
Abstract
Study Design
Randomised controlled trial.
Objective
This study aimed to determine the effectiveness of a preoperative bowel preparation protocol comprising bisacodyl to minimize postoperative gastrointestinal morbidities and the hospital length of stay for patients with adolescent idiopathic scoliosis.
Summary of Background Data
Patients who undergo scoliosis correction surgery frequently experience postoperative gastrointestinal morbidities and a prolonged hospital length of stay. Emesis, paralytic ileus and constipation are the most common gastrointestinal morbidities. Opioid medication is a well-known risk factor for gastrointestinal complications after scoliosis correction surgery.
Methods
Eighty-seven patients (22 boys [25.3%] and 65 girls [74.7%]) with a mean age of 17.7 years (standard deviation [SD], ±2.2 years) diagnosed with adolescent idiopathic scoliosis were enrolled in this study and randomized into 2 groups. Group A comprised 44 patients who received a preoperative bowel preparation comprising bisacodyl. Group B comprised 43 patients who did not receive any preoperative medication. Demographic data, height, weight, medical and surgical comorbidities, Risser status, number of instrumented levels and preoperative opioid consumption of all patients were evaluated.
Results
Group A experienced fewer postoperative abdominal symptoms than group B. The mean hospital length of stay was 4.1 days (SD, ±.6 days; median, 4 days; range, 3-5 days) for group A; however, it was 5.3 days (SD, ±.8 days; median, 5 days; range, 4-7 days) for group B (P = .01).
Conclusion
The use of a bowel preparation protocol before scoliosis correction surgery for patients with adolescent idiopathic scoliosis can effectively decrease postoperative gastrointestinal morbidities and the hospital length of stay.
Keywords
Introduction
The Scoliosis Research Society reported that the overall rate of surgical complications among 11 227 patients with adolescent idiopathic scoliosis is 6.3 %. 1 Gastrointestinal complications (paralytic ileus or constipation) are common among these patients. 2 Harris et al. reported that 31% of the patients who underwent surgery for idiopathic scoliosis returned to the emergency department after hospital discharge because of constipation. 3 Patients who undergo scoliosis correction surgery experience more postoperative gastrointestinal morbidities and a prolonged hospital (LOS) than those who undergo elective degenerative lumbar spine surgeries. Gruskay et al. reported a mean hospital LOS of 3.6 days (standard deviation [SD], ±1.8 days) among 103 patients who underwent open 1-3 levels posterior lumbar fusion. 4 Additionally, Lavelle et al. reported that the mean LOS among patients with adolescent idiopathic scoliosis was 4.9 days (SD, ±2.1 days). 5
Emesis, paralytic ileus and constipation are the most common gastrointestinal morbidities. The use of opioid medication is a well-known risk factor for gastrointestinal complications after scoliosis correction surgery.6,7
This study aimed to determine the effectiveness of a preoperative bowel preparation protocol comprising bisacodyl to minimize postoperative gastrointestinal morbidities and the hospital LOS of patients with adolescent idiopathic scoliosis.
Methods
Institutional review board (IRB) approval was obtained before performing this prospective randomised control trial of 87 consecutive patients who underwent scoliosis correction surgery between July 2021 and July 2022. All surgeries were performed by a senior spine surgeon, and the same surgical technique was used for all patients. All pedicle screws, 2 cobalt-chrome rods and allograft bone grafts were used for all patients. The inclusion criteria were age 12-21 years and adolescent idiopathic scoliosis. Patients with medical and surgical comorbidities, congenital deformities or spinal cord anomalies were excluded. Informed consent was obtained from the parents or legal guardians of all patients enrolled in this study.
There were 22 boys (25.3%) and 65 girls (74.7%) with a mean age of 17.7 years (SD, ±2.2 years). The patients were randomized into 2 groups: Group A included 44 patients, and group B included 43 patients. Patients in group A received a preoperative bowel preparation comprising bisacodyl. They were asked to use the recommended dose of bisacodyl (10 mg) at 5:00 PM 1 day prior to the surgery date. Patients in group B did not receive any preoperative medication.
The Comparative Data Between Groups A and B.
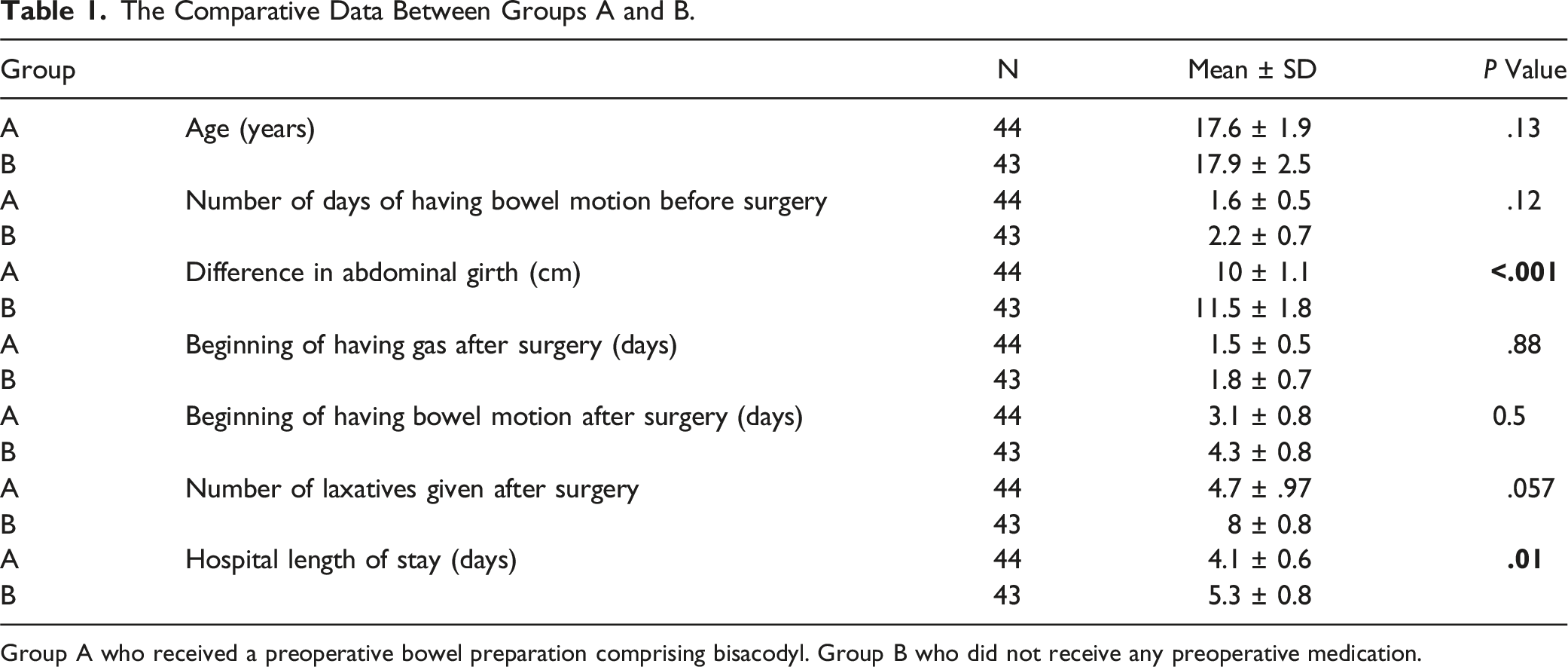
Group A who received a preoperative bowel preparation comprising bisacodyl. Group B who did not receive any preoperative medication.
An enhanced postoperative care recovery plan was implemented for all patients. Patients-controlled analgesia with hydromorphone was administered postoperatively as a 15-µg bolus every 6 min to a maximum of 150 µg/h, Ketorolac .3 mg/kg every 8 h and Paracetamol 15 mg/kg every 6 h.
On the first postoperative day, the patients were transitioned from Patients-controlled analgesia with hydromorphone to an extended-release morphine dose of 10 mg administered orally every 8 to 12 h and an extended-release Hydromorphone dose of 3 mg administered every 8 to 12 h. Medications were administered until discharge. Additionally, ketorolac was discontinued, and ibuprofen (10 mg/kg orally every 6 h) was initiated.
All patients underwent physical therapy on the first postoperative day. Physical therapy consists of walking, bed exercises, dynamic and static sitting exercises, and standing balance exercises. The functional ability was assessed by evaluating the patients’ ability to roll from right to left and from left to right, transition from the prone position to the sitting position, transition from sitting to standing, and mobilize from both a bed and a chair.
All patients received a standardized diet postoperatively. The data collected included, the hospital LOS, need for postoperative gastrointestinal medications and date of the last bowel movement before surgery. Daily clinical examination were performed by experienced staff nurses to assess abdominal tenderness or rigidity, bowel sounds in the 4 quadrants and date of the last bowel motion. Additionally, abdominal girth at the umbilical level was measured preoperatively and on the first postoperative day. SPSS version 23 (IBM, Chicago, IL, USA) was used for data analysis. The level of significance was set at P value <.05.
Result
Eighty-seven consecutive patients were enrolled in this study over the course of 1 year. All patients diagnosed with adolescent idiopathic scoliosis. The patients who received the bowel preparation experienced less abdominal distension and, received few doses of laxatives postoperatively. The mean hospital LOS of group A was 4.1 days (SD, ±.6 days; median, 4 days; range, 3-5 days;); however, the mean hospital LOS of group B was 5.3 days (SD, ±.8 days; median, 5 days; range, 4-7 days) (P = .01).
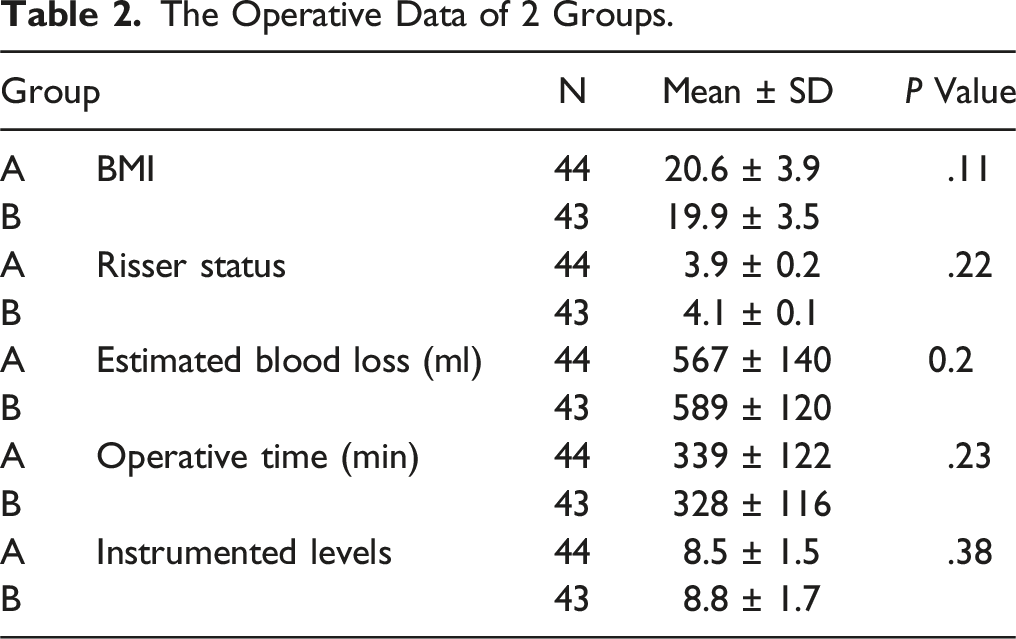
The Operative Data of 2 Groups.
The majority of patients had Lenke type 1 curves (61 % in group A and 67 % in group B). Lenke type 2 curves were observed in 22 % and 13 % of patients in group A and B, respectively. The curve magnitudes were 54 ± 10 and 53 ± 9 for patients in group A and B, respectively. (P value >.05). The flexibility rates were 44 ± 18 and 48 ± 19 for patients in group A and B, respectively. (P value >.05). The cumulative patient-controlled analgesia with hydromorphone doses within 24 hours were .12 ± .02 mg/kg and .13 ± .03 mg/kg for patients in groups A and B, respectively (P value >.05).
Discussion
This study highlights the effectiveness of a bowel preparation protocol to decrease possible gastrointestinal morbidities in patients with adolescent idiopathic scoliosis after scoliosis correction surgery. Fewer laxatives were administered postoperatively to patients who received bowel preparation than to those who did not; however, this finding was not statistically significant (P = .057). Patients in group A had significantly lower abdominal girth than those in group B. Moreover, the hospital LOS was significantly longer for patients in group B than for those in group A (P value <.05).
Fincher et al. observed similar results when comparing 2 different bowel preparation protocols comprising bisacodyl and hypertonic enemas. Furthermore, Bini et al. and Sharma et al. reported that oral sodium phosphate with bisacodyl had superior quality and was more cost-effective than enemas for bowel preparation before colonoscopy.8-10 The availability of bisacodyl in an oral form increased patient compliance with this protocol.
Crawford et al. reported that 77.9% of paediatric patients who underwent a scoliosis correction surgery developed gastrointestinal morbidities. Emesis (50.6%), paralytic ileus (42.3%) and constipation (22.5%) were the most common gastrointestinal morbidities. 3 Medical comorbidities, surgical procedures, and prolonged use of opioids were risk factors associated with gastrointestinal morbidities and a significantly long hospital LOS. 11
Several postoperative protocols, including multimodal non-narcotic pain protocols, epidural pain catheters, and early postoperative ambulation, have been implemented to minimize these risks. 12 Smith et al. observed a modest reduction in bowel morbidities among patients who received bowel preparation before scoliosis correction surgery; however, this reduction had a non-statistically significant effect on the hospital LOS. 13
The cost of hospitalization comprises approximately 19% of the total treatment cost, with a mean cost per day of $8825. 14 Missios et al. reported that mean and median costs of hospitalization for patients who undergo spine surgery were $21,928 (95% confidence interval $21,868–$21,988) and $14,202 (interquartile range $4772–$23,632), respectively. 15 The use of a regular preoperative bowel preparation protocol before scoliosis correction surgery for patients with adolescents idiopathic scoliosis might decrease postoperative gastrointestinal comorbidities, and subsequently decreasing the hospital LOS and total cost of treatment.
This study represents the largest investigation of the effectiveness of preoperative bowel preparation for patients with adolescent idiopathic scoliosis. The hospital LOS was shorter for patients who received the preoperative bowel preparation than for those who did not. Moreover, patients who received the preoperative bowel preparation experienced less abdominal distention and required few laxatives postoperatively.
Supplemental Material
Supplemental Material - Effectiveness of a Preoperative Bowel Preparation Protocol for Patients With Adolescent Idiopathic Scoliosis to Decrease Postoperative Gastrointestinal Morbidities and the Hospital Length of Stay
Supplemental Material for Effectiveness of a Preoperative Bowel Preparation Protocol for Patients With Adolescent Idiopathic Scoliosis to Decrease Postoperative Gastrointestinal Morbidities and the Hospital Length of Stay by Alzakri Abdulmajeed in Global Spine Journal
Footnotes
Acknowledgments
The authors thank the nursing staff for their support during this study.
Author contributions
Conceptualization: Abdulmajeed Alzakri; Formal analysis: Abdulmajeed Alzakri; Writing-original draft preparation: Abdulmajeed Alzakri; Approval of final version of manuscript: Abdulmajeed Alzakri; Agreement to be accountable for all aspects of the work: Abdulmajeed Alzakri.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.