
Abstract
Study Design:
Meta-analysis.
Objective:
To compare outcomes between minimally invasive scoliosis surgery (MISS) and traditional posterior instrumentation and fusion in the correction of adolescent idiopathic scoliosis (AIS).
Methods:
A literature search was performed using MEDLINE, PubMed, EMBASE, Google scholar and Cochrane databases, including studies reporting outcomes for both MISS and open correction of AIS. Study details, demographics, and outcomes, including curve correction, estimated blood loss (EBL), operative time, postoperative pain, length of stay (LOS), and complications, were collected and analyzed.
Results:
A total of 4 studies met the selection criteria and were included in the analysis, totaling 107 patients (42 MIS and 65 open) with a mean age of 16 years. Overall there was no difference in curve correction between MISS (73.2%) and open (76.7%) cohorts. EBL was significantly lower in the MISS (271 ml) compared to the open (527 ml) group, but operative time was significantly longer (380 min for MISS versus 302 min for open). There were no significant differences between the approaches in pain, LOS, complications, or reoperations.
Conclusion:
MISS was associated with less blood loss but longer operative times compared to traditional open fusion for AIS. There was no difference in curve correction, postoperative pain, LOS, or complications/reoperations. While MISS has emerged as a feasible option for the surgical management of AIS, further research is warranted to compare these 2 approaches.
Keywords
Introduction
Defined as a coronal Cobb angle >10 degrees, idiopathic scoliosis is the most common spinal disorder in pediatric and adolescent populations, occurring in approximately 1-3% of the community.1-5 While mild curves occur with high frequency, the incidence of AIS based on the magnitude of deformity varies, with severe deformity being less common. Curves >10 degrees, for example, have an incidence of 1-3%, whereas the incidence decreases to 0.15% to 0.3% for curves of >30 degrees. 1 Management options for AIS vary and are dependent on curve morphology and magnitude and remaining growth potential, and range from nonoperative measures such as observation and bracing to surgical correction.
For severe or progressive cases that require operative management, the primary goals of surgery are to correct the deformity, restore coronal and sagittal balance, and ultimately achieve solid arthrodesis.6-8 Historically, the gold standard in the surgical correction of AIS has been traditional open posterior instrumentation and fusion. 9 This technique is typically performed using a large midline incision with extensive subperiosteal stripping of the posterior elements and is associated with substantial blood loss, significant postoperative pain, surgical site infection, and poor cosmesis.8-10
Minimally invasive scoliosis surgery (MISS) has been proposed as a potential means of improving on these shortcomings. Compared to traditional open surgery, the potential benefits of MISS include smaller incisions with less soft tissue disruption, decreased blood loss, early mobilization, and shorter postoperative hospitalization.11,12 Though it offers these theoretical advantages, this less invasive approach can be more technically demanding and may rely, to a greater extent, on intraoperative imaging with potential for increased radiation exposure to the patient and staff. While there have been reports of acceptable outcomes associated with minimally invasive correction of AIS,8,9,12-16 to our knowledge no direct comparison between MISS and traditional open surgery has been conducted and the differences between these 2 approaches remains largely unclear. The aim of this meta-analysis is to review the literature comparing outcomes between MISS and traditional posterior instrumentation and fusion in the correction of AIS.
Materials and Methods
A systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 17 A search was performed in the MEDLINE, PubMed, EMBASE, Google scholar and Cochrane databases using the search terms “adolescent idiopathic scoliosis”, “open surgery”, and “minimally invasive surgery”. The final search was performed on December 31, 2019. In addition to these databases, the references of each article were also assessed manually for potential inclusion in the study.
Selection Criteria
Clinical studies were evaluated and included if they were written in English and reported a comparative cohort of traditional open versus minimally invasive surgical techniques for the treatment of AIS. Nonclinical studies, literature reviews, expert opinions, case reports, and those not reporting both MISS and open surgical treatment of AIS were excluded. Studies were reviewed by 2 of the study authors (AA, YA), who performed title and abstract reviews separately. The full texts of the articles meeting inclusion criteria based on title and abstract were then reviewed for final inclusion into the study, with authors coming to a consensus in instances of disagreement.
Quality Evaluation
Only non-randomized trials evaluating MISS versus open surgical correction of AIS were identified. Therefore, included studies were evaluated using the Newcastle–Ottawa Scale. 18 This quality assessment was performed independently by 2 authors (AA, YA).
Data Extraction and Analysis
The data items that were collected included (1) study characteristics (author name, study year, level of evidence, follow-up period, and number of patients), (2) patient demographics (age, sex), (3) number of patients undergoing MISS and open surgery, (4) subgroups as per Lenke classification, and (5) outcome measures. The primary outcome measure was major curve correction, determined using the following calculation: (Post-operative curve magnitude – Pre-operative curve magnitude) x 100. The secondary outcomes were blood loss (ml), operative time (minutes), VAS pain score, hospital length of stay (days), and complication and reoperation rates. The data was extracted by 2 authors independently.
The data analysis was performed by constructing a random-effects model using open Meta-Analysis Software. For continuous variables, the mean difference was utilized for estimating effect, with the values depicted in a forest plot diagram. For both types of variables, a 95% confidence interval (CI) was used. Statistical heterogeneity across the studies was tested using I 2 .
Surgical Technique
As reported in the included studies, traditional open scoliosis surgery was performed through a standard posterior midline approach with subperiosteal muscle dissection, pedicle screw insertion (freehand or fluoroscopy-guided), facetectomy/decortication and posterior release, followed by rod insertion and manual correction maneuvers. The MISS approach was performed using 1 to 3 midline incisions (∼3-5 cm in length) with subsequent skin and subcutaneous tissue mobilization to provide access to facet joints and pedicle screw starting points through a Wiltse approach. Pedicle screws were placed using O-arm navigation or via direct visualization and freehand technique, followed by subfascial rod insertion and manual reduction maneuvers with posterolateral fusion around the facets.
Results
Study Characteristics and Patient Demographics
A total of 4 studies were included in the analysis according to PRISMA guidelines (Figure 1
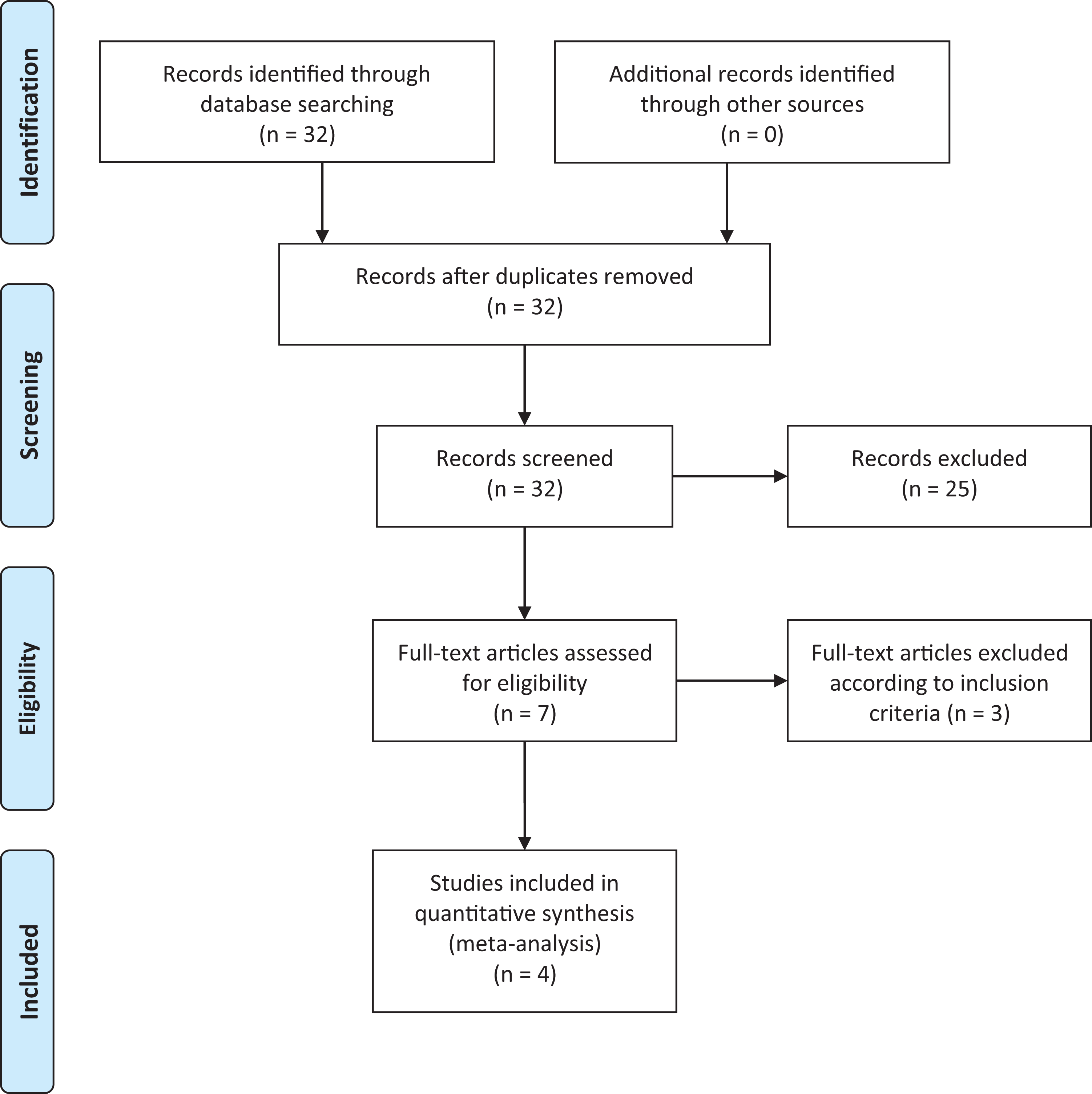
PRISMA 2009 flow diagram.
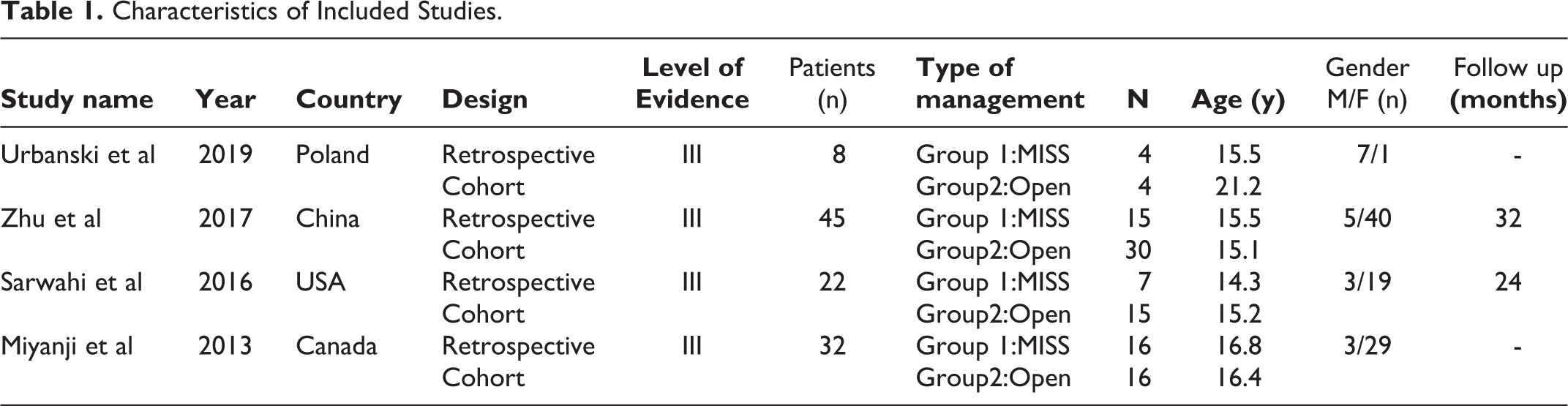
Characteristics of Included Studies.
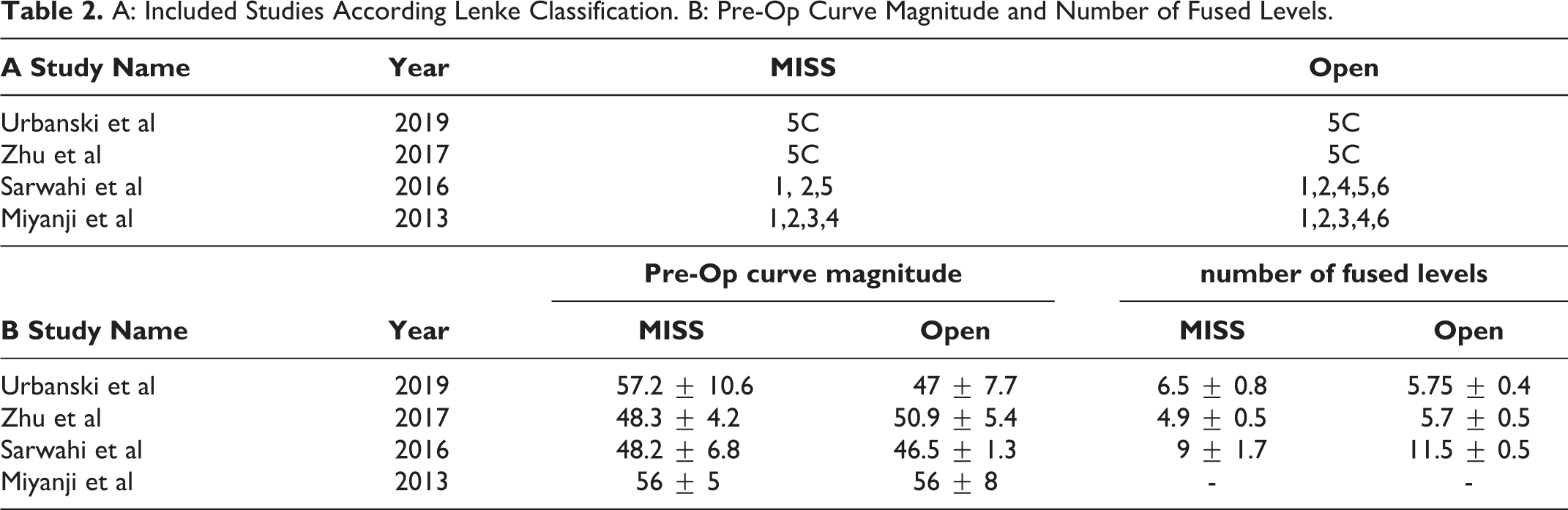
A: Included Studies According Lenke Classification. B: Pre-Op Curve Magnitude and Number of Fused Levels.
Quality Assessment
The quality of included studies was assessed according to the Newcastle-Ottawa Scale (Table 3
Quality Assessment.

Newcastle–Ottawa Scale.
Outcomes
Surgical correction
Major curve correction for MISS and open approaches is shown in Figure 2. There was no significant difference in preoperative curve magnitude between cohorts (Table 2B). There was no statistically significant difference in the major curve correction between the MISS (73.2%, CI 66.4%- 80.1%) and open (76.7%, CI 70.1%-83.3%) cohorts (MD: -2.05; CI -4.18 to 0.07; I2:99.2%). On subgroup analysis by curve type, there was similarly no statistically significant difference in curve correction between MISS (73.7%, CI 63.8%-83.6%) and open (78.3%, CI 78.1%-78.4) cohorts for Lenke 5C curves. However, there was a statistically significant difference in correction achieved for Lenke 1-4 curve types, with the MISS group (72.8%, CI 55.9%-89.65%) having a lower overall correction compared to the open group (75.5%, CI 60.4%-90.5%) (p < 0.001).
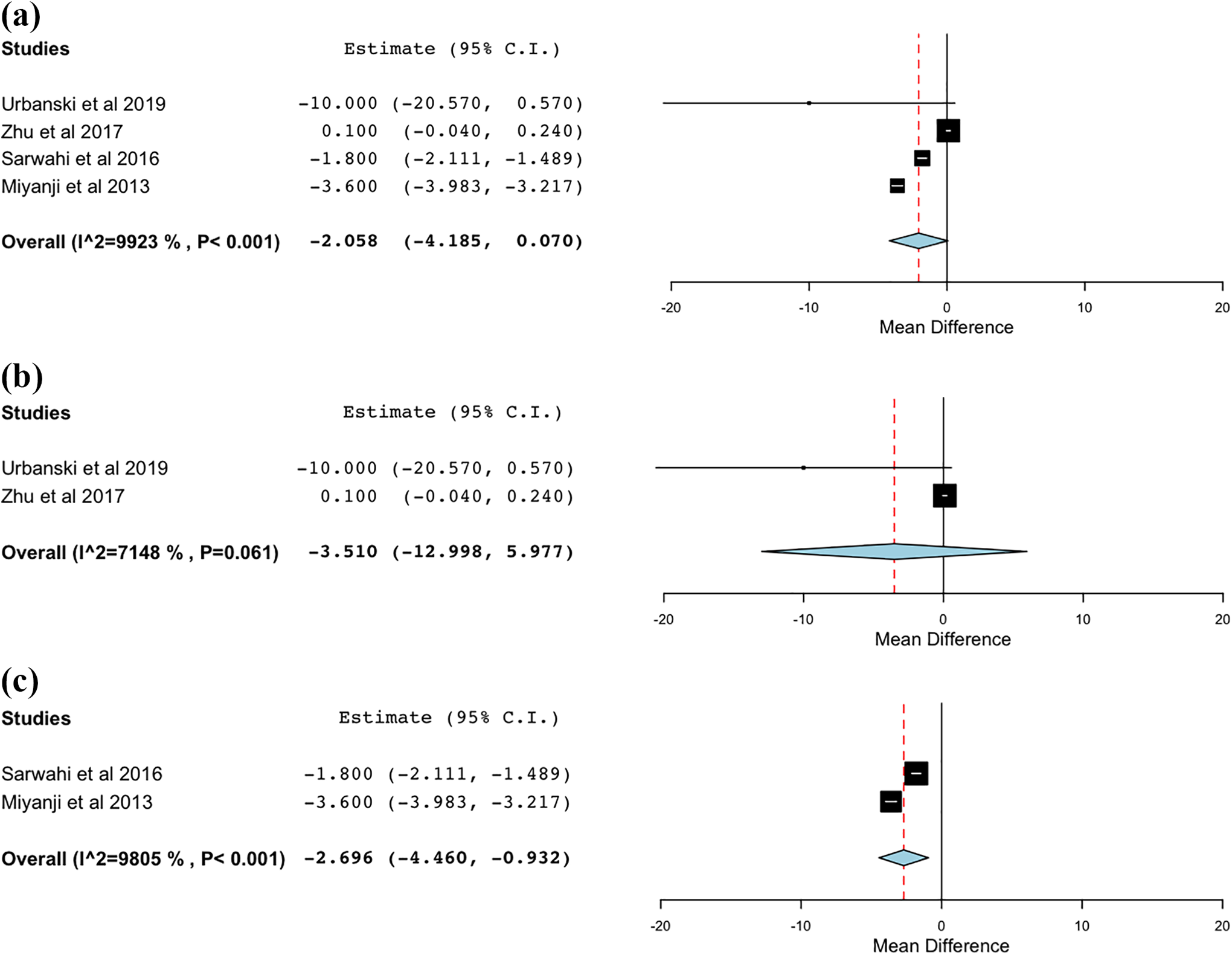
Curve correction. (a) Overall; (b) Lenke 5; (c) Lenke 1-4.
Estimated blood loss
Estimated blood loss was recorded for the open and MISS groups (Figure 3
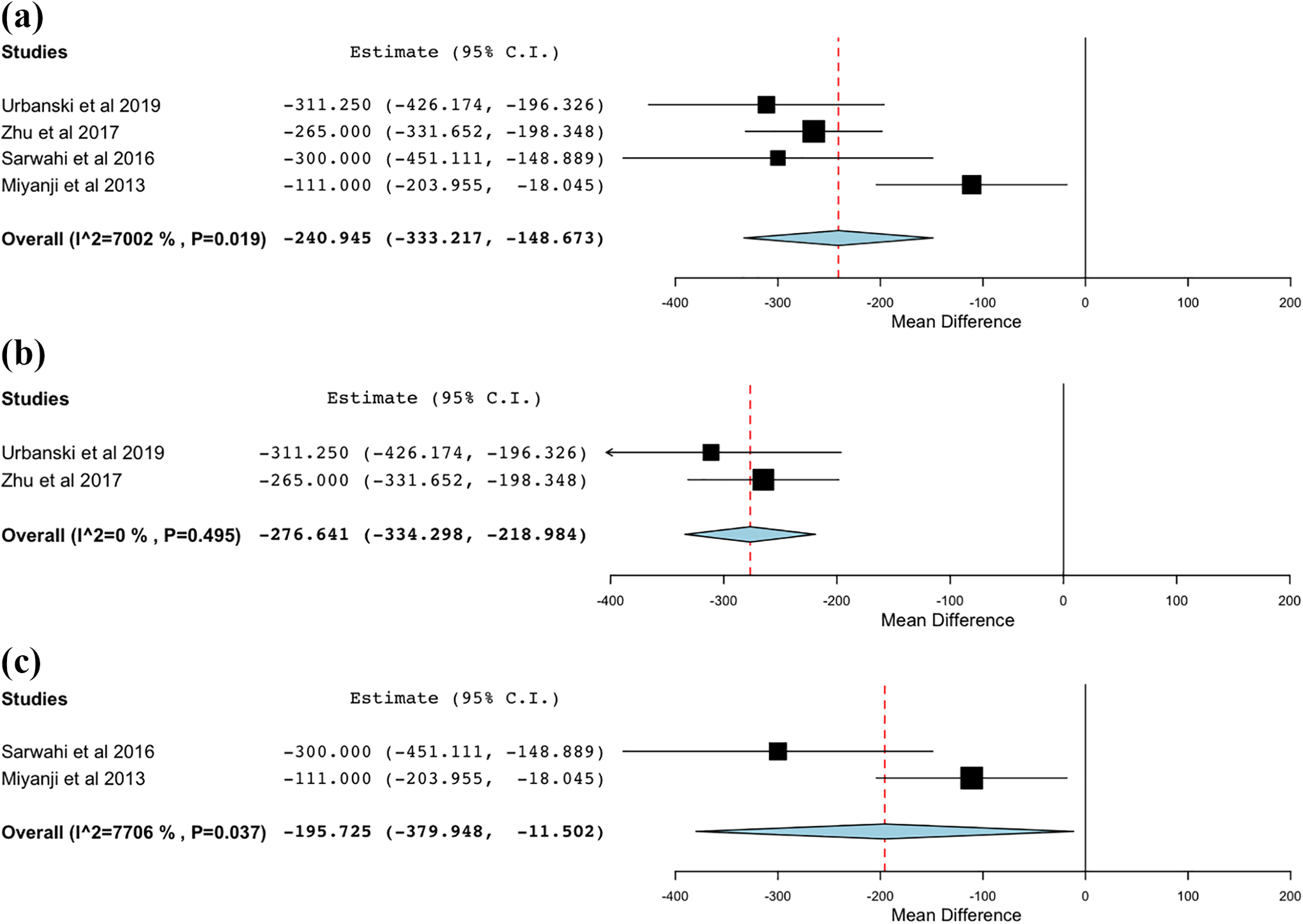
Estimated blood loss. (a) Overall; (b) Lenke 5; (c) Lenke 1-4.
Operative time
The operative times were recorded between MISS and traditional open approaches and compared in Figure 4. Overall, the MISS approach was associated with significantly longer operative times (379.9 min, CI 229.1 min - 530.6 min) compared to the open approach (301.5 min, CI 173.3- 439.7). These differences persisted on subgroup analysis with the MISS approach having significantly longer operative time in the Lenke 5C (mean difference, 53 min) and Lenke 1-4 (mean difference, 110.8 min) groups.
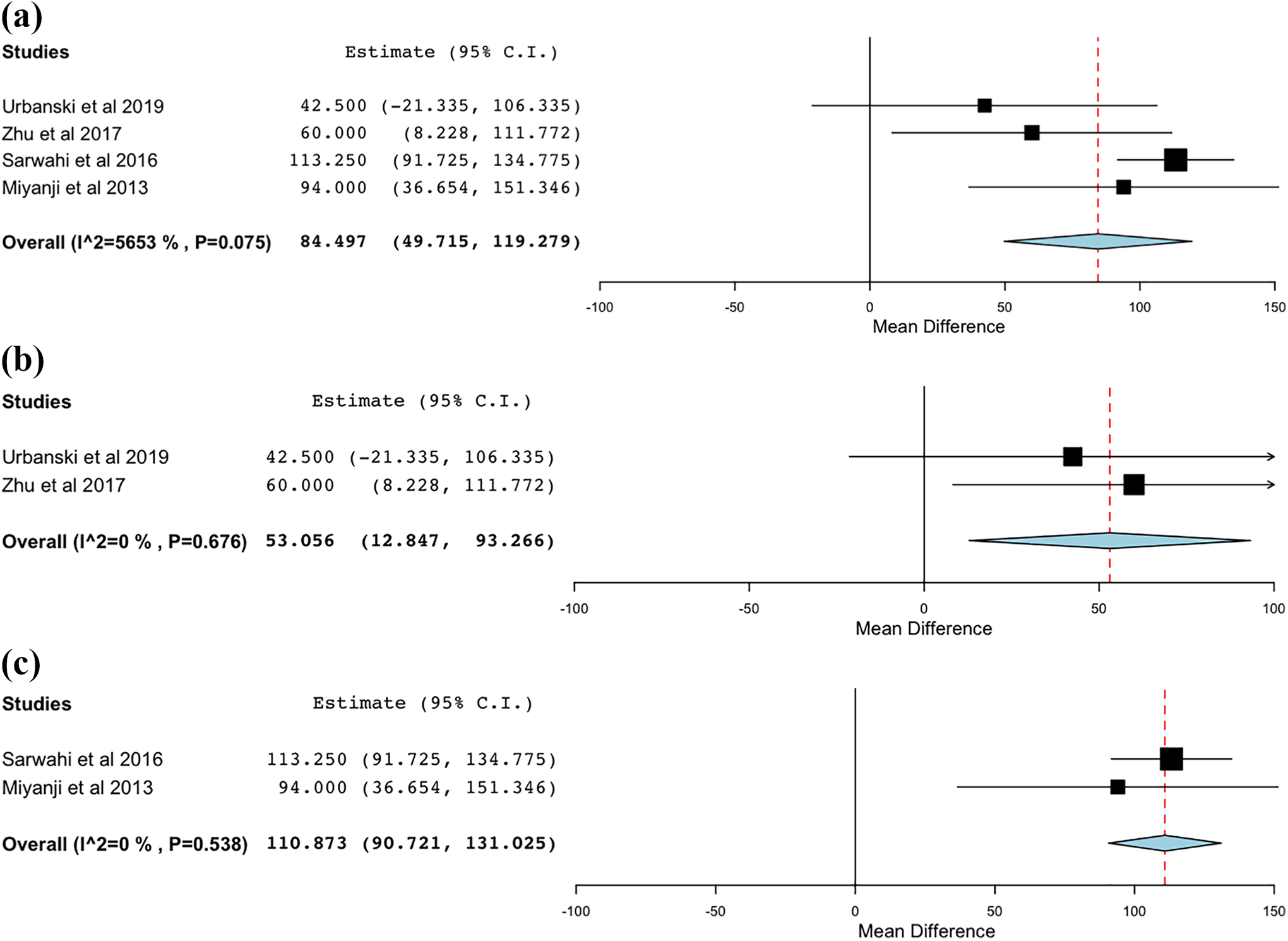
Operation time. (a) Overall; (b) Lenke 5; (c) Lenke 1-4.
Post-operative VAS pain
VAS pain scores were reported by 3 of the studies (Figure 5
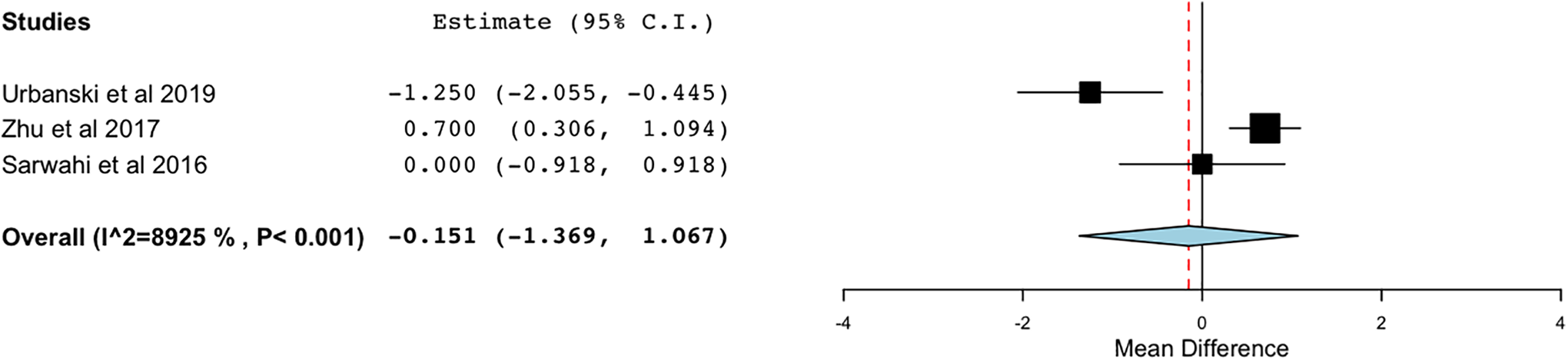
Pain score.
Length of stay
Length of stay was reported by 3 studies (Figure 6
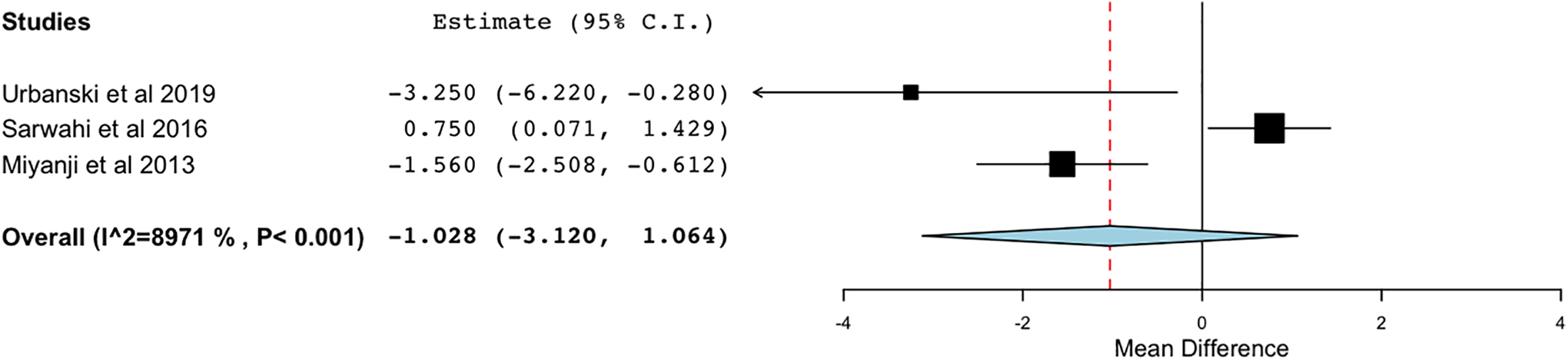
Hospital stay.
Complications and reoperation
Complications and reoperations were reported by 2 studies (Figure 7
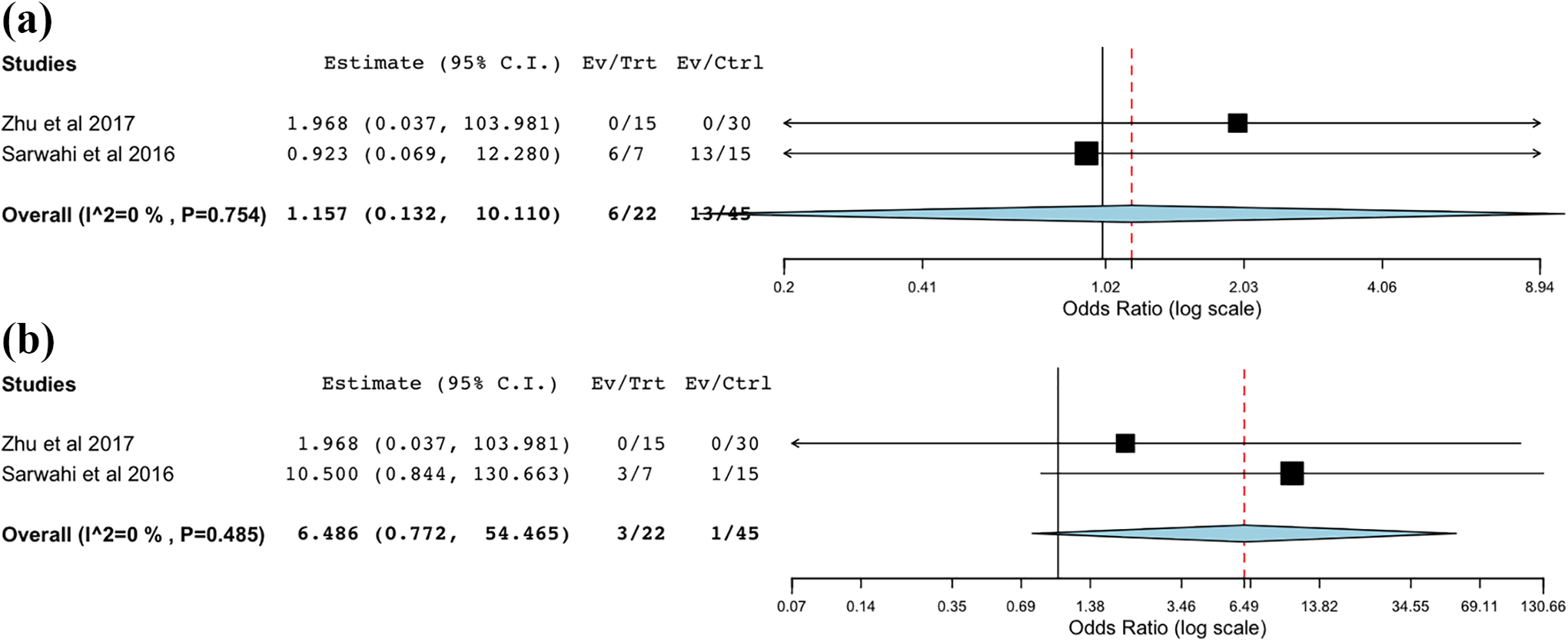
Overall complication (a) and reoperation rate (b).
Discussion
Traditional open techniques are considered the gold standard for the surgical management of scoliosis, though as minimally invasive spine surgery is becoming more widely practiced it is being increasingly applied to pediatric deformity correction.15-20 This meta-analysis was conducted to evaluate the differences in outcomes between open and MIS deformity correction and found that MISS is associated with less blood loss but longer operative times compared to traditional open fusion for AIS, while demonstrating similar outcomes in terms of curve correction, postoperative pain, LOS, and complications/reoperations.
MISS is emerging as a feasible tool in deformity correction, particularly in adult populations. The technique has found applications in adult degenerative scoliosis, demonstrating excellent short- and long-term radiographic and patient reported outcomes.21-24 More recently, several studies have demonstrated similar success in the treatment of AIS with minimally invasive techniques.8,9,12,14-16 Theoretical advantages include reduced soft tissue trauma, decreased blood loss, less postoperative pain, shorter hospital LOS, and fewer infections. 16 However, it is unclear if the limited exposure associated with MIS techniques limits the ability to perform an adequate correction. To our knowledge, this is the first meta-analysis to examine MISS and traditional open approaches in the surgical management of AIS. Here we demonstrate that MISS was associated with less blood loss (240 mL) compared to open surgery. We further found no differences in curve correction, postoperative pain, hospital LOS, or complications and reoperations. While there appear to be certain benefits associated with the MISS approach, this analysis did show that operative times were longer when compared to traditional open surgery, with MISS taking ∼85 minutes longer on average to perform.
A critical factor that supports the use of MISS is the reduction in intraoperative blood loss and the corresponding decreased need for intra- and postoperative blood transfusion. Managing blood loss has been a focus of deformity surgery, as it has important implications on patient outcome thought to be associated with reducing the use of allogeneic blood products, which can increase the risk for postoperative infection25,26 As a result, many efforts have been put forth to study pharmacologic agents to help limit blood loss during these procedures.27-31 In the pediatric and adolescent population these effects may be even more pronounced, as smaller overall body size increases the percentage of blood volume loss during posterior fusion. 32 Regarding transfusion requirements in the current study, the data was incompletely reported among the 4 included studies which precluded meaningful analysis. Sawarhi et al noted that 11 of 15 patients in the open group required transfusion (7 intraoperative, 4 postoperative; 73.3%) versus 1 patient in the MISS group (postoperative; 14.3%), while Zhu et al reported that 3 of 30 patients in the open group (10%) required transfusion versus none in the MIS group. Our results are consistent with the findings of prior studies, with MIS techniques demonstrating significantly less blood loss than open procedures.
In addition to blood loss, another commonly cited benefit of the MIS approach is reduced hospital LOS, as patients undergoing MIS procedures tend to show quicker recover and earlier hospital discharge. 14 While the results of our meta-analysis showed a lower mean length of stay for the MIS cohort by 1 day, this difference was not statistically significant. The data is based on the results of only 3 studies, with 2 studies (Urbanski, Miyanji) reporting reduced LOS for the MIS group and 1 study (Sarwahi et al 2016) reporting longer LOS for the MIS cohort. Sarwahi et al. may represent an outlier since the reported LOS in this study (8 and 9 days for the open and MIS cohorts, respectively) is substantially longer than what is reported in the literature.
Despite the observed advantages of MIS approaches, several important concerns must be acknowledged. Longer operative times have been consistently reported with the adoption of MIS techniques, with all included studies in our analysis noting longer OR times
The overall complication profile and reoperation rate is important aspect of any surgical procedure, particularly 1 in the early stages of adoption. A comparable complication rate was found between both approaches in the 2 studies where they were reported, though low overall numbers preclude a meaningful comparison. The most commonly reported complications in both groups were instrumentation-related, surgical site infection or wound dehiscence, and anemia.12,14,15,16
Finally, as with any surgical procedure and technique, appropriate patient selection is paramount. Though minimally invasive surgery has many benefits, by definition there is less soft tissue dissection and exposure and therefore it may not be suitable for more severe deformities. As this is a relatively novel technique, there is no consensus on the characteristics which make a patient appropriate for MISS. Sarwahi et al. limited their indications to patients with less severe (<70 degrees) and flexible (>50% flexibility on bending films) curves. Others have focused on a narrow population of patients with Lenke type 5C curves (Urbanski, Zhu). Urbanski et al. note that early adoption of MIS may be most appropriate in patients with flexible curves and wide pedicles, making type 5C curves requiring fusion only in the lumbar and lower thoracic spine ideal initial candidates. This is supported by the finding that MISS techniques achieved less correction by percentage versus open techniques in a subgroup analysis of Lenke types 1-4. Whether these indications can be extended to include more severe and less flexible curves is unclear based on the findings of the current study.
There are several limitations associated with this study. First, as a meta-analysis, it is limited by the primary data that was reported by the included studies. These studies were all retrospective in nature and therefore could introduce selection bias with underlying differences in those undergoing MIS versus open techniques. Furthermore, the included studies are small and heterogeneous, with 2 studies focused on a narrow population of Lenke type 5C curves and 2 other studies inclusive of more curve types. We attempted to limit this drawback and further evaluate the Lenke 5C curves, where MIS techniques appear to be most applicable, by performing subgroup analysis of these patients where possible. Third, as this is an emerging technique, our study is limited to the relatively early and perhaps varied experience of several surgeons, and results may change as these surgeons gain more experience and adopt new or refined techniques. Finally, there are important variables about which we are not able to report given the lack of data, including radiation exposure and fusion rate. Further research is needed to bolster the current findings and better understand the differences between these approaches.
Conclusion
For surgeons with the appropriate training, MISS appears to be a safe and effective alternative to open posterior fusion in the surgical treatment of AIS, particularly for patients with Lenke 5C curves. While MISS has emerged as a feasible option for the surgical management of AIS, further research is warranted to compare these 2 approaches.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Qureshi reports other from Cervical Spine Research Society, personal fees from Stryker K2M, other from Simplify Medical, Inc., other from Avaz Surgical, other from International Society for the Advancement of Spine Surgery, other from North American Spine Society, other from ![]() Inc., other from Association of Bone and Joint Surgeons, other from Society of Lateral Access Surgery, personal fees from Globus Medical, Inc., personal fees from Paradigm Spine, other from Society of Minimally Invasive Spine Surgery, other from Minimally Invasive Spine Study Group, personal fees from RTI Surgical Inc., other from Spinal Simplicity, LLC, personal fees from AMOpportunities, other from Contemporary Spine Surgery, other from Annals of Translational Medicine, personal fees from Healthgrades, other from The American Orthopaedic Association, other from Vital 5, outside the submitted work
Inc., other from Association of Bone and Joint Surgeons, other from Society of Lateral Access Surgery, personal fees from Globus Medical, Inc., personal fees from Paradigm Spine, other from Society of Minimally Invasive Spine Surgery, other from Minimally Invasive Spine Study Group, personal fees from RTI Surgical Inc., other from Spinal Simplicity, LLC, personal fees from AMOpportunities, other from Contemporary Spine Surgery, other from Annals of Translational Medicine, personal fees from Healthgrades, other from The American Orthopaedic Association, other from Vital 5, outside the submitted work
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.