
Abstract
Study design
Retrospective Cohort Study
Objectives
To compare early postoperative radiological and clinical outcomes between 2-level minimally invasive (MIS) trans-psoas lateral lumbar interbody fusion (LLIF) and MIS transforaminal lumbar interbody fusion (TLIF) for degenerative lumbar spinal stenosis.
Methods
Fifty three consecutive patients undergoing 2-level lumbar interbody fusion from L3-L5 for degenerative lumbar spinal stenosis were enrolled. Twenty four patients underwent LLIF and 29 underwent TLIF.
Results
Operative time and length of stay were similar between LLIF and TLIF (272.8 ± 82.4 vs 256.1 ± 59.4 minutes; 5.5 ± 2.8 vs 4.7 ± 3.3 days, P > .05), whereas blood loss was lower for LLIF (229.0 ± 125.6 vs 302.4 ± 97.1mls, P = .026). Neurological deficits were more common in LLIF (9 vs 3, P = .025), whereas persistent deficits were rare for both (1 vs 1, P = 1). For both groups, all patient reported outcomes visual analogue scale (VAS back pain, VAS leg pain, ODI, SF-36 physical) improved from preoperative to 2-years postoperative (P < .05), with both groups showing no significant differences in extent of improvement for any outcome. Lateral lumbar interbody fusion demonstrated superior restoration of disc height (L3-L4: 4.1 ± 2.4 vs 1.2 ± 1.9 mm, P < .001; L4-L5: 4.6 ± 2.4 vs .8 ± 2.8 mm, P < .001), foraminal height (FH) (L3-L4: 3.5 ± 3.6 vs 1.0 ± 3.6 mm, P = .014; L4-L5: 3.0 ± 3.5 vs -.1 ± 4.4 mm, P = .0080), segmental lordosis (4.1 ± 6.4 vs -2.1 ± 8.1°, P = .005), lumbar lordosis (LL) (4.1 ± 7.0 vs -2.3 ± 12.6°, P = .026) and pelvic incidence-lumbar lordosis (PI-LL) mismatch (−4.1 ± 7.0 vs 2.3 ± 12.6°, P = .019) at 2-years follow-up.
Conclusion
The superior radiological outcomes demonstrated by 2-level trans-psoas LLIF did not translate into difference in clinical outcomes compared to 2-level TLIF at the 2-years follow-up, suggesting both approaches are reasonable for 2-level lumbar interbody fusion in degenerative lumbar spinal stenosis.
Keywords
Introduction
The incidence of multi-level degenerative lumbar disease is rising as average life expectancy increases. As such, the frequency of multi-level lumbar fusion surgeries is also increasing. 1 Minimally invasive (MIS) techniques for lumbar fusion have been developed with good clinical outcomes2,3 and potentially fewer complications compared with open procedures.3,4 However, a recent study revealed that the clinical benefits of MIS lumbar interbody fusion appear to diminish as a function of fusion length. 5 This finding may seem intuitive since the increased length of fusion compounds the complexity of the case, and are relatively infrequent compared to single-level fusions,6,7 contributing to a steeper learning curve for multilevel MIS fusions.
This raises an important question about how different approaches for MIS lumbar interbody fusion perform with increasing number of fusion levels. Two such MIS approaches that are often considered in clinical settings between similar patients and pathology 8 are MIS transforaminal lumbar interbody fusion (TLIF) and lateral lumbar interbody fusion (LLIF). In recent years, these 2 approaches have been compared, with meta-analysis establishing comparable outcomes in single-level interbody fusion. 9 However, literature suggests that outcomes may change based on the number of levels fused. A study by Wong et al revealed that the rates of durotomy in TLIF were higher with multilevel fusions than with single-level fusions. 6 Additionally, Saadeh et al concluded that neither 1-level LLIF nor 1-level TLIF had a significant impact on global sagittal alignment; however, the superior segmental lordosis correction achieved in LLIF compared with TLIF may achieve a more globally impactful correction of sagittal alignment in fusions with increased levels of fusion. 10
Lateral lumbar interbody fusion is preferred for multiple-level lumbar interbody fusion in the context of adult spine deformity as it enhances coronal and sagittal plane correction, 11 whereas TLIF is favoured in single-level fusions as it avoids the need for repositioning for supplementary posterior instrumentation which is required in LLIF. 12 While both LLIF and TLIF have been utilized for intermediate length 2-level fusions, 13 there has yet to be a direct comparison of these approaches for specifically 2-level lumbar interbody fusion. Hence our study aims to compare the 2-years clinical and radiological outcomes of MIS-TLIF against trans-psoas LLIF for 2-level lumbar interbody fusion.
Materials and Methods
A retrospective analysis was performed on the prospectively collected clinical and radiographic records of 53 consecutive patients who underwent 2-level MIS-TLIF and 2-level LLIF from 2010 to 2018 performed by 2 fellowship trained surgeons with 10 years of working experience. Inclusion criteria included patients undergoing 2-level lumbar interbody fusion at L3/4 and L4/5 for degenerative lumbar spinal stenosis. All patients had symptomatic mechanical back pain associated with radicular pain, intermittent neurological claudication and failed at least 6 months of conservative management. Patients undergoing revision surgery, with prior L5-S1 fusion surgery, spondylolisthesis of grade 2 or more, severe coronal deformity (Cobb angle greater than 20°), concomitant tumour, previous trauma or infection were excluded.
Factors Determining Selection of LLIF vs TLIF
The decision to perform LLIF vs TLIF was based on both technical factors and patient factors. In terms of technical factors, upon reviewing the pre-operative MRI scans, patients with suitable lateral corridors were allowed to undergo the LLIF procedure. 12 Patients who required significant attention to PI-LL mismatch were preferentially selected by the surgeon to undergo LLIF. However, beyond these technical considerations, patient preference still took precedence in choice of LLIF vs TLIF . Patients were counselled that the LLIF approach would require a 2-step procedure (including repositioning for posterior instrumentation) with 2 incision sites compared to the 1-step procedure performed in TLIF. Additionally, the risk of transient thigh discomfort in LLIF 12 was counselled, and patients who were candidates for LLIF were empowered to decide between these 2 options.
Baseline Characteristics of Participants
Baseline Characteristics of LLIF vs TLIF Groups.
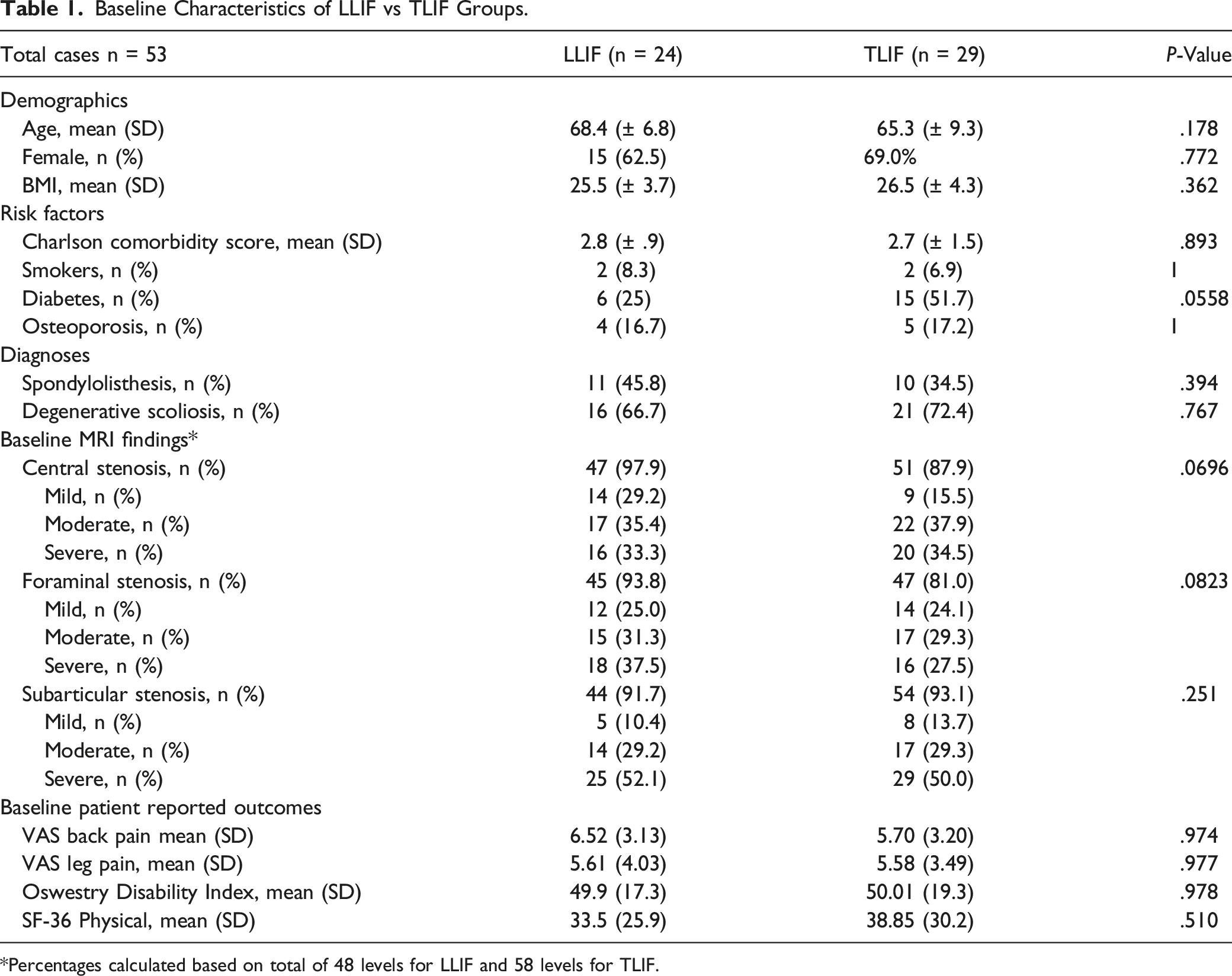
*Percentages calculated based on total of 48 levels for LLIF and 58 levels for TLIF.
Clinical Outcomes
Perioperative outcomes included surgery time, intraoperative blood loss, and hospitalization period. Additionally, complications and reoperations were recorded at all relevant peri- and postoperative time points. Patient reported outcomes 20 were collected by trained personnel not directly involved in the study, at baseline and at each postoperative visit (1, 3, 6 and 24 months) and included Oswestry disability index (ODI), back and leg pain visual analogue scale (VAS) and the SF-36 physical component score (PCS).
Radiographic Outcomes
Preoperative, immediate postoperative and 2-years postoperative anteroposterior and lateral radiographs of the lumbar spine with the subjects in an upright standing neutral position were obtained. All quantitative radiological parameters were measured by 2 authors on 2 separate occasions, with the average scores utilized. The quantitative radiological parameters include: (1) disk height (DH; the mean of the anterior and posterior disc heights,
21
defined as the distance between the inferior to superior vertebral endplates at the anterior and posterior vertebral margins respectively
22
), (2) foraminal height (FH; the distance from the inferior pedicle wall to superior pedicle wall of the level below
23
) (3) segmental lordotic angle (SLA; angle between the upper and lower endplates of the L3-L5 fused segment
24
), (4) lumbar lordosis (LL; angle between the upper endplates of both L1 and S1
24
), (5) pelvic tilt (PT; angle between the line joining the midpoint of the upper endplate of S1 with the centre of the hip joint and a vertical line
25
), (6) pelvic incidence (PI; angle between an inferior perpendicular line from the midpoint of the S1 endplate and a line extending from the midpoint of S1 endplate towards the centre of the femoral head
25
), (7) pelvic incidence-lumbar lordosis mismatch (PI-LL; the numerical difference between PI and LL
26
). (Figure 1). The overall intraobserver reliability was excellent
27
at .993 and .994, while the interobserver reliability was good to excellent
27
for all outcomes (ranging from .784 to .978). Qualitative radiological outcomes included (1) fusion according to the Bridwell Fusion grading system,
28
(2) cage subsidence (≥ 3-mm loss of disc height between postoperative and last follow-up
29
), (3) cage migration ( > 2 mm posterior migration between postoperative and last follow-up
30
), and (4) adjacent segment disease (ASD; new degenerative changes found at spinal levels adjacent to the treated levels, accompanied by neurological symptoms.
31
) Diagrammatic depictions of the quantitative radiological outcomes utilized in this study, including disc height, foraminal height, segmental lordotic angle, lumbar lordosis, pelvic tilt and pelvic incidence.
Surgical procedure for MIS-TLIF
Minimally invasive-TLIF was performed as described by Schwender et al. 4 Capstone cages (Medtronic PLC., Fridley, MN, USA) were used in all cases. The cages were filled with demineralized bone matrix and local autograft bone obtained from unilateral total facetectomy. The cage height and width ranged from 7 to 14 mm, and 26 to 32 mm respectively, with cage angle ranging from 0 to 6°. Posterior bilateral percutaneous pedicle screw fixation with intraoperative 3D-CT based navigation guidance was performed. Compression to increase segmental lordosis was not routinely performed.
Surgical procedure for LLIF
The general technique for transpsoas LLIF has been described previously.
32
Coroent cages (NuVasive Inc., San Diego, CA, USA) were utilized in all cases. One half each of autogenous iliac bone graft and synthetic bone graft (collagen hybrid) were placed in the cages. The cage width, height, and length ranged from 45 to 60 mm, 8 to 12 mm, and 18 to 22 mm, respectively, with a mixture of 10° lordotic and parallel cages utilized based on surgeon’s discretion. After cage placement, each patient was repositioned prone onto a Jackson table and underwent posterior bilateral percutaneous pedicle screw fixation with intraoperative 3D-CT based navigation guidance. Direct decompressions were not performed in LLIF patients. (Figure 2). (A) preoperative, (B) immediate post-operative and (C) 2-years postoperative erect plain lateral radiographs for a patient who underwent LLIF using Coroent cages with 10° lordosis, displayed alongside the (D) preoperative, (E) immediate post-operative and (F) 2-years postoperative radiographs from a patient who underwent TLIF using Medtronic Capstone cages with 0° lordosis.
Post-operative rehabilitation
Patients underwent standardised post-operative rehabilitation involving adequate analgesia, bed exercises and transferring out of bed. Patients were allowed to weight bear from post-operative day 1 under supervision from an inpatient physiotherapist. Patients were allowed home once deemed safe by the physiotherapist.
Ethics approval
Institutional review Board exemption was granted for this study and informed consent was not required.
Statistical analysis
SPSS version 21.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Fisher’s exact and independent T test were used to compare outcomes between the 2 groups (LLIF and TLIF). Paired testing was used to compare preoperative to postoperative time points within groups. Intraclass correlation coefficient were used to ascertain intraobserver and interobserver reliability. Statistical significance was defined at P < .05.
Results
Perioperative Results
Comparison of Perioperative Outcomes in LLIF vs TLIF.

Patient Reported Outcomes
All patient reported outcomes improved in both LLIF and TLIF groups at the 2-years follow-up compared to baseline (P < .05), with no difference between LLIF and TLIF in extent of improvement for any outcome (P > .05). Comparing baseline against 2-years follow-up, for the LLIF and TLIF groups respectively, VAS-back pain improved from 6.5 ± 3.1 to 2.3 ± 3.6 and from 5.7 ± 2.9 to 1.3 ± 2.7, VAS-leg pain improved from 5.6 ± 4.0 to 2.2 ± 4.1 and from 5.6 ± 3.5 to .8 ± 2.4, ODI improved from 49.9 ± 17.3 to 24.5 ± 25.9% and from 50 ± 19.3 to 16.2 ± 16.6%, and PCS improved from 36.4 ± 26.4 to 62.2 ± 26.9 and from 38.8 ± 30.2 to 65.8 ± 26.7. (Figure 3). Graphs showing changes over time between the LLIF and TLIF groups across VAS back and leg pain, ODI and SF-36 Physical. Both groups experienced significant improvements (P < .05) from baseline to 2-years.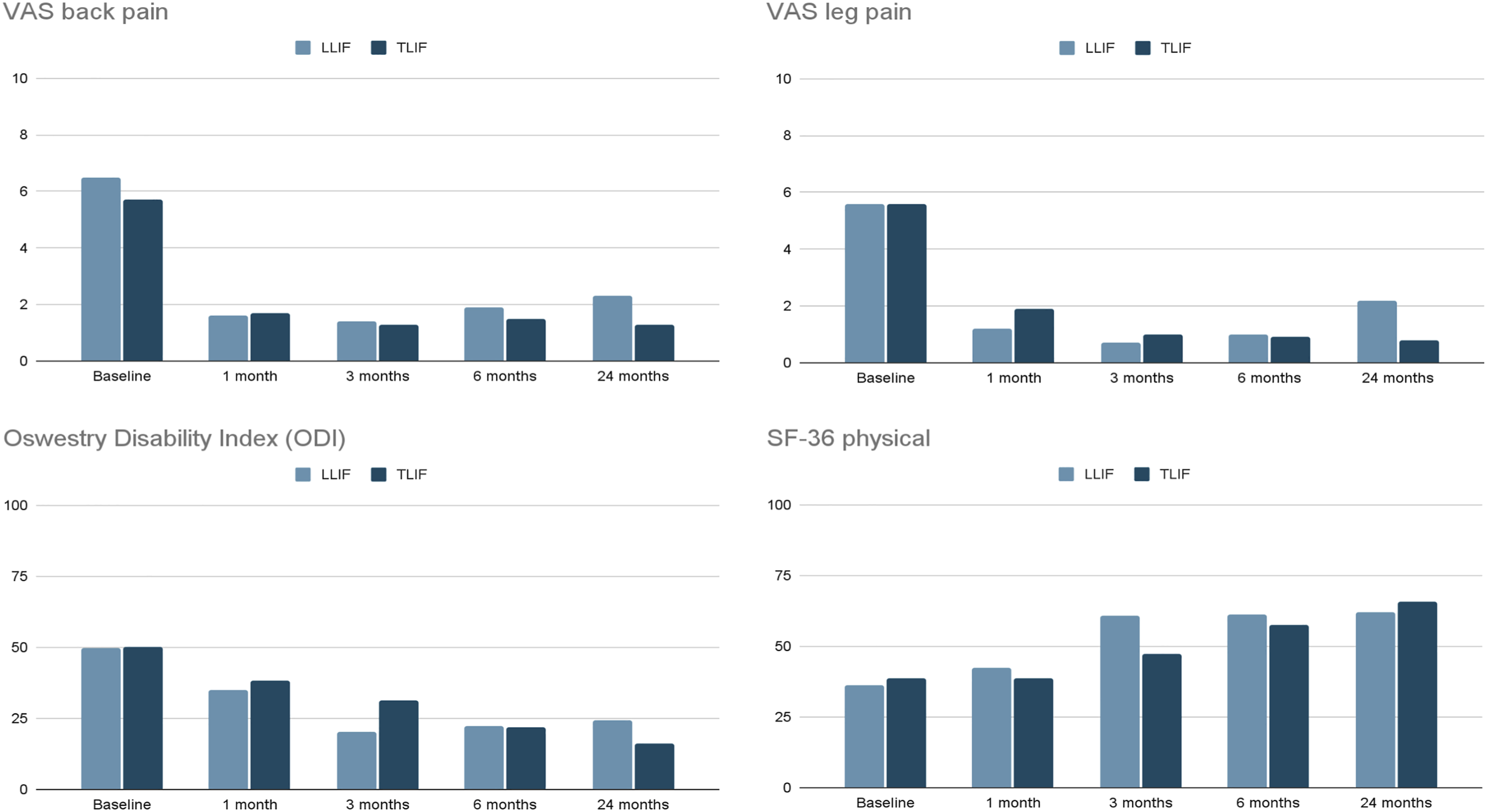
Radiographic Outcomes
Preoperative measurements
Comparison of Preoperative Measurements for Radiological Outcomes.
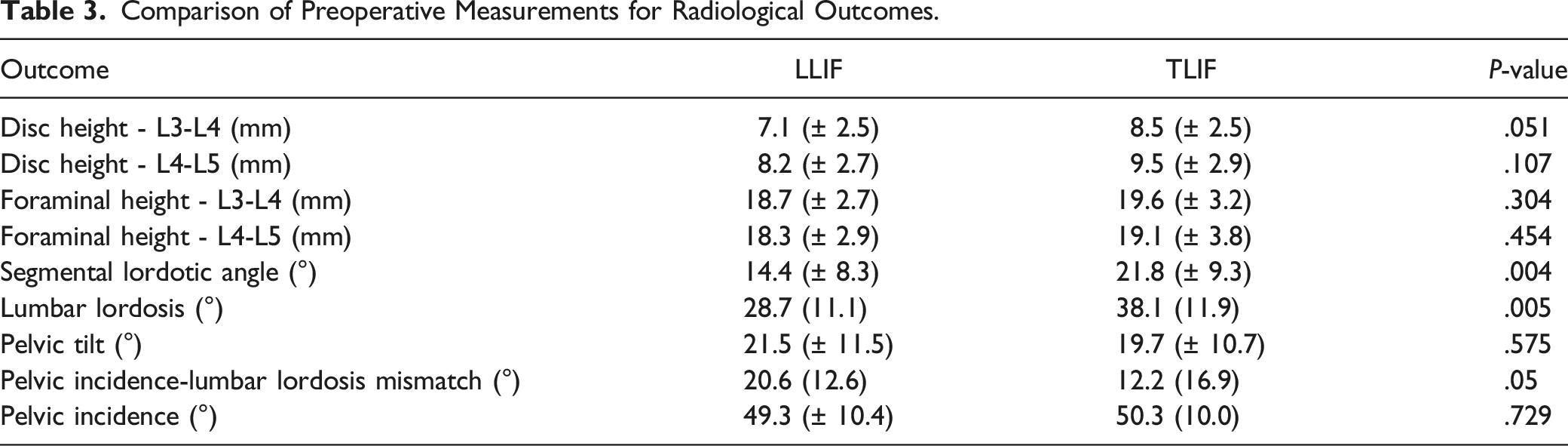
Preoperative SLA was smaller in the LLIF group compared to the TLIF group (14.4° vs 21.8°, P = .004). Similarly, preoperative LL was smaller in LLIF compared to TLIF (28.7° vs 38.1°, P = .005). Moreover, preoperative PI was similar between LLIF and TLIF groups (49.3° vs 50.3°, P = .729), hence PI-LL discrepancy was greater in the LLIF group compared to the TLIF group (20.6° vs 12.2°, P = .05). Preoperative PT was similar between LLIF and TLIF groups (21.5°vs 19.7°, P = .575).
Disc height
Comparison of Disc Height and Foraminal Height in LLIF vs TLIF.
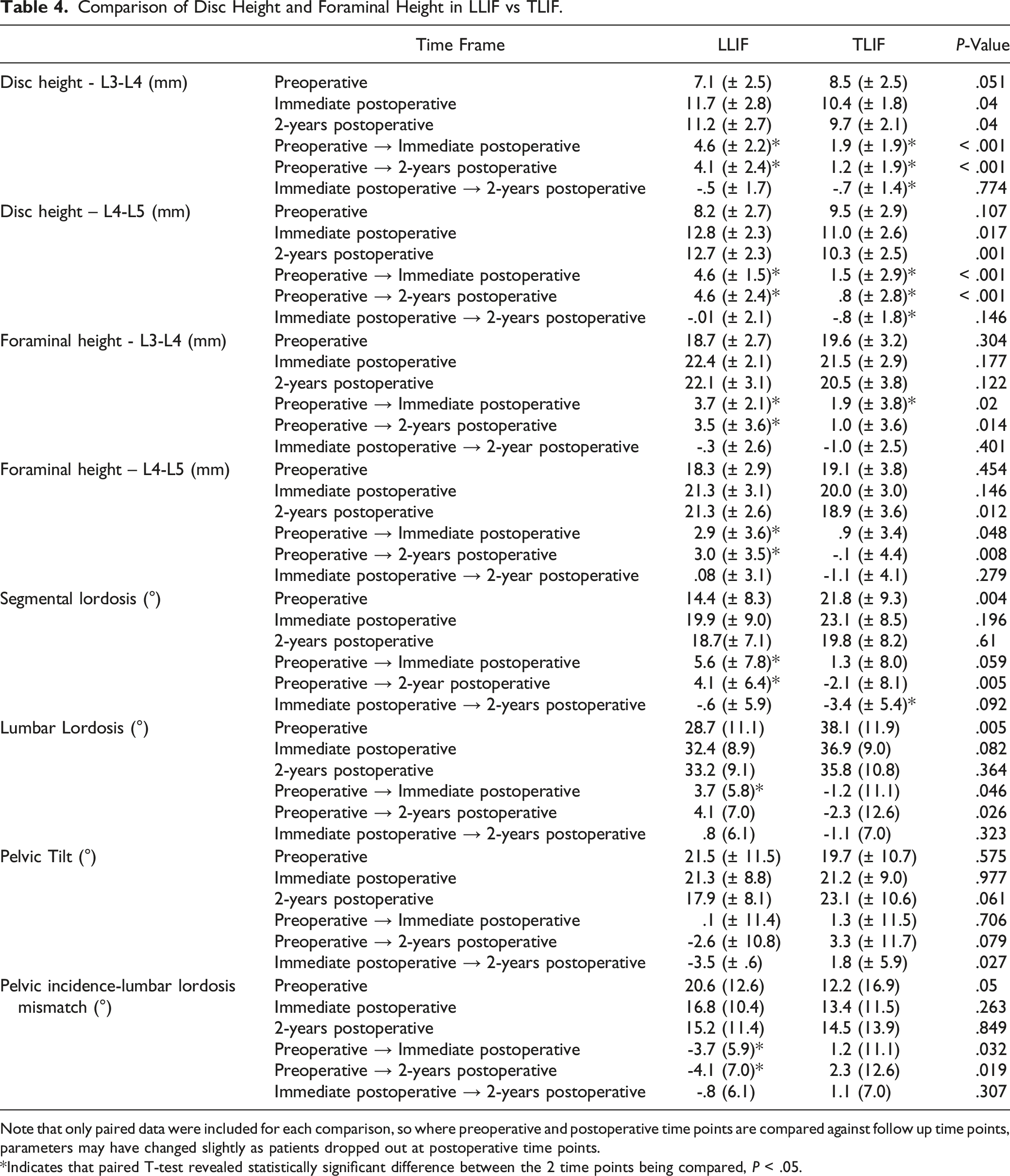
Note that only paired data were included for each comparison, so where preoperative and postoperative time points are compared against follow up time points, parameters may have changed slightly as patients dropped out at postoperative time points.
*Indicates that paired T-test revealed statistically significant difference between the 2 time points being compared, P < .05.
Foraminal Height
Foraminal Height was significantly increased in the LLIF group postoperatively, and at the 2-years follow-up for both L3-L4 and L4-L5 segments. Conversely in the TLIF group, changes in FH were statistically insignificant over the course of 2 years. Overall, there was greater improvement in FH at the 2-years follow-up in LLIF compared to TLIF (L3-L4: 3.5 mm vs 1.0 mm, P = .014; L4-L5: 3.0 mm vs -0.1 mm, P = .008).
Segmental lordosis angle
Segmental lordosis angle was significantly increased in the LLIF group postoperatively and at the 2-years follow-up. Conversely in the TLIF group, changes in SLA over the course of 2 years were statistically insignificant. Overall, there was greater increase in SLA at the 2-years follow-up in LLIF compared to TLIF (4.1 ± 6.4° vs -2.1 ± 8.1°, P = .005).
Lumbar lordosis
Lumbar lordosis was significantly increased in the LLIF group postoperatively and at the 2-years follow-up. Conversely in the TLIF group, changes in LL were statistically insignificant over the course of 2 years. Overall, there was greater improvement in LL at the 2-years follow-up in LLIF compared to TLIF (4.1° vs -2.3°, P = .026).
Pelvic tilt
The LLIF group exhibited a decreasing trend in PT at the immediate postoperative and 2-years follow-up, but this was not statistically significant. Similarly in the TLIF group, changes in PT over the course of 2 years were statistically insignificant. Overall, comparing LLIF to TLIF, there was no statistically significant difference in change in PT at the 2-years follow-up (-2.6° vs 3.3°, P = .079).
Pelvic incidence-lumbar lordosis mismatch
Pelvic incidence-lumbar lordosis was reduced significantly in the LLIF group postoperatively and at the 2-years follow-up. Conversely in the TLIF group, changes in PI-LL were statistically insignificant over the course of 2 years. Overall, there was greater reduction in PI-LL mismatch at the 2-years follow-up in LLIF compared to TLIF (-4.1° vs 2.3°, P = .019).
Additionally, LLIF demonstrated an increase in the proportion of patients with PI-LL < 10° at the 2-years follow-up, but this was not statistically significant (.21 to .38, P = .34). Conversely, for TLIF, the proportion of patients with PI-LL < 10° remained constant at the 2-years follow-up (.38 to .41, P = 1).
Fusion and cage positioning
Comparison of Qualitative Radiological Outcomes in LLIF vs TLIF.
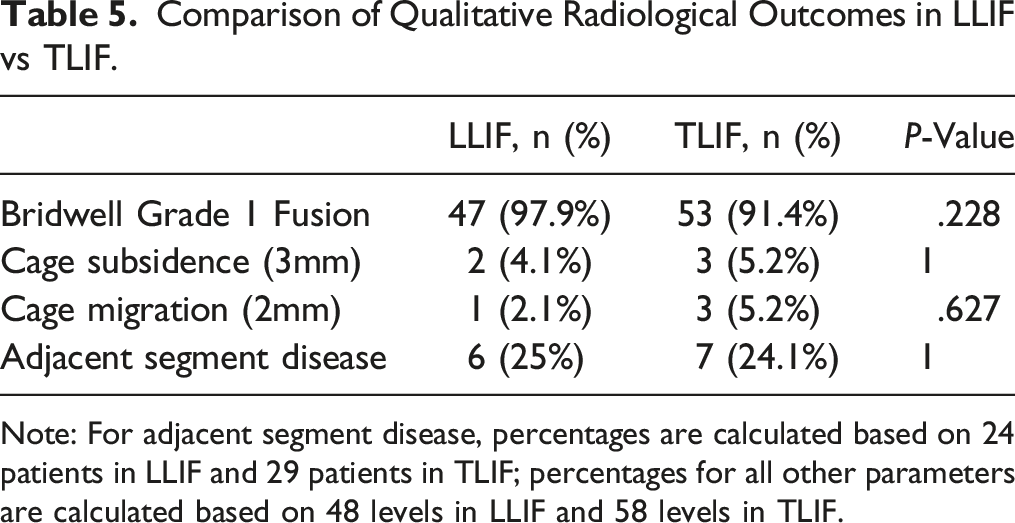
Note: For adjacent segment disease, percentages are calculated based on 24 patients in LLIF and 29 patients in TLIF; percentages for all other parameters are calculated based on 48 levels in LLIF and 58 levels in TLIF.
Complications
Comparison of Complications in LLIF vs TLIF.
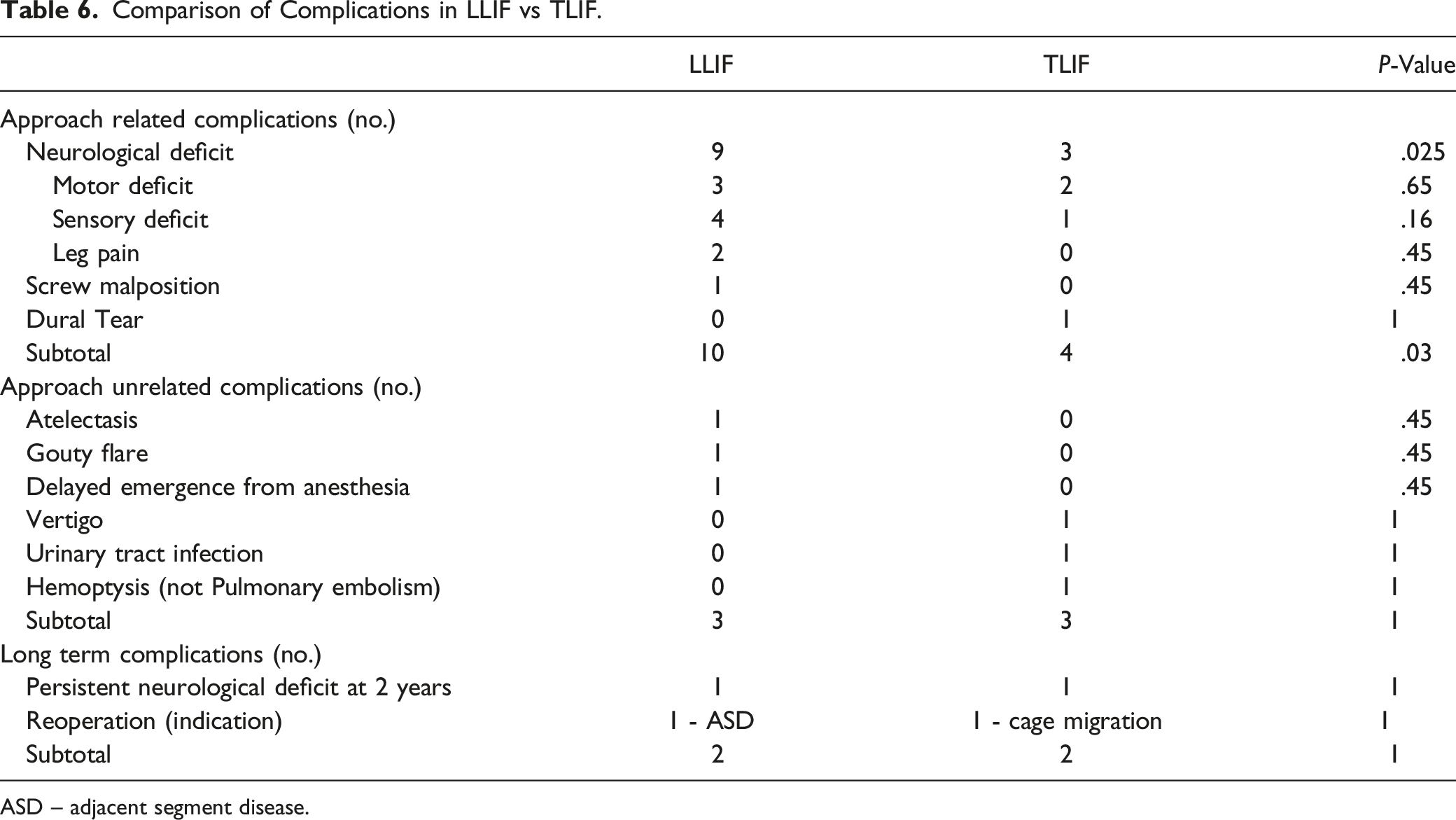
ASD – adjacent segment disease.
Discussion
While numerous studies have reported clinical and radiological outcomes of both the LLIF and MIS-TLIF procedures, comparative studies between the procedures have remained scarce, 9 and to our knowledge this is the first comparative study of 2-level LLIF vs 2-level MIS-TLIF. Our main findings include that 2-level LLIF demonstrated superior radiological outcomes compared to 2-level TLIF, but this did not translate into any significant difference in clinical outcomes at the 2-years follow-up. Moreover, perioperative performance and rates of persistent complications were comparable between 2-level LLIF and 2-level TLIF.
Radiological Outcomes
For radiological measures of indirect decompression, our study revealed that LLIF was superior to TLIF in DH, FH and SLA restoration. These results are expected as the approach of the LLIF procedure facilitates disc distraction at the disc midline 33 and placement of larger cages which span over the epiphyseal ring compared to a TLIF cage which spans the central and weakest region of the endplate, 34 accounting for difference in cage subsidence. 35 Furthermore, the indirect approach confers SLA restoration as it facilitates implant placement anteriorly within the disk space, 36 and utilization of wedge-shaped lordotic cages. 37 Our results are similar to studies comparing 1-level LLIF to 1-level TLIFs, which also found that LLIF is superior to TLIF in improving intervertebral DH,37,38 FH37,39 and segmental lordosis angle.10,37,38
Moving beyond single-level fusions, Saadeh et al 10 postulates that a multi-segmental fusion may result in a more globally impactful correction in sagittal alignment compared to single-level fusions, since each additional disc level contributes to the overall LL. Concordant with this reasoning, our study found that 2-level LLIFs displayed greater restoration of sagittal alignment, including greater restoration of LL and PI-LL mismatch compared to 2-level TLIF. Moreover, our study focused on the 2-level segment from L3-L5, which are levels known to contribute significantly to overall LL, 37 hence increased lordosis from each segment as seen in LLIF would impact overall sagittal alignment. This is a significant finding as previous studies have found that short segment fusions have no impact on overall global sagittal alignment. 10
Clinical Outcomes
Sagittal alignment has long been known to affect clinical outcomes. 40 This was previously defined by an increased sagittal vertical axis, although more recently scores have been developed to account for pelvic incidence, PT and LL. 41
Despite our findings that there was superior restoration of sagittal alignment in LLIF compared to TLIF, there were no differences in clinical outcomes at the 2-years follow-up. Both LLIF and TLIF showed significant improvements in all patient-reported outcomes from preoperative to 2-years follow-up measurements, with no significant differences between LLIF and TLIF in terms of extent of improvement in any outcome. One possible explanation is that the absolute differences in radiologic parameters between both procedures were small and thus not clinically significant. 9 More importantly, our 2-years follow-up period may have been inadequate to assess the long term impact of correction of sagittal alignment. More long term studies comparing 2-level fusions are required to compare downstream clinical outcomes.
Perioperative Performance and Complications
In terms of perioperative performance, the LLIF group had lower intraoperative blood loss compared to the TLIF group, which is expected and related to the differences in approach.42-44 Other measures including operation time and length and hospital were equivalent, suggesting that LLIF and TLIF are both good options for 2-level interbody fusion. Notably, considering the LLIF requires intraoperative repositioning to complete supplementary posterior instrumentation with bilateral pedicle screws, 12 the equivalent operating time in both groups suggests that the LLIF approach may continue to offer more time savings with increasing number of fusion levels. Surgeons also should not avoid offering LLIF in intermediate 2-level fusions out of concerns of longer operative time, especially if patients are good candidates for it.
In terms of surgical complications, we found that the LLIF group was more prone to neurological deficits compared to TLIF group (9 vs 3). Neurological injury is a well-documented surgical complication related to the LLIF approach 45 as surgical access via the retroperitoneal window intrinsically places the psoas muscle, lateral femoral cutaneous nerve, genitofemoral nerve, and lumbosacral plexus46-48 at risk. However, similar to other studies,49,50 a large proportion of these neurological deficits were transient. The results from our study confirm that the distinct approach related complications of LLIF and TLIF should continue to be anticipated in 2-level fusions, and that both LLIF and TLIF are comparable in terms of persistent complication rate at the 2-years follow up. More long term studies comparing complications of 2-level fusions are required.
Limitations of Study
The small sample size of this study can lead to type 2 error. Additionally, in view of the retrospective nature of our study and the technical considerations involved in selecting patients for each procedure as outlined in the methodology section, there were differences in radiological outcomes at baseline, reflecting surgeon preference in selecting patients who require greater correction of sagittal alignment for the LLIF procedure. Whilst this presents a limitation in terms of comparability of radiological outcomes achieved by LLIF vs TLIF (as the radiological measurements were not the same at baseline), the results from the study were still able to establish that LLIF in a relatively short 2-level fusion can still achieve significant improvements in global sagittal alignment – especially when the correct surgical candidates (who require correction in PI-LL mismatch) are selected for LLIF. Additionally, despite the limitation in comparability of radiological outcomes achieved by LLIF vs TLIF, other baseline characteristics including preoperative demographics, risk factors, diagnosis and MRI findings were similar between the LLIF and TLIF cohorts. Hence our study still provides valuable comparisons of perioperative outcomes, complication rates and patient reported outcomes between the 2 groups. Finally, our study had a relatively short follow-up period. A larger study with a longer follow-up period is necessary to provide additional data on the optimal surgical approach and longevity for 2-level lumbar interbody fusion. Potential outcome differences between 2-level LLIF and 2-level TLIF may be picked up given a longer horizon considering the potential increased stability and longevity of LLIF constructs given that the wider corridor into the disk space in LLIF allows greater release and placement of a larger implant, which provides a greater surface area for anterior column support and decreases the risk of subsidence. 10 Furthermore, the impact of LLIF’s superior restoration of sagittal alignment may also be better appreciated over a longer horizon, as disequilibrium of sagittal balance may lead to adjacent level syndrome and hardware failure, as well as further consequences on underling segments and joints, 11 the underlying processes for which may take time to manifest in significant impact on clinical outcomes.
Strengths of Study
This is the first head-to-head comparison of 2-level LLIF against 2-level TLIF. Our study cohort comprised a consecutive series of patients operated on by 2 senior surgeons from the same institution; both surgeons followed the same protocol for the LLIF and TLIF procedures, avoiding potential cross-institution variation in surgical technique or approach which may affect outcomes, as well as variation in data collection. Both clinical and radiological outcomes were prospectively collected in an electronic medical database and retrospectively analysed.
Conclusion
The superior radiological outcomes demonstrated by 2-level trans-psoas LLIF did not translate into any difference in clinical outcomes compared to 2-level TLIF at the 2-years follow-up, suggesting the need for more studies with longer follow-up to investigate potential downstream clinical outcomes. The current outcomes at 2-years follow-up suggest both LLIF and TLIF approaches are reasonable options for 2-level lumbar interbody fusion in degenerative lumbar spinal stenosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.