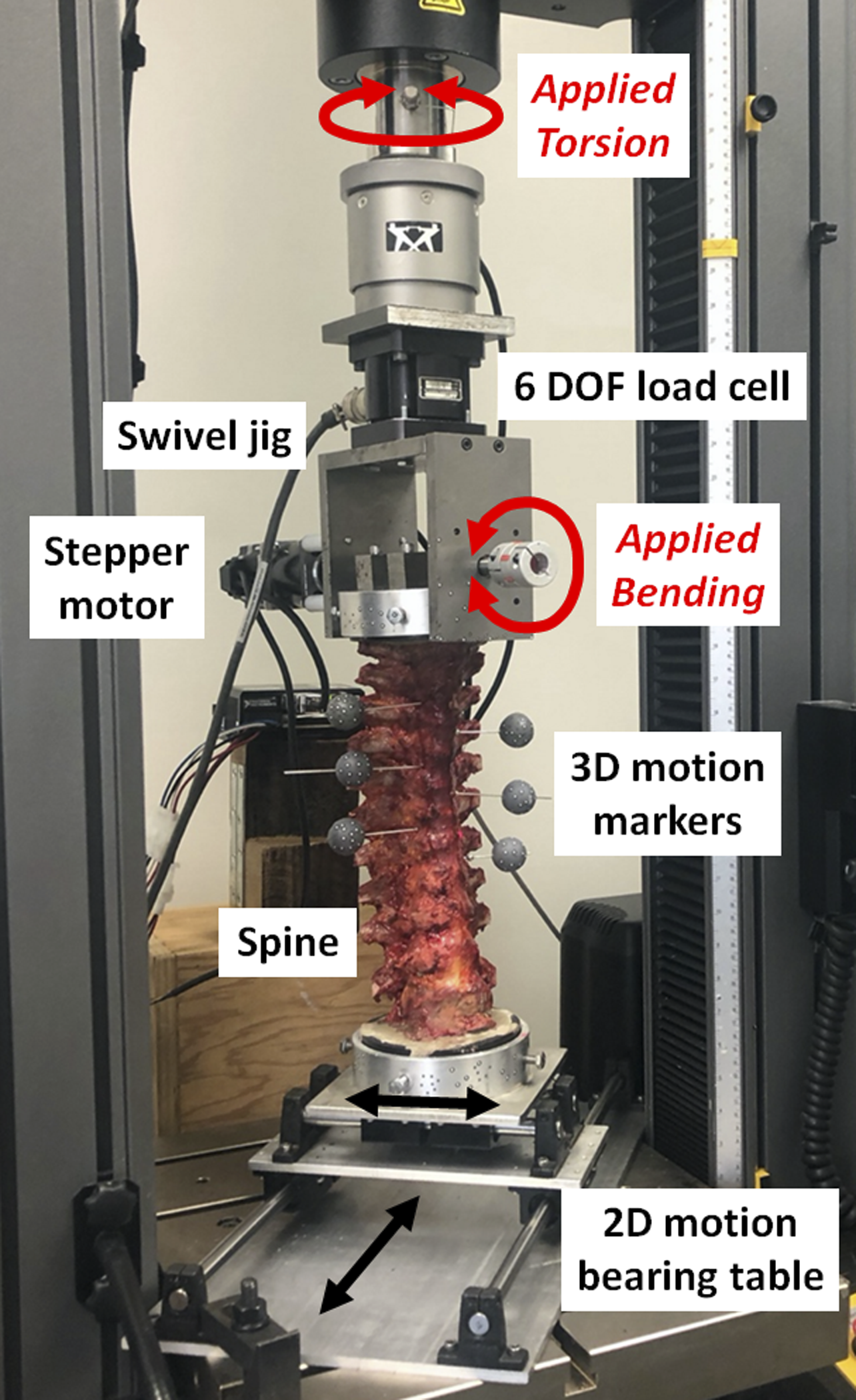
Statistical Analysis
Normalized range of motion (ROM) (ie, relative angle) for each vertebra was computed as the total angular motion of the 3-dimensional motion markers observed by the DIC system compared to the intact state.


Results
Normalized ROM
Relative movements between adjacent vertebrae are reported as percentages of intact spine values (Figure 3). All loading modes showed similar results. First, all constructs started with smaller ROM at T6-T7, but this increased during the T4-T6 “transition zone” either suddenly (ie, APS and APS + SB) or progressively (ie, APS + TH, APS + SS, and APS + SH) until ROM reached the intact value at T3-T4. Second, there was no statistical difference in ROM between any constructs at T6-T7 (P = .074 to .999) (ie, fully inside the APS fusion) or T3-T4 (P > .999) (ie, fully outside any implant fusion). Next, there was no statistical difference (P > .97) in ROM between APS and APS + SB at any vertebral level. At T5–T6 (ie, the junctional level between the rigid APS construct and the semi-rigid constructs), APS + TH had lower ROM vs APS and APS + SB (P < .001) and equivalent ROM in torsion to APS + SS and APS + SH (P > .149), while APS + SS and APS + SH had lower ROM vs APS and APS + SB in all directions and APS + TH (flexion-extension and lateral bending) (P < .028). Finally, at T4-T5, APS + SH had lower ROM vs all other constructs (P < .004). Finally, there was no statistical difference (P > .33) in ROM between any constructs at T7-T8 or T8-T9, although this is not shown graphically. Normalized ROM for relative motion between adjacent vertebrae. (A) Flexion-extension, (B) lateral bending, (C) torsion. Average values are connected by straight lines. Average coefficients of variation (1 standard deviation/average x 100%) are 132% (graph A), 47% (graph B), and 32% (graph C), but they are not shown to avoid graph clutter. Key: *, statistical difference (P < .05) at T5-T6 for APS + TH vs APS and APS + SB; #, statistical difference (P < .05) at T5-T6 for APS + SS and APS + SH vs APS, APS + SB, and APS + TH; £, statistical difference (P < .05) at T4-T5 for APS + SH vs all other constructs. All other comparisons were statistically equivalent (P ≥ .05).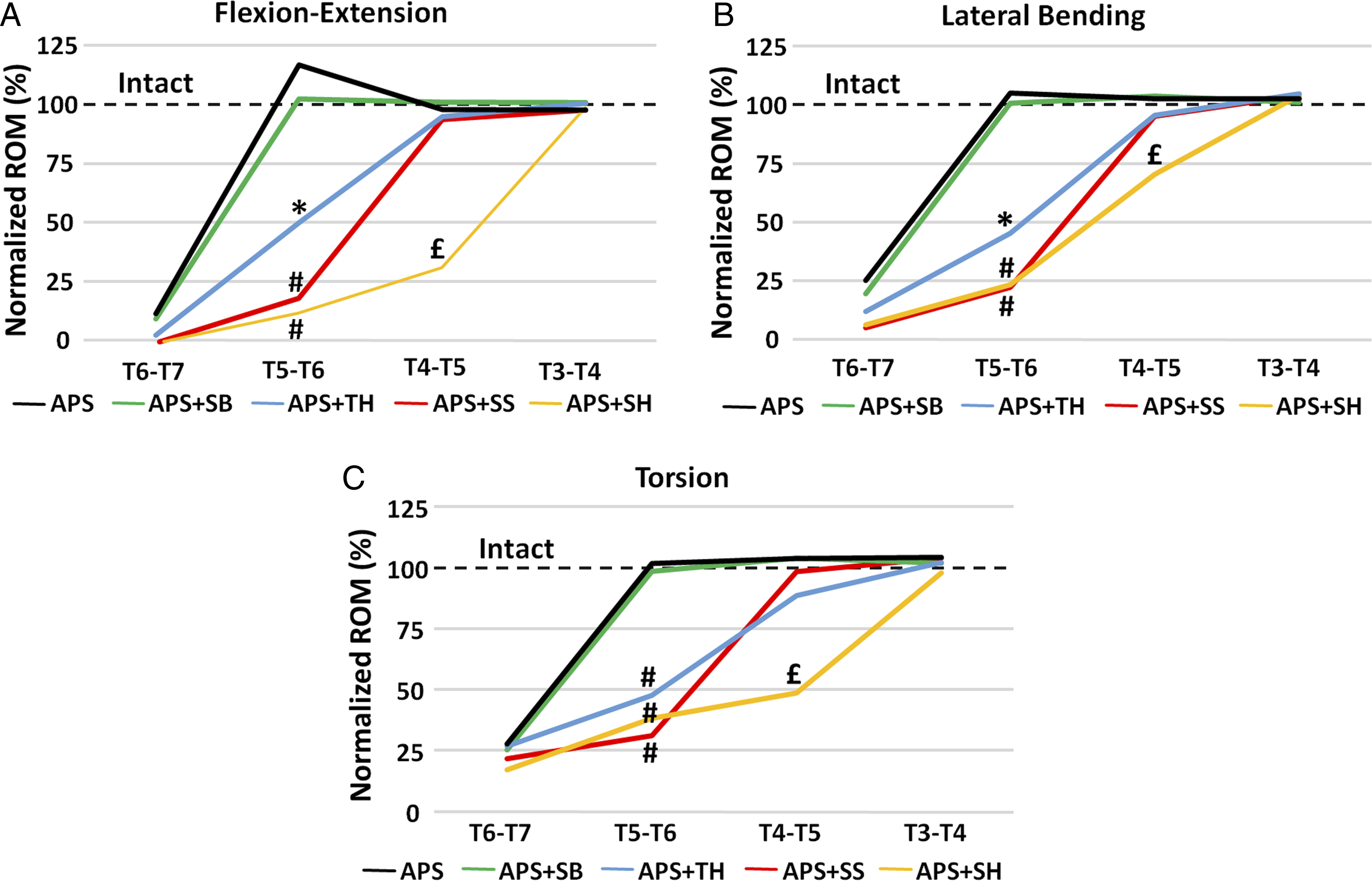
Normalized K
Stiffness for T1-T12 constructs are reported as percentages of intact spine values (Figure 4). All loading modes showed the identical order as the normalized stiffness rose from its lowest value for intact spines followed by progressively increasing normalized stiffness for APS, APS + SB, APS + TH, APS + SS, and then APS + SH. However, there were variations between loading modes as to which group comparisons were statistically equivalent. Specifically, intact spines had statistically equivalent normalized stiffness (P Normalized stiffness (K) for the entire spine T1-T12. (A) Flexion-extension, (B) lateral bending, (C) torsion. Blue bars are average values, while error bars show 95% confidence intervals. Bars sharing at least one symbol (*, #, £) indicate statistical equivalence for comparisons between groups (P ≥ .05). All other comparisons between groups were statistically different (P < .05).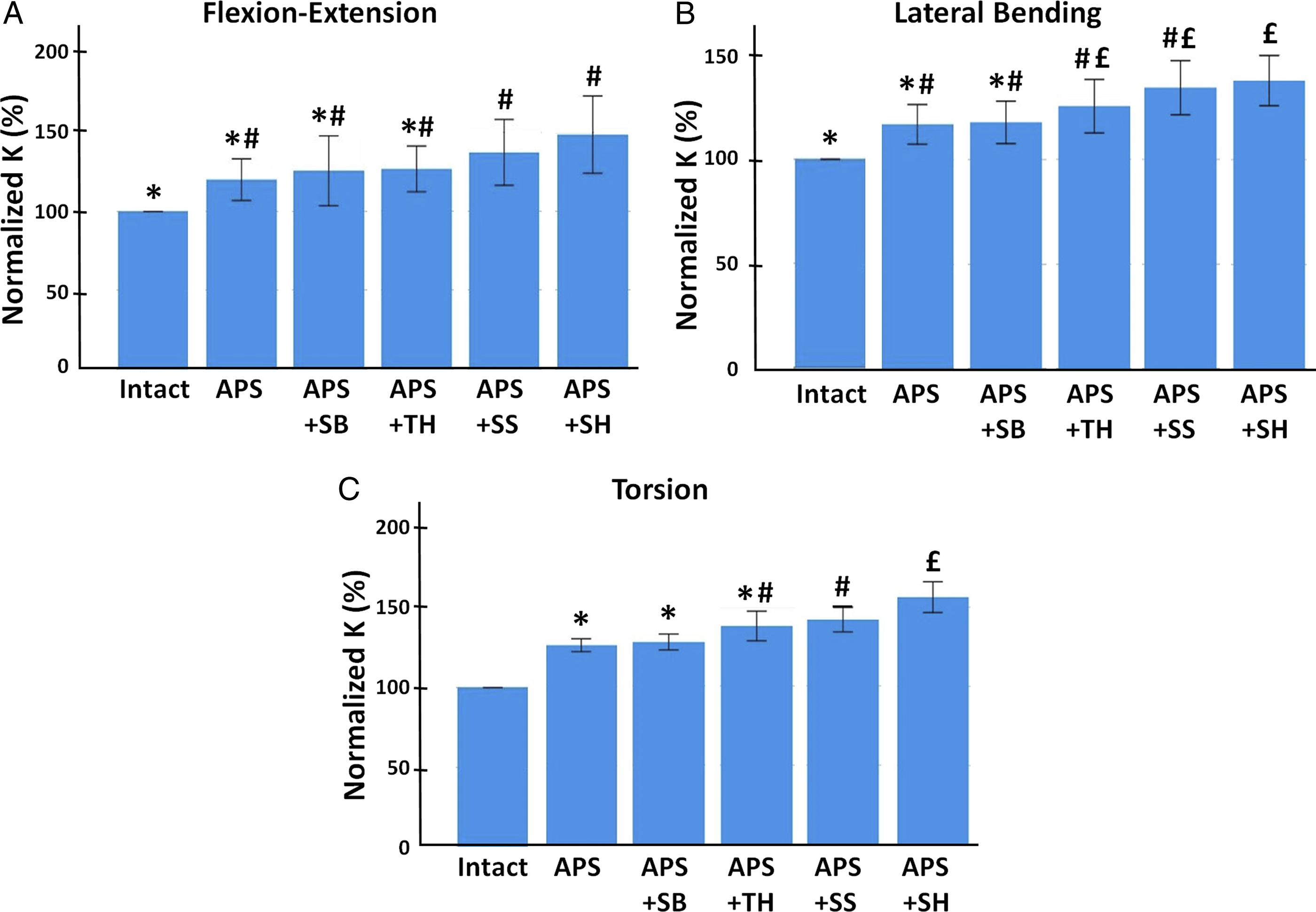
Neutral Zone
There were no significant differences observed in flexion-extension (P > .83) or lateral bending (P > .25) when measuring the neutral zone (Figure 5). In torsion, the neutral zone was significantly greater (P < .008) in the intact state as compared to APS + TH and APS + SH, but no other significant differences were found (P > .2). The ratio of the neutral zone to the total range of motion. (A) Flexion-extension, (B) lateral bending, (C) torsion. Blue bars are average values, while error bars show 95% confidence intervals. Bars sharing at least one symbol (*, #) indicate statistical equivalence for comparisons between groups (P ≥ .05). All other comparisons between groups were statistically different (P < .05).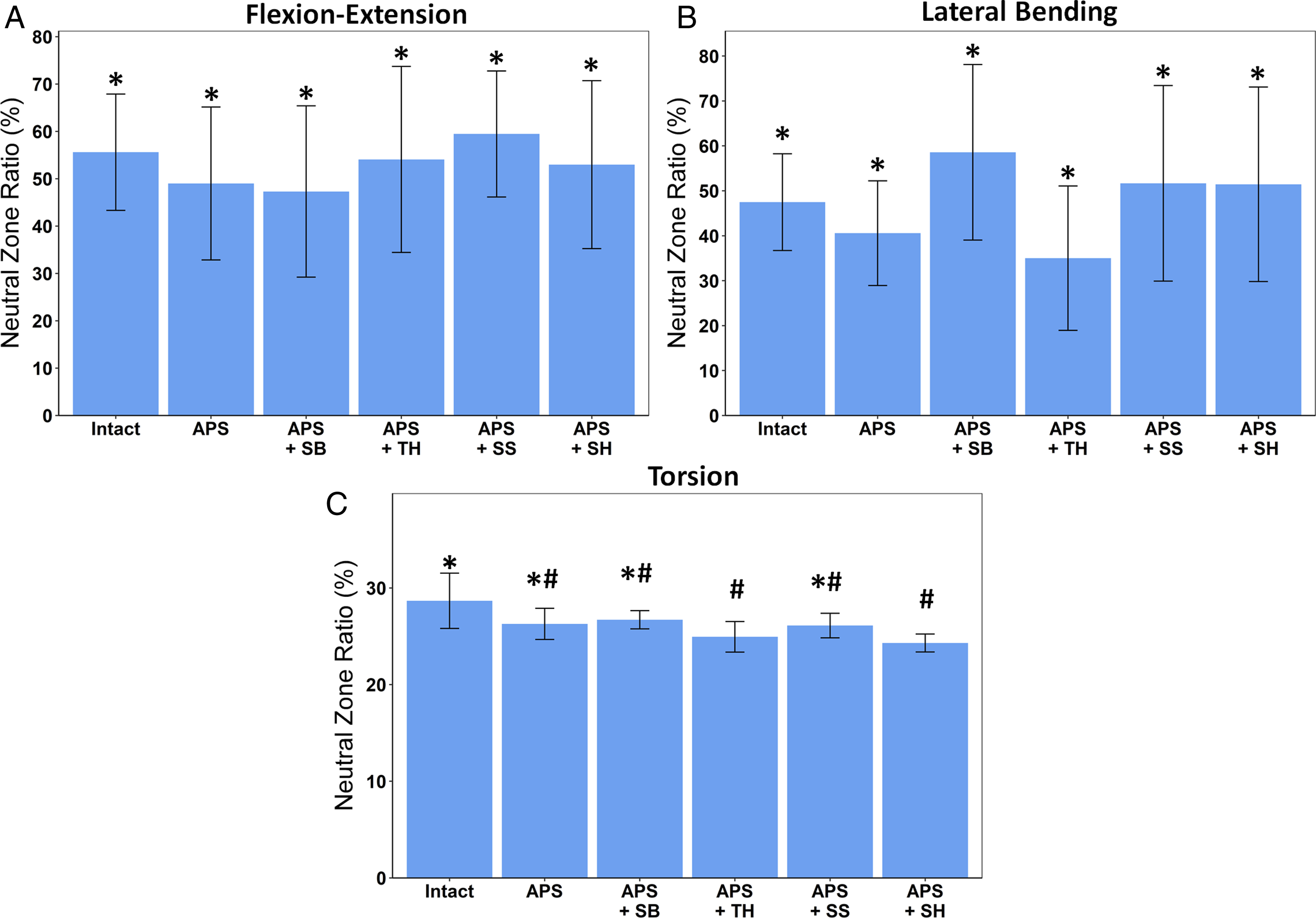
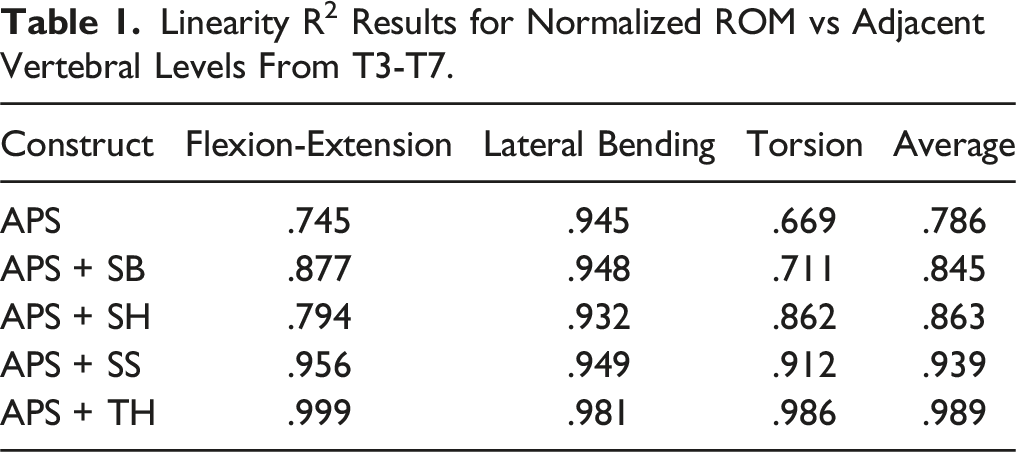
Linearity R2
Linearity R2 Results for Normalized ROM vs Adjacent Vertebral Levels From T3-T7.
Discussion
General Findings
The present investigation examined the biomechanical performance of various semi-rigid constructs to identify which construct(s) could effectively decrease the risk of PJK. In particular, a standard, rigid APS construct was compared with a fusion augmented with widely used semi-rigid constructs, such as SB, SH, TH, and SS. The findings showed that the APS + TH construct had a normalized ROM and a normalized stiffness that were between the extreme data of the other groups. Also, APS + TH had the most linear change in normalized ROM across T3-T7, which included the “transition zone” of T4-T6. From a biomechanical viewpoint, this suggests that APS + TH could be the most appropriate construct among those assessed to reduce stress at the transitional zone, and may help reduce the risk of PJK in a long posterior spinal fusion.
Basic Physics
A consideration of basic physics may help explain some of the present apparent trends for the stiffness results, even though the statistical analysis was not sensitive enough to detect all the differences (Figure 4). The intact spine group had the lowest stiffness as no instrumentation was placed. APS and APS + SB had a higher stiffness as the instrumentation limited motion across all fixated segments, creating a longer lever arm compared to the native spine. Limited difference was seen in stiffness between APS and APS + SB as the bands were made of a low-stiffness, non-metallic material with low tension applied. Next, APS + TH had a higher stiffness since the hooks extended the lever arm as compared to APS and APS + SB. This is likely due to both the material of the hooks and the stability in their application. Next, the APS + SS construct was even stiffer, as the screws likely provided more anchorage into the bone itself as compared to hooks overtop of the lamina. Lastly, APS + SH had the highest stiffness as its motion was reduced up until UIV+3, resulting in the longest lever arm of the constructs tested. Similar comments could be made about ROM data, which is discussed further below.
Substantial data variability was seen in the neutral zone between specimens potentially caused by the majority of the spine being fused, with the remaining segments having little free motion, and secondly, to the nature of the thoracic spine without ribs and variability between cadaveric soft tissues. Additionally, the ratio of the neutral zone to the total range of motion was high in the intact state and across all constructs. This could be due to the testing conditions, as the specimens were tested to 5 Nm, not to a maximum load to failure. As the ratio is dependent on how much load is applied, we would expect the ratio to be smaller if the specimens were tested at higher loads.
Comparison to Prior Work
The application of transverse process hooks (APS + TH) reduced motion at T4-T5 and T5-T6 compared to the APS construct (Figure 3), and was shown to have the most linear change in motion across T3-T7 among all constructs (Table 1); which is consistent with findings for transverse process hooks from previous studies.19,21,23 This also supports clinical evidence from several studies that showed decreased rates of PJK when using constructs with transverse process hooks at the UIV+1 compared to APS alone. It is suggested that the more limited dissection required for these hooks may contribute to increased stability at adjacent levels, as compared to pedicle screws.10,31 Additionally, computational studies have found transverse process hooks decrease forces at the posterior ligamentous complex and nucleus pulposus in comparison to APS constructs, which may provide further rationale for the decreased rates of PJK seen with transverse process hooks. 14
Next, as the bands were hand-tied in the APS + SB construct, there may not have been sufficient tension produced; leading to no statistical difference from the APS construct (Figures 3 and 4). This is supported by a previous study that used cadaveric functional spine units to study spinous process tether pretension, whereby the amount of tension significantly affected motion. 16 In contrast, some other studies used industrial clamps or custom-made tensioning devices to secure bands, which could result in higher band tension and reduced motion.19,22,32 Although commercial tensiometers are readily available and easy to use, we elected to rely on the surgeon’s judgment as to how tight the band should be made. This was done to best replicate a realistic intraoperative scenario since the commercially available tensiometers are not medical devices. Thus, the variability seen across these studies may also occur clinically, which may lead to inconsistent results with SB.
The APS + SH construct showed significant decreases in ROM at T5-6 and T4-5 (Figure 3, Table 1), which has been shown previously in the literature.22,33 However, this study demonstrated a large increase in motion at T3-4, or UIV+3, whereas other studies only measured motion up to two levels above the fusion construct (UIV+2). 33 This is important as others may not have captured a sudden increase in motion at UIV+3, as was seen here. These results were even more pronounced in the current study when flexion and extension were isolated and analyzed. For example, in extension, APS + SH reduced the motion by 75% (ie, 25% of the original intact spine motion) at T4–T5 but climbed by 5% compared to the intact spine motion at T3–T4. This raises the question if APS + SH simply shifts the abrupt change seen with APS to a higher level, rather than gradually changing across levels. Furthermore, APS + SH had the highest stiffness of all constructs (Figure 4). It has been suggested that the supralaminar hooks may come into contact with the superior lamina, and block motion at adjacent levels, thereby generating significant stiffness and rigidity. 22
Lastly, limited biomechanical research exists on semi-rigid constructs in the upper thoracic spine, despite PJK occurring there. 34 In particular, only one other study selected the uppermost implanted vertebrae and the adjacent vertebra between T1-T6. 35 Also, no previous report utilized short pedicle screws as a semi-rigid construct; but, a prior study investigated the effect of leaving pedicle screws at the uppermost instrumented vertebrae not fully seated, which led to a more gradual change in motion vs fully seated screws. 36 Thus, further research could be considered with this construct.
Surgical Aspects
From a technical standpoint, the number of individual hardware components and manual tasks involved may quantify the challenges in performing a spine fusion procedure. Defined in this way, the present spine fusion constructs could be ranked in order of ascending technical difficulty as APS alone, followed by APS + SS, then equally by APS + SH or APS + TH, and finally by APS + SB. Therefore, APS + SS would be the most preferred among the semi-rigid constructs themselves, while APS + SB is the least preferred. Moreover, surgical treatments that are more technically difficult may potentially also result in poor outcomes, such as increased soft tissue stripping, blood loss, longer operating time, and more postoperative complications. It could also reflect a higher chance of secondary surgery, slower patient recovery time, and higher financial burden to the health care system. However, these observations must be systematically evaluated for the current spine fusion constructs in a future laboratory or clinical study.
From a clinical standpoint, mechanical postoperative complications, such as PJK, may be modifiable with improved surgical equipment or technique; thus, it is critical to investigate possible means to improve them. Research on the use of semi-rigid constructs and their effect on motion and construct stiffness helps further understand how to best optimize fusion constructs to decrease the risk of PJK. Ultimately, by decreasing the risk of PJK, there may be a decrease in post-operative pain experienced by patients and the need for revision surgery; therefore, the morbidity and financial costs associated with this complication may be reduced.
Potential Drawbacks
There were limitations to this study typical of biomechanics research. First, the use of a cadaver model, in comparison to an animal model, does not account for the dynamic nature of spinal movement and muscular contributions. Given that movement is a dynamic process, range of motion testing in an isolated plane does not truly simulate physiologic conditions. To our knowledge, motion simulators that can produce a more realistic motion pattern are not available and the methods utilized in this study are in keeping with other modern publications. Next, in this study, the paraspinal muscles were removed to facilitate instrumentation and testing, but these muscles may help provide stability and reduce the risk of PJK. 37 However, the entire thoracic spine was used, with the costovertebral joints left intact, which likely helps replicate physiology. 38
A hemilaminectomy was performed during the instrumentation of SB and SH which could potentially impact the stability and ROM in the test cycles following. Repetitive testing may also disrupt the posterior ligamentous complex and compromise its protective role against PJK.39,40 To help minimize these effects on construct outcomes, the order of instrumentation and testing varied using a “step ladder” algorithm. As testing was limited to nine specimens, the number of semi-rigid constructs was also limited to help lessen the impact of instrumentation and repetitive testing. For example, posterior tethers were not selected as a semi-rigid construct, despite being used in previous studies since their placement disrupts the posterior ligamentous complex and would likely affect the results of constructs tested after their use.39,40
Next, T3 or T4 is typically selected for semi-rigid instrumentation in a clinical setting, whereas the present study used T5. This was done to ensure ROM could be measured at least 2 levels above and that there was sufficient room for the most proximal vertebra to be potted in cement. Prior biomechanical studies suggest upper thoracic segments (ie, T1-T6) have similar kinematics; thus, the results of the current study are likely applicable to instrumentation across these segments. 41 In contrast, the results of this study should not be translated to scenarios in which the UIV is located in the lower thoracic spine as biomechanics may differ. Lastly, stresses on the vertebrae or discs were not directly measured at the “transition zone” from T4-T6; however, ROM and stiffness are commonly-used parameters from which stress states can be inferred.
Conclusions
This biomechanical study compared a multi-level fusion construct “topped off” with various semi-rigid constructs to determine which could decrease ROM at adjacent levels and potentially reduce the risk of PJK. The APS + TH construct was found to have a most favourable ROM and stiffness, as it reduced motion at adjacent levels without a stark increase in stiffness, as compared to the other constructs tested. Moreover, APS + TH had the most linear change in ROM across T3-T7 that included the T4-T6 “transition zone”. Thus, our biomechanical findings suggest that using APS + TH may be advantageous in a long posterior spinal fusion, to help reduce the risk of PJK. Further clinical studies are necessary to verify that these biomechanical findings can be translated to long-term clinical outcomes and a reduction of PJK.
Supplemental Material
Supplemental Material - Topping-Off a Long Thoracic Stabilization With Semi-Rigid Constructs May Have Favorable Biomechanical Effects to Prevent Proximal Junctional Kyphosis: A Biomechanical Comparison
Supplemental Material for Topping-Off a Long Thoracic Stabilization With Semi-Rigid Constructs May Have Favorable Biomechanical Effects to Prevent Proximal Junctional Kyphosis: A Biomechanical Comparison by Chloe Cadieux, Pawel Brzozowski, Renan J. R. Fernandes, Martine E. McGregor, Radovan Zdero,, Christopher S. Bailey, Stewart D. McLachlin, and Parham Rasoulinejad
Footnotes
Author Contributions
CC was involved in study design, data collection, analysis, and manuscript writing and editing. PB was involved in data collection, data analysis, and manuscript editing. RJRF was involved in study design, data analysis review, and manuscript editing. MM was involved in data collection, data analysis, and manuscript editing. RZ was involved in study design, data analysis review, and manuscript writing. CSB was involved in data analysis review and manuscript editing. SM was involved in data analysis review and manuscript editing. PR was involved in study design, data analysis review, and manuscript editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data availability statement
The corresponding author can provide original data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.