
Abstract
Study Design
Systematic Review and Meta-Analysis.
Objectives
This study aimed to evaluate the clinical and radiological outcomes of surgically treated adjacent segment disease (ASDis) following ACDF with either anterior plate construct (APC) or stand-alone anchored spacers (SAAS).
Method
Multiple databases were searched until December 2022 for pertinent studies. The primary outcome was health-related quality of life outcomes [JOA, NDI, and VAS], whereas, the secondary outcomes included operative characteristics [estimated blood loss (EBL) and operative time (OT)], radiological outcomes [C2-C7 Cobb angle, disc height index (DHI) changes, fusion rate], and complications.
Results
A total of 5 studies were included, comprising 210 patients who had been surgically treated for cervical ASDis. Among them, 113 received APC, and 97 received SAAS. Postoperative dysphagia was significantly higher in the APC group [47% vs 11%, OR = 7.7, 95% CI = 3.1-18.9, P < .05]. Similarly, operative time and blood loss were higher in the APC group compared to the SAAS group; [MD = 16.96, 95% CI = 7.87-26.06, P < .05] and [MD = 5.22, 95% CI = .35 - 10.09, P < .05], respectively. However, there was no difference in the rate of prolonged dysphagia and clinical outcomes in terms of JOA, NDI, and VAS. Furthermore, there was no difference in the radiological parameters including the C2-7 Cobb angle and DHI as well as the fusion rate.
Conclusion
Our meta-analysis demonstrated that both surgical techniques (APC and SAAS) are effective in treating ASDis. However, with low certainty of the evidence, considering patients are at high risk of dysphagia following revision cervical spine surgery SAAS may be the preferred choice.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) was first introduced by Robinson and Smith 1 and Cloward 2 in 1950’s. It is one of the most commonly performed cervical spine procedures 3 and has been proven to be a safe and effective surgical technique in the treatment of a variety of cervical disorders including spondylotic myelopathy or radiculopathy, disc herniation, and cervical fractures.4,5 Although it has an excellent safety profile and remarkable short- and long-term clinical outcomes, a few drawbacks remain. One well-described complication of ACDF is adjacent segment degenerative changes, which can be asymptomatic (adjacent segment degeneration; ASD), or symptomatic (adjacent segment disease; ASDis). 6 Hilibrand et al reported in a 10-year follow-up study that the incidence of adjacent segment disease is 2.9% per year, with up to one-third of patients having ASDis 10 years after the index surgery. 7 The reported risk of ASDis requiring surgery ranges from 2.9 to 5.6% with annual incidence ranging from .4 to .8%.8,9
The majority of ASDis surgical treatments require decompression and fusion, 10 either through anterior or posterior approach. The fusion component in the anterior approach can be achieved with a stand-alone cage (SAC), anterior plate construct (APC), or stand-alone anchored spacers (SAAS). The SAC technique includes discectomy and cage or bone graft insertion without anterior plating, whereas the APC technique includes anterior plating in addition to cage or graft insertion. The anterior plating in APC has been shown to increase stability, improve cervical lordosis, increase the likelihood of fusion, and decrease graft or cage subsidence.11-14 APC surgery for ASDis after ACDF necessitates the exchange of a previously placed plate with a new one, which may entail additional soft tissue dissection, increasing surgical time, blood loss, and the risk of postoperative dysphagia. By contrast, SAAS involves inserting an interbody spacer that is secured to the cranial and caudal vertebral bodies with integrated fixation instead of anterior plating. This system is low-profile, originally designed as an alternative to traditional ACDF (APC) to reduce dysphagia while also achieving the advantages of anterior plating by increasing the construct stability and fusion rate.15-18
To date, the literature on APC vs SAAS for the treatment of ASDis after ACDF is debatable, and no systematic reviews have summarized the use of APC vs SAAS to treat ASDis. The purpose of this study was to compare the clinical and radiological outcomes of surgically treated ASDis following ACDF with APC vs SAAS in the literature. We hypothesize that there is no significant difference in outcomes and complication rates between patients treated with APC vs those treated with SAAS.
Method
Literature Search Strategy
A systematic review and meta-analysis of relevant comparative studies based on the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines were performed. 19 A systematic search was conducted to identify relevant studies using PubMed, Google Scholar, and the Cochrane database along with a manual search of references listed in included studies and relevant reviews from inception till December 2022. The search strategy included Mesh subject headings combined with relevant keywords “adjacent segment disease”, “stand-alone”, “treatment” and “ACDF”.
Study Eligibility Criteria
Inclusion criteria were studies (1) comparing SAAS and ACP in the treatment of ASDis; (2) whether retrospective, prospective, or cohort; (3) reporting at least one of the clinical and/or radiological outcomes; (4) follow-up of at least 6 months; and (5) published in the English literature. Exclusion criteria were studies that were (1) duplicate publications; (2) nonhuman in vivo and in vitro studies; or (3) reviews, case reports, protocols, and editorial letters.
Assessment of Quality and Certainty of the Evidence
The risk of bias in nonrandomized studies of intervention (ROBINS-I) tool was used for assessing the risk of bias in the involved publications. 20 It includes a risk of bias due to confounding factors, selection of participants for the study, measurement of interventions, missing data, measurement of outcomes, and selection of the reported results. Each of these domains could be rated as: ‘low risk’, ‘moderate risk’, ‘serious risk’, ‘critical risk’, or ‘no information’. All components must be rated as at low risk of bias for the overall study to be rated as at low risk. If there is no component with serious or critical risk, moderate risk in at least one component is enough to rate the study as at moderate risk of bias.
The GRADE approach (Grading of Recommendations Assessment, Development, and Evaluation Working Group) was used to assess the certainty of the evidence for outcomes, and a summary of findings table was created using the GRADEpro GDT software (McMaster University, ON, Canada). 21 The GRADE approach assesses the certainty of evidence based on five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias, and accordingly classifies the certainty of the evidence as high, moderate, low, or very low.
Data Extraction
Two reviewers extracted data independently, and any disagreements were resolved through consensus discussion. The following information was retrieved: study characteristics (authors’ names, country, year of publication, and level of evidence), participants’ demographic characteristics (sample size, age, sex, and follow-up time), and relevant outcomes parameters including functional outcomes (Japanese Orthopedic Association Score (JOA), visual analog score (VAS), and neck disability index (NDI)), operative characteristics (operative time (OT), and estimated blood loss (EBL)) radiological outcomes (disc height index (DHI), C2-7 Cobb angle, and fusion rate), and complications (post-operative dysphagia, revision rate, and cage subsidence)
Statistical and Data Analysis
Meta-analysis was performed using a random-effect model with the Comprehensive Meta-analysis Software version 3.3 (Biostat Inc., NJ, USA,). 22 Mean difference or standardized mean difference and 95% confidence interval (CI) were calculated for continuous variables, while odds ratio (OR) and 95% CI were calculated for dichotomous variables. Heterogeneity across studies was assessed using I2 statistics, which estimate the percentage of variability in effect estimates caused by heterogeneity rather than chance. 23 If the value is less than 25%, it indicates low heterogeneity. Values of 50% and 75%, respectively, indicate moderate and high levels of heterogeneity. 24 We used the weighted mean difference (WMD) to describe the data as JOA, NDI, and VAS are continuous outcomes expressed at baseline and last follow-up time points.25,26
Results
Literature Search
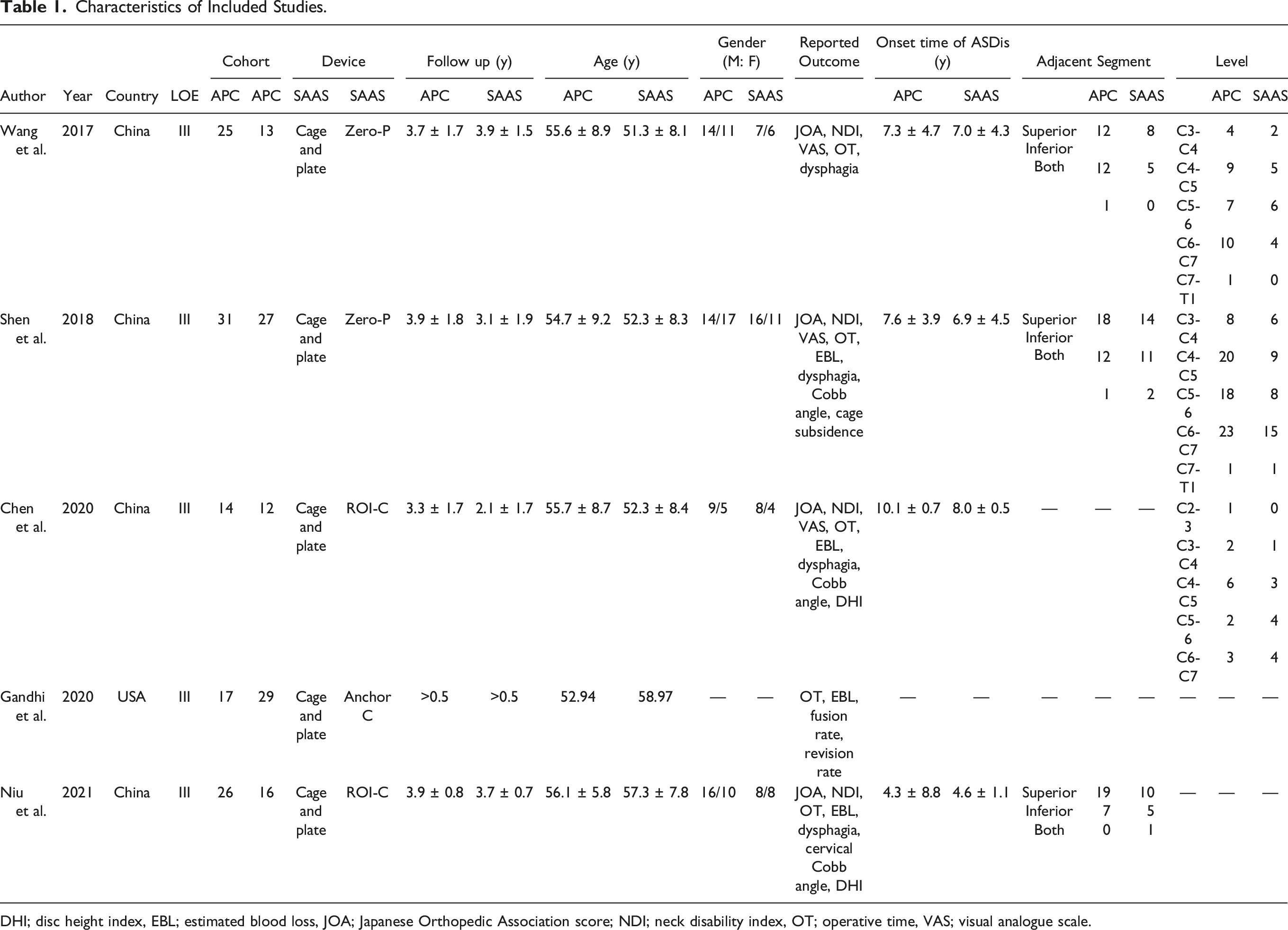
The initial literature search identified 851 articles. Of these, 239 were duplicates and removed. Six hundred and twelve were screened by titles and abstracts, and 590 were excluded leaving 22 articles for full-text review. Of the 22 articles, 4 were retained based on the stated selection criteria. A search of bibliographic references yielded one additional study that met the selection criteria. As a result, 5 studies in total were included in the meta-analysis27-31 (Figure 1). The characteristics of the included studies are summarized in Table 1. Flow diagram of the search strategy and study selection as per PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Characteristics of Included Studies. DHI; disc height index, EBL; estimated blood loss, JOA; Japanese Orthopedic Association score; NDI; neck disability index, OT; operative time, VAS; visual analogue scale.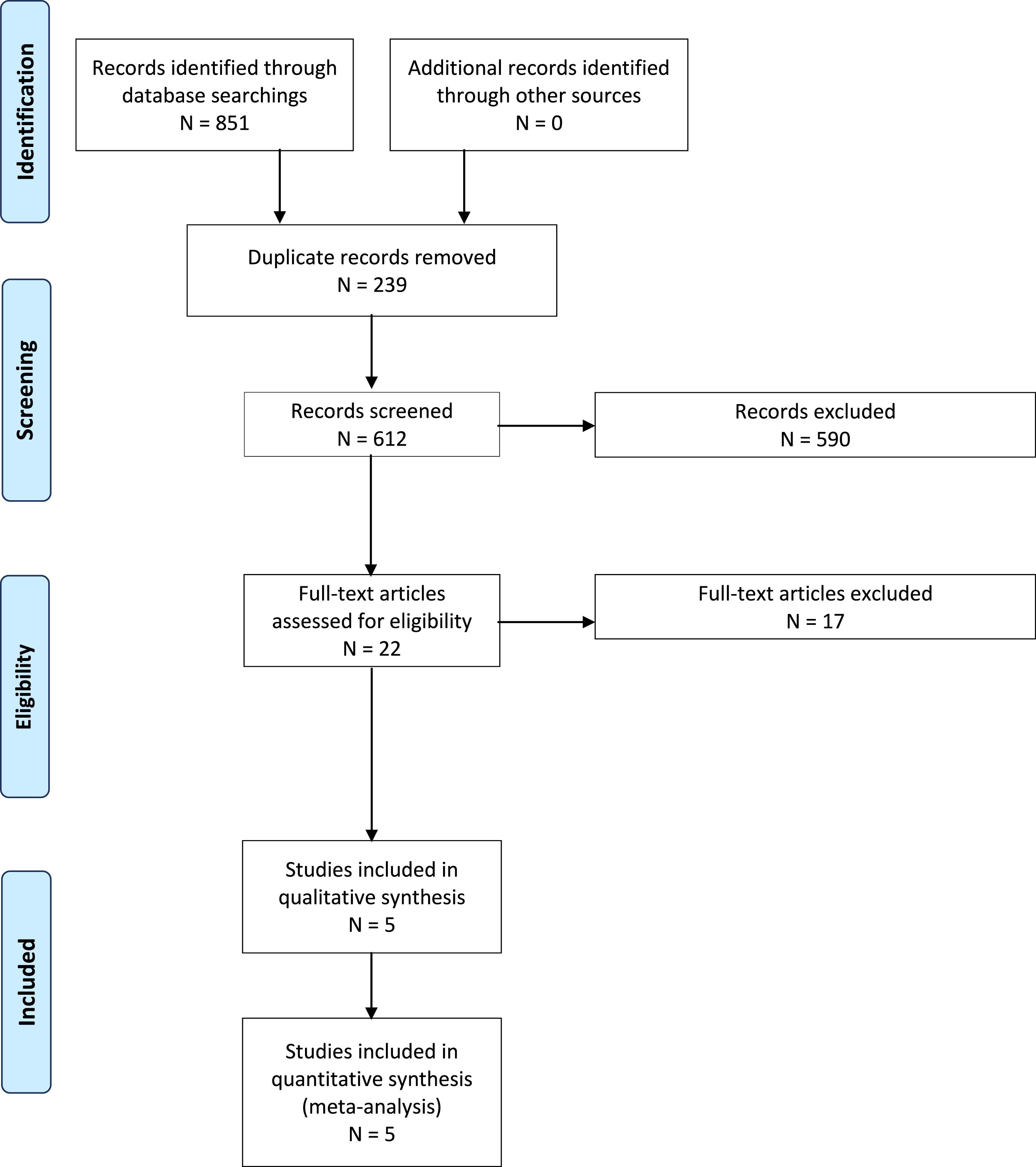
Baseline Characteristics
Baseline Cohorts Characteristics.
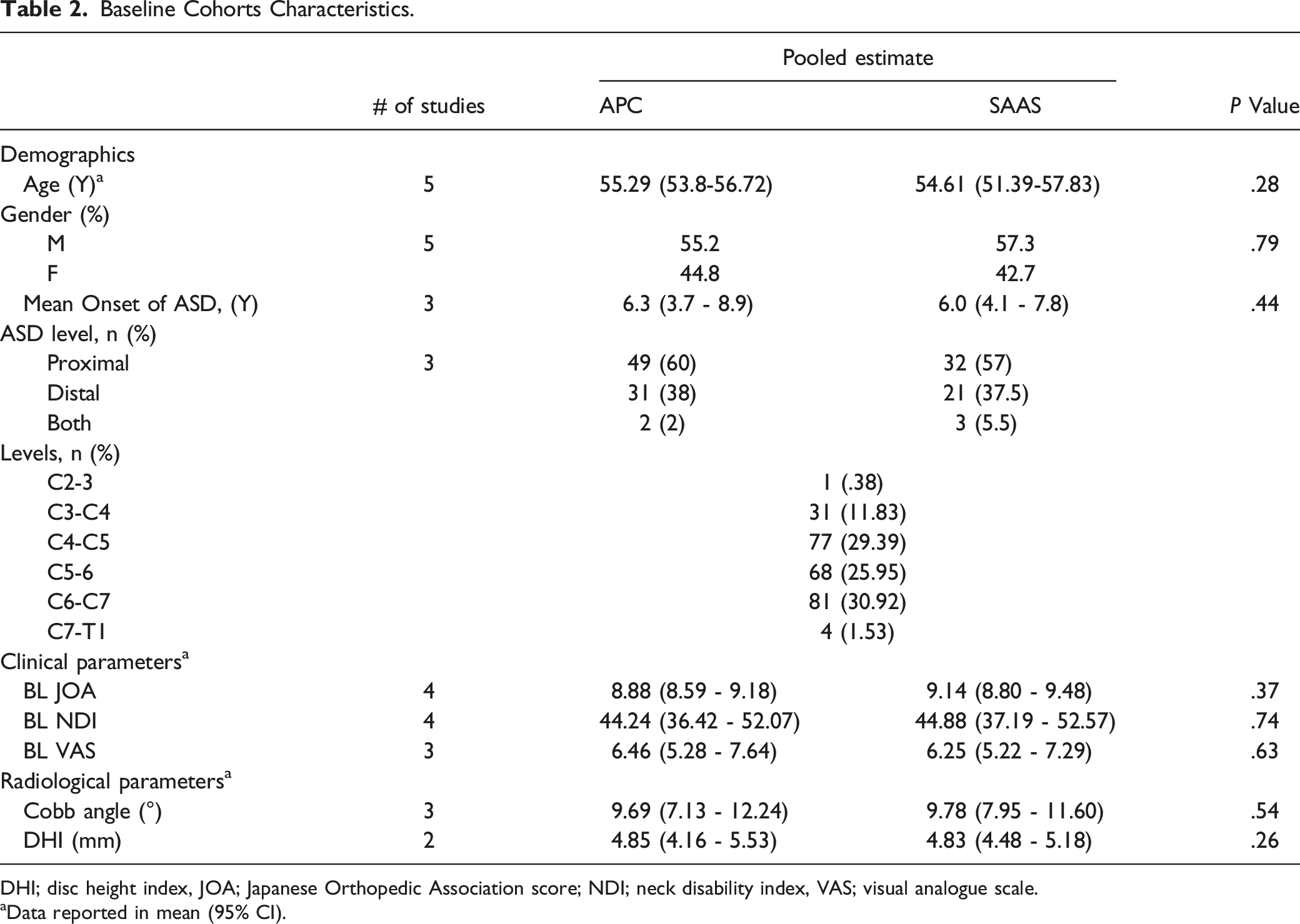
DHI; disc height index, JOA; Japanese Orthopedic Association score; NDI; neck disability index, VAS; visual analogue scale.
aData reported in mean (95% CI).
Efficacy and Functional Outcomes
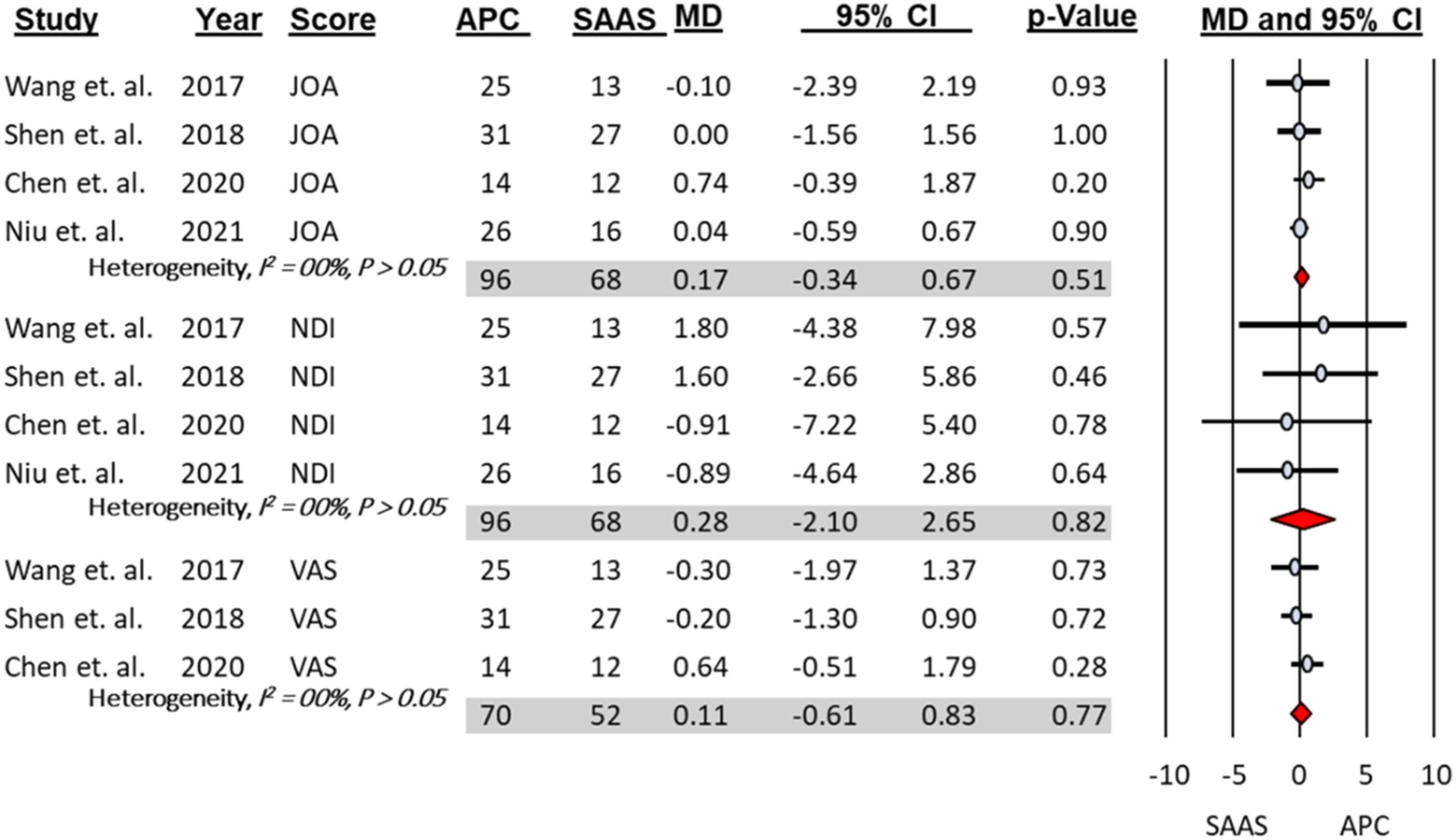
Final follow-up clinical scores improved significantly in the APC group compared to baseline, including JOA [MD = 5.36, 95% CI = 5.03 - 5.69, P < .05], NDI [MD = − 27.09, 95% CI = − 28.45 - − 25.73, P < .05], and VAS [MD = − 4.52, 95% CI = −4.98 - −4.06, P < .05]. Similarly, final follow-up clinical scores improved significantly in the SAAS group compared to the baseline, including JOA [MD = 5.16, 95% CI = 4.81 - 5.52 P < .05], NDI [MD = − 29.86, 95% CI = −36.88 - −22.85, P < .05], and VAS [MD = − 4.61, 95% CI = −5.17 - −4.06 P < .05] (Figure 2). At the final follow-up, there was no significant difference in these clinical scores between APC and SAAS (Figure 3). Forest plots and meta-analysis of the mean difference between postoperative and preoperative clinical scores to the ASDis patients treated with either anterior plate construct (APC) or stand-alone anchor spacer (SAAS). JOA; Japanese Orthopedic Association score; NDI; neck disability index, VAS; visual analog scale. Forest plots and meta-analysis comparing the final follow-up clinical scores of the ASDis patients treated with anterior plate construct (APC) vs stand-alone anchor spacer (SAAS). JOA; Japanese Orthopedic Association score; NDI; neck disability index, VAS; visual analog scale.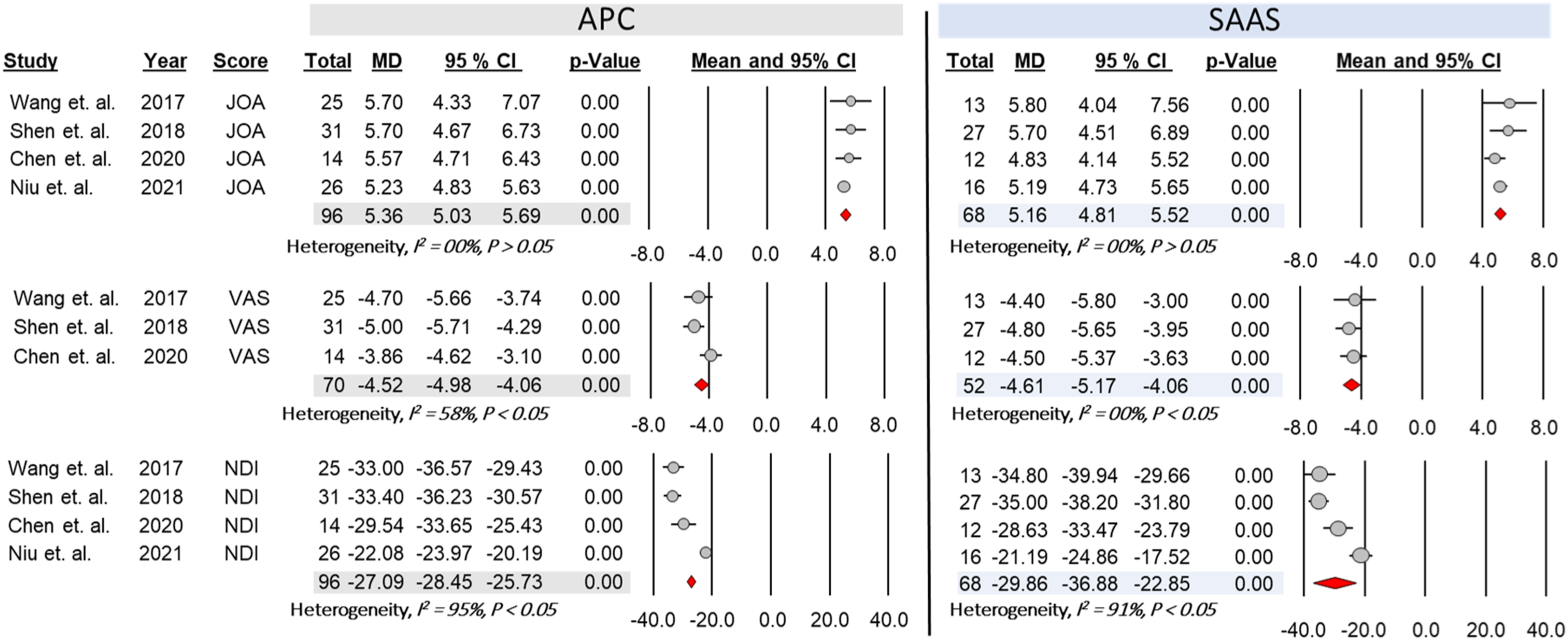
Operative Characteristics
The APC group had significantly longer operative time and higher estimated blood loss than the SAAS group (MD = 16.96, 95% CI = 7.87 - 26.06, P < .05) and (MD = 5.22, 95% CI = .35 - 10.09, P < .05), respectively (Figure 4). Forest plots and meta-analysis comparing the estimated blood loss (EBL) and operative time OT between the anterior plate construct (APC) group and stand alone anchor spacer (SAAS) group.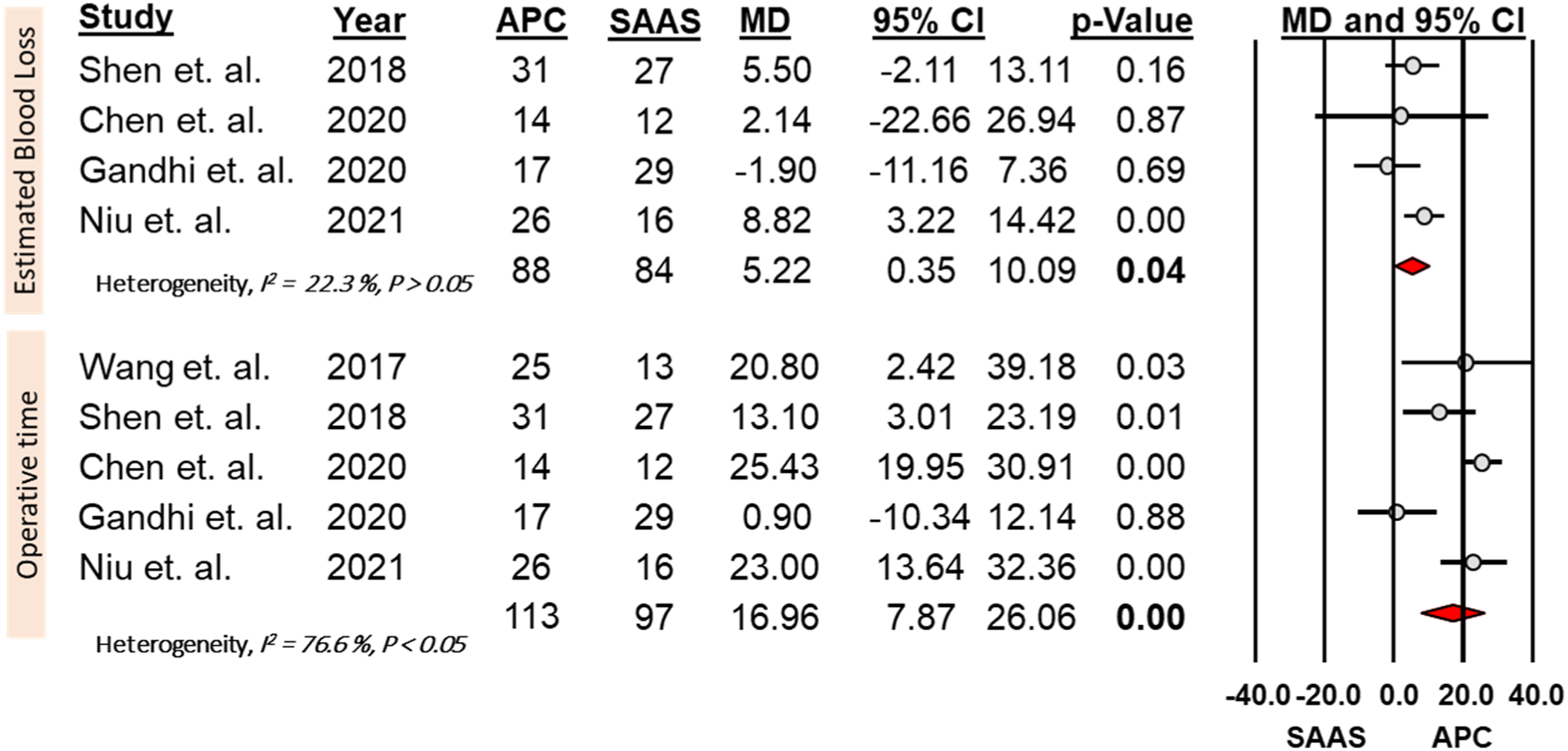
Radiological Outcomes and Fusion Rate
Meta-Analysis Summary of the Different Outcomes Between the Anterior Plate Construct (APC) Group and Stand-alone Anchor Spacer (SAAS) Group.
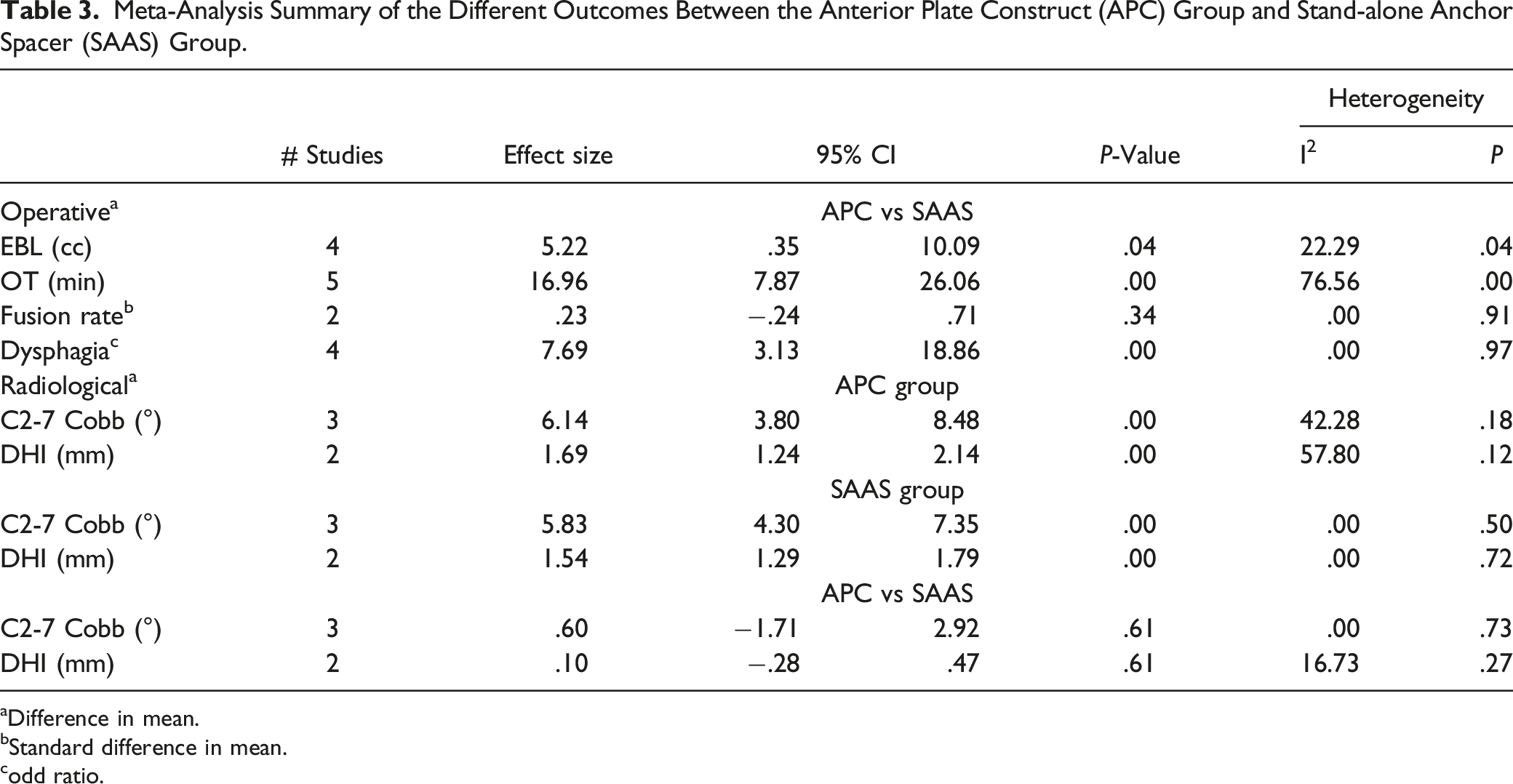
aDifference in mean.
bStandard difference in mean.
codd ratio.
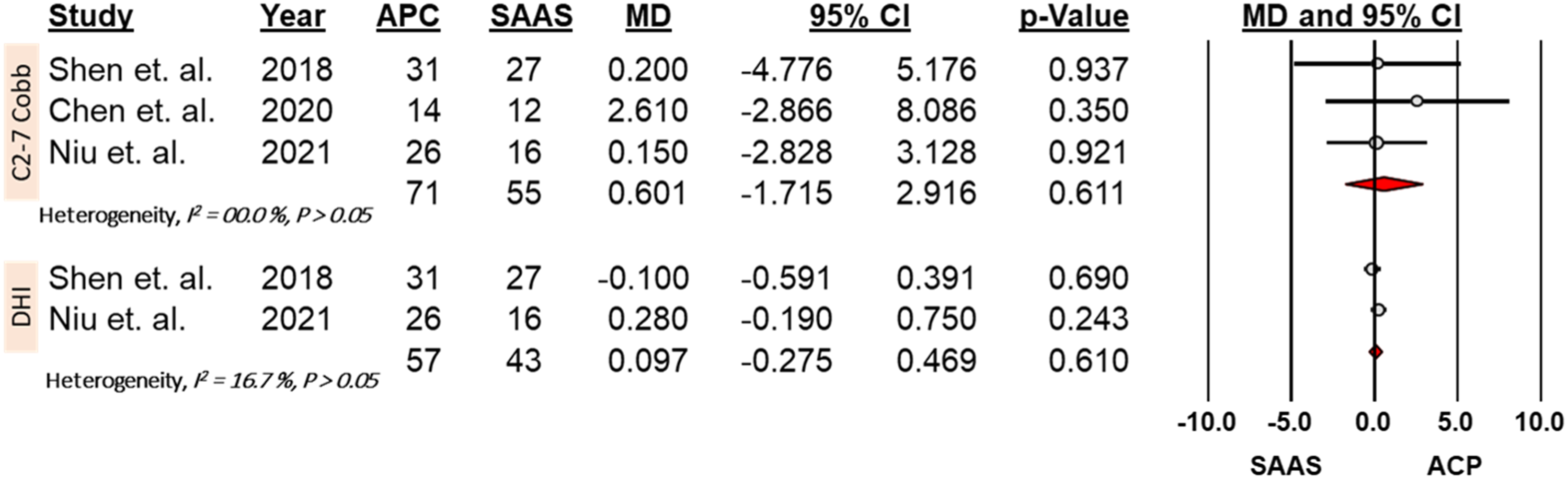
Forest plots and meta-analysis of the C2-C7 Cobb angle and disc height index (DHI) changes between the anterior plate construct (APC) group and stand-alone anchor spacer (SAAS) group.
Complications
Four studies reported postoperative dysphagia.27,29-31 The total incidence rate of postoperative dysphagia in the whole cohort was 26.9% [95% CI = 18.5 - 37.5]. The post-operative dysphagia was significantly higher in the APC group with a rate of 47% [ 45/96, 95% CI = 37 - 57%] compared to the SAAS group with a rate of 11% [ 7/68, 95% CI = 5 - 22%], and odd ratio of 7.7 [95% CI = 3.1 - 18.9, P < .05] (Figure 6). However, the prolonged dysphagia (at the final follow-up) rate was 5.2% (5/96) in the APC group compared to 0% (0/68) in the SAAS group (P > .05). One study
28
reported a revision rate of 13.79% (4/29) for the SAAS group compared to 0% (0/17) for the APC group. One study
30
reported cage subsidence with a rate of 9.7% (3/31) and 7.4% (2/27) for the APC and SAAS groups, respectively. No major neurological or vascular complications were reported in either group. Forest plots and meta-analysis of dysphagia rate between the anterior plate construct (APC) group and stand-alone anchor spacer (SAAS) group.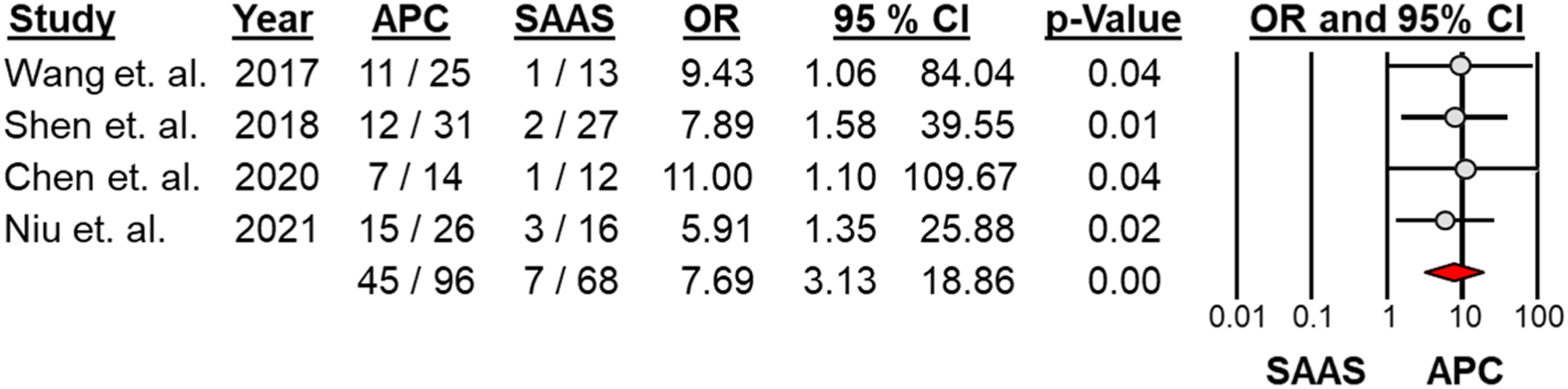
Quality Assessment and Certainty of the Evidence
Summary of Findings (GRADE Assessment).
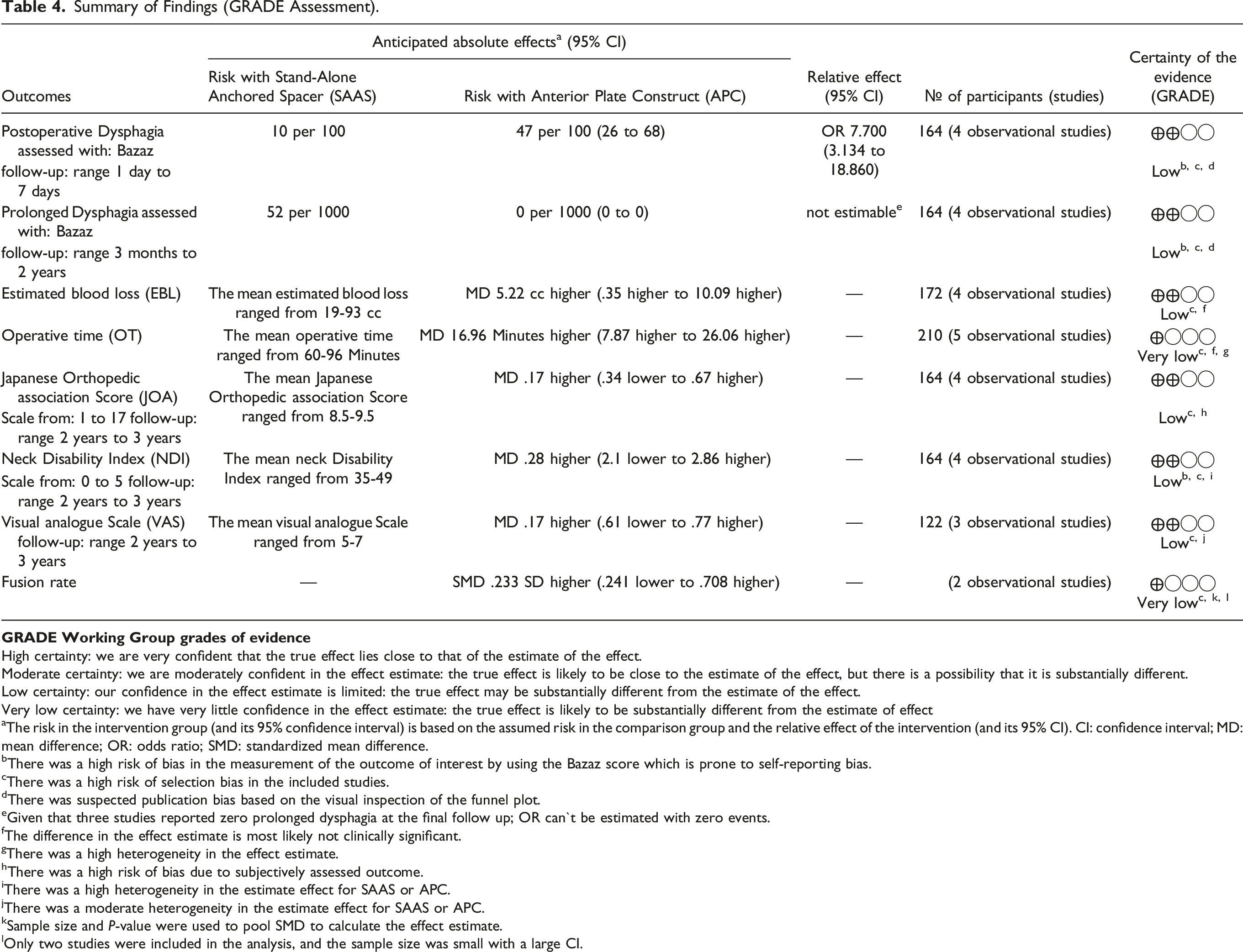
High certainty: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect
aThe risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; OR: odds ratio; SMD: standardized mean difference.
bThere was a high risk of bias in the measurement of the outcome of interest by using the Bazaz score which is prone to self-reporting bias.
cThere was a high risk of selection bias in the included studies.
dThere was suspected publication bias based on the visual inspection of the funnel plot.
eGiven that three studies reported zero prolonged dysphagia at the final follow up; OR can`t be estimated with zero events.
fThe difference in the effect estimate is most likely not clinically significant.
gThere was a high heterogeneity in the effect estimate.
hThere was a high risk of bias due to subjectively assessed outcome.
iThere was a high heterogeneity in the estimate effect for SAAS or APC.
jThere was a moderate heterogeneity in the estimate effect for SAAS or APC.
kSample size and P-value were used to pool SMD to calculate the effect estimate.
lOnly two studies were included in the analysis, and the sample size was small with a large CI.
Discussion
ASDis is one of the most commonly discussed consequences of cervical fusion. Whether ASDis is a natural result of aging or a consequence of biomechanical changes surrounding a fused segment is still debated.32,33 Kong et al 34 found in a systematic review that the prevalence of ASDis after cervical fusion ranged from 11% to 16% and that 4.99% - 6.69% of ASDis patients required surgery. Along with pseudoarthrosis, ASDis is the most common reason for reoperation after cervical fusion. 35 Cervical ASDis can be treated using an anterior or combined approach. The current literature offers no consensus on the best choice for the treatment of ASDis. Due to the restrictive indications for CDR and the downfalls of the posterior approach, the APC technique remains the most commonly chosen approach for the treatment of ASDis. The stand-alone anchored spacer (SAAS) technique was developed to avoid the undesirable complications linked to anterior cervical plating, including dysphagia, screw loosening, and adjacent segment disease. Furthermore, as SAAS obviates the need to replace the previous plate, this technique may be preferable to APC in terms of reducing dissection in revision cases. SAAS would seem an ideal choice for revision of ACDF for ASDis, as it may result in decreased blood loss, surgical time, and postoperative dysphagia in one and two-level cases.27,28,30,31,36
This study, to the best of our knowledge, is the first up-to-date meta-analysis and review of all comparative studies (5 studies with 210 patients, 97 in the SAAS group and 113 in the APC group) for the surgical treatment of ASDis using SAAS vs APC. An overall comparative profile of functional outcomes, operative characteristics, radiological outcomes, and complication rates between APC and SAAS groups showed significantly higher postoperative dysphagia, operative time, and blood loss in the APC group compared to the SAAS group. However, after thorough examination of our study using the GRADE tool, we have low to very low confidence in the evidence of these findings, and thus the estimate effect could be significantly different from the true estimate effect.
Efficacy and Functional Outcomes
The goals of surgery in primary anterior cervical fusion using either APC or SAAS for the treatment of cervical radiculopathy or myelopathy are to prevent disease progression and to improve the patient’s clinical condition. In a recent long-term prospective study evaluating the effectiveness of APC, patients demonstrated a significant improvement in outcome scores regardless of the primary diagnosis (e.g., disk herniation, stenosis, or degenerative disk disease), and this improvement persisted for more than 10 years after surgery. 37 According to several reviews of the literature, functional outcomes for primary APC and SAAS using JOA, NDI, and VAS are comparable.38-44 Our meta-analysis confirmed the same findings as primary APC and SAAS, as both lead to improvements in JOA, VAS, and NDI in revision surgery. This similarity should be interpreted with caution due to the inherent differences between primary and revision surgery. When Chen et al 45 compared primary vs revision ACDF, they observed that the revision group had comparable JOA scores but a significantly lower VAS than the primary group.
Operative Characteristics
The estimated blood loss and operative time for APC were significantly higher in our meta-analysis. This could be due to fewer steps being needed to insert the anchoring clips or screws with the SAAS implant than there would be with a traditional APC construct. Additionally, though both APC and SAAS use the Smith-Robinson approach to access the spine, additional soft tissue dissection may be required in APC when revising the plate as opposed to SAAS, where the plate does not need to be removed. Although we found a statistically significant difference in OT (16.96 min) and EBL (5.22 mL), this difference is too small to have clinical significance. While MCID thresholds for EBL and OT are not definitively established, it has been reported that EBL >300 mL and OT >5 hours are associated with increased complications and morbidity in anterior cervical surgery. 46 Finally, the surgeon’s familiarity with the chosen technique influences these operative parameters.
Radiological Outcomes
Although it is debatable, restoring the proper cervical sagittal alignment may be a factor in achieving better outcomes. Malalignment has been negatively associated with postoperative neck pain, adjacent segment disease, fusion rate, construct failure, and neurological recovery.47,48 Evaniew et al, 49 on the other hand, found no significant associations between cervical alignment changes following surgery and clinical outcome in patients with cervical spondylotic myelopathy (CSM). Guo et al 50 in a recent meta-analysis showed that both SAAS and APC improve C2-C7 lordosis compared with preoperative measures, without any significant difference between the two techniques in primary ACDF. Our study showed similar findings in the treatment of ASDis, with neither SAAS nor APC demonstrating superior restoration of sagittal parameters. This is in contrast to Lu et al 41 who found that APC achieved better cervical lordosis than SAAS. Indirect decompression, judged by disc height restoration, is critical for neurological improvement, particularly in the contribution of foraminal stenosis. Unsurprisingly, as both techniques rely on cage or graft insertion, our meta-analysis found no difference between SAAS and APC in restoring disc height. 50
It has been reported that primary ACDF showed a fusion rate of 92-95% in treating primary cervical pathologies such as spondylosis or trauma.51,52 Guo et al, 50 on the other hand, found lower but comparable fusion rates between APC and SAAS groups, with rates of (173/199 = 86.9%) and (156/184 = 84.8%), respectively. Chen et al 53 reviewed 63 patients who underwent ACDF with SAAS for ASDis and found a 2-year fusion rate of 95.2%. In our review, only two studies28,29 reported the fusion rate. Ghandi et al found that SAAS and APC fusion rates in treating ASDis were 82.35% and 68.97%, respectively. 28 In the meta-analysis, at the final follow-up, there was no difference in the fusion rate between APC and SAAS groups [SDM = .23, 95%CI = .71-1.34, P = .34]. Due to the small sample size of the cohort, we believe that future studies with a larger cohort and longer-term follow-up would be beneficial in determining the fusion rates for either technique.
Dysphagia
Postoperative dysphagia is a common complaint following primary and revision ACDF and was reported in up to 8.5% of primary ACDF and 15% of revision cases.54,55 It may present in two forms- either mild, short-term, and self-limited, or severe and persistent, which adversely affects the overall outcome and may be a devasting sequela. Although it is one of the most common complications following ACDF, the exact mechanism is unclear. It could be influenced by tracheal intubation, soft tissue retraction, esophageal irritation, postoperative hematoma, prevertebral soft tissue edema, plate prominence, or adhesion formations around the plate.56-59 Female gender, baseline or previous history of dysphagia, increased number of operative levels, longer operative time, and smoking are all well-documented risk factors for postoperative dysphagia. 55 SAAS was first introduced to overcome the protentional side effects of the conventional ACDF with APC such as postoperative dysphagia. Yang et al 60 reported in a meta-analysis of 10 studies that the overall dysphagia in primary ACDF using SAAS was significantly lower compared to the APC group at one month, three months, and 6 months follow-up. In our meta-analysis, four out of five studies reported postoperative dysphagia which was significantly higher in the APC group compared to the SAAS group (OR = 7.7) with an overall incidence of 26.9%.27,29,30 In contrast to our findings, a recent meta-analysis comparing primary APC vs SAAS for 2-level fusion found no difference in postoperative dysphagia between the two techniques. 41 Lastly, in our review, only one study reported the incidence of prolonged dysphagia, at 19% (5 of 26) in the APC group compared to none in the SAAS group. 31 This is consistent with the findings of Nguyen et al, 55 who reported a 15.3% incidence of prolonged dysphagia in a multicenter study of 170 patients who had ACDF. They also found that baseline dysphagia and smoking were significant predictors for prolonged dysphagia. 55 Based on this, some might consider using SAAS for patients with risk factors for dysphagia such as a history of dysphagia, baseline dysphagia, and smokers.
Major Complications
Major complications such as recurrent laryngeal nerve injury, esophageal perforation, postoperative hematoma, Horner’s syndrome, major vascular or spinal cord injury, and cerebrospinal fluid (CSF) leak after primary ACDF are uncommon. 61 Although such complications may be more common in revision surgery, 61 none of the patients in our meta-analysis developed such complications. Similarly, none experienced wound healing issues. This may be potentially explained by the small number of patients and the fact that these complications are uncommon following the anterior cervical approach. 62 Lastly, one study 31 reported hoarseness and cough as a result of recurrent laryngeal nerve irritation that resolved completely after conservative treatment; with 2 out of 26 and 1 out of 16 respectively in the APC and SAAS groups.
Revision Rate
Although the reoperation rate after primary ACF has been extensively reported in the literature, it remains sparsely reported after treatment for ASDis. In a long-term study by Bydon et al involving 888 patients who underwent primary ACDF, 108 patients experienced ASDis and underwent fusion. Of these, 27 underwent a second revision as a result of the subsequent ASDis (25%). 11 In contrast, Ghandi et al reported the revision rate in the SAAS group following fusion for ASDis was 13.79% as opposed to zero in the APC group. 28 Of the 4 revisions in the SAAS group, two patients had hardware migration that required reoperation, and two patients required surgery for pseudarthrosis. Lastly, Shen et al 30 found no significant difference in cage subsidence between the two groups.
Limitations
It is plausible that several limitations could have influenced the results of this review. First, because studies were scarce, all single and multilevel pathologies were analyzed, which could bias the analysis and result in underpowered outcomes. Second, the sample size in each study and the number of studies comparing APC vs SAAP in treating ASDis are both limited (only five studies with small sample sizes were included), raising concerns about potential bias in the study's conclusions. However, this could be attributed to the naturally decreased incidence of ASDis necessitating revision surgery after ACDF, and it could be a call for a future collaborative multicenter study. Third, different devices for SAAS (zero-p or ROI-C) were used among the included studies adding another potential confounding factor.
Conclusion
Both SAAS and APC are effective surgical techniques for the treatment of ASDis, with comparable functional outcomes and radiological outcomes. Although their clinical significance is debatable, SAAS appears to have several advantages over APC, including decreased postoperative dysphagia, operative time, and blood loss. Given that patients undergoing revision cervical spine surgery are at risk of dysphagia, SAAS maybe is a preferred option. Further studies are warranted to clarify the findings of this meta-analysis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.