
Abstract
Pulmonary embolism is a significant complication of surgery. This report presents a case of suspected fatal postoperative acute pulmonary embolism following posterior correction surgery in a 16-year-old female with idiopathic scoliosis. The patient presented with a suspected pulmonary embolism 2 h postoperatively. She lost consciousness quickly, and cardiac respiratory arrest occurred. Cardiopulmonary resuscitation was started immediately. The patient was stabilized but underwent a further suspected pulmonary embolism the following day. Cardiopulmonary resuscitation was performed again, but she lost consciousness and respirator support was required. At 40 days after surgery, a computed tomography scan revealed an area of necrotic brain tissue near the lateral cerebral ventricle. The patient remained in a comatose state for 16 months, after which active management was withdrawn. This case reminds us to be alert to potentially fatal postoperative pulmonary embolism in young patients without any risk factors for thrombosis.
Keywords
Introduction
Pulmonary embolism (PE) is a frequently reported, dangerous complication in patients undergoing surgical procedures.1,2 The risk factors for thromboembolic disease vary between patients and according to the type of surgery. 3 Knee and hip arthroplasty have been associated with a high incidence of deep venous thrombosis (DVT) and PE,4,5 and studies of these surgeries form the basis for a series of thrombosis prevention guidelines and recommendations for knee and hip surgery. 4 The risk of DVT was found to be 42–57% following total hip arthroplasty, and 41–85% following total knee arthroplasty. 5 The corresponding risks of pulmonary embolism were 0.9–28% and 1.5–10%, respectively. 5 In spinal surgery, the risk of DVT with PE ranges between 0.048% and 3.14%,6–14 but the incidence of PE alone remains unknown. 15 The incidence of PE may vary according to the type of spinal surgery: 2.4% of patients undergoing deformity correction experienced symptomatic PE compared with 0.65% of patients undergoing posterior spinal surgery. 14
This report presents a case of suspected severe acute PE occurring 2 h after posterior spinal correction surgery in a 16-year-old female with idiopathic scoliosis.
Case report
A 16-year-old female with adolescent idiopathic scoliosis underwent posterior scoliosis correction surgery at the Department of Orthopaedics, Chaoyang Hospital, China Capital Medical University, Beijing, China on 27 January 2010. The patient weighed 34 kg and was 161 cm tall. A preoperative X-radiograph revealed a Lenke type II main thoracic curve of 63° (Figure 1). Routine preoperative examination findings, including blood tests, chest X-radiograph and echocardiography, were unremarkable. Surgery took place under routine general anaesthesia, and no haemostatic drugs were used. A wake-up test was performed during the surgery and the patient was able to move her toes normally. Posterior spinal instrumentation was applied from T2 to L1 with pedicle screws.
Preoperative chest X-radiograph of a 16-year-old female with idiopathic scoliosis, revealing a Lenke type II main thoracic curve of 63°.
Surgery was uneventful and was completed in 210 min. Perioperative blood loss was 800 ml; 250 ml of salvaged red blood cells were transfused but packed red blood cells were not used. Preoperative haemoglobin and haematocrit were 121 g/l and 35.2%, respectively, compared with postoperative values of 76 g/l and 22.6%. The patient was hypovolaemic and received 2000 ml of fluids via intravenous infusion (1000 ml saline and 1000 ml colloidal liquid). The patient was sent to the surgical intensive care unit, conscious, with a blood pressure of 105/43 mmHg and a heart rate of 106 beats/min.
At 2 h after the operation, the patient suddenly experienced chest pain with dyspnoeic respiration. Her blood pressure dropped rapidly to 53/38 mmHg, oxygen saturation decreased to 74%, pulmonary second sound increased and she lost consciousness. At this time blood pressure and heart rate could not be recorded. External cardiac massage was initiated immediately, the patient was intubated and adrenaline and dopamine were administered. The circulation was unstable during resuscitation, and oxygen saturation fluctuated between 70% and 90%. An emergency bedside chest X-radiograph showed a widened heart shadow and no pulmonary vessel markings could be detected on the lower parts of both lungs (Figure 2). Ultrasonography examination showed right ventricular enlargement, tricuspid regurgitation, increased estimated pulmonary artery pressure and widened jugular vein diameter. Electrocardiogram revealed incomplete right bundle branch block, and D Emergency bedside chest X-radiograph of a 16-year-old female 2 h after surgical correction of idiopathic scoliosis, and immediately after onset of suspected pulmonary embolism. The pulmonary vessel marking is not visible on the lower parts of both pulmonary lobes.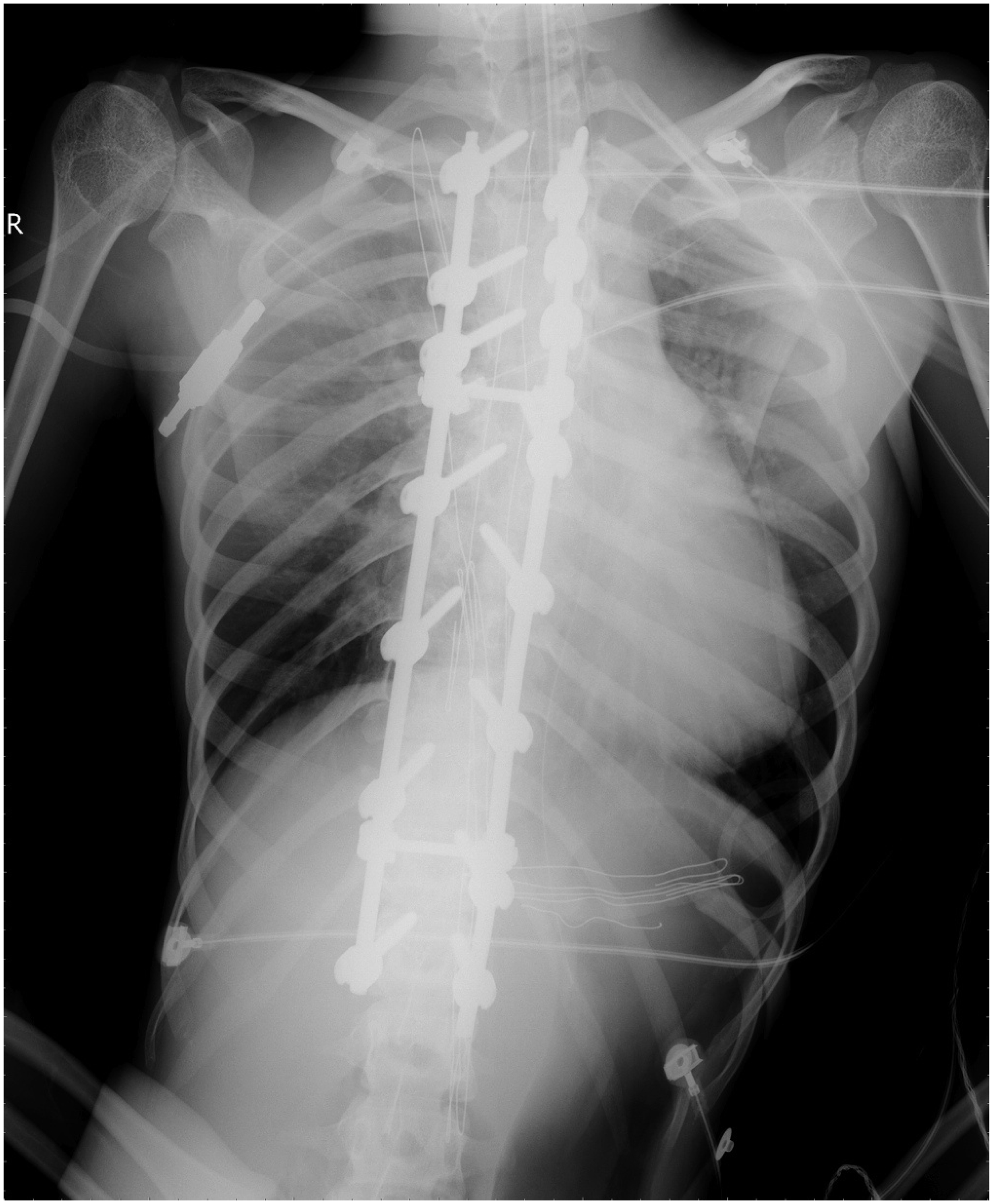
The next morning, approximately 16 h after surgery, the patient became agitated and exhibited tachypnoea, reduced blood pressure and reduced oxygen saturation. Her heart stopped 5 min later, and external cardiac massage was initiated. Emergency bedside chest X-radiograph showed that pulmonary vessel markings had disappeared on the upper part of the left lung and were absent from the lower parts of both lungs (Figure 3). Multiple doses of resuscitation medications including epinephrine, atropine and tissue plasminogen activator were administered intravenously to achieve thrombolysis, which was completed in 1 h. Intermittent episodes of ventricular fibrillation occurred during resuscitation that were treated with four applications of biphasic defibrillation. Cardiopulmonary resuscitation lasted 26 min, following which an independent heartbeat was restored and maintained with continuous intravenous epinephrine and atropine. The patient’s circulation was stable 4 days later, but she remained unconscious. Chest X-radiographs revealed pulmonary vessel markings in the areas from which they had disappeared (Figure 4), and epinephrine and atropine were discontinued. Echocardiographic examination showed that the right heart volume and pulmonary artery pressure had returned to normal. A computed tomography (CT) scan performed 40 days later showed brain tissue necrosis near the lateral cerebral ventricle. The patient remained in a comatose state for 16 months, after which active management was withdrawn. The patient died on 30 July 2011.
Emergency bedside chest X-radiograph of a 16-year-old female after surgical correction of idiopathic scoliosis, 16 h after onset of suspected pulmonary embolism. The pulmonary vessel marking is not visible on the upper part of the left lung. Emergency bedside chest X-radiograph of a 16-year-old female 4 days after surgical correction of idiopathic scoliosis with suspected postoperative pulmonary embolism. The pulmonary marking is visible on the parts of the lung that lacked vessel markings after surgery.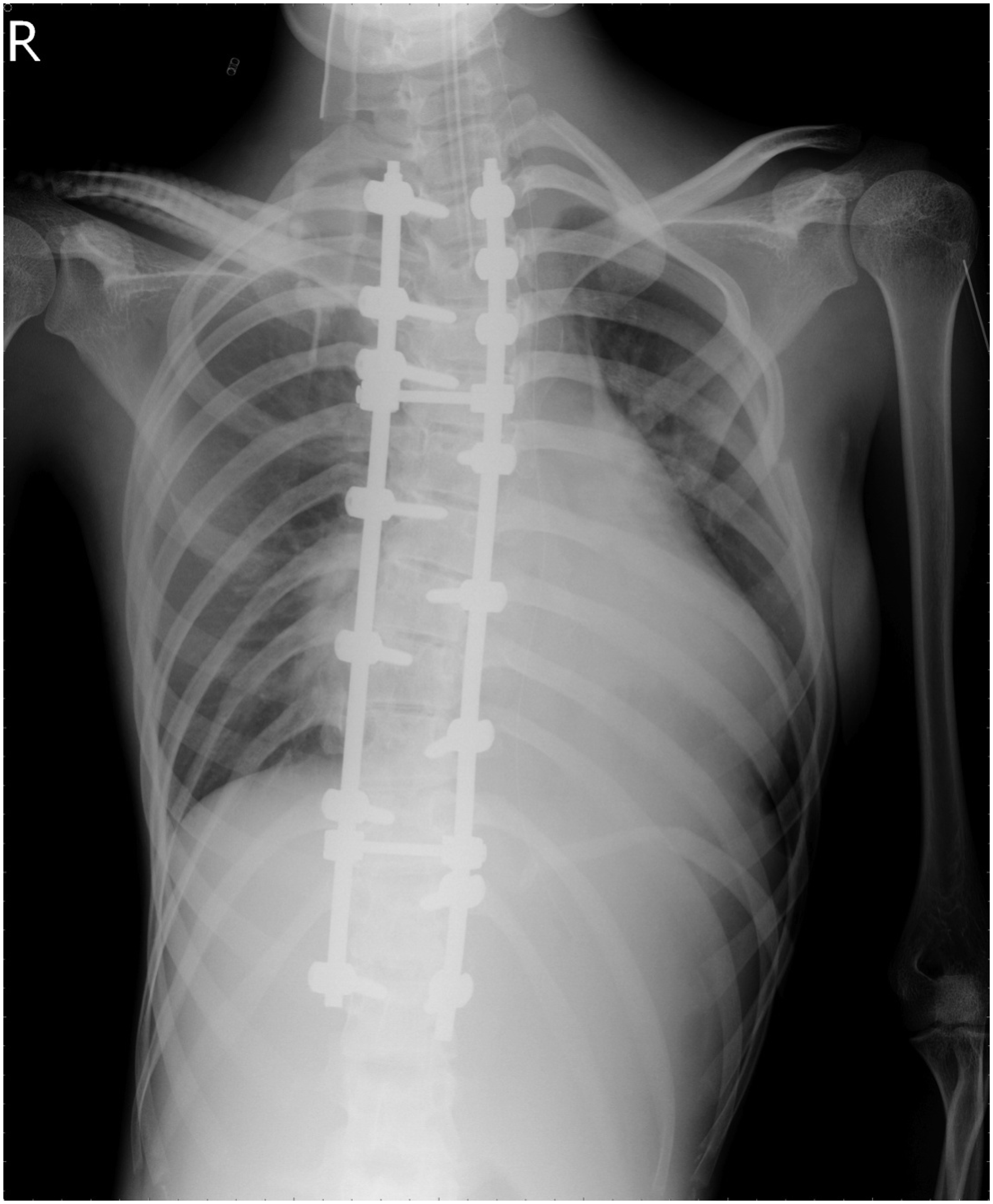

Discussion
The diagnosis of postoperative PE can be challenging as it depends on a pulmonary ventilation perfusion scan, pulmonary spiral CT, magnetic resonance imaging and pulmonary arteriography, of which pulmonary arteriography is the gold standard. 16 Diagnosis can also be confirmed by the presence of a thrombus echo in the right chambers of the heart or pulmonary echo on echocardiography. 16 The diagnostic value of many tests is limited, including clinical symptoms, chest X-radiography, electrocardiography, arterial blood gas analysis and D-dimer analysis. 16 This complicates PE diagnosis in critically ill postoperative patients, in whom the lack of emergency management can have serious consequences.
Preoperative pulmonary angiography and other diagnostic examinations were not performed in the current case, but the patient had no underlying diseases. The acute postoperative clinical symptoms and rapid deterioration suggested acute PE, however. In addition, supportive evidence of PE was present, including a loud pulmonary artery second heart sound, the disappearance of pulmonary vessel markings on the lower parts of both lungs on X-radiography, the disappearance of the right upper pulmonary vascular marking after the second deterioration the following morning, findings from arterial blood gas analysis and D-dimer concentration. In addition, echocardiography showed signs of right heart dilatation and pulmonary hypertension, and the electrocardiogram showed incomplete right bundle branch block. Taken together, these signs and symptoms supported the diagnosis of PE. With anticoagulant and thrombolytic therapy, circulation was stabilized, lung vascular markings could be observed on the chest radiograph and pulmonary artery pressure decreased to normal, confirming the diagnosis of PE.
Thromboembolic events are among the most frequent serious complications following major orthopaedic surgery, and the most common cause of death in the United States. 3 Approximately 500000 cases of DVT and PE were reported each year in the United States in the 2000s. 17 Even with optimal therapy, the mortality rate remains considerable, at 8.6% after 3 months. 18 PE is the initial clinical manifestation of venous thromboembolism in about 20% of cases. 19
Postoperative PE following idiopathic scoliosis correction surgery is a rare occurrence. In a study including 1229 patients, eight exhibited DVT (0.65%), one of which was a fatal case of massive PE. 20 A study including 110 patients who underwent posterior spinal surgery found no cases of postoperative DVT or PE. 21 A further report of 313 patients with spine disease revealed a single case of clinically symptomatic postoperative DVT and none of PE. 22
It has been shown that PE occurs more commonly in anterior than in posterior spinal surgery.6,14,23 In a group of adult patients with thoracolumbar spinal deformity, Dearborn et al 6 found an overall PE rate of 2.2%, but patients who underwent anterior spinal surgery had a much higher incidence than those that underwent posterior spinal surgery alone. A further study found that the rate of PE was 0.65% following posterior spinal surgery compared with 2.4% following anterior spinal surgery. 14 This difference may be due to the retraction and manipulation of major vascular structures during anterior spinal surgery. 14
The proven risk factors for thrombosis include smoking, hormone replacement therapy, previous thromboembolism, neoplasm, diabetes, steroid use and inherited coagulation disorders. 24 Noted risk factors for DVT development in patients who undergo spinal surgery are lengthy operative procedures, prolonged postoperative bed rest, manipulation of the great vessels during anterior approaches, and the use of frames that may compress the femoral venous system.9,20,21,23–25 These patients may have additional risk factors for venous thromboembolism, including advanced age, cervical versus lumbar surgery, anterior surgical approach, surgery for malignancy, and reduced preoperative and postoperative ambulation. 26 The patient described in the current report had none of the above risk factors. In addition, her preoperative activity was not restricted and she climbed stairs every day in preparation for surgery.
There are multiple hereditary abnormal clotting disorders, such as resistance to activated protein C, or deficiency of protein C, protein S or antithrombin III, which could lead to abnormal perioperative clot formation. 27 Postoperative examination of the current patient’s blood revealed no such congenital risk factors, however. To date, we cannot explain the cause of the suspected PE. After reviewing the treatment process, it is possible that the PE may have been related to the serious reduction in blood volume in this patient. Perioperative blood loss was 800 ml, only 250 ml of salvaged red blood cells were infused, and the patient weighed only 34 kg. A review of the literature found no previous reports of low blood volume being associated with PE, however.
Most patients (70%) with postoperative PE die within 1 h of symptom onset,28–30 underlining the importance of active treatment measures. However, treatment is complicated by the fact that thrombolytic therapy is contraindicated in the first 14 days after surgery and may lead to major bleeding and death. The patient in the present report showed symptoms of PE only 2 h after surgery, and gastrointestinal bleeding occurred during resuscitation. Thrombolytic therapy would probably have resulted in fatal bleeding in this case, and anticoagulation therapy was administered under close monitoring. It is possible that the use of an interventional catheter to break up the embolus or the use of suction to remove part of the thrombus could have improved the patient’s haemodynamic status, and the second fatal PE may not have occurred. However, these procedures were not available in our hospital.
In conclusion, we present a case of suspected acute PE following posterior spinal surgery in a 16-year-old female with adolescent idiopathic scoliosis and no risk factors for thrombosis. Careful evaluation of this rare complication may provide an underlying aetiology for unexplained cases of sudden death after scoliosis correction surgery. This case reminds us to be alert to potentially fatal postoperative PE that may occur in young patients without any risk factors for thrombosis formation.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.