
Abstract
Study Design:
Survey study and retrospective review of prospective data.
Objectives:
To contrast surgeons’ perceptions and reported national data regarding the rates of postoperative adverse events following anterior cervical discectomy and fusion (ACDF) and to assess the accuracy of surgeons in predicting the impact of patient factors on such outcomes.
Methods:
A survey investigating perceived rates of perioperative complications and the perceived effect of patient risk factors on the occurrence of complications following ACDF was distributed to spine surgeons at the Cervical Spine Research Society (CSRS) 2015 Annual Meeting. The equivalent reported rates of adverse events and impacts of patient risk factors on such complications were assessed in patients undergoing elective ACDF from the National Surgical Quality Improvement Program (NSQIP).
Results:
There were 110 completed surveys from attending physicians at CSRS (response rate = 44%). There were 18 019 patients who met inclusion criteria in NSQIP years 2011 to 2014. The rates of 11 out of 17 (65%) postoperative adverse events were mildly overestimated by surgeons responding to the CSRS questionnaire in comparison to reported NSQIP data (overestimates ranged from 0.24% to 1.50%). The rates of 2 out of 17 (12%) postoperative adverse events were mildly underestimated by surgeons (range = 0.08% to 1.2%). The impacts of 5 out of 10 (50%) patient factors were overestimated by surgeons (range relative risk = 0.56 to 1.48).
Conclusions:
Surgeon estimates of risk factors for and rates of adverse events following ACDF procedures were reasonably nearer to national data. Despite an overall tendency toward overestimation, surgeons’ assessments are roughly appropriate for surgical planning, expectation setting, and quality improvement initiatives.
Introduction
Rising patient expectations, changes in health care reimbursement, and increasing transparency in the delivery of medicine have led to postoperative adverse outcomes receiving greater attention. To this end, many recent studies, which have been facilitated by national databases such as the American College of Surgeons National Surgical Quality Improvement Program (NSQIP), have evaluated adverse events after anterior cervical discectomy and fusion (ACDF). 1 –5
ACDF procedures are frequently utilized in patients that have failed conservative management for cervical disc disease. The incidence of this procedure has been increasing since 1990, and published literature has cited complications after ACDF to be as high as 3% following primary procedures, and 8% following revision procedures. 1,6 –8
Discussing the possibility of postoperative adverse outcomes is an important part of the shared decision-making process prior to surgery, which is crucial as patient expectations regarding their peri- and postoperative course can have a direct impact on their satisfaction. 9 In a meta-analysis by Witiw et al, 10 preoperative expectations were compared to actual outcomes in patients undergoing surgery for degenerative spinal pathology. This study demonstrated that low expectation–actuality discrepancies, or small differences between patients’ expected results prior to the surgery and perceived outcome following the procedure, are associated with higher satisfaction.
In a different area of orthopedics, Younger and colleagues 11 evaluated the relationship of expectations and outcomes on patient satisfaction following operative fixation of end-stage ankle arthritis. They concluded that patient satisfaction was optimized not only when greater functional scores were achieved but also when there was better meeting of preoperative expectations.
In order for surgeons to set appropriate preoperative expectations, they need to correctly educate their patients on the risk of potential adverse events and predisposing factors for such complications. To our knowledge, no recent studies have compared spine surgeons’ perceptions of rates and risk factors for adverse events following spinal procedures with reported data.
In this context, the purpose of the present study was to assess surgeon perception regarding the incidence and risk factors for postoperative adverse events following ACDF. This was addressed by surveying surgeons at a national spine meeting (Cervical Spine Research Society [CSRS]). The results of the survey were then to be compared with analogous data from a national database (NSQIP). It was hoped that this would provide a yardstick with respect to the accuracy of information that is utilized in surgical planning and expectation setting.
Methods
Survey
A single-page survey was designed and piloted in order to assess surgeons’ perceptions regarding the rates of postoperative complications within 30 days of ACDF procedures for degenerative conditions. There was no stratification by the number of levels of fusion for the queried degenerative disease population. This was due to the fact that generalizable, overall morbidity for this type of approach was the goal. It was thought that potential small incremental changes by levels fused (identified by some but not other prior studies when controlling for other patient and surgical factors 12,13 ) would be difficult to quantify in this type of overview questionnaire.
Adverse events were chosen that were available in NSQIP for later comparison and included acute kidney injury, anemia requiring transfusion, cardiac arrest, coma, death, deep vein thrombosis, hospital readmission, myocardial infarction, pneumonia, postoperative intubation, pulmonary embolism, return to the operating room, sepsis, surgical site infection, stroke, urinary tract infection, and wound dehiscence.
Furthermore, the survey addressed the perceived change in risk for having any of the aforementioned adverse events when certain patient factors were present compared to when they were not present. The patient factors were available in NSQIP for later comparison and included chronic obstructive pulmonary disease, current smoking, dyspnea on exertion, hypertension, insulin-dependent diabetes, more than one-level surgery, non–insulin-dependent diabetes, obesity (body mass index [BMI] ≥ 30), older age (70 years or older), and preoperative anemia.
The survey also obtained respondent demographic information, including type of residency, completion of spine surgery fellowship, practice setting (private, academic, hybrid), practice location, and years in practice. The survey is included in the appendix.
The survey was distributed to attendees at the 2015 CSRS 43rd Annual Meeting (San Diego, CA, December 2015). The CSRS, founded in 1973, is a society of biomechanical engineers, neurologists, neurosurgeons, radiologists, and orthopedic surgeons who are interested in clinical and research problems of the cervical spine. 14 Surveys were collected following completion.
NSQIP Sample
A cohort of patients undergoing ACDF for degenerative cervical conditions (the same population asked about in the above-described survey) was identified in NSQIP data years 2011 to 2014. NSQIP is a data set that presents information on more than 300 HIPAA compliant patient variables, including demographics, comorbid conditions, and postoperative morbidity and mortality with a 30-day follow-up. The information is drawn from patients undergoing surgery at over 500 sites across the nation, and the data undergoes rigorous accuracy audits. 11
Patients were identified using current procedural terminology codes for anterior cervical decompression and fusion (22551 and 22554). Exclusion criteria included a primary diagnosis of fracture, neoplasm, or infection, as well as patients undergoing emergency surgery, anterior/posterior fusion, or more than 3 levels of fusion, as these are all uncommon presentations of degenerative disc disease in the cervical spine treated with an anterior approach.
Patient baseline characteristics extracted from the data set included patient age, gender, BMI, and the American Society of Anesthesiologists (ASA) classification. Using this cohort, the reported rates of the adverse events listed in the CSRS survey were extracted along with the prevalence of patient risk factors.
Statistical Analysis
For the CSRS survey data, survey completion rate was calculated based on the number of attending surgeons attending the conference (data provided from course coordinators). The mean estimation for the rates of each complication, as well as the average perceived impact of patient risk factors, were calculated.
For the NSQIP data, the reported rates of each adverse event were evaluated, and the effects of patient factors were analyzed using a Poisson regression with robust error variance. The perceived rates of adverse events and the impacts patient factors had on these from the CSRS data were compared with the reported NSQIP data using Welch’s t test.
Questionnaire and NSQIP data were analyzed using STATA version 11.0 (StataCorp, LP, College Station, TX). Statistical difference was established at a 2-sided α level of .05 (P < .05). The institutional review board at the senior author’s institution approved this study.
Results
CSRS Respondent Demographics
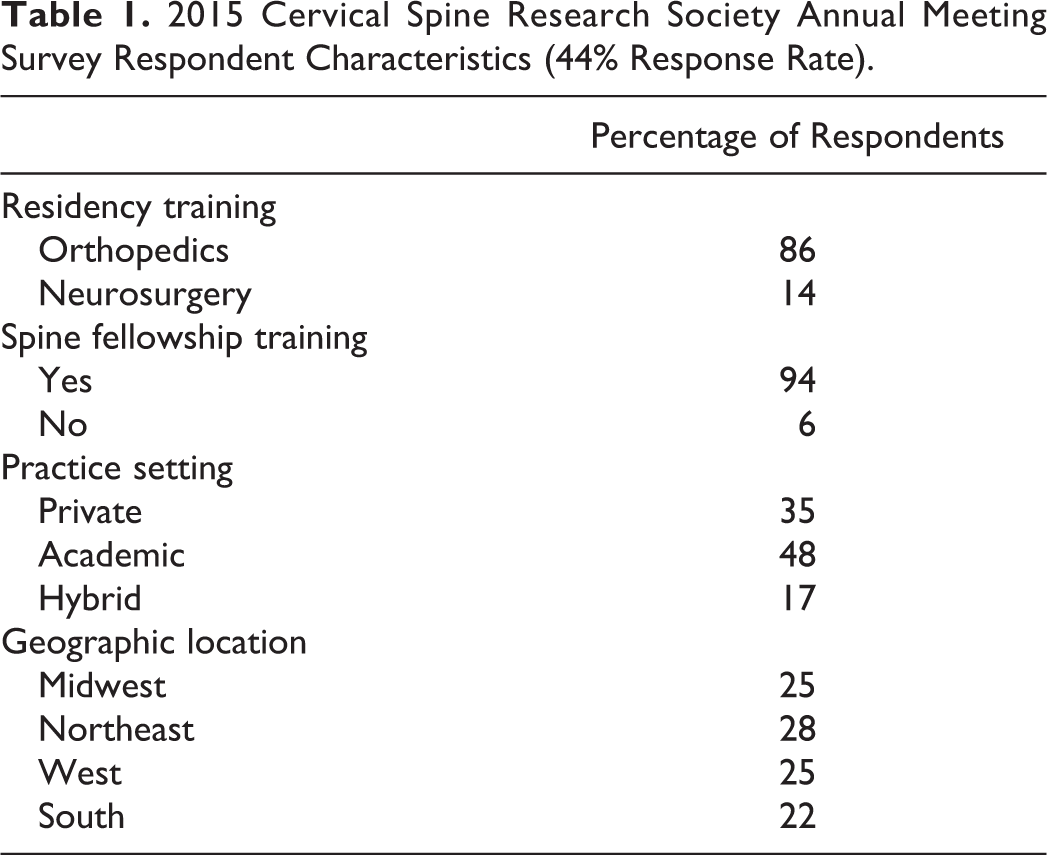
Of the 251 attending-level US spine surgeons in attendance at the 2015 meeting of CSRS (medical doctors and doctors of osteopathic medicine), 110 returned completed surveys (completion rate of 44%). The CSRS questionnaire respondents had predominantly received orthopedic surgery residency training (86%), had spine fellowship training (94%), practiced in an academic setting (48%), and were located in the northeast section of the United States (28%; Table 1).
2015 Cervical Spine Research Society Annual Meeting Survey Respondent Characteristics (44% Response Rate).
NSQIP Sample Demographics
In total, 18 019 patients were identified based on the defined inclusion and exclusion criteria. The population had an average age of 53.5 ± 11.5 years, 48.5% of patients were male, had an average BMI of 30.0 ± 6.8 kg/m2, and a median ASA of 2 with an interquartile range of 2 to 3 (Table 2).
Patient Characteristics in NSQIP Years 2011 to 2014 for Patients Undergoing Anterior Cervical Discectomy and Fusion.
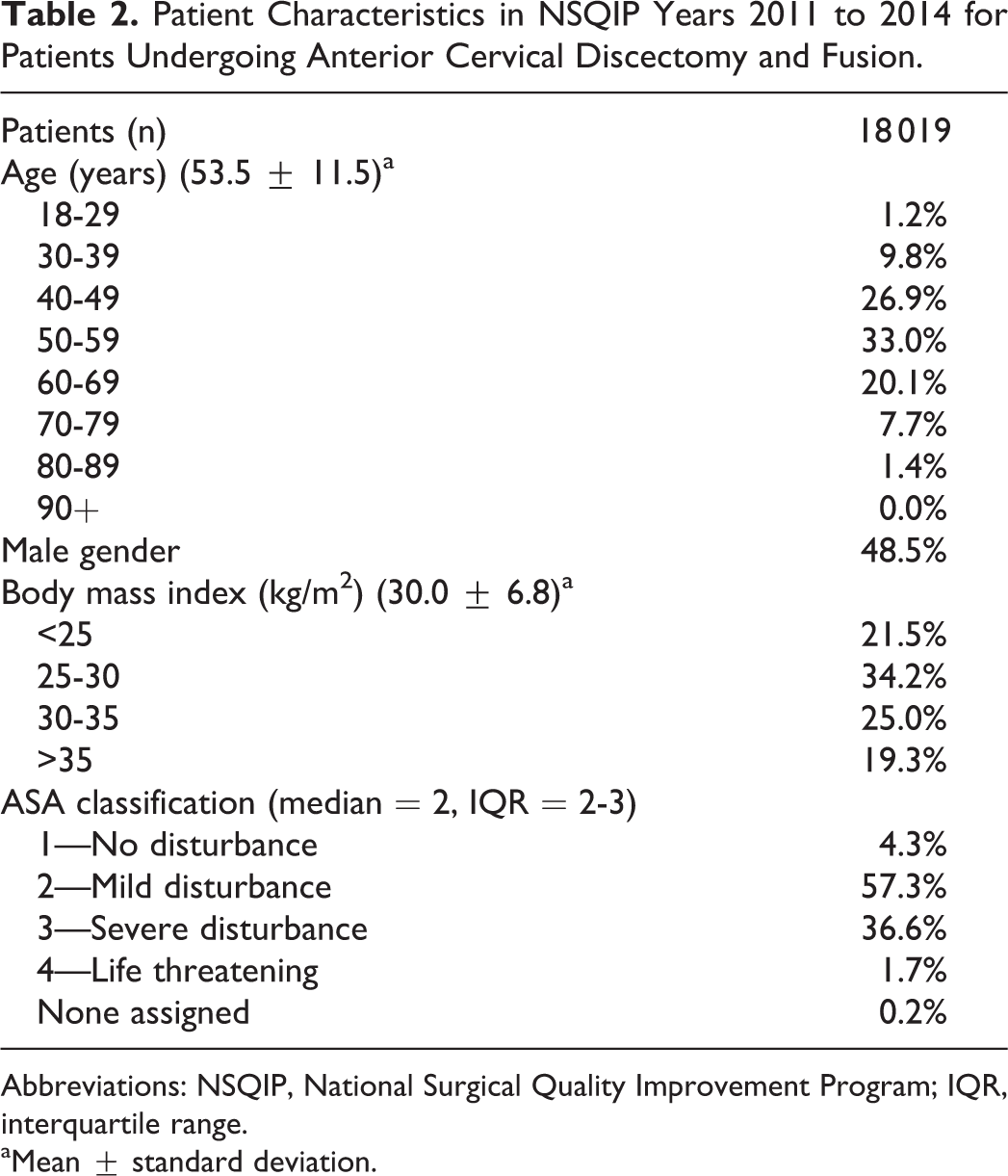
Abbreviations: NSQIP, National Surgical Quality Improvement Program; IQR, interquartile range.
aMean ± standard deviation.
Rates of Adverse Events
The perceived incidence of the 17 adverse events from the surgeons at the CSRS conference ranged from 0.10% to 1.96%, and the reported incidence of the same adverse events from the NSQIP data ranged from 0.00% to 2.83% (left half of Figure 1).
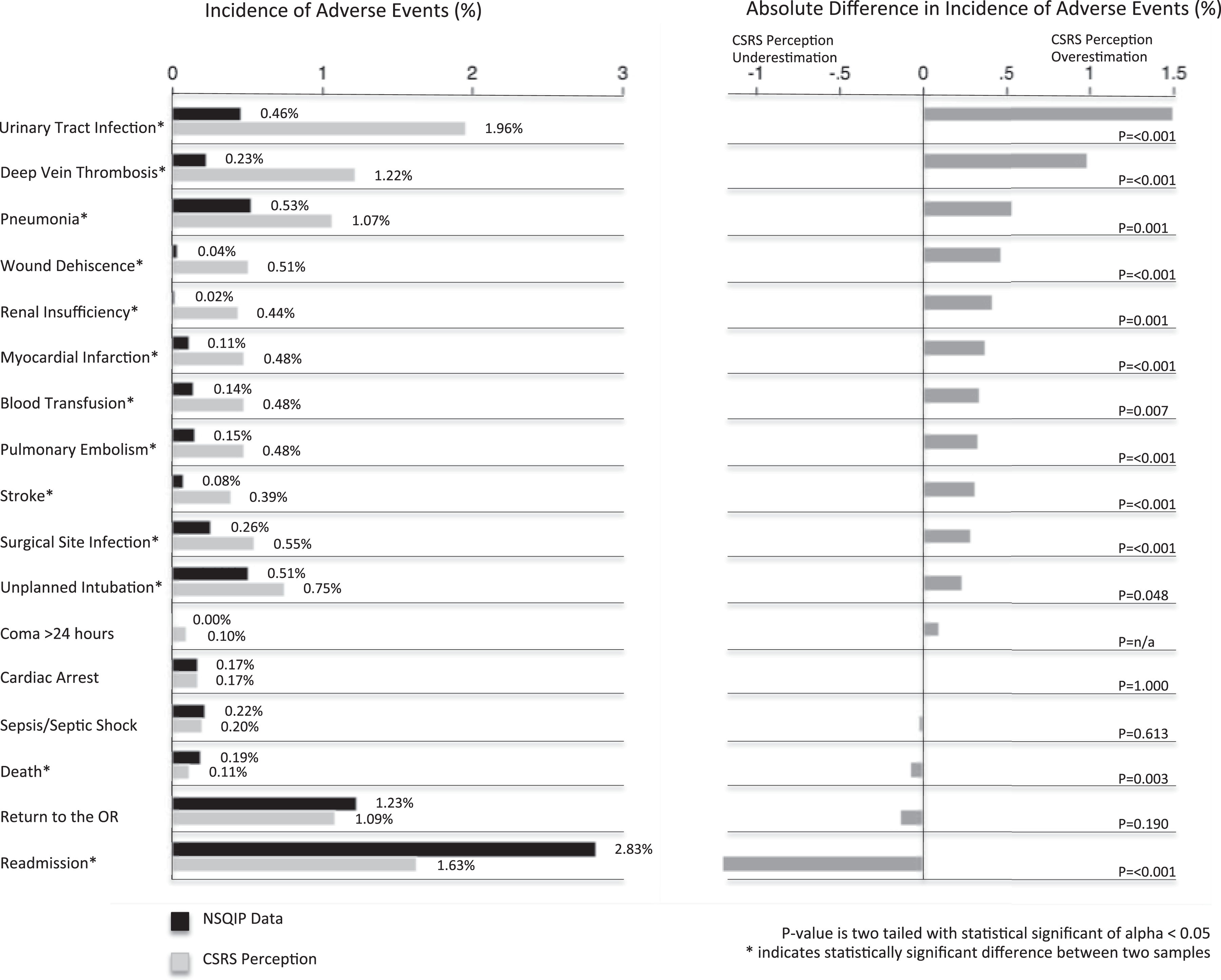
Incidence of adverse events for NSQIP data and CSRS perception.
The differences between the CSRS surgeons’ perceptions and the NSQIP cohort data ranged from CSRS surgeons’ overestimates of 1.50% to underestimates of 1.20% (right half of Figure 1). Following statistical analysis, physicians overestimated the incidence of 65% (11 out of 17) of the adverse events and underestimated the incidence of 12% (2 out of 17) of the adverse events. The adverse events with the largest survey overestimations included the incidence of urinary tract infection (1.50%, P ≤ .001) and deep vein thrombosis (0.99%, P ≤ .001). Surgeons accurately estimated the occurrence of coma, cardiac arrest, sepsis, and patients returning to the operating room following ACDF procedures. The rates of patient mortality and readmission were underestimated by 0.08% (P = .003) and 1.20% (P ≤ .001), respectively.
Risk Factors for Adverse Events
The perceived impact of 10 patient characteristics on the risk of adverse events from the CSRS surgeons were estimated to range from 1.33 relative risk to 2.51 relative risk, and the reported impact of the same patient characteristics on the risk of adverse events from the NSQIP data ranged from 0.80 relative risk to 6.38 relative risk (left half of Figure 2).
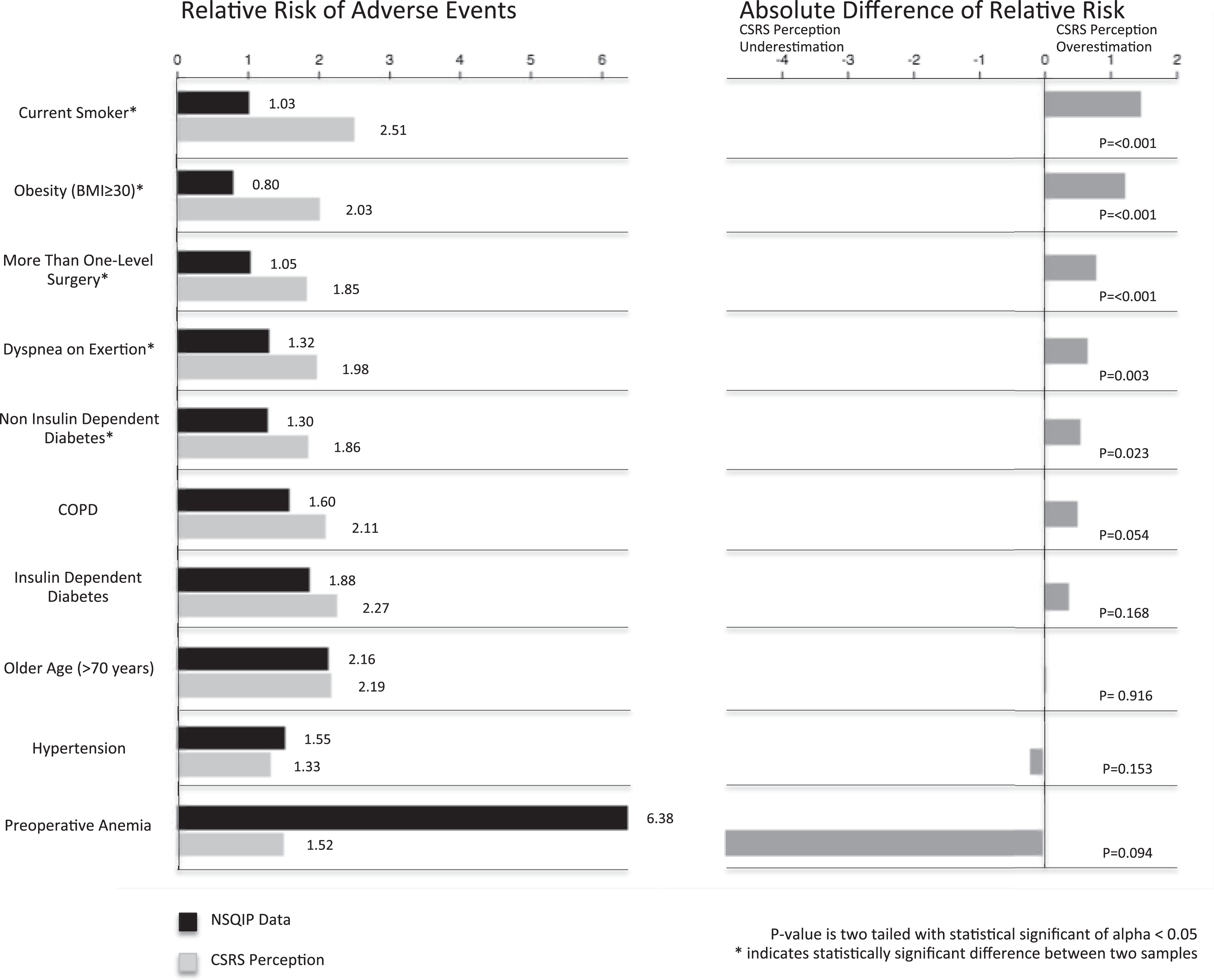
Risk factors for adverse events for NSQIP data and CSRS perception.
The differences between the CSRS survey and the NSQIP cohort results ranged from CSRS survey overestimates of 1.48 relative risk to underestimates of 4.86 relative risk (right half of Figure 2). Following statistical analysis, surgeons overestimated the relative risk of 50% (5 out of 10) of the patient characteristics. The largest differences existed in patients who are currently smoking (overestimation of 1.48 relative risk, P ≤ .001) and who are obese (overestimation of 1.23 relative risk, P ≤ .001). Surgeons accurately estimated the relative risk of chronic obstructive pulmonary disease, insulin-dependent diabetes, older age (>70 years), hypertension, and preoperative anemia following ACDF procedures with the differences between the 2 data sources being statistically insignificant.
Discussion
Postoperative adverse events and risk factors for complications after surgeries such as ACDF have been receiving increasing attention as we strive to optimize outcomes, minimize cost, and reduce inpatient stays. 15 The current study aims to contrast surgeon perception and NSQIP reported data for the rates of postoperative adverse events following ACDF and then to compare surgeons’ understanding of the impact of patient characteristics on the risks for such outcomes compared to the same NSQIP cohort.
The CSRS annual meeting attracts spine surgeons from across the world and aims to provide a forum for scientific discussion regarding the diagnosis and treatment of cervical spine diseases and injuries. 14 Survey data was collected at the CSRS annual meeting in 2015 and yielded a response rate of 44%. This rate compares well to other studies of physician surveys reported in the literature. 16 The NSQIP database, to which the survey study was compared, currently gathers data on over 300 unique perioperative variables from patients at over 500 institutions in the United States. 17 This data set is well regarded and often used for national database studies. 1 –5,18
Statistical analysis of survey data collected at CSRS and data extracted from NSQIP confirmed that surgeon-perceived rates of adverse events following ACDF surgery were overall similar to NSQIP data. Surgeons mildly overestimated the incidence of 65% (11 out of 17) of the adverse events and only mildly underestimated 12% (2 out of 17; Figure 1). Although these absolute differences are small, potential explanations for the discrepancies are discussed.
The 1.50% overestimation of the incidence of urinary tract infections (UTI) may be explained by the recent advancements in the understanding of risk factors for these infections. 19 Identification of helpful preventive measures, such as early removal of Foley catheters, and other efforts of quality improvement have been shown to reduce incidence of UTIs. 19,20 Surgeons’ responses may not have adjusted for decreased rates of UTIs over time.
Analogously, the 0.99% overestimation of deep vein thrombosis may be due to surgeons transferring knowledge from other orthopedic surgeries in which the rates of venous thromboembolism is higher. For example, recent studies have shown the incidence of venous thromboembolism following lower extremity arthroplasty to be roughly 4.0%. 21,22
In terms of CSRS surgeons’ underestimations, the 1.20% discrepancy in the rate of readmissions may be related to the fact that patients are readmitted for nonsurgical issues or to different surgeons. Studies have shown that discharging physician teams were aware of only 48.5% of patient readmissions. 23 This highlights an important issue regarding physician communication. The lost opportunity to share information about readmitted patients by prior caregivers may require greater attention in the future as there is greater emphasis placed on minimizing postoperative readmissions.
CSRS survey results regarding the impact of patient factors on the risks for postoperative adverse events were also reasonably close to the NSQIP data. Surgeons mildly overestimated the relative risk of 50% (5 out of 10) of the patient characteristics while underestimating none (Figure 2).
Spine surgeons overestimated the impact that current smoking has on the occurrence of adverse outcomes by 1.48 relative risk. This could be due to the transference of knowledge that smoking has on longer term nonunion to the perioperative adverse outcomes analyzed in the current investigation. 24 The impact of obesity was also overestimated by 1.23 relative risk and may be due to recent studies focusing on the effects of this modifiable risk factor. 18,25 Finally, the underestimated impact of preoperative anemia, although not statistically significant, may be explained by a stringent American College of Surgeons NSQIP definition for this status. 11
An accurate understanding of the risks of a surgical intervention is not only critical in the decision-making process and informed consent for both surgeons and patients but also important for optimizing outcomes. 26,27 Research has shown that the caliber of preoperative information facilitates a patient’s active involvement in his or her own care. 28 Furthermore, an understanding of how to estimate and predict mortality and morbidity has led to reductions in adverse events along with cost savings. 27,29 While the error in surgeon-perceived occurrences and impact of patient characteristics on risks of adverse events in this study could be characterized as overestimation, this type of overemphasis benefits the safety of the patient. The information provided is close to national data, and it emphasizes to patients the risks inherent in ACDF and allows them to prepare for their discussed intervention.
Strengths of this investigation include the novelty of this analysis. No recent study, to the authors’ knowledge, has compared spine surgeons’ perceptions of rates of postoperative adverse events and the impact of patient characteristics on the rates of those adverse events with the reported national data for ACDF procedures. The current study builds off of related work evaluating outcomes after lumbar fusions (N. T. Ondeck et al, 2017, unpublished data). Limitations of this study include that ACDF procedures were not stratified by the number of levels of fusion. As stated earlier, this was due to the fact that generalizable overall morbidity for this type of approach was the goal. It was thought that potential small incremental changes by levels fused (identified by some but not other prior studies when controlling for other patient and surgical factors 12,13 ) would be difficult to quantify in this type of overview questionnaire. A second limitation is that the physicians from CSRS may not be representative of the nationally queried NSQIP surgeons. However, as demonstrated from Table 1, the CSRS physicians were from diverse geographical locations and practice settings. Additionally, NSQIP only collects short-term general health adverse events no longer than the 30th postoperative day. 30 Procedure-specific complications, such as dysphagia, are not recorded variables in the data set.
In conclusion, US spine surgeons appear to have a relatively accurate understanding of the rates of postoperative adverse events as well as the impact of patient characteristics on risk for such adverse outcomes for patients who are undergoing ACDF procedures. The consistent overestimation was not great and errs on the side of caution when it comes to decision making and assisting with setting realistic expectations for postoperative recovery. The underestimate in readmission is a reminder of the importance of physicians practicing diligent postoperative communication in order to provide the best possible care in the case of an unforeseen hospitalization.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.