
Abstract
Study Design
A retrospective study was performed.
Objective
To investigate the prevalence and risk factors for adjacent segment disease (ASD) after anterior cervical discectomy and fusion (ACDF) and the clinical efficacy of revision surgery.
Method
A total of 219 patients treated with ACDF were analyzed retrospectively. Demographic characteristics, including age, sex, body mass index (BMI) and bone mineral density (BMD), and radiographic measurements, including C2-C7 cervical sagittal vertical axis (cSVA), T1 slope (T1S), thoracic inlet angle (TIA) and C2-C7 Cobb angle, were analyzed. Modified Japanese Orthopaedic Association (mJOA) score and visual analog scale (VAS) score were used to evaluate patient function. Parameters were analyzed with Student's t test, and potential risk factors for ASD were further analyzed with multivariate logistic regression analysis.
Results
The incidence of ASD after ACDF surgeries was 21%. The severity of osteoporosis, BMI and C2-C7 cSVA were significantly higher in the ASD group than in the NASD group (P < .05). The preoperative and postoperative TIAs were lower in the ASD group (P < .05). Multivariate logistic regression analysis showed that a high BMI, severe osteoporosis and a high C2-C7 cSVA were risk factors for ASD after ACDF (P < .05). The postoperative TIA and postoperative T1S were also correlated with ASD (P < .05).
Conclusion
Patients with a high BMI, severe osteoporosis, and a large C2-C7 cSVA after ACDF have a higher risk of ASD, while a large T1S and TIA may be protective factors. In addition, revision surgery can restore cervical spine balance in patients with ASD and promote better clinical outcomes.
Keywords
Introduction
Cervical spondylosis is mainly characterized by neck, shoulder and upper limb pain, finger numbness, nausea and vomiting, and even tachycardia and dysphagia. 1 It is a common surgical disease in middle-aged and elderly individuals. With lifestyle changes, the prevalence of cervical spondylosis is increasing, and patient age at diagnosis is gradually becoming younger. Anterior cervical discectomy and fusion (ACDF) is one of the commonly used surgical methods in spine surgery, and its therapeutic effect has been widely recognized. 2 However, surgeons may pay less attention to the impact of the physiological cervical curvature on cervical degeneration, resulting in insufficient recovery of cervical curvature after operation. In addition, the application of internal fixation accelerates the degeneration of adjacent vertebral bodies, leading to the occurrence of adjacent segment disease (ASD). 3 Clinically, ASD is one of the common complications of cervical spine surgery, with corresponding imaging changes or clinical symptoms. Imaging findings may include cervical disc degeneration, cervical instability, local kyphosis, or local bone graft nonfusion. Clinical symptoms may be cervical pain, cervical spondylotic radiculopathy or cervical spondylotic myelopathy.4,5 In this study, we defined ASD as the presence of both radiographic changes and clinical symptoms. At present, although there have been a large number of studies on the necessity and efficacy of cervical spine surgery, there is no conclusion on the risk factors for the onset of ASD after cervical spine surgery or the treatment strategy.
This article explores the potential risk factors for ASD after ACDF surgery and discusses the therapeutic effect of reoperation to facilitate the clinical treatment of patients.
Materials and Methods
Patient Selection
Patients who underwent ACDF surgery at our hospital from May 2006 to May 2015 were selected with a minimum of 5 years of follow-up.
The inclusion criteria included the following: ① refractory neck pain, radiation pain of the upper limb, numbness of the limbs, or pyramidal sign with no response to conservative treatment for more than 3 months; ② age ≥18 years without craniocerebral diseases; and ③ radiographic data demonstrating ≥2 cervical segments compressing the spinal cord or cervical nerve root.
The exclusion criteria were as follows: ① patients with severe comorbidities who could not undergo surgery; ② patients with trauma, cervical deformity, tumor or infection; and ③ patients with prior spine surgeries or posterior cervical surgeries.
According to whether the patient had ASD after initial ACDF surgery, patients were divided into two groups: patients without ASD (NASD group) and patients with ASD (ASD group).
Demographic and clinical characteristics included age, sex, body mass index (BMI), bone mineral density (BMD, T score), number of lesion segments (single segment/multiple segments), medical comorbidities and duration of follow-up. A T score ≥ -1 indicated no osteoporosis, -2.5 ≤ T score < -1 osteoporosis, and T score < -2.5 severe osteoporosis.
Operative data included the operative duration and intraoperative blood loss.
Radiographic measurements included the following sagittal parameters in lateral cervical X-rays: ① the C2-C7 cervical sagittal vertical axis 6 (cSVA), namely, the horizontal distance between the vertical line of the midpoint of the C2 vertebra and the posterior upper corner of the C7 superior endplate; ② the T1 slope (T1S), namely, the angle between the parallel line on the upper edge of the T1 endplate and the horizontal straight line; ③ the thoracic inlet angle (TIA), namely, the angle between the line connecting the midpoint of the C7 superior endplate and the upper edge of the sternal manubrium and the vertical line crossing the midpoint of the C7 superior endplate; and ④ the C2-C7 Cobb angle, namely, the angle between the parallel line of the C2 inferior endplate and the parallel line of the C7 inferior endplate (Figure 1).
In addition, the modified Japanese Orthopaedic Association (mJOA) score
7
was used to evaluate the patients’ functional state, and the visual analog scale (VAS) pain score was used for pain assessment. Male patient, 65 years old. (A/B) Lateral view of the cervical spine during the initial operation. The C2-C7 Cobb angle was decreased and the C2-C7 SVA is increased before the first operation. The C2-C7 Cobb angle increased slightly, but the C2-C7 SVA did not decrease significantly after the first operation. (D/E/F) Lateral cervical view before, after, and at the last follow-up after the reoperation. The patient’s C2-C7 SVA slightly decreased after the reoperation; the C2-C7 Cobb angle did not change significantly, and it was in the normal curvature range. The sagittal balance of the patient’s cervical spine was improved. There was no significant change in the TIA or T1S at any stage.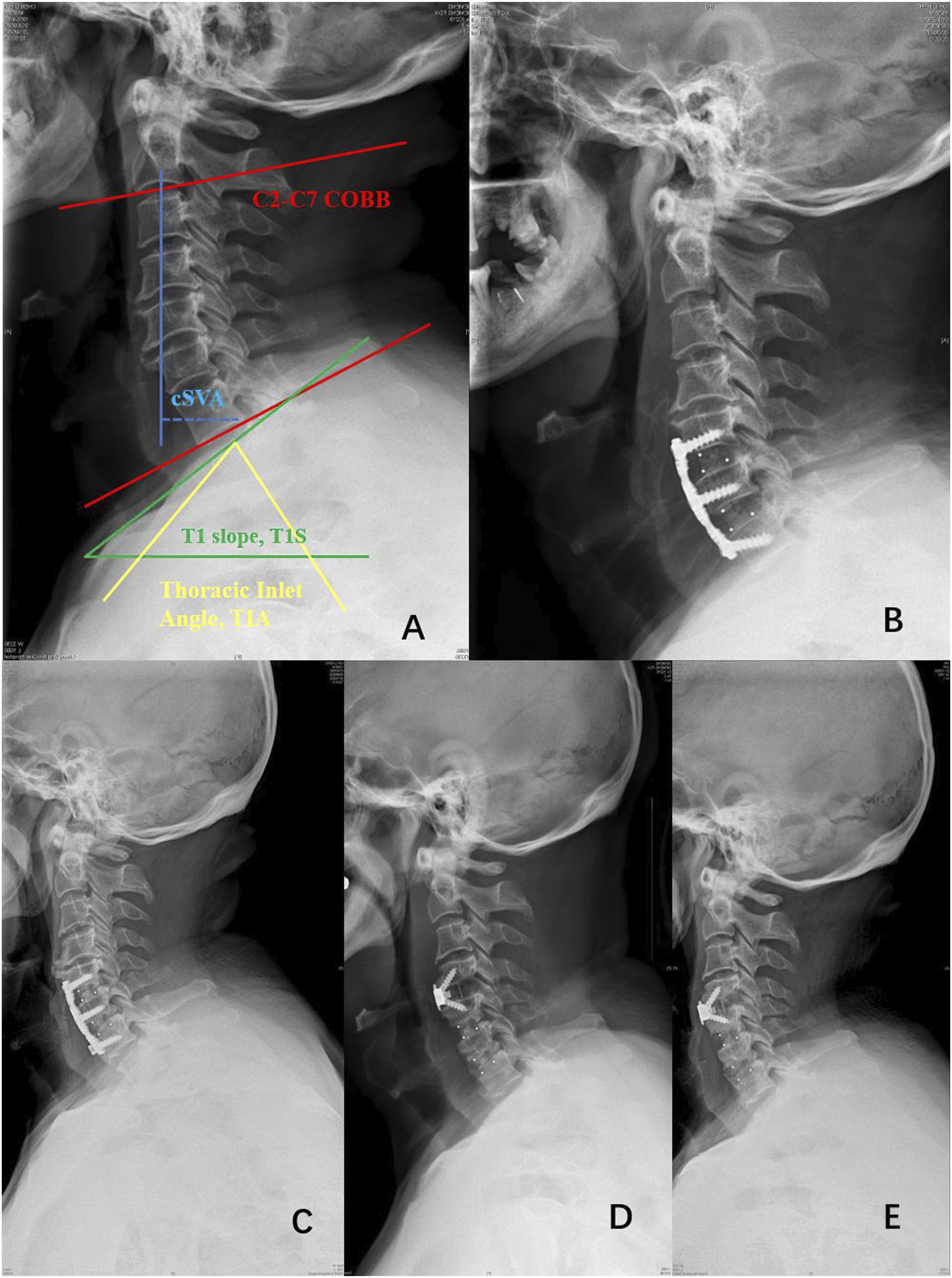
Statistical Processing
Statistical analyses were performed with Statistical Package for the Social Science (SPSS) software (version 23.0; IBM, Inc.). Continuous variables are presented as the mean ± standard deviation (SD) and were analyzed by Student's t test or analysis of variance. Categorical variables were expressed as frequencies or percentages and were analyzed by the rank-sum test and the χ2 test. Potential related risk factors were further analyzed by multivariate logistic regression analysis. A P value of <.05 was considered statistically significant. Odds ratios (ORs) and their 95% confidence intervals were calculated.
Results
A total of 219 patients were included in our study. There were 131 males and 88 females with an average age of 55.72 ± 11.51 years.
Comparison of General Data Between the Two Groups at the First Operation.

aNo/osteoporosis/severe osteoporosis. BMI, body mass index.
Comparison of Index Operative Data Between the Two Groups.

The Number of lesion segments in NASD group and ASD group.

Comparison of the Radiographical Indicators Between the Two Groups for the First Operation.
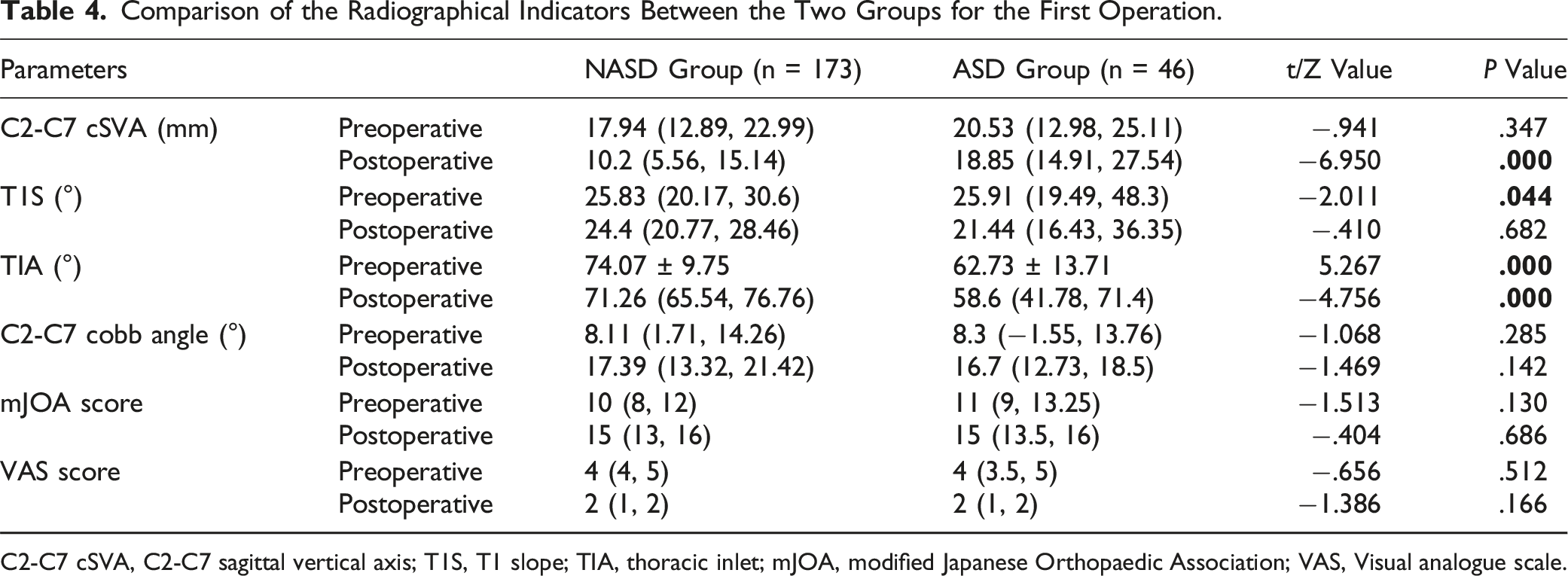
C2-C7 cSVA, C2-C7 sagittal vertical axis; T1S, T1 slope; TIA, thoracic inlet; mJOA, modified Japanese Orthopaedic Association; VAS, Visual analogue scale.
Multivariate Logistic Regression Analysis of Related Risk Factors.
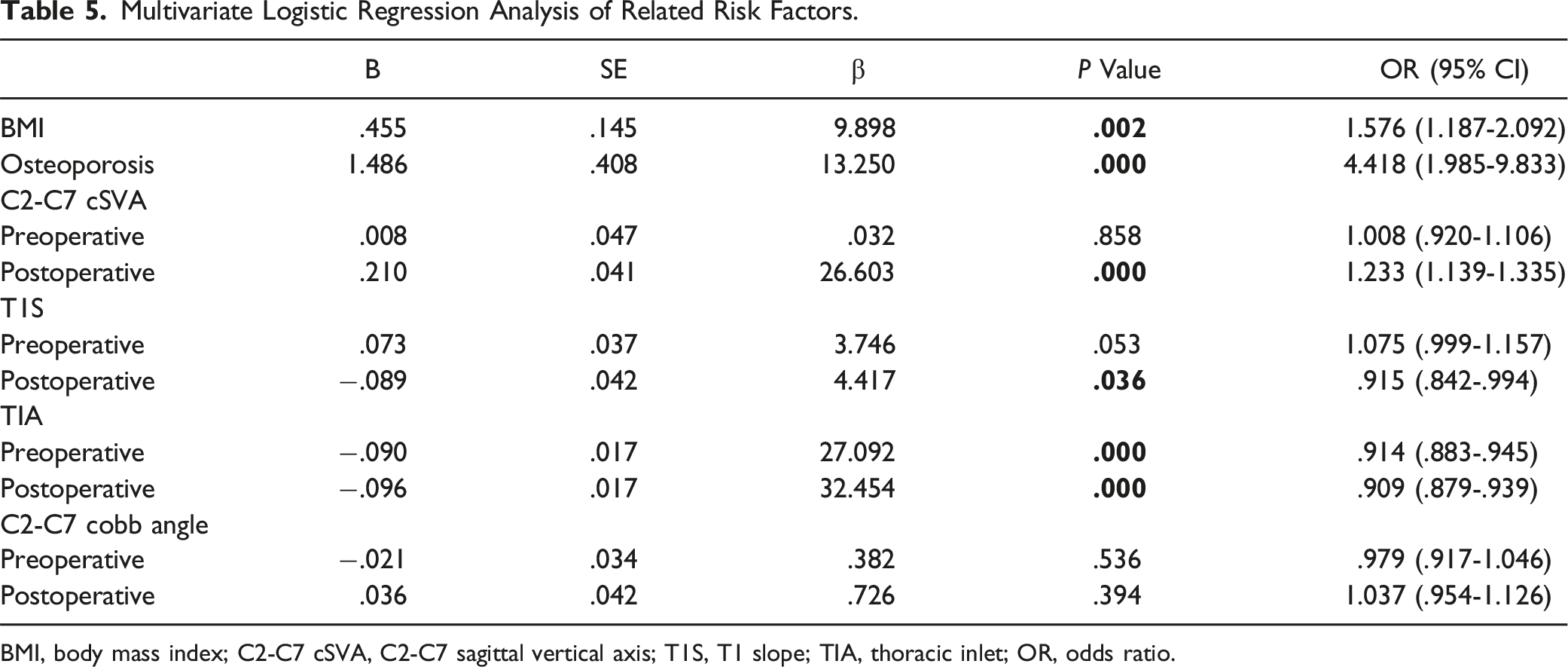
BMI, body mass index; C2-C7 cSVA, C2-C7 sagittal vertical axis; T1S, T1 slope; TIA, thoracic inlet; OR, odds ratio.
Comparison of Specific Indicators in ASD Group Before and After Revision Surgery (n = 46).
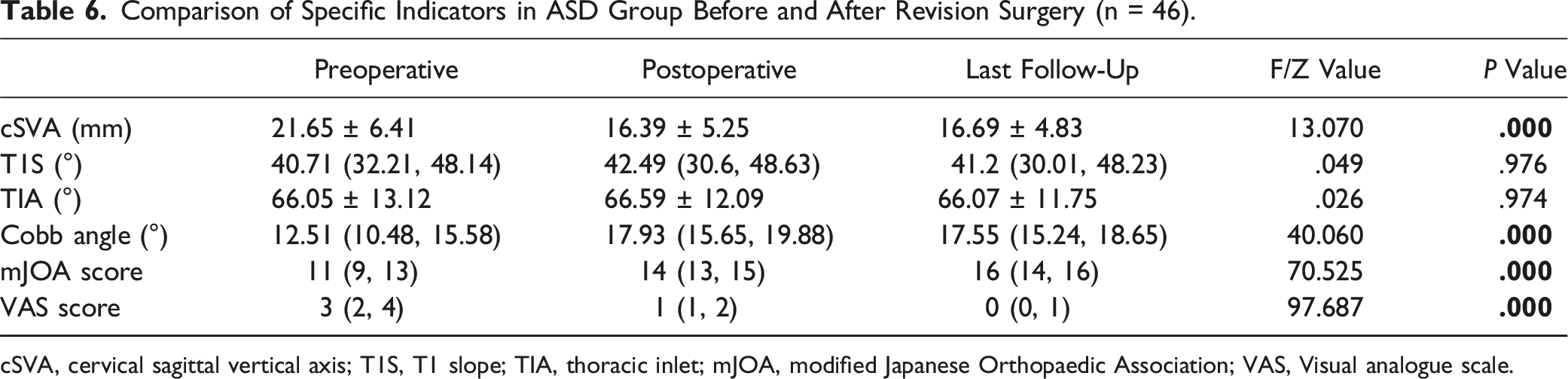
cSVA, cervical sagittal vertical axis; T1S, T1 slope; TIA, thoracic inlet; mJOA, modified Japanese Orthopaedic Association; VAS, Visual analogue scale.
Discussion
Cervical spondylosis is divided into many types, namely, cervical spondylotic radiculopathy and cervical spondylotic myelopathy. Usually, when conservative treatment fails, surgery is considered. 2 In recent decades, ACDF has been demonstrated to have good clinical effects and to be widely used. 8 However, ACDF may accelerate adjacent intervertebral disc degeneration, resulting in ASD after cervical spine surgery in the long run. ASD usually manifests as recurrent neck, shoulder or upper limb pain. 9 Park et al. found that approximately 3% of patients in the U.S. suffer from ASD each year, and the estimated incidence rate of ASD is 25% within 10 years after ACDF. 10 Additionally, Wu et al. reported that only 5.6% of patients with ASD in China had undergone revision surgeries in 10 years, and they believed that the annual incidence of ASD was .8%. 11 However, few reports have explained the risk factors and etiology of ASD. 12
Regarding demographic data in our study, there was no significant difference in sex or age between the two groups. Additionally, the mJOA and VAS scores of the two groups of patients were significantly improved after ACDF, indicating that ACDF can effectively achieve favorable clinical outcomes and improve patient quality of life, which is similar to the results reported by Chowdhury et al. 13 Furthermore, our study showed there was no significant difference in the lesion segments (single segment/multiple segments) between the two groups.
Our results showed that the severity of osteoporosis and BMI were significantly higher in the ASD group than in the NASD group (P < .05), and multivariate logistic regression analysis demonstrated that a high BMI and severe osteoporosis were independent risk factors for ASD after ACDF, which is similar to the findings reported by Lau Kenney K L et al. 14 Biomechanically, obesity will overload intervertebral discs, accelerate the degeneration of cervical intervertebral discs, and lead to the occurrence of ASD. Conversely, it has been reported that weight loss after ACDF is beneficial for decreasing surgical complications. 15 The severity of osteoporosis not only affects bone graft fusion but also may be related to the vertebral height loss of the surgical segment. Indefinite bone fusion after ACDF causes imbalance and abnormal activity in the area of the surgical segment, which accelerate the degeneration of adjacent intervertebral discs.
We also found that a larger C2-C7 SVA after ACDF was an independent risk factor for ASD. A greater C2-C7 cSVA postoperatively leads to hyperextension of the neck, causing greater forward and backward torque around the cervical spine, thereby increasing the vertical pressure on the cervical spine. At present, most surgeons only pay attention to the recovery of the C2-C7 Cobb angle and pay no attention to the impact of the C2-C7 cSVA on cervical spine degeneration. If the C2-C7 cSVA is not corrected properly after the operation, it will overload the motion segments between adjacent vertebral bodies.16-18
Furthermore, we noticed that the T1S and TIA were lower in the ASD group than in the NASD group. The results of multivariate logistic regression analysis also showed that a larger postoperative T1S and TIA after ACDF were protective factors for ASD. T1S and TIA are indicators of the sagittal balance of the T1 vertebral body, and because the upper endplate of T1 serves as the base of the cervical spine, its location greatly affects the balance of the cervical spine. There was no significant difference in the T1S or TIA before or after ACDF (P > .05), which means that these two indicators are essentially constant for individuals. Patients with a smaller T1S will bear more vertical pressure on the cervical spine, which will accelerate the degeneration of cervical intervertebral discs. With improvement in the C2-C7 Cobb angle after ACDF, 6 the cervical curvature will transform from a straight morphology to a normal physiological curvature, and the smaller T1S cannot accommodate the change in the force line conduction of the entire cervical spine. Finally, the vertebral body or intervertebral disc adjacent to the surgical segment, as a stress concentration site, will bear extra pressure, leading to the risk of ASD. The TIA, as one of the parameters that also represents the balance of the cervical spine, is positively correlated with the T1S. 19 Similarly, patients with a smaller TIA are more likely to develop ASD after ACDF because of the similar biomechanical mechanism. Previous studies have also shown that patients with a smaller T1S and TIA are less likely to develop cervical spondylosis. 20 Cervical spine surgery artificially changes the physiological curvature of the cervical spine, but T1S and TIA are constant, which leads to abnormal force conduction and the acceleration of cervical spine degeneration. To the best of our knowledge, this is the first report of the effect of T1S and TIA on ASD.
Previous studies have shown that more than two-thirds of patients with ASD require revision surgery after the failure of nonsurgical treatment.12,21 In our study, all patients with ASD underwent revision surgeries. We found that the C2-C7 SVA, C2-C7 Cobb angle, and mJOA and VAS scores of patients after revision surgery were significantly improved compared with those preoperatively (P < .05). This demonstrated that revision surgery for ASD can achieve significantly better clinical outcomes and restore the physiological curvature of the cervical spine22-24.
There are some limitations of our study, including the following points. First, this was a retrospective single-center study. Second, the number of patients included in our study was relatively small. In addition, some studies have found that compared with the use of titanium cages and titanium plates, the use of zero-profile spacers reduces the incidence of adjacent spondylopathy; however, the material properties and manufacturers of the implants used in our study were not assessed. 25 Furthermore, a titanium plate with a shorter distance from the fusion cage reduces the stress on the screws and bone graft, thereby reducing damage to the adjacent vertebral bodies. 14 Consequently, in our revision operation, a zero-profile spacer was used in all patients, but the effect of this fixation device on adjacent spondylopathy needs further exploration.
Conclusion
Patients with a high BMI, severe osteoporosis, and a large C2-C7 cSVA after ACDF have a much higher risk of postoperative ASD, while a large T1S and TIA may be protective factors for ASD. In addition, revision surgery can achieve better clinical outcomes and restore cervical spine balance in patients with ASD if conservative treatment fails.
Supplemental Material
Supplemental Material - Prevalence and Risk Factors for Cervical Adjacent Segment Disease and Analysis of the Clinical Effect of Revision Surgery: A Minimum of 5 Years’ Follow-Up
Supplemental Material for Prevalence and Risk Factors for Cervical Adjacent Segment Disease and Analysis of the Clinical Effect of Revision Surgery: A Minimum of 5 Years’ Follow-Up by Zi-han Wei, Si-zhen Yang, Ying Zhang, Jia-wen Ye and Tong-wei Chu in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the General project of Chongqing Natural Science Foundation of China (No. cstc2020jcyj‐msxmX0688), National Key Research and Development Plan Project (2016YFC1101504), and the Clinical Research Project of the Second Affiliated Hospital of the Army Military Medical University (2018XLC2016).
Ethics Declarations
Ethics approval and consent to participate the Medical Ethics Committee of the Second Affiliated Hospital Army Military Medical University. Informed consent was obtained from all participants.
Consent to Participate
Written informed consent for participation was obtained from all participants in this study. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for Publication
All the authors are consent to publish.
Availability of Data and Materials
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.