
Abstract
Study Design
Retrospective cohort study.
Objectives
With the aging of the Japanese population, patients with athetoid cerebral palsy (ACP) are getting older, and the rate of surgery for CSM is increasing in ACP patients. However, postoperative complications of such surgery among adult patients with ACP have not been reported yet. We investigated postoperative complications of surgery for CSM with ACP and compared them with those of surgery for CSM without ACP using a national inpatient database of Japan.
Methods
Using the Diagnosis Procedure Combination database, we identified 61382 patients who underwent surgery for CSM from July 2010 to March 2018. We examined patient backgrounds, surgical procedures, and type of hospital, and a 4:1 propensity score matching was performed to compare the outcomes between the non-ACP and ACP groups.
Results
There were 60 847 patients without ACP and 535 patients with ACP. The mean age was 68.5 years in the non-ACP group and 55 years in the ACP group. The percentages of patients who underwent fusion surgery were 21.6% and 68.8% in the non-ACP and ACP groups, respectively. The 4:1 propensity score matching selected 1858 in the non-ACP group and 465 in the ACP group. The ACP group was more likely to have postoperative urinary tract infection (.4% vs 2.8%, P < .001), postoperative pneumonia (.4% vs 2.4%, P < .001), and 90-day readmission for reoperation (1.9% vs 4.3%, P = .003).
Conclusions
We found that ACP patients were more vulnerable to postoperative complications and reoperation after CSM than non-ACP patients.
Keywords
Introduction
Cerebral palsy (CP) was first described by Little in 1861, and is defined as a series of permanent disorders of movement and posture with activity limited by a non-progressive disorder of the developing brain in the fetus or infant. 1 In recent years, the number of adult cases of CP has been increasing, 2 and it is estimated to be approximately 700 000 to 1 million patients with CP in the United States. 3 Although CP is caused by non-progressive brain damage, involuntary movements exacerbate the patients’ musculoskeletal components over time. Motor disorders in adult cases of CP include osteoarthritis, chronic pain associated with joint contraction, scoliosis, cervical spondylosis, and dysplasia of the hip joint. 3 Previous studies showed that myelopathy was about 8 times more common in patients with CP than in non-CP patients. 2
Athetoid CP (ACP) is 1 of the typical diseases of CP. Intermittent involuntary movements of the neck could cause cervical spondylotic myelopathy (CSM), which was first reported in 1962. 4 With the aging of the Japanese population, the age of patients with ACP is advancing. Therefore, there are increasing opportunities for surgery for CSM in patients with ACP. Regarding postoperative complications of surgery in patients with ACP, those of interventions for pediatric deformity have been reported.5-10 However, postoperative complications of surgery for CSM in adult patients with ACP have not been described. Hence, we aimed to compare characteristics and postoperative complications for CSM between patients with and without ACP, using a national inpatient database in Japan.
Materials and Methods
Data Source
The Diagnostic Procedure Combination database contains administrative claims data and hospital discharge abstracts for approximately 1000 hospitals in Japan. 11 All 82 university hospitals are required to contribute to the database, but participation by community hospitals is voluntary. This database includes information on patient age and gender, body mass index (BMI), smoking status, admission route (admission from home or somewhere else), main diagnosis, complications that are already present at admission, and complications that occurred after admission, recorded using the International Classification of Diseases, 10th Edition (ICD-10) codes; surgical procedures coded with Japanese original codes; duration of anesthesia; and discharge status. The database clearly distinguishes between preoperative comorbidities and postoperative complications.12,13 The study did not require the informed consent of the patients to participate in the study because of the anonymity of the data. The Institutional Review Board of The University of Tokyo approved this study (approval number: 3501-(3)).
Patients
Data of patients admitted between July 2010 and March 2018 were extracted from the database. We included those who had a diagnostic code for cervical spondylosis (M4782), CSM (M4712), or athetoid CP (G803) and underwent surgery for CSM. We excluded patients undergoing dialysis, those with rheumatoid arthritis (M05, M06), and those who previously received revision spine surgery. We calculated Charlson Comorbidity Index (CCI) based on ICD-10 codes for each patient with Quan’s algorithm. 14
Outcomes
The primary outcomes were postoperative complications including surgical site infection (T813 and T814), pneumonia (J12–J18), cardiac events (acute coronary events (I21–I24) or heart failure (I50)), pulmonary embolism (I26), stroke (cerebral infarction or hemorrhage (I60–I64)), and renal failure (N17–N19). The secondary outcomes included duration of anesthesia, in-hospital mortality, and readmissions for reoperation within 90 days after discharge.
Statistical Analysis
We compared the background and postoperative complications of patients with and without ACP. To adjust for the measured confounders, we performed propensity score matching. 15 To estimate the propensity score, we used a logistic regression model for ACP as a function of patient demographic and hospital factors, including patient age, gender, CCI, BMI, smoking status (smokers or non-smokers), diabetes mellitus (ICD-10 codes, E10–E14), surgical procedures (decompression or fusion), admission route (admission from home or other than home), and hospital volume. BMI was categorized into <18.5, 18.5-24.9, 25-29.9, and ≥30 kg/m2. Hospital volume was defined as the number of patients who underwent spine surgery at each hospital, and was categorized into tertiles. The four-to-one nearest-neighbor matching without replacement was used between the non-ACP and ACP groups. We set the width of the caliper to <.2 of the pooled standard deviation of the assessed propensity scores. We calculated the C-statistics using the area under the receiver operating characteristic curve to evaluate the ability of the model to predict ACP. An absolute value of the standardized difference of >10% indicated a significant imbalance of the baseline covariates. 16 Categorical variables were summarized according to numbers and percentages, and continuous variables according to the mean and standard deviation. The t test was used for continuous variables, and the chi-squared test or Fisher’s exact test was used for categorical variables. The level of statistical significance was set at P < .05 by a two-sided test. Statistical analyses were performed using Stata/MP version 17 (StataCorp, College Station, TX, USA).
Results
Comparison of Preoperative Data Between the ACP and Non-ACP Groups.
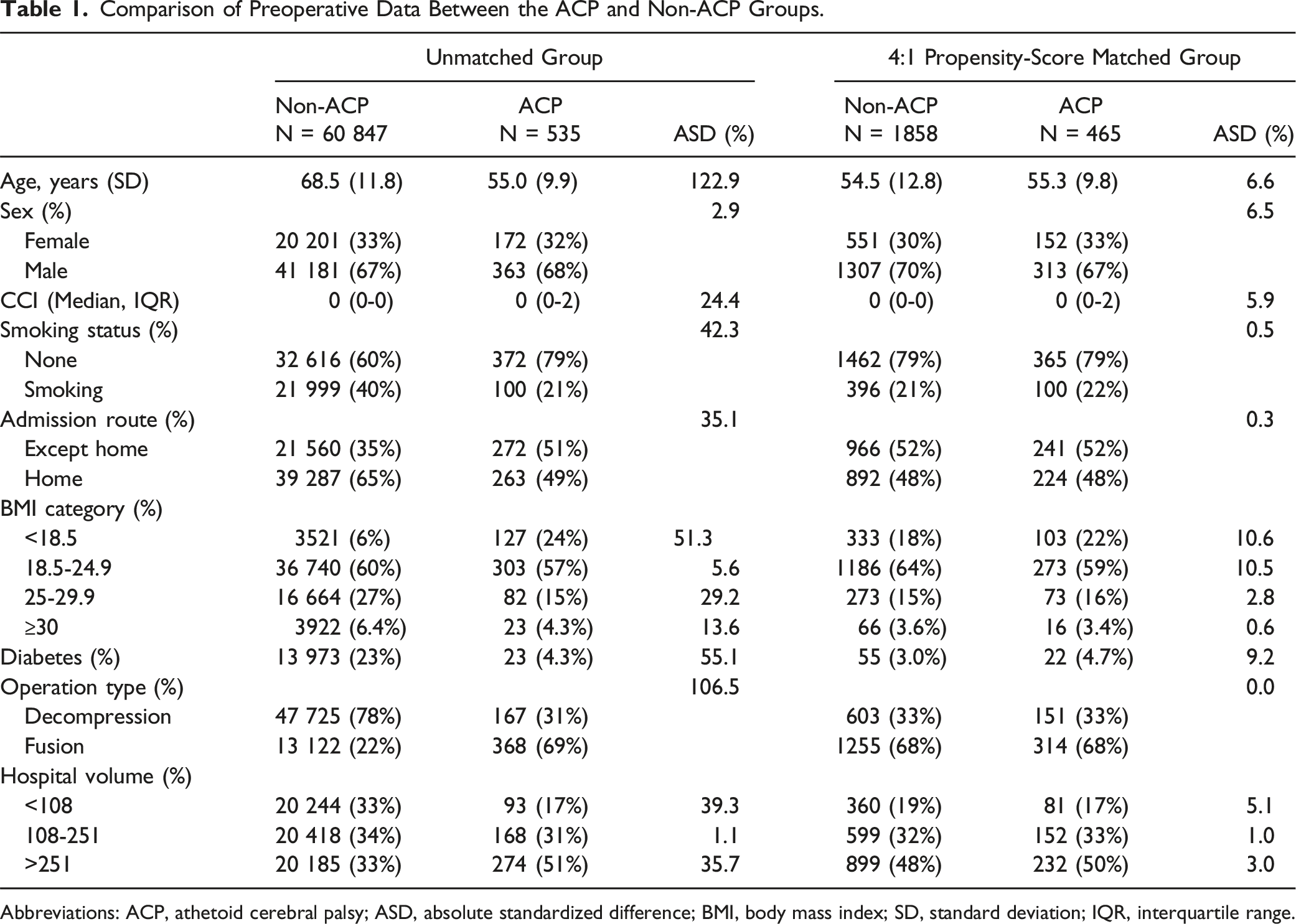
Abbreviations: ACP, athetoid cerebral palsy; ASD, absolute standardized difference; BMI, body mass index; SD, standard deviation; IQR, interquartile range.
Comparison of Duration of Anesthesia, Perioperative Complications, and Readmission Within 90 days Between the Non-ACP and ACP Groups in the 4:1 Propensity-Score Matched Population.
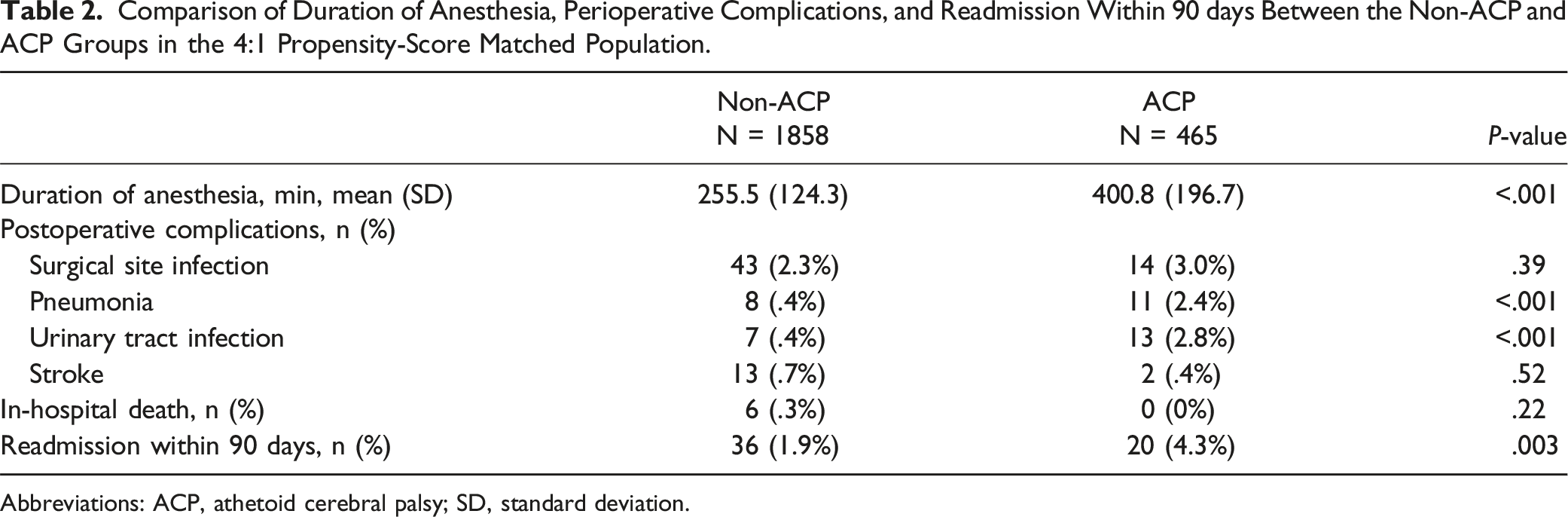
Abbreviations: ACP, athetoid cerebral palsy; SD, standard deviation.
Discussion
We compared the rate of postoperative complications between patients having cervical myelopathy with and without ACP using a nationwide inpatient database in Japan. Overall, patients in the ACP group tended to be younger and to undergo fusion surgery more frequently. After propensity score matching, the ACP group had a significantly higher proportion of perioperative complications, including urinary tract infection, pneumonia, and readmission for reoperation. To the best of our knowledge, this was the first study that clarified clinical characteristics and postoperative complications in patients with CSM associated with ACP.
In patients with ACP, involuntary movement of the neck can cause spondylotic changes in their early-middle age, and the accelerated degeneration of the cervical spine and repetitive neck motion result in cervical compressive myelopathy. Therefore, it was reasonable that patients in the ACP group underwent cervical spine surgery in their 50s, which was significantly younger than the age for such surgery in the non-ACP group. This finding is in line with those of previous case series.17-21 As for the surgical procedure, the present study showed that about 70% of patients with ACP underwent fusion surgery. This figure may represent the recent trend toward rigid fixation surgery in CSM cases with ACP. Indeed, although the number of patients was relatively small, recent studies also showed that most patients underwent fusion surgery.18,20,21. Given that the dynamic factor is considered 1 of the main causes of myelopathy in ACP patients, it was reasonable that fixation surgery was the main therapeutic procedure for CSM patients with ACP.
In the present study, readmission for reoperation occurred more frequently after CSM surgery in the ACP patient group. Owing to the nature of involuntary movement in ACP patients, spinal instability and implant failure can occur after cervical spine surgery.22-24 In addition, morphological abnormalities of the cervical spine 25 and bone structure abnormalities 26 have been reported in patients with CP, and these make surgical procedures technically demanding. For example, a previous study reported 3 out of the 31 patients with ACP undergoing cervical fusion surgery, including 1 patient with screw malposition and 2 patients with SSI. 18 Another study reported that 29% of the cases showed a critical breach of pedicle screws. 25 The difficulty in decompression or the fixation procedure in ACP patients may be further supported by the longer duration of anesthesia in this study. This result may reflect the recent trend of longer surgery durations. Although the precise reason for the readmission was uncertain, we believe that implant-related revision surgery (such as the loosening of screws or rod breakage) was the main cause of readmission in ACP patients.
The present study showed that patients with ACP were at a higher risk of postoperative pneumonia and urinary tract infection, and these results were in line with those of previous reports. For example, previous studies reported that the proportion of postoperative pneumonia was about .5% after spinal surgery27,28 and the proportion of urinary tract infection was around 1% in patients undergoing spine surgery.29,30 Conversely, an increased risk of postoperative pneumonia (odds ratio: 2.21) or postoperative urinary tract infections (odds ratio: 2.75) was reported in CP patients with scoliosis compared to those with adolescent idiopathic scoliosis. 10 We speculate that delayed mobilization may have led to a higher incidence of postoperative infectious diseases in ACP patients in the current study. Indeed, long-term bed rest is considered a risk factor for postoperative pneumonia, and CP is associated with other ADL impairments, such as osteoarthritis and joint contractures.3,31 Surgeons are therefore required to reduce the duration of postoperative bed rest and to start rehabilitation immediately after surgery.
This study has several limitations. First, because our data set consisted of administrative claims data, postoperative complications may have been underreported, and complications such as neuropathy and arterial injury were unknown. Second, the DPC database did not include all relevant clinical information, such as ACP severity, the number of levels, and patient-reported outcomes. In particular, preoperative JOA scores and other information were unknown, but the ACP group had involuntary movements that tended to delay the diagnosis of CSM and may have resulted in differences in the severity of neurologic symptoms. In addition, because this study used a database that examined medical costs during hospitalization, no assessment of the details and optimization of outpatient drug therapy existed in this study’s database. Third, coded diagnoses may have been less accurate than those documented in prospective studies because of the possibility of misclassification and underreporting. Finally, the reasons for reoperation were unknown, although infection and implant failure were speculated to be the causes of reoperation. Nevertheless, we believe that our study provides some insight into postoperative complications in CSM patients with ACP that would be difficult to track at a single institution.
Conclusion
Patients with ACP were more vulnerable to postoperative pneumoniae and urinary tract infection than non-ACP patients following cervical spine surgery. Furthermore, the 90-day readmission rate for reoperation was higher among patients with ACP.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Ministry of Health, Labour and Welfare, Japan (23AA2003 and 22AA2003). There are no relevant financial activities outside the submitted work.