
Abstract
Study Design
Systematic review and meta-analysis.
Objectives
To assess the radiographic risk factors for adjacent segment disease (ASD) following anterior cervical discectomy and fusion (ACDF) for degenerative cervical spine pathologies.
Methods
PubMed, Embase and the Cochrane Library databases were searched up to December 2023. The primary inclusion criteria were degenerative spinal conditions treated with ACDF, comparing radiological parameters in patients with and without postoperative ASD. The radiographic parameters included intervertebral disc height, cervical sagittal alignment, sagittal segmental alignment, range of motion, segmental height, T1 slope, sagittal vertical axis (SVA), thoracic inlet angle (TIA), and plate to disc distance (PPD). Risk of bias was assessed for all studies. The Cochrane Review Manager was utilized to perform the meta-analysis.
Results
From 7044 articles, 13 retrospective studies were included in the final analysis. Three studies had “not serious” bias and the other 10 studies had serious or very serious bias. The total number of patients in the included studies was 1799 patients. Five studies included single-level ACDF, 2 studies included multi-level ACDF, and 6 studies included single or multi-level ACDF. On meta-analysis, the significant risk factors associated with ASD development were reduced postoperative cervical lordosis (mean difference [MD] = 3.35°, P = .002), reduced last-follow-up cervical lordosis (MD = −3.02°, P = .0003), increased preoperative to postoperative cervical sagittal alignment change (MD = −3.68°, P = .03), and the presence of developmental cervical canal stenosis (Odds ratio [OR] = 4.17, P < .001).
Conclusions
Decreased postoperative cervical lordosis, greater change in cervical sagittal alignment and developmental cervical canal stenosis were associated with an increased risk of ASD following ACDF.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) is a frequent surgical procedure for cervical spine degenerative conditions, with more than 130,000 ACDFs performed yearly in the United States and an annual increase of more than 5%.1-4
Despite its effectiveness in relieving neck pain, radiculopathy, and myelopathy, ACDF is not without short-term and long-term complications. 5 Following ACDF, there is alteration in the cervical spine biomechanics with increased intradiscal pressure and segmental motion at adjacent segments.6,7 These changes contribute to the development of radiographic degenerative changes in the adjacent levels.8,9 Yet, radiographically evident degenerative changes do not necessarily lead to increased symptomatic disease incidence. 10 Adjacent segment disease (ASD) comprises a clinically significant degeneration of the level above or below the fusion area with symptoms of new radiculopathy and/or myelopathy, which may lead to severe dysfunction and the need for reoperation.11,12
The incidence of ASD has been reported in the literature, ranging from 2.9% to 92%, with approximately 40% reoperations after spine surgery.13-15 Notably, these revision surgeries are associated with enormous direct and indirect medical costs. 16
Given this high prevalence and the potential detrimental effects, identification of the pre and perioperative factors linked to ASD could have significant clinical and economic implications.17,18
The risk factors of ASD are still not fully understood, and the findings of different studies have been inconsistent. 19 Up to now, radiographic risk factors for ASD development after ACDF have not been extensively analyzed. Therefore, this systematic review and meta-analysis aimed to identify the radiographic risk factors for ASD occurrence following the management of degenerative cervical spine pathologies with ACDF.
Methods
This systematic review was performed while adhering to the PRISMA statement guidelines. 20
Electronic literature search
PubMed, Embase and the Cochrane Library databases were searched for relevant articles from the commencement to December 2023.
The search terminology included anterior cervical discectomy and fusion or ACDF AND adjacent segment degeneration, adjacent segment disease, adjacent segment failure, proximal junctional failure, proximal junctional disease, distal junctional failure, distal junctional disease, reoperation spine fusion, or extension of fusion.
Studies Selection
Three independent reviewers (Z.B., M.B. and C.Y.) screened the studies for qualification of full-text review. Each article title and abstract were reviewed, and articles that were not relevant to the topic of the study were excluded. Rayyan.ai 21 was used to facilitate the screening and selection process. Full-text evaluation was then performed to choose the studies that matched the criteria for inclusion.
Inclusion and Exclusion Criteria
Inclusion criteria were: (A) Studies that included degenerative spinal conditions requiring ACDF. (B) Articles that compared the radiological parameters in patients with and without postoperative ASD. (C) English articles with available full text. (D) Each comparative group must have at least ten patients.
PICO Table.
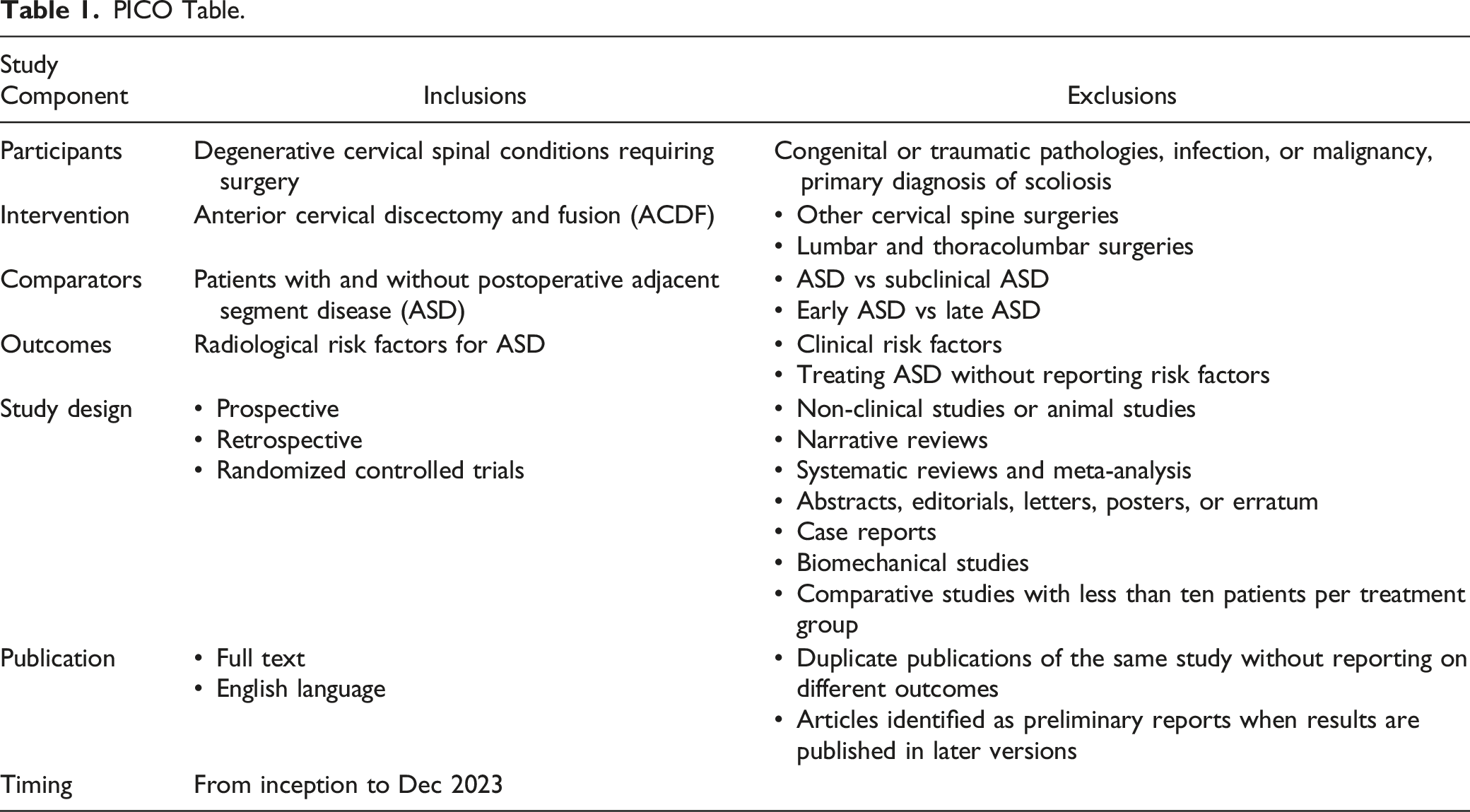
Any disagreement between the reviewers over the inclusion of the studies was resolved by a discussion.
Data Extraction
The following information was obtained and written in a custom-made sheet using Microsoft Office Excel® version 2022 (Microsoft Corporation, Redmond, Washington, United States): authors, study design, demographics, follow-up duration, surgery, number of levels, ASD diagnostic methods and definition, values of each radiographic risk factor for both ASD and No-ASD groups, odds ratio, and P-value. Two reviewers (M.B. and C.Y.) independently extracted data from each study.
Quality Assessment
Two reviewers (M.B. and C.Y) independently evaluated the risk of bias in the included observational studies based on the methodological index for non‐randomized studies (MINORS) checklist. 22 A MINORS score of 17-24 indicated “not serious” bias. A score of 10-16 indicated “serious” bias. A score of 9 or lower indicated “very serious” bias. In a case of a disagreement, the senior reviewer (ZB) reviewed and resolved the points in question.
Outcome Measures
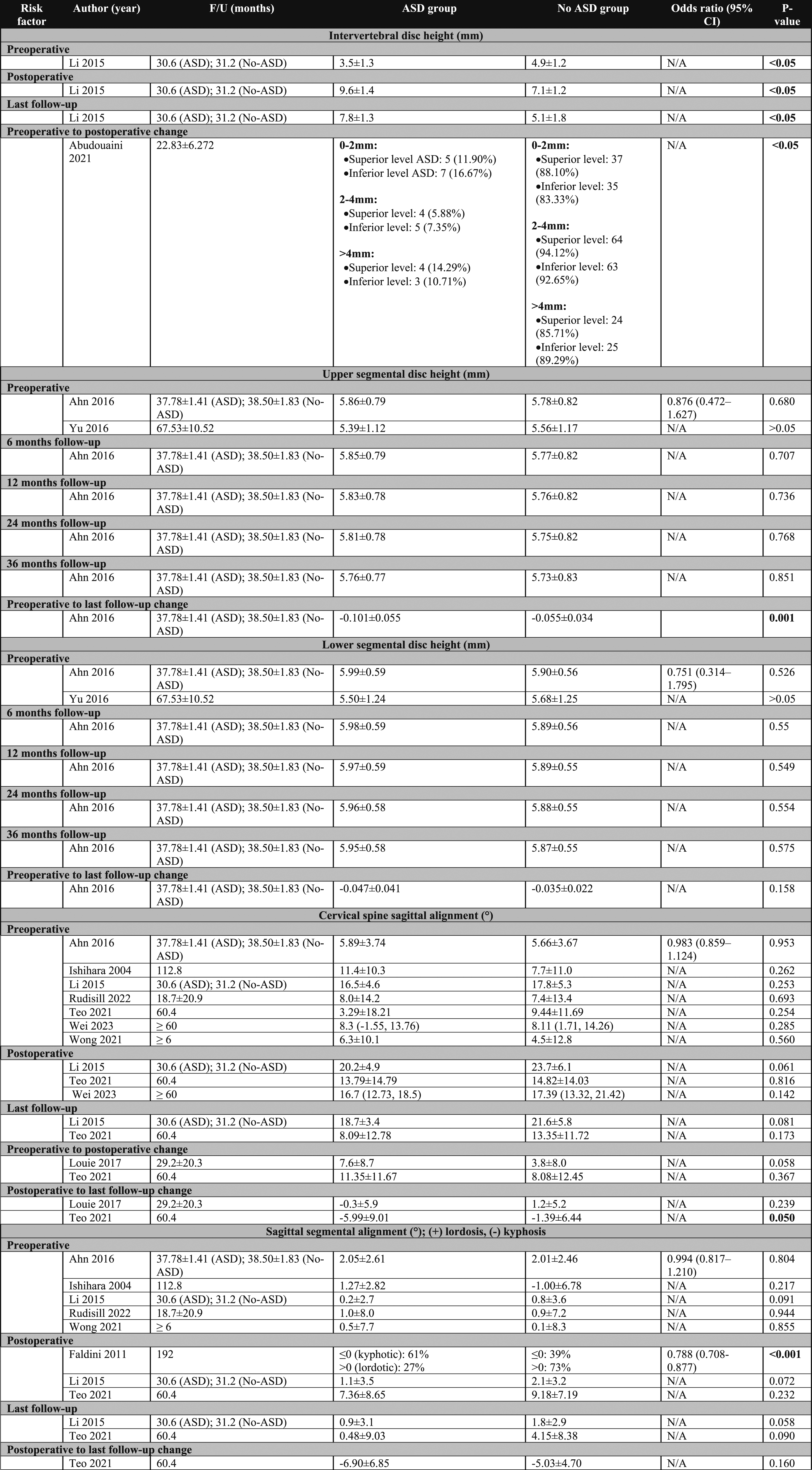
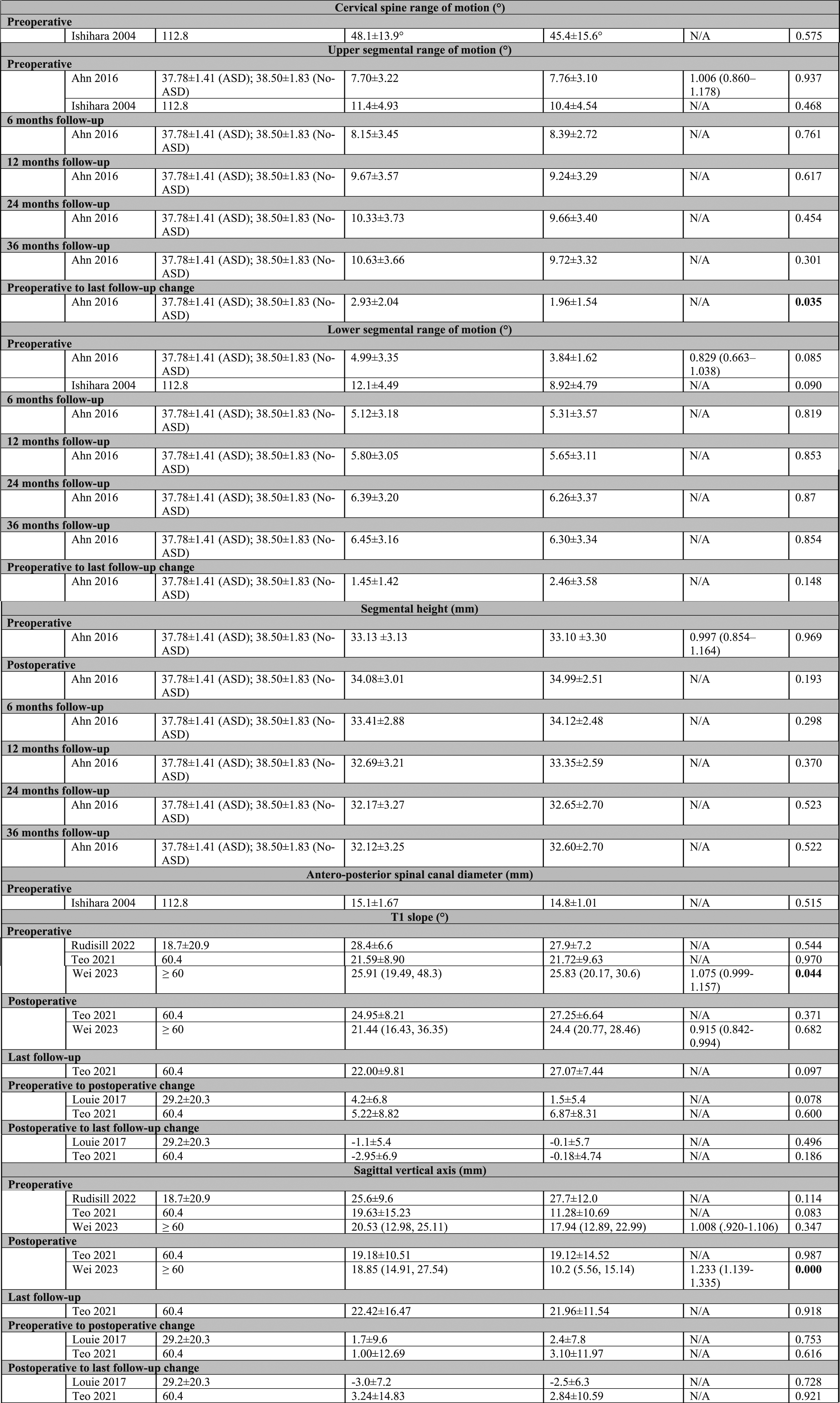
The primary outcome measure was the radiographic risk factors for ASD development after cervical spinal surgeries. The radiographic parameters included intervertebral disc height, cervical sagittal alignment, sagittal segmental alignment, range of motion, segmental height, T1 slope, sagittal vertical axis (SVA), thoracic inlet angle (TIA), and plate-to-disc distance.
statistical Analysis
The Cochrane Review Manager (RevMan V.5), Nordic Cochrane Centre, Copenhagen, Denmark, was Utilized to Perform the Meta-analysis.
Meta-analysis of a specific risk factor was performed if at least two studies reported the value of that risk factor in patients with and without ASD.
In continuous data, the mean difference (MD) and 95% confidence interval (CI) were estimated, whereas the odds ratio (OR) and 95% CI were calculated in dichotomous data.
The statistical heterogeneity was judged using the I2 test. The fixed-effects model was used with I2 values <50%, while the random-effects model was used with I2 values >50%. P-values less than .05 were significant.
Results
Search Results and Study Selection
Database searches and removal of duplicates yielded 7044 unique articles.After the screening of titles and abstracts, 85 studies were selected for full-paper review. Eventually, 13 articles23-35 were considered in the qualitative and quantitative analyses, Figure 1. The PRISMA flow diagram.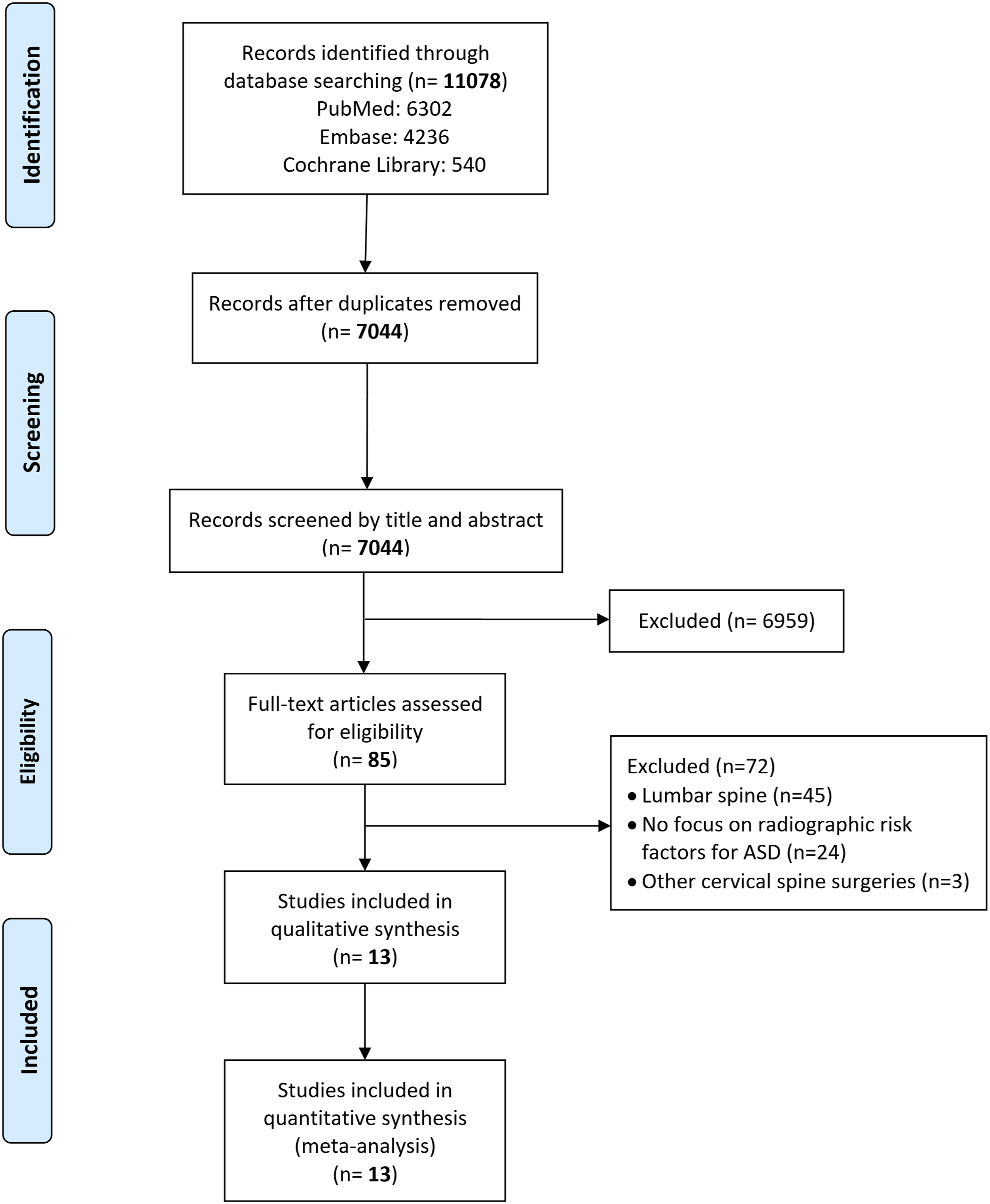
Risk of Bias and Methodological Quality
Methodologic Quality Assessment of the Included Non-randomized Studies Utilizing the Methodological Index for non‐randomized Studies (MINORS) Criteria.
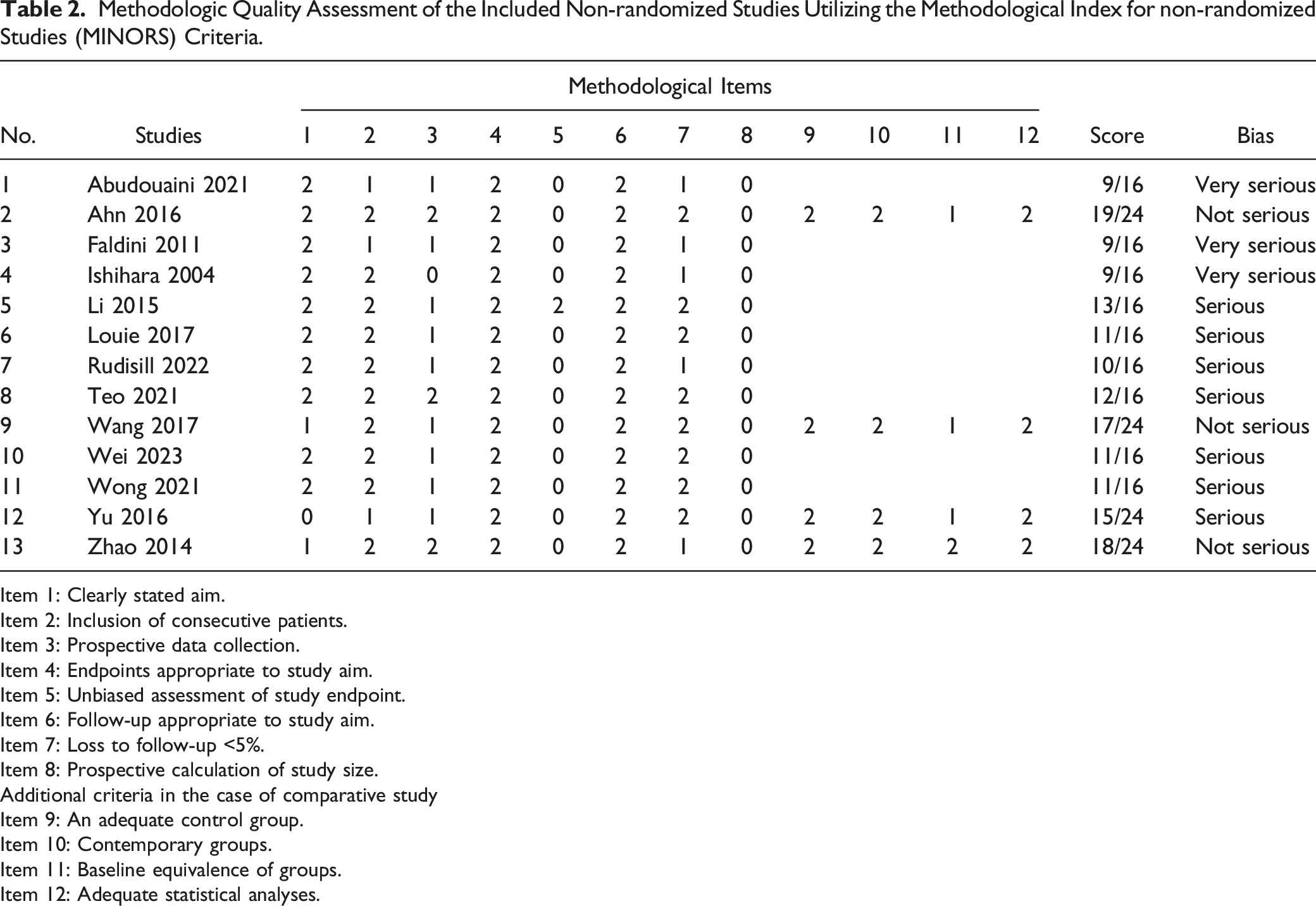
Item 1: Clearly stated aim.
Item 2: Inclusion of consecutive patients.
Item 3: Prospective data collection.
Item 4: Endpoints appropriate to study aim.
Item 5: Unbiased assessment of study endpoint.
Item 6: Follow-up appropriate to study aim.
Item 7: Loss to follow-up <5%.
Item 8: Prospective calculation of study size.
Additional criteria in the case of comparative study
Item 9: An adequate control group.
Item 10: Contemporary groups.
Item 11: Baseline equivalence of groups.
Item 12: Adequate statistical analyses.
Characteristics of Included Studies
All studies23-35 were retrospective. The total number of patients in the included studies was 1788 patients with degenerative cervical spine conditions who had ACDF. Overall, 1034 (57.83%) patients were males, and 754 (42.17%) were females.
In terms of the number of operated levels, 5 studies23-25,27,31 included single-level ACDF, 6 studies26,28,29,32,34,35 included single or multi-level ACDF, and 2 studies30,33 included multiple-level ACDF.
Characteristics of the Included Studies.
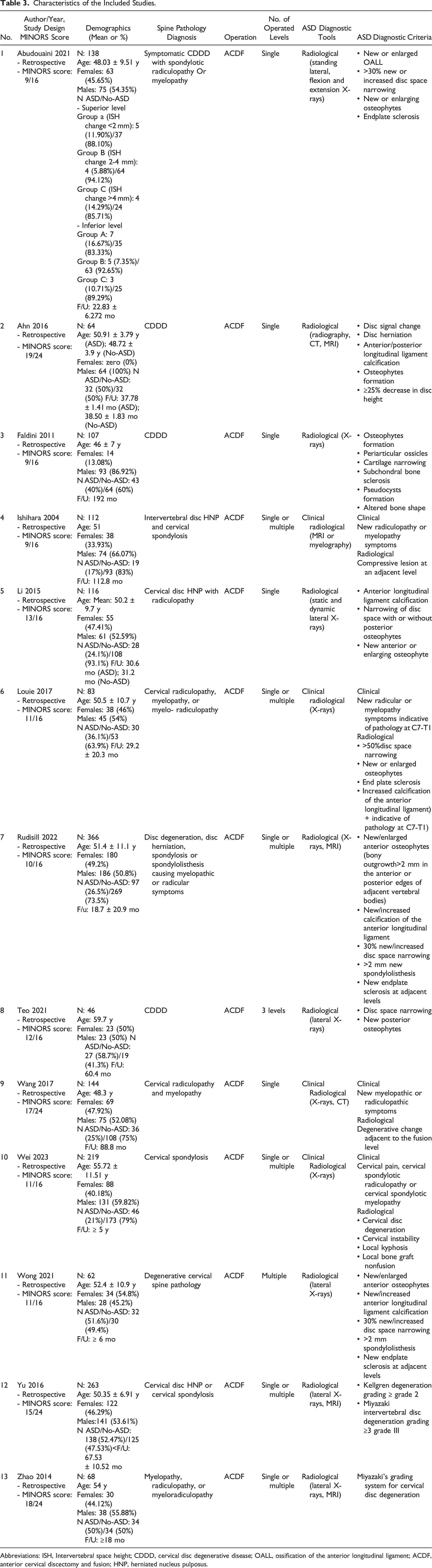
Abbreviations: ISH, Intervertebral space height; CDDD, cervical disc degenerative disease; OALL, ossification of the anterior longitudinal ligament; ACDF, anterior cervical discectomy and fusion; HNP, herniated nucleus pulposus.
Meta-Analysis of Radiographic Risk Factors
Cervical Sagittal Alignment
Six studies24,26,27,29,30,33 were included in the meta-analysis of the preoperative cervical sagittal alignment, which was not different in ASD and No-ASD groups (mean difference [MD] = -.13°; 95% confidence interval [CI] = −1.29 to 1.04; P = .83; I2 = 18%).
However, patients with ASD had significantly lower postoperative cervical lordosis than patients without ASD (MD = −3.35°; 95% CI = −5.43 to −1.27; P = .002; I2 = 0%) on the meta-analysis performed on two studies.27,30
Similarly, patients with ASD had a significantly lower cervical lordosis at the last follow-up time than patients without ASD (MD = −3.02°; 95% CI = −4.65 to −1.40; P = .0003; I2 = 0%).
On meta-analysis from two studies,28,30 the preoperative to postoperative cervical sagittal alignment change was significantly higher in patients with ASD than in patients with no ASD (MD = 3.68°; 95% CI = .34 to 7.03; P = .03; I2 = 0%), while the postoperative to last follow-up cervical sagittal alignment change was insignificantly lower in patients with ASD than patients without ASD (MD = −2.05°; 95% CI = −4.25 to .15; P = .07; I2 = 40%), Figure 2. Forest plots of meta-analysis of cervical spine sagittal alignment.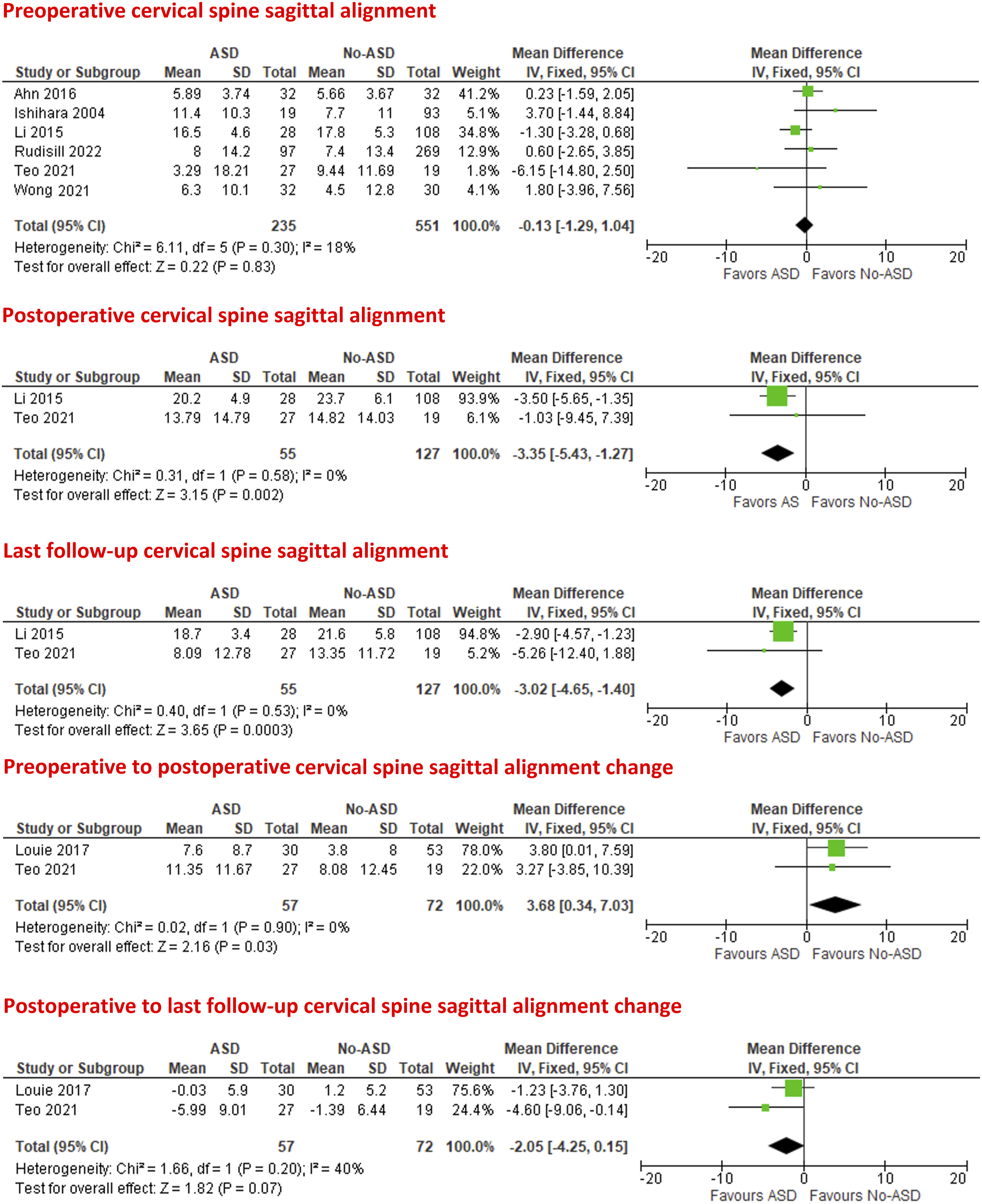
Sagittal Segmental Alignment
Five studies24,26,27,29,33 were included in the meta-analysis of the preoperative sagittal segmental alignment, which was found to be comparable in patients with and without ASD (MD = .16°; 95% CI = −.55 to .87; P = .66; I2 = 38%).
Two studies27,30 evaluated the postoperative and last follow-up sagittal segmental alignment. Both postoperative and last follow-up sagittal segmental alignment were lower in patients with ASD than patients without ASD with no statistical significance (MD = −1.07°; 95% CI = −2.44 to .29; P = .12; I2 = 0%) (MD = −1.06°; 95% CI = −2.30 to .17; P = .09; I2 = 7%), respectively, Figure 3 Forest plots of meta-analysis of the sagittal segmental alignment.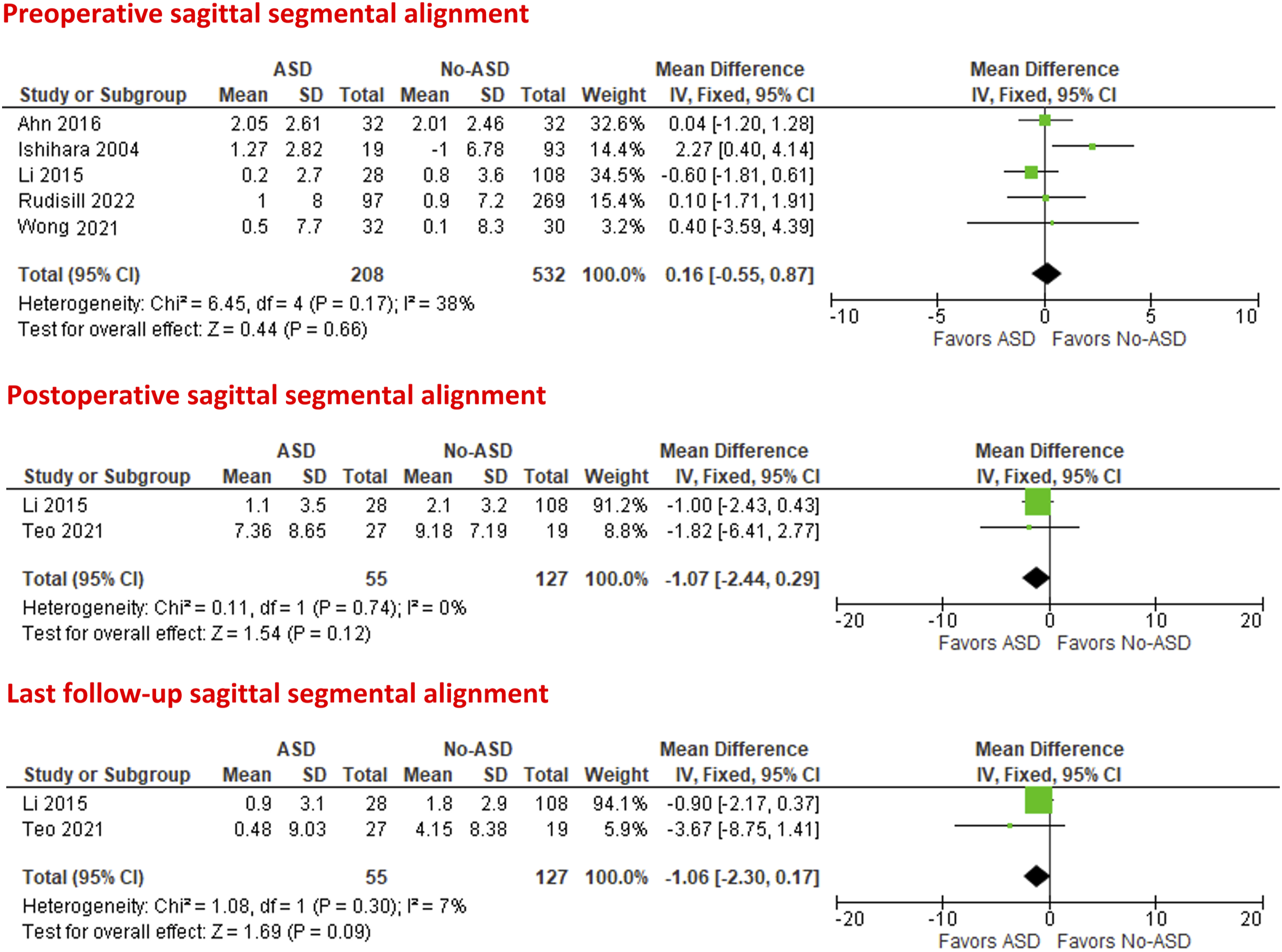
Upper and lower segmental range of motion
Meta-analysis of the preoperative upper and lower segmental range of motion was feasible in two studies.24,26
The preoperative upper segmental range of motion was comparable in patients with and without ASD (MD = .25°; 95% CI = −1.05 to 1.55; P = .70; I2 = 0%). The preoperative lower segmental range of motion was higher in patients with ASD (MD = 1.95°; 95% CI = .01 to 3.89; P = .05; I2 = 58%), Figure 4. Forest plots of meta-analysis of the preoperative upper and lower segmental range of motion.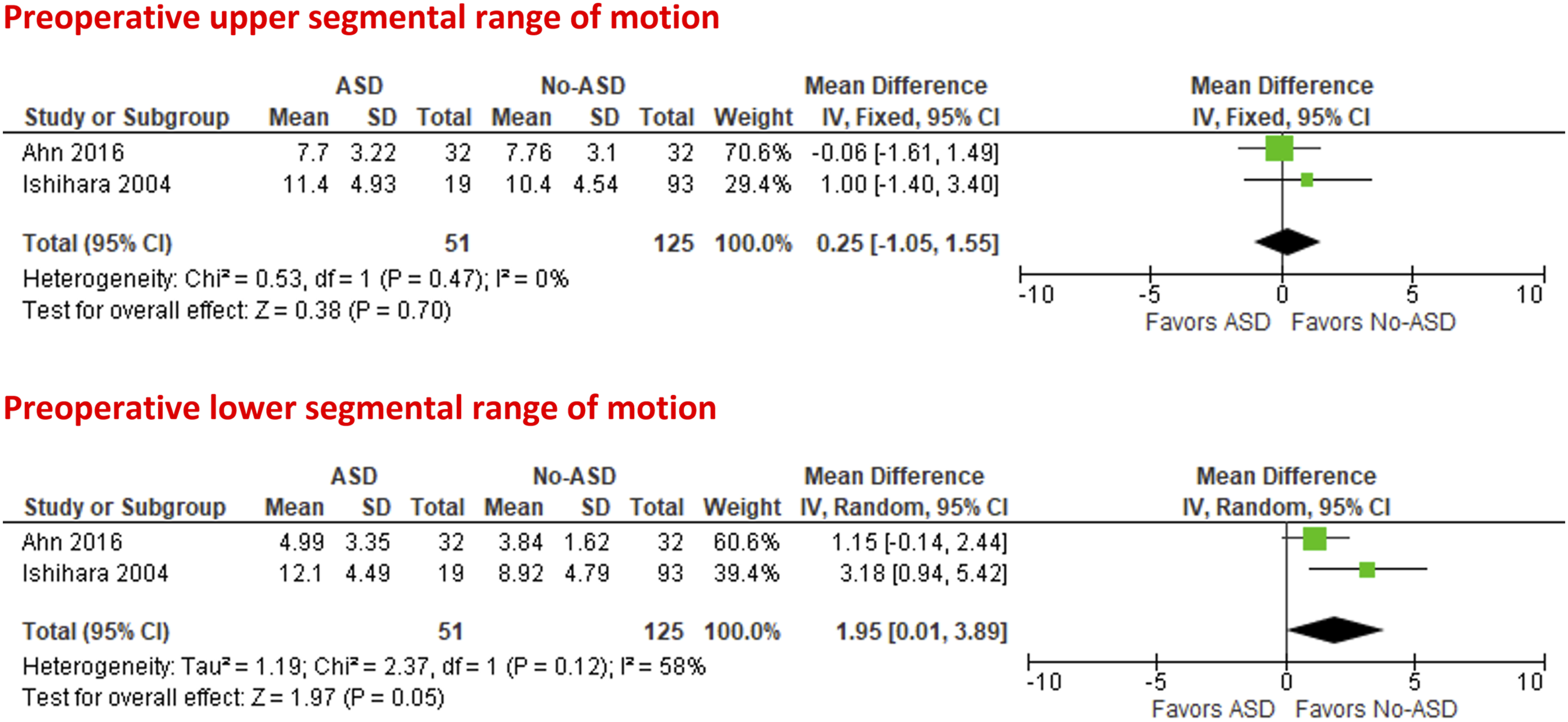
T1 Slope
On meta-analysis from two studies,29,30 the preoperative T1 slope was comparable in patients with and without ASD (MD = .45°; 95% CI = −1.06 to 1.95; P = .56; I2 = 0%).
With pooled data from two studies,28,30 the preoperative to postoperative T1 slope change was higher in patients with ASD but without statistical significance (MD = 1.03°; 95% CI = −3.11 to 5.18; P = .63; I2 = 55%). Additionally, the postoperative to last follow-up T1 slope change was lower in patients with ASD without statistical significance (MD = −1.62°; 95% CI = −3.61 to .37; P = .11; I2 = 0%), Figure 5. Forest plots of meta-analysis of T1 slope.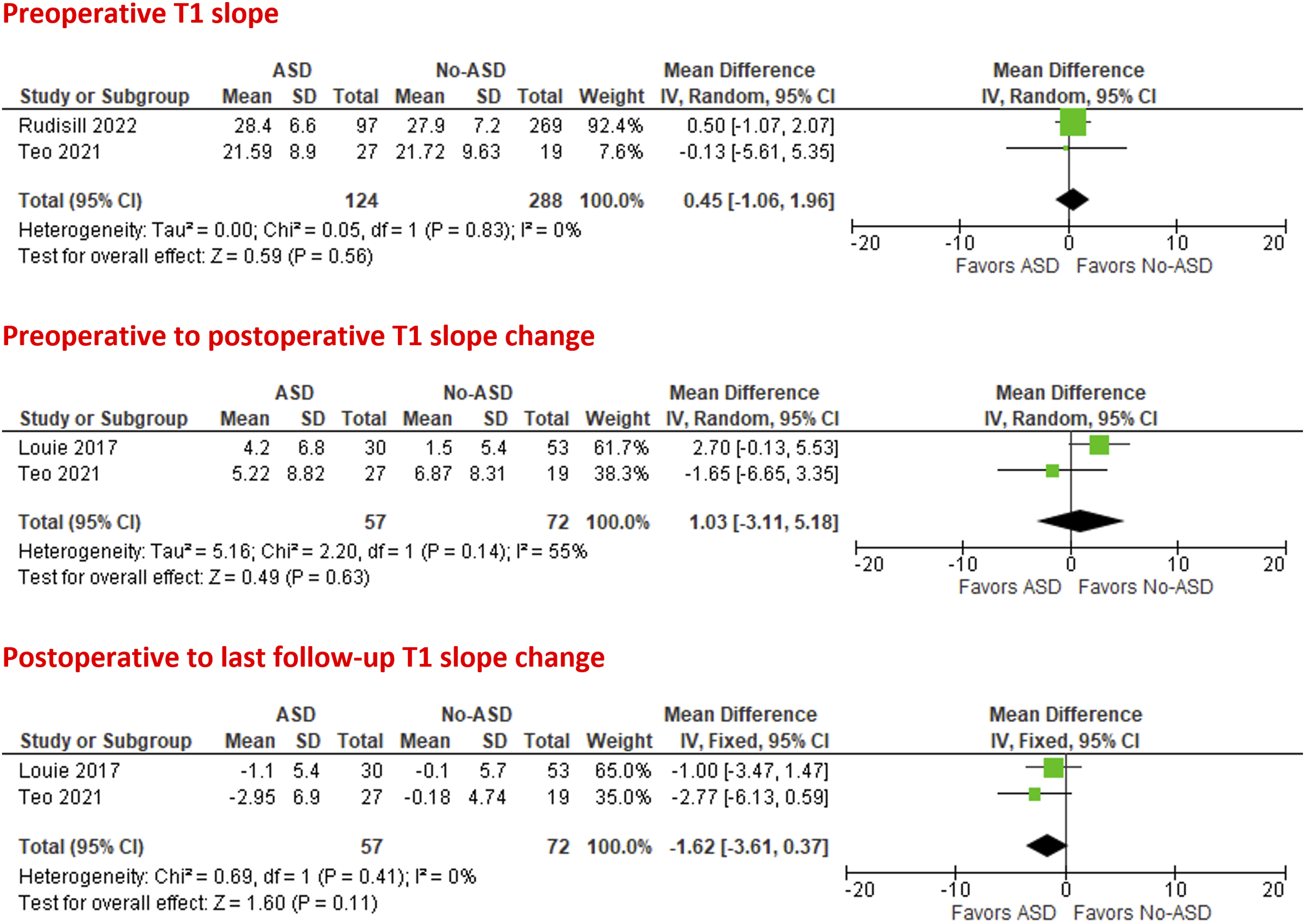
Sagittal Vertical Axis
On meta-analysis from two studies,29,30 the preoperative sagittal vertical axis was non-significantly higher in patients with ASD than patients without ASD (MD = 2.50 mm; 95% CI = −7.67 to 12.66; P = .63; I2 = 85%).
With pooled data from two studies,28,30 both preoperative to postoperative and postoperative to last follow-up sagittal vertical axis changes were lower in patients with ASD than in patients without ASD with no statistical significance (MD = −1.03 mm; 95% CI = −4.55 to 2.48; P = .56; I2 = 0%) and (MD = −.37 mm; 95% CI = −3.21 to 2.48; P = .80; I2 = 0%), respectively, Figure 6. Forest plots of meta-analysis of sagittal vertical axis.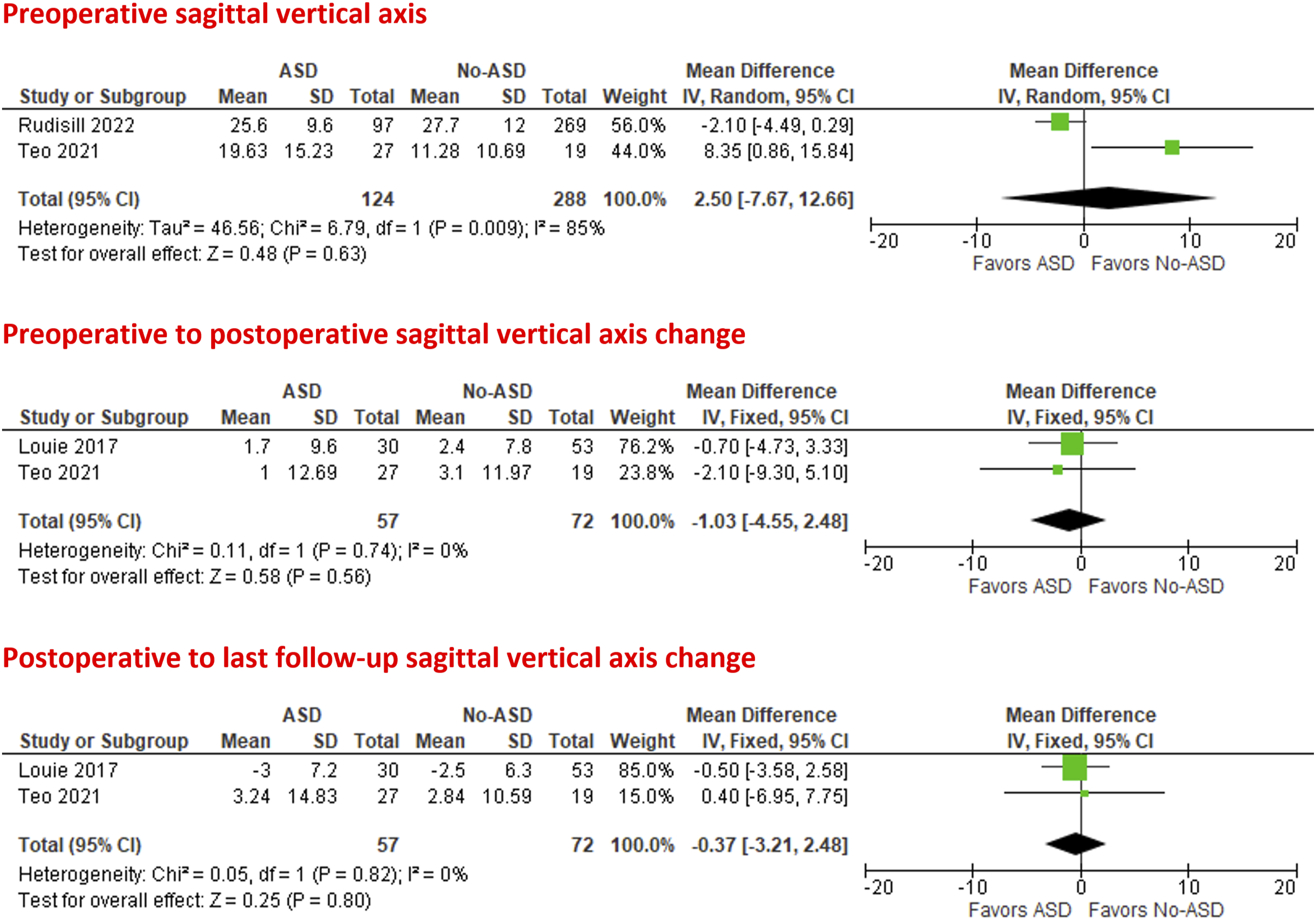
Proximal and Distal Adjacent Segment Lordosis
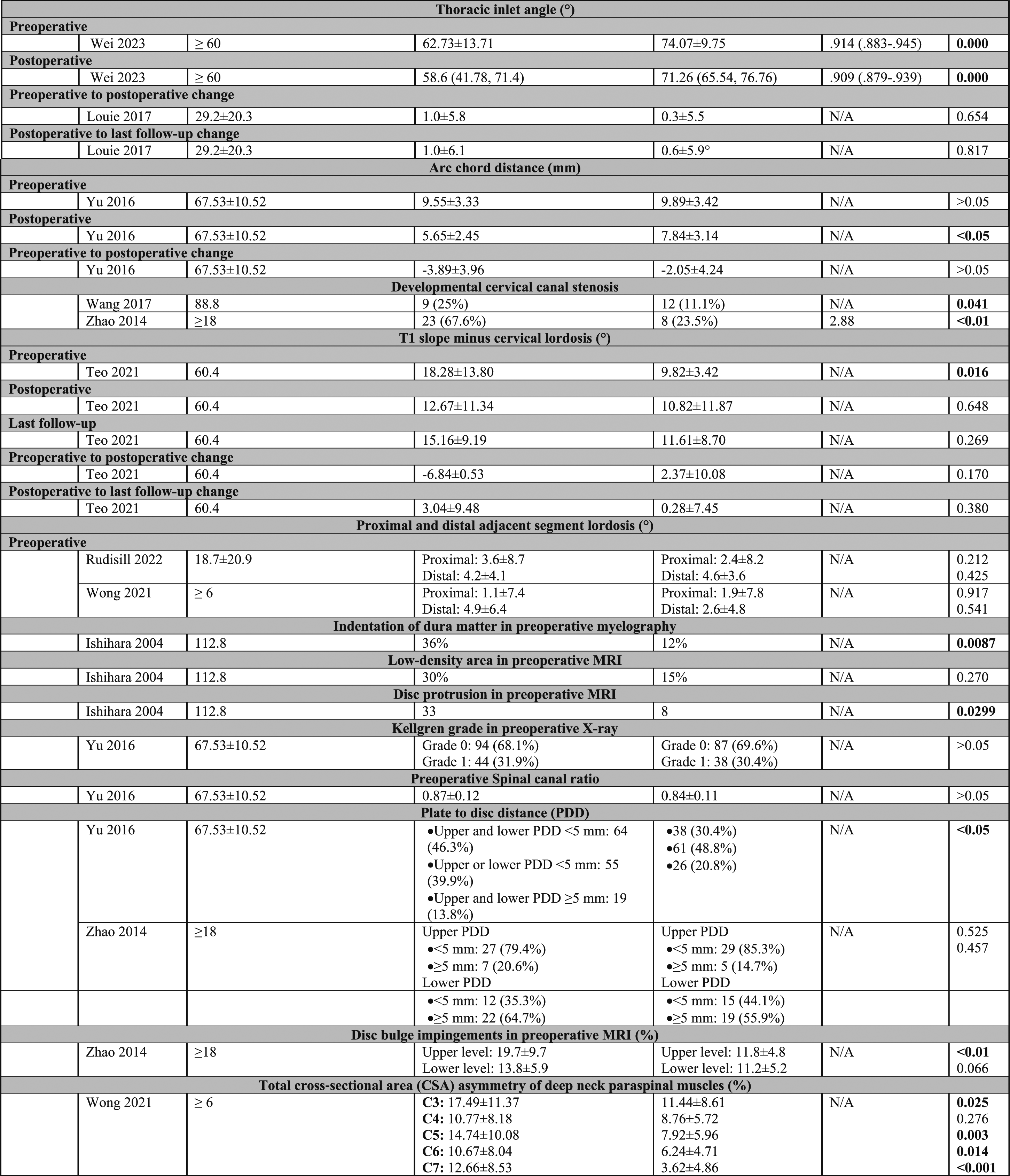
Two studies29,33 were included in the meta-analysis of the preoperative proximal and distal adjacent segment lordosis, which was found to be comparable in patients with and without ASD (MD = .77°; 95% CI = −.99 to 2.53; P = .39; I2 = 0%) and (MD = .61°; 95% CI = −1.95 to 3.17; P = .64; I2 = 69%), respectively, Figure 7. Forest plots of meta-analysis of the preoperative proximal and distal adjacent segment lordosis.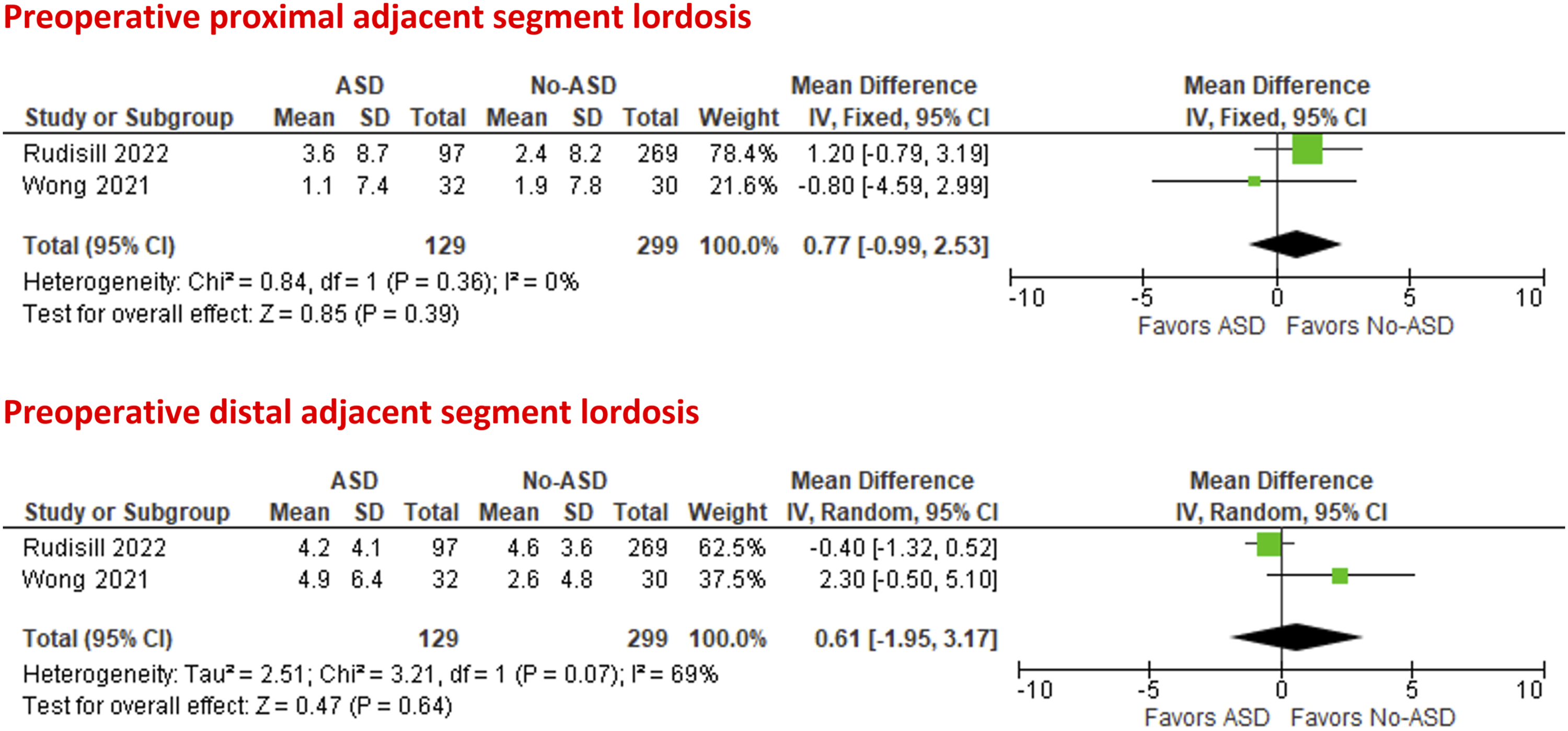
Upper and lower segmental disc height
Two studies24,34 were included in the meta-analysis of the preoperative upper and lower adjacent segmental disc height, which was to be comparable in patients with and without ASD (MD = −.09 mm; 95% CI = −.31 to .14; P = .45; I2 = 3%) and (MD = −.04 mm; 95% CI = −.24 to .17; P = .73; I2 = 39%), respectively.
Developmental Cervical Canal Stenosis
Pooled data from two studies31,35 showed that a diagnosis of developmental cervical canal stenosis significantly increases the odds of ASD development (OR = 4.17; 95% CI = 2.08 to 8.38; P < .001; I2 = 39%), Figure 8. Forest plots of meta-analysis of preoperative adjacent segmental disc height and developmental cervical canal stenosis.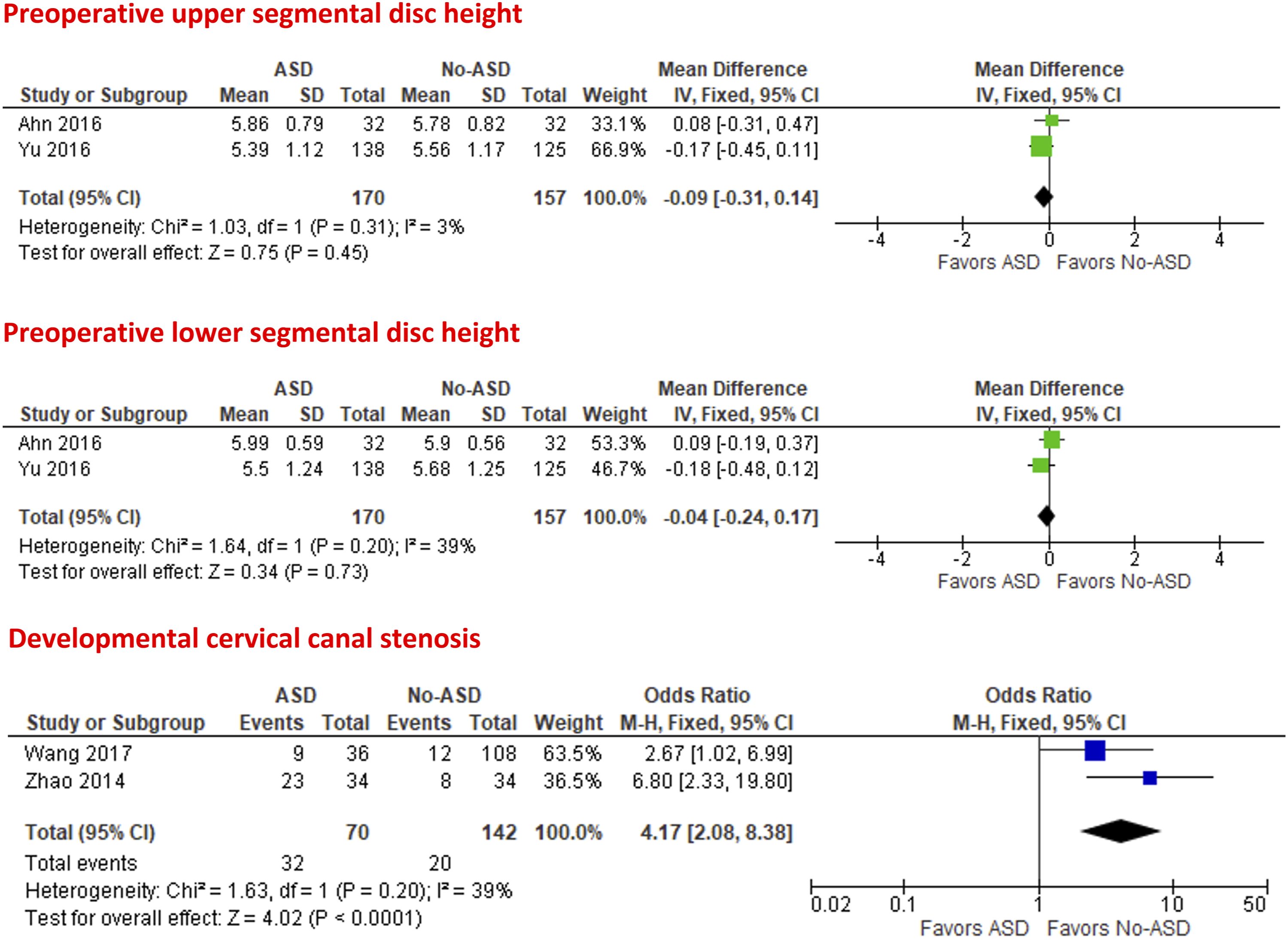
Other Risk Factors
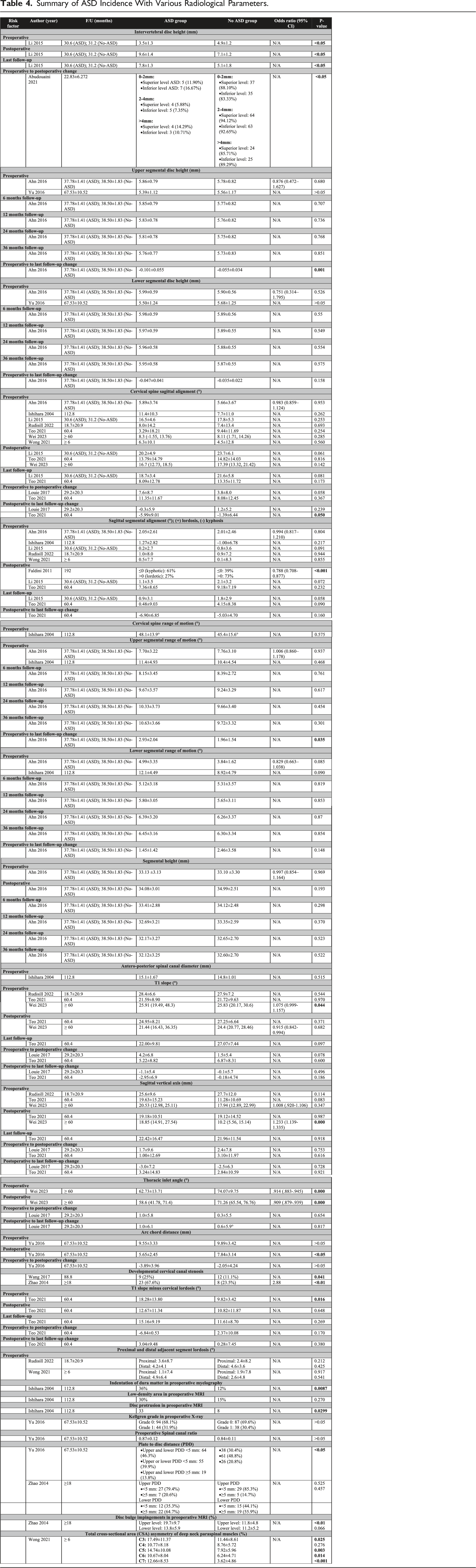
Summary of ASD Incidence With Various Radiological Parameters.
Discussion
ACDF is an effective procedure for addressing degenerative diseases of the cervical spine; however, some patients may develop ASD due to the increased stress on the levels above or below the fused segments.11,36,37 This may lead to a progressive worsening of symptoms with a possible need for revision surgery.36,38
This systematic review and meta-analysis focused on investigating the radiographic parameters as possible risk factors for ASD development following ACDF. Overall, the significant risk factors included lower postoperative and last follow-up cervical lordosis, higher preoperative to postoperative cervical spine sagittal alignment change, and the presence of developmental cervical canal stenosis.
Li et al 27 compared the preoperative and follow-up cervical sagittal alignment of patients with degenerative changes and straightening or kyphosis of the cervical spine who underwent an ACDF and found that the surgery was effective in correcting the cervical sagittal misalignment. However, the ASD group maintained a smaller sagittal alignment angle. 27 Teo et al 30 found that both ASD and non-ASD groups had a gradual decrease in mean cervical sagittal alignment over the course of postoperative follow-ups. However, there was a more significant deterioration in patients who developed ASD. 30 In addition, upon analyzing radiographs from the study, it was observed that an increase in cervical kyphosis often led to the development of ASD. 30 Their findings corroborate the hypothesis that sagittal imbalance after a cervical fusion abnormally distributes stress and predisposes the adjacent segment to an increased rate of degeneration. 11 Similarly, in a biomechanical study using cadaveric specimens, Patwardhan et al 39 concluded that cervical sagittal imbalance exacerbates the mechanical load and degeneration on the levels adjacent to cervical multilevel fusions.
Two studies28,30 reported that change of cervical sagittal alignment between preoperative and postoperative was significantly higher in patients with ASD in comparison to patients without ASD. Louie et al 28 found that patients who required a greater correction in cervical sagittal alignment had an increased risk of radiographic ASD, likely due to a greater change in the distribution of stress.
Ahn et al. 24 and Ishihara et al 26 reported that the preoperative range of motion at the upper adjacent level was not different between the ASD and No-ASD groups. Yet, a meta-analysis of the two studies24,26 found that preoperative lower segmental range of motion was higher in patients with ASD. This finding needs to be further investigated in future meta-analysis studies, including more studies, given that the P-value was exactly .05.
Congenital cervical canal stenosis impacts the cervical kinematics with increased mechanical loading, and degenerative disc disease may be associated with a cervical spinal canal diameter of less than 13 mm. 40
Current meta-analysis revealed that a diagnosis of developmental cervical canal stenosis significantly increased the chances of developing ASD. Wang et al 31 and Zhao et al 35 found that developmental cervical canal stenosis was a significant risk factor for ASD following ACDF. Morishita et al 40 reported that congenital stenosis impacts cervical kinematics with increased mechanical loading, and that degenerative disc disease may be associated with a cervical spinal canal diameter of less than 13 mm. Zhang et al 41 concluded that congenital stenosis is a predictor of radiographic ASD following ACDF.
Several significant radiographic risk factors for ASD were identified, for which a meta-analysis could not be conducted. However, the association between these factors and ASD development is still uncertain and future studies are needed to investigate the interplay between these factors and the risk of ASD. For example, Yu et al 34 reported that a PDD of <5 mm was a significant risk factor for ASD. The use of longer plates in ACDF reduces the PPD, which may increase cervical spine stiffness during motion and exert undue stress on the adjacent segments. 34
Wei et al 32 reported that decreased preoperative and postoperative TIA was a risk factor for ASD. The TIA is an important parameter of the cervical spine sagittal balance since the upper endplate of the T1 vertebra forms the base of the cervical spine. 42
Wong et al 33 found that increased asymmetry in the preoperative total CSA of deep neck paraspinal muscles at C3, C5, C6, and C7 significantly contributed to the risk of ASD development. Improvement of the paraspinal neck muscle condition and function preoperatively may reduce the incidence of ASD, but future studies are needed in this regard, given the limited evidence.
The current study findings have clinical implementations, and future research should focus on the impact of addressing the identified modifiable risk factors for ASD development. These risk factors may alter the distribution of stress in the cervical spine, thus predisposing the vertebral levels above and below the fused segment to quicker deterioration.7,37 Yet, it remains unclear whether ASD is the result of raised mechanical stress on adjacent levels, a natural continuing process of degeneration, or a combination of the two factors. 26
This study has some limitations. First, all the included studies were retrospective in nature. Second, only three out of thirteen studies had “not serious” methodological bias, providing limited evidence for the identified risk factors. Third, preoperative diagnosis, number of operated levels, and the definition of ASD were inconsistent among the included studies. Fourth, single included studies reported significant radiographic risk factors for ASD development, but we could not perform a meta-analysis due to insufficient data.
Conclusion
This study found that decreased postoperative cervical lordosis, greater change in preoperative to postoperative cervical sagittal alignment, and developmental cervical canal stenosis are associated with an increased risk of developing ASD following ACDF.
Footnotes
Acknowledgments
This study was organized by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine degenerative experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.