
Abstract
Study Design
Retrospective cohort study
Objectives
To evaluate the effect of caudal instrumentation level on revision rates following posterior cervical laminectomy and fusion.
Methods
A retrospective review of a prospectively collected database was performed. Minimum follow-up was one year. Patients were divided into two groups based on the caudal level of their index fusion construct (Group 1-cervical and Group 2- thoracic). Reoperation rates were compared between the two groups, and preoperative demographics and radiographic parameters were compared between patients who required revision and those who did not. Multivariate binomial regression analysis was performed to determine independent risk factors for revision surgery.
Results
One hundred thirty-seven (137/204) patients received fusion constructs that terminated at C7 (Group 1), while 67 (67/204) received fusion constructs that terminated at T1 or T2 (Group 2). The revision rate was 8.33% in the combined cohort, 7.3% in Group 1, and 10.4% in Group 2. There was no significant difference in revision rates between the 2 groups (P = .43). Multivariate regression analysis did not identify any independent risk factors for revision surgery.
Conclusion
This study shows no evidence of increased risk of revision in patients with fusion constructs terminating in the cervical spine when compared to patients with constructs crossing the cervicothoracic junction. These findings support terminating the fusion construct proximal to the cervicothoracic junction when indicated.
Level of Evidence
III
Keywords
Introduction
Cervical spondylotic myelopathy (CSM) is a common clinical entity that results in progressive neurologic dysfunction and disability.1,2 Symptomatic CSM has become a leading indication for surgical cervical spine decompression, with patients typically reporting significant improvement in their symptoms following surgery.3-5 Posterior cervical laminectomy and fusion is a commonly utilized surgical strategy, particularly in patients with ≥3 stenotic segments, maintained cervical lordosis, and/or ossification of the posterior longitudinal ligament (OPLL).3,4 Fusions terminating about the cervicothoracic junction (CTJ) are of particular interest, as the transition from the flexible cervical spine to the semi-rigid thoracic spine creates unique treatment challenges.6-13
Prior literature comparing surgical outcomes in fusions terminating cranial and caudal to the CTJ are inconclusive.14-18 In a recent meta-analysis, Goyal et al 16 demonstrated higher fusion rates and lower reoperation rates in cervical fusion constructs that cross the CTJ. Prior studies have also reported lower incidence of adjacent segment disease (ASD) in constructs terminating in the upper thoracic spine, supporting the notion that crossing the CTJ may be protective against the development of ASD.14,15 However, extending fusion constructs past the CTJ has been shown to substantially limit post-operative range of motion and results in increased operative time, EBL, and healthcare costs, as crossing the CTJ leads to the use of additional level and thoracic arthrodesis codes.15,18,19
Given these disadvantages of extending posterior fusion constructs past the cervicothoracic junction, it is important to characterize the full risk/benefit profile of terminating posterior fusion constructs at various vertebral levels. The purpose of the present study was to determine if terminating posterior fusion constructs cranial to the CTJ results in a higher revision rate when compared to constructs terminating in the upper thoracic spine. It was hypothesized that revision rates would be similar between the two groups.
Methods
Following Institutional Review Board (IRB) approval at the University of Pittsburgh (STUDY19100333), a prospectively collected database was used to identify all patients who underwent posterior cervical laminectomy and fusion performed by two fellowship-trained spine surgeons at a single institution from August 2012 to August 2019. Four hundred ninety-six posterior cervical laminectomy and fusion procedures were identified in this manner. All patients received lateral mass screws in the cervical spine and pedicle screws in the thoracic spine. Fusions were performed using the Stryker (Kalamazoo, MI) Oasys system with a combination of local autograft and cancellous allograft chips or iliac crest bone graft. Patients with less than 1-year clinical follow-up, less than 4 vertebral levels fused, surgery performed for trauma or tumor, or fusion constructs terminating cranial to C7 or caudal to T2 were excluded (Figure 1). If adequate decompression could be accomplished without complete C7 laminectomy and there was no radiographic evidence of C7-T1 instability, the cervicothoracic junction was not crossed. One patient who received a fusion ending at C7 did receive a complete laminectomy at C7, though the reasoning for this decision was not clear from the medical records. Following exclusion, 204 patients with at least 1-year clinical follow-up who underwent primary posterior cervical laminectomy and fusion for degenerative indications were included in the study cohort. Inclusion/Exclusion Criteria.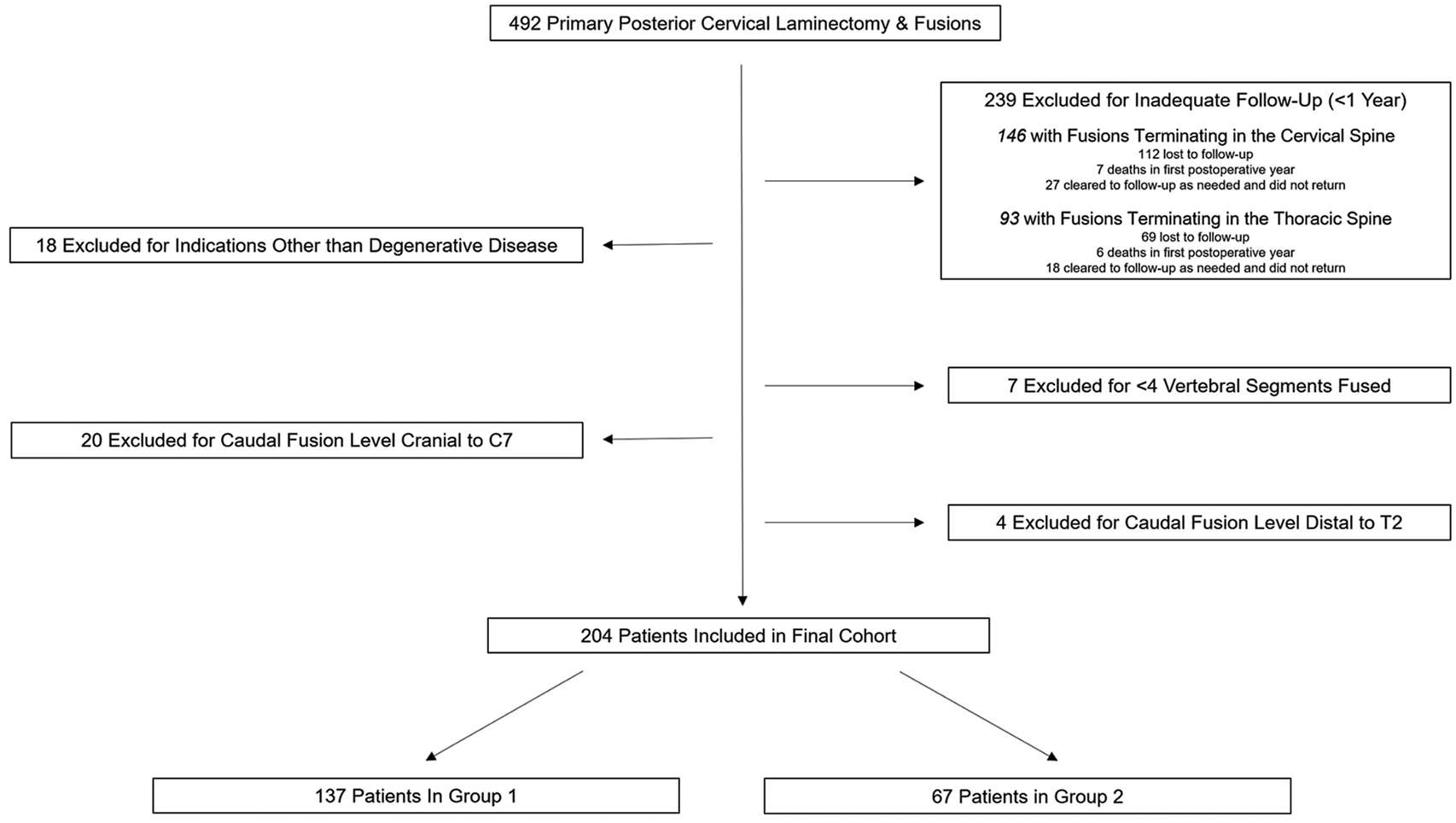
The electronic medical record (EMR) was queried to identify patients who required revision cervical surgery following their index posterior cervical laminectomy and fusion. Patients were divided into 2 groups based on the caudal level of their index fusion construct. All patients in Group 1 received a fusion construct that terminated at C7, while all patients in Group 2 received a fusion construct that terminated in the upper thoracic spine (T1 or T2). Revision rates of each group were calculated. Relevant preoperative demographic and radiographic measurements were collected and compared between Group 1 and Group 2 as well as between patients requiring revision and those who did not. Continuous variables were analyzed using two-way Student t-tests, and categorical variables were analyzed using Fischer’s exact test. Multivariate binomial regression analysis was performed accounting for all reported variables to determine independent risk factors for revision surgery. Age, Charlson Comorbidity Index (CCI), and age-adjusted CCI were suspected of collinearity. Therefore, age and CCI were independently included while age-adjusted CCI was excluded from the multivariate model. A prior power analysis using the revision rates found by Schroeder et al 14 revealed that 202 patients would be required to obtain a power of 80%. Statistical significance was defined as P < .05.
Results
Four hundred ninety-two primary posterior cervical fusions were identified during the study period. Following exclusion, a total of 204 patients were included in the analysis (Figure 1). Two hundred thirty-nine patients were excluded due to less than 1-year of clinical follow-up, 18 excluded as surgery was performed for trauma or tumor, 7 excluded as <4 vertebral segments were fused, 20 excluded as their most caudal instrumented vertebra was cranial to C7, and 4 excluded as their most caudal instrumented vertebra was distal to T2. Of the patients with less than 1-year clinical follow-up, 146 had fusions terminating in the cervical spine and 93 had fusions terminating in the thoracic spine. Of those with fusions terminating in the cervical spine, 77% (112/146) did not return for recommended clinic visit, 5% (7/146) died in the first post-operative year, and 18% (27/146) were cleared to follow-up as needed prior to 1-year and did not return. Of those with fusions terminating in the thoracic spine, 74% (69/93) did not return for recommended clinic visit, 6% (6/93) died in the first post-operative year, and 19% (18/93) were cleared to follow-up as needed prior to 1-year and did not return. There was no significant difference between the groups when comparing reasons for inadequate follow-up (P = .81).
Demographic and Operative Characteristics of Fusions Terminating in Cervical Spine vs Thoracic Spine.
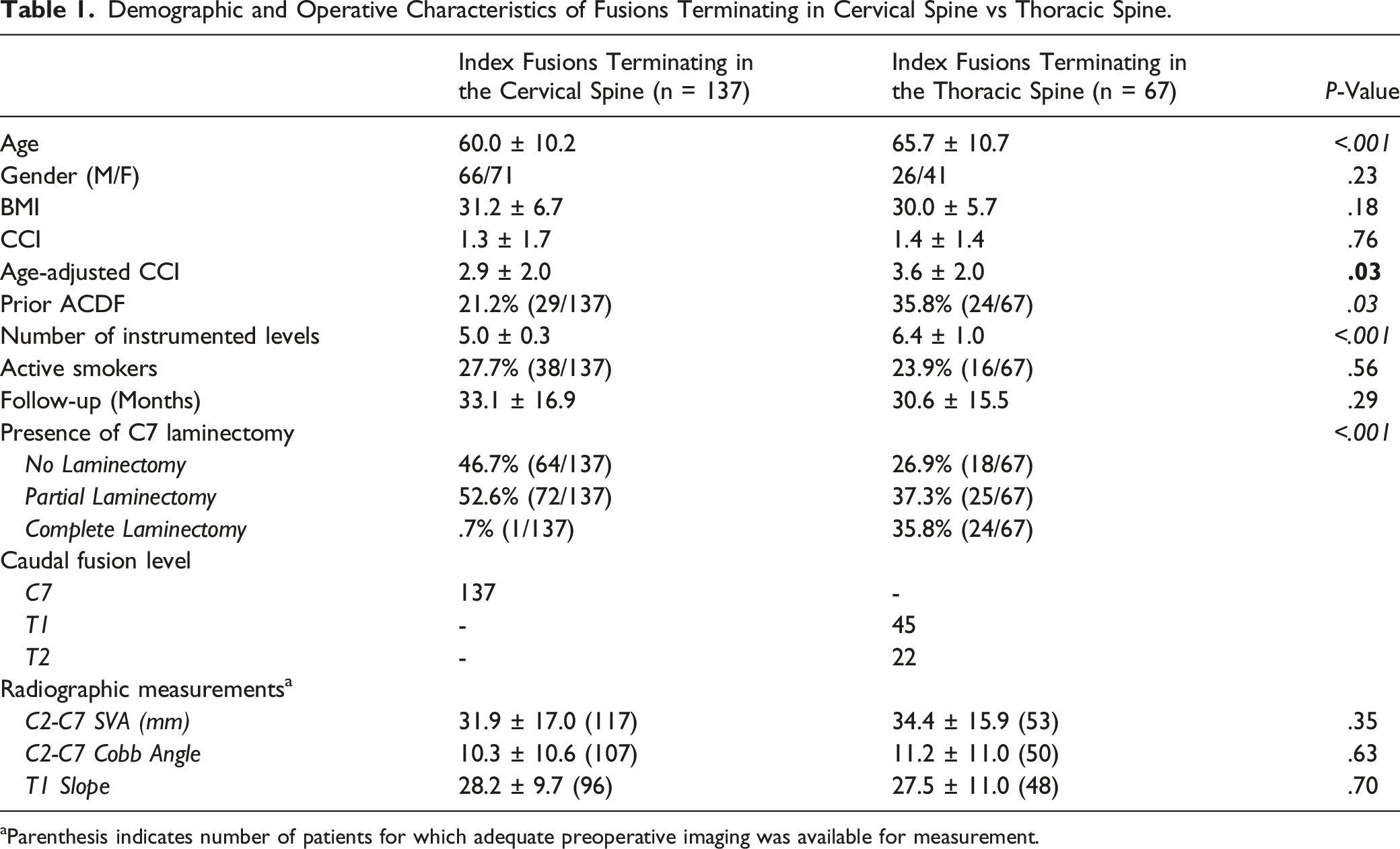
aParenthesis indicates number of patients for which adequate preoperative imaging was available for measurement.
Demographic and Operative Characteristics in Cases Requiring Revision vs Those that Did Not.
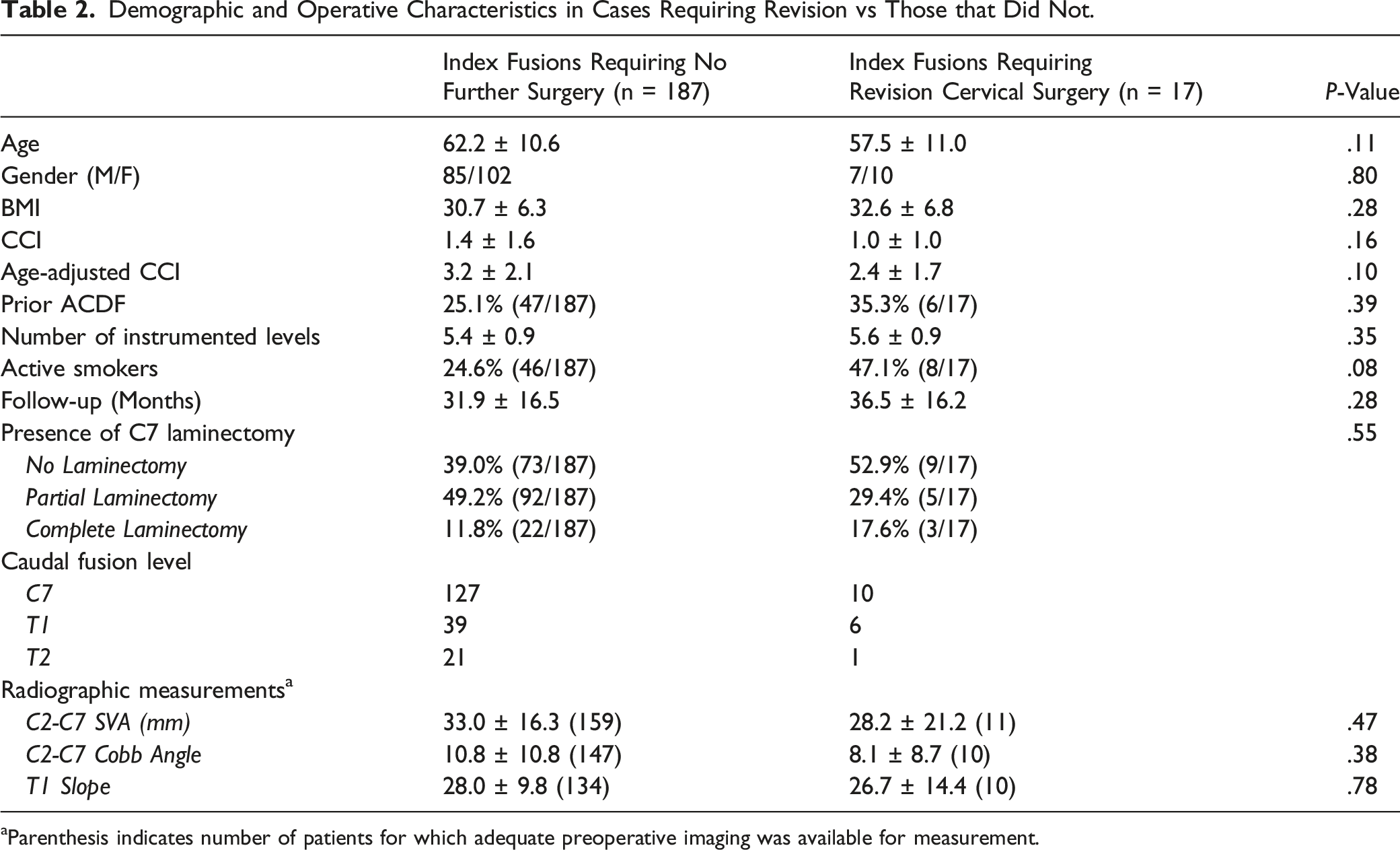
aParenthesis indicates number of patients for which adequate preoperative imaging was available for measurement.
Revision Rates Stratified by Caudal Level of Index Fusion.
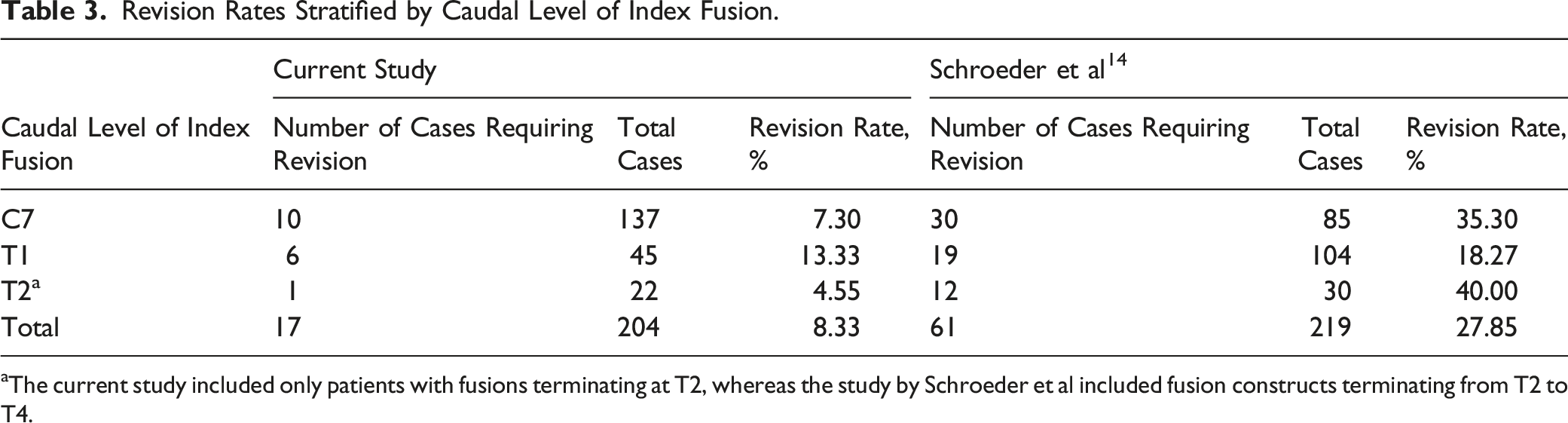
aThe current study included only patients with fusions terminating at T2, whereas the study by Schroeder et al included fusion constructs terminating from T2 to T4.
Multivariate Regression Analysis—Revision Requirement.
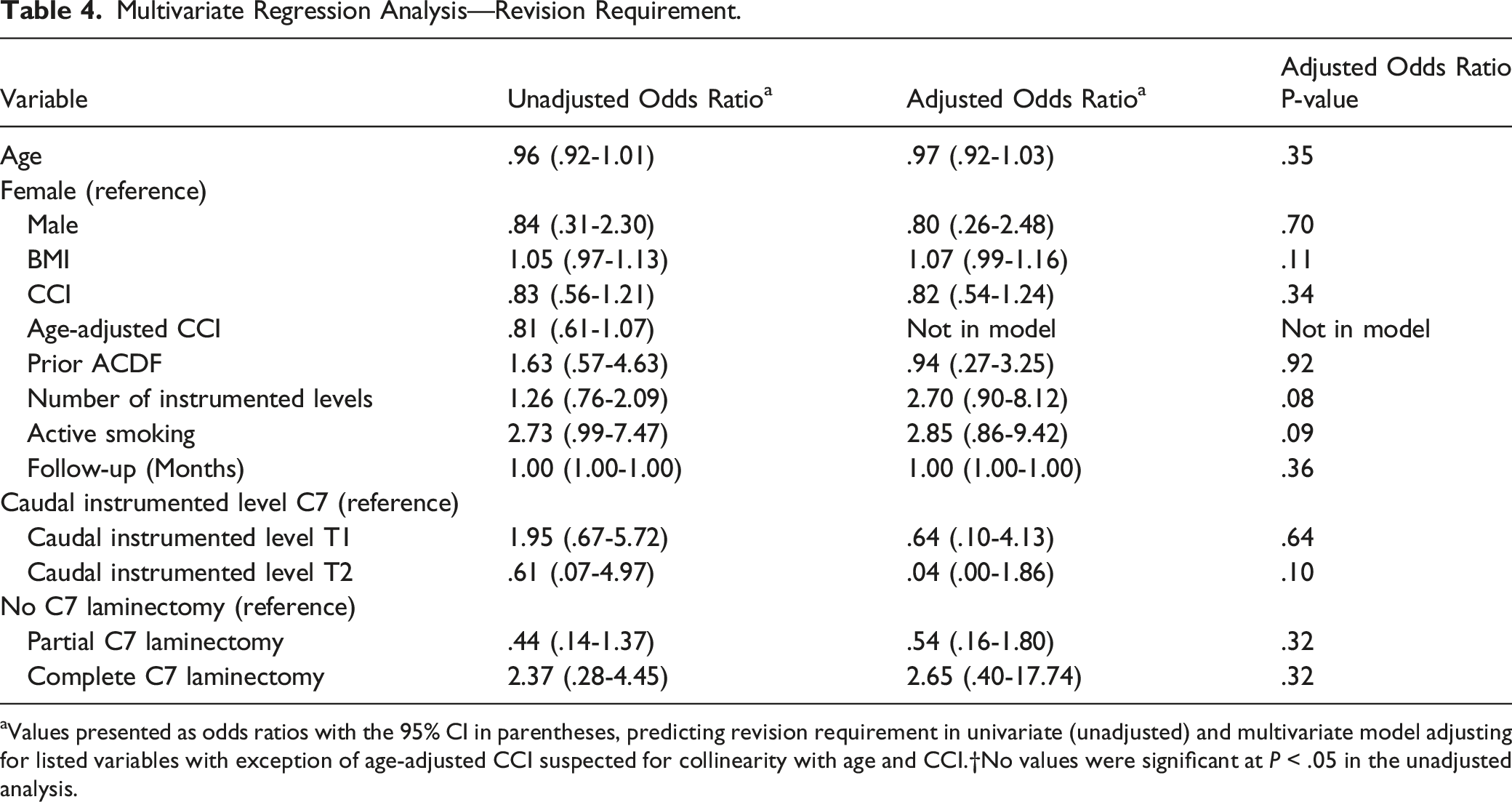
aValues presented as odds ratios with the 95% CI in parentheses, predicting revision requirement in univariate (unadjusted) and multivariate model adjusting for listed variables with exception of age-adjusted CCI suspected for collinearity with age and CCI.†No values were significant at P < .05 in the unadjusted analysis.
Operative Details and Indications for Revision Cases.
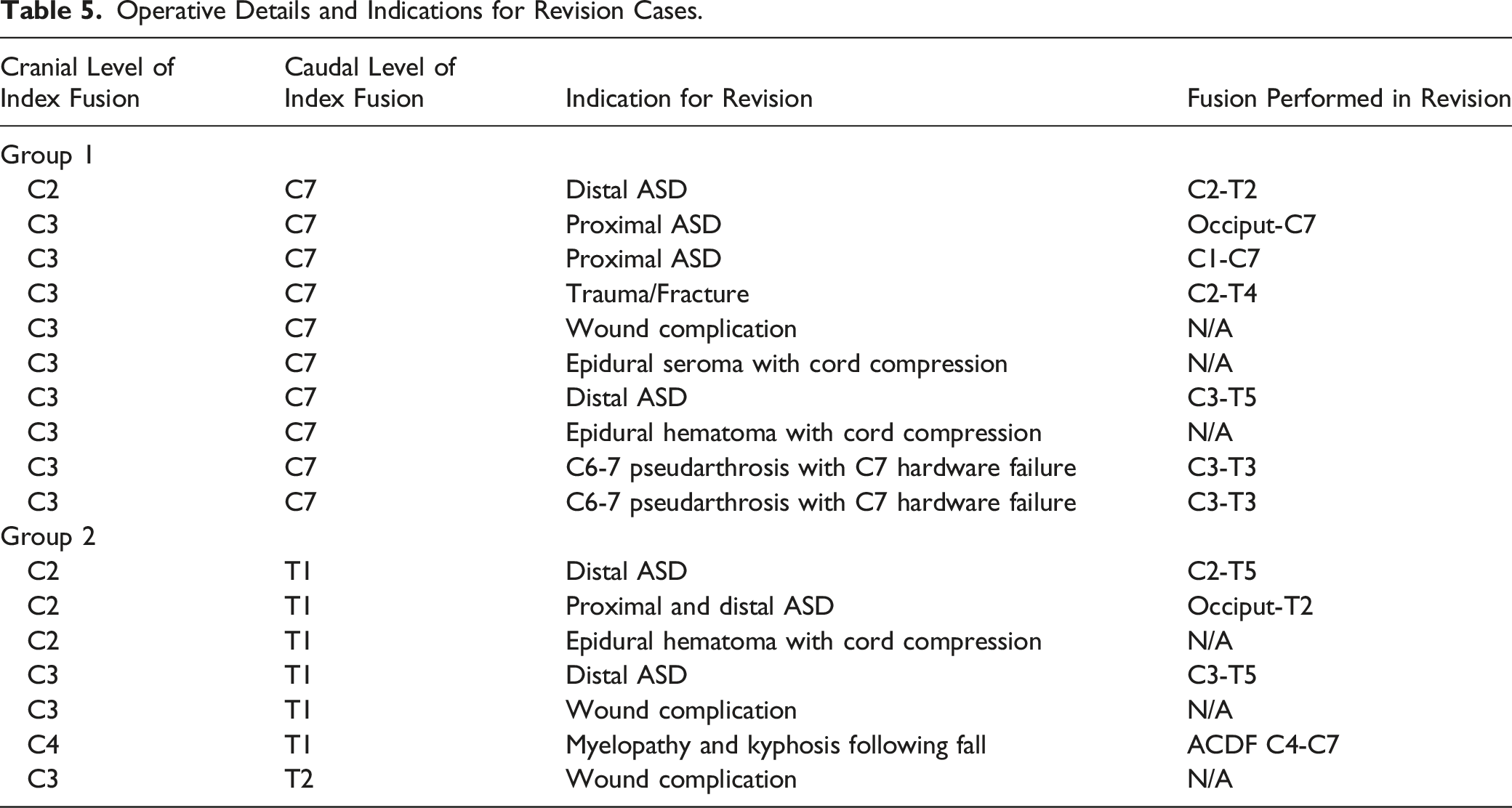
Progressive upper extremity radiculopathy and weakness were the most common presenting symptoms in patients requiring revision for distal ASD, present in 3 of the 4 patients in this cohort. The remaining patient presented with increasing pain at the base of her neck and difficulty keeping her gaze on the horizon. Routine plain radiographs obtained in clinic revealed that she was becoming progressively more kyphotic, prompting revision surgery. Both patients revised for proximal ASD presented with chief complaints of severe pain in their upper cervical spine and the base of their skull. In one case, workup by the neurosurgical service for a pain pump revealed significant ASD, while in the other a repeat CT scan revealed extensive erosive arthritis at C1-C2 prompting extension of the fusion to C1. The patient who was revised for concomitant proximal and distal ASD presented with global upper and lower extremity weakness leading to an inability to ambulate. Both patients with C6-7 pseudarthrosis presented with focal pain in their lower neck that progressed to upper extremity radiculopathy. After failing courses of conservative treatment, advanced imaging was obtained that revealed evidence of pullout of the C7 lateral mass screws. The remaining 2 patients were revised following injuries sustained after incidental traumas. One patient was unfortunately involved in a motor vehicle accident in which he sustained a C7-T1 fracture/dislocation below his fusion construct with associated complete spinal cord injury. The other patient returned to clinic with increasing upper and lower extremity dysfunction after sustaining multiple falls, 1 down a flight of stairs. Repeat imaging revealed cord compression from a large disc herniation with associated kyphotic deformity at C5-C6. This patient required anterior cervical discectomy and fusion to relieve her spinal cord compression and prevent further deformity.
Discussion
This study investigated the impact of crossing the CTJ on revision rates following posterior cervical laminectomy and fusion for degenerative cervical spine disease. The results of the study suggest that there may be no difference in revision rates, and posterior cervical constructs may be safely terminated in the cervical spine without significant increase in need for revision surgery. In fact, patients whose initial construct extended to the thoracic spine showed a higher rate of revision surgery than patients whose construct stopped proximal to the cervicothoracic junction, though this difference was not significant (7.3% vs 10.4%, P=.43). While it is possible that factors influencing the surgeons’ decision to extend the fusion to the thoracic spine (CTJ instability, need for a complete C7 laminectomy, prior ACDF) predisposed this group to failure, the statistically significant differences found in age and prior ACDF rates between the 2 groups is likely not clinically significant. In fact, neither of these variables were identified as risk factors for revision surgery based on univariate analysis, and none of the variables analyzed in this study were identified as risk factors for revision in the multivariate regression.
Previously published reports comparing revision rates in posterior cervical fusions with and without crossing of the CTJ are inconclusive, with reported revision rates ranging from 5.3% to 35.3% in patients whose constructs terminate proximal to the junction.14-18,20-22 The revision rate of posterior cervical constructs terminating proximal to the CTJ was found to be considerably lower in the current study than many reported rates in the literature. In a series of 219 patients who underwent multilevel posterior cervical laminectomy and fusion, Schroeder et al. identified termination of the fusion construct at C7 as a significant risk factor for revision. 14 However, the largest proportion of patients requiring revision in this cohort was seen in the group of patients with fusions terminating at T2-T4 (40% vs 35.3% in the C7 group and 18.3% in the T1 group). Osterhoff et al found that 31% of patients required secondary intervention (22.4% requiring surgical intervention, 5.1% facet joint injection, and 6.9% long-term orthotic treatment) following posterior cervical fusion terminating in the cervical spine. 17 Furthermore, Schroeder et al and Huang et al did not report any occurrences of ASD in cases crossing the cervicothoracic junction, supporting the hypothesis that extending cervical fusion constructs distal to the CTJ may be protective against ASD.14,15 However, the current study found that 42.9% (3/7) of the revisions in cases crossing the CTJ were performed secondary to symptomatic ASD, comparable to the 40% (4/10) of revision cases in the cervical group that were performed for symptomatic ASD. Overall, 4.5% of patients in the thoracic group required reoperation due to ASD, compared to 2.9% in the cervical group. The findings of this series may call into question whether crossing the CTJ indeed protects against development of ASD, traditionally a prominent argument in favor of crossing the cervicothoracic junction.
The findings of the current study suggest that posterior cervical constructs may be terminated in the cervical spine without increased risk of reoperation in patients without spondylolisthesis of C7-T1 and/or need for a complete C7 laminectomy. These results are consistent with those found by Chan et al and Fayed et al, who reported cervical revision rates of 6.1% and 6.3%, respectively.20,21 Multiple other studies have failed to find evidence that extending the fusion to the thoracic spine is advantageous.15,18,23 Truumees et al concluded that routine extension of long posterior cervical fusions into the thoracic spine does not confer significant benefits in terms of revision rates, cervical alignment or patient-reported outcomes at 2-year follow-up. 18 Huang et al reported a similar overall reoperation rate when comparing fusions terminating at C7 to those terminating in the thoracic spine (10.8% vs 9.4%), with a significantly greater incidence of wound dehiscence in the thoracic group (7.8% vs 0%). 15
Determining the safety of terminating posterior cervical constructs proximal to the CTJ is important as spinal fusions involving the CTJ present many distinct treatment challenges, and complications are common following surgical intervention.6-13 Transition from the flexible, lordotic cervical spine to the semi-rigid, kyphotic thoracic spine leads to relative force concentration about the C7-T1 disc space.7,10 Further, decreased size and cortical thickness of the lateral masses in the lower cervical spine reduce overall construct strength and lead to an increased risk of screw pullout and instrumentation failure with the use of lateral mass screws.11,12 C7 pedicle screws may be utilized to increase pullout strength but require accurate imaging and meticulous placement in order to avoid devastating injuries to the spinal cord or vertebral artery.24,25 As such, prior literature has advocated against stopping posterior fusion constructs at C7, instead electing to extend these constructs past the cervicothoracic junction, and thus allowing for safer, stronger fixation via thoracic pedicle screws.14,16,17
However, extending posterior fusion constructs to the thoracic spine has been associated with increased blood loss, operative time, length of stay, and wound complications.15,18 Though the nature of the current study precluded the analysis of post-operative range of motion and patient-reported outcomes, previous research has indicated that cervical fusions crossing the CTJ result in substantial losses in range of motion compared to those ending at C7 19 . In a study of 82 patients following posterior cervical laminectomy and fusion, Bechara et al 19 found that C3-T1 fusion resulted in average losses of 23 of total head flexion/extension, 17o of axial rotation, and 13o of lateral bend when compared to C3-C7 fusion. This corresponded to patients in the C3-T1 fusion group reporting significantly worse NDI scores than patients in C3-C7 fusion group, though the average scores in both groups fell in the “mild disability” category. These results may be extrapolated to the current study as the study population included patients who had previously undergone C3-C7 or C3-T1 posterior fusions for degenerative indications. Given the significant morbidity associated with extension of fusion constructs to the thoracic spine, it is of utmost importance to determine the true risk/benefit profile of crossing the cervicothoracic junction.
Strengths of this study include stringent inclusion criteria resulting in a cohort of patients who underwent exclusively posterior fusions for degenerative indications, the identification of indications for revision in all cases requiring reoperation, and the prospective collection of the database. Limitations of this study include its design as a retrospective review. As with all retrospective studies, this study relied on the accuracy and availability of information present in the electronic medical record. It is possible that the revision rate in this series was underestimated due to patients undergoing revision outside of the authors’ system.
Conclusion
This study shows no evidence of increased risk of revision surgery or ASD in patients with posterior cervical fusion constructs terminating in the cervical spine when compared to patients with constructs crossing the cervicothoracic junction. These findings support prior evidence showing that terminating fusion constructs proximal to the CTJ is a feasible and safe option in posterior cervical fusions in patients without spondylolisthesis at C7-T1 or need for a complete C7 laminectomy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Note
Jeremy Shaw and William Donaldson have received reimbursements for travel and lodging and food and beverage from Stryker within the last 36 months. Emmett Gannon has received reimbursement for food and beverage from Zimmer Biomet, Stryker, Medtronic, Globus, RSW, Nuvasive, and Depuy Synthes within the last 36 months.
Ethics Approval
This study was approved by the IRB at the University of Pittsburgh (IRB#: STUDY19100333).