
Abstract
Study Design
Systematic review of the literature and subsequent meta-analysis for the development of a new guideline.
Objectives
This manuscript summarizes the recommendations from a new clinical guideline published by the German Spine Society. It covers the current evidence on recommendations regarding the indication, test blocks and use of radiofrequency denervation. The guidelines aim is to improve patient care and efficiency of the procedure.
Methods
A multidisciplinary working group formulated recommendations based on the Grades of Recommendations, Assessment, Development, and Evaluation (GRADE) approach and the Appraisal of Guidelines for Research and Evaluation II (AGREE II) instrument.
Results
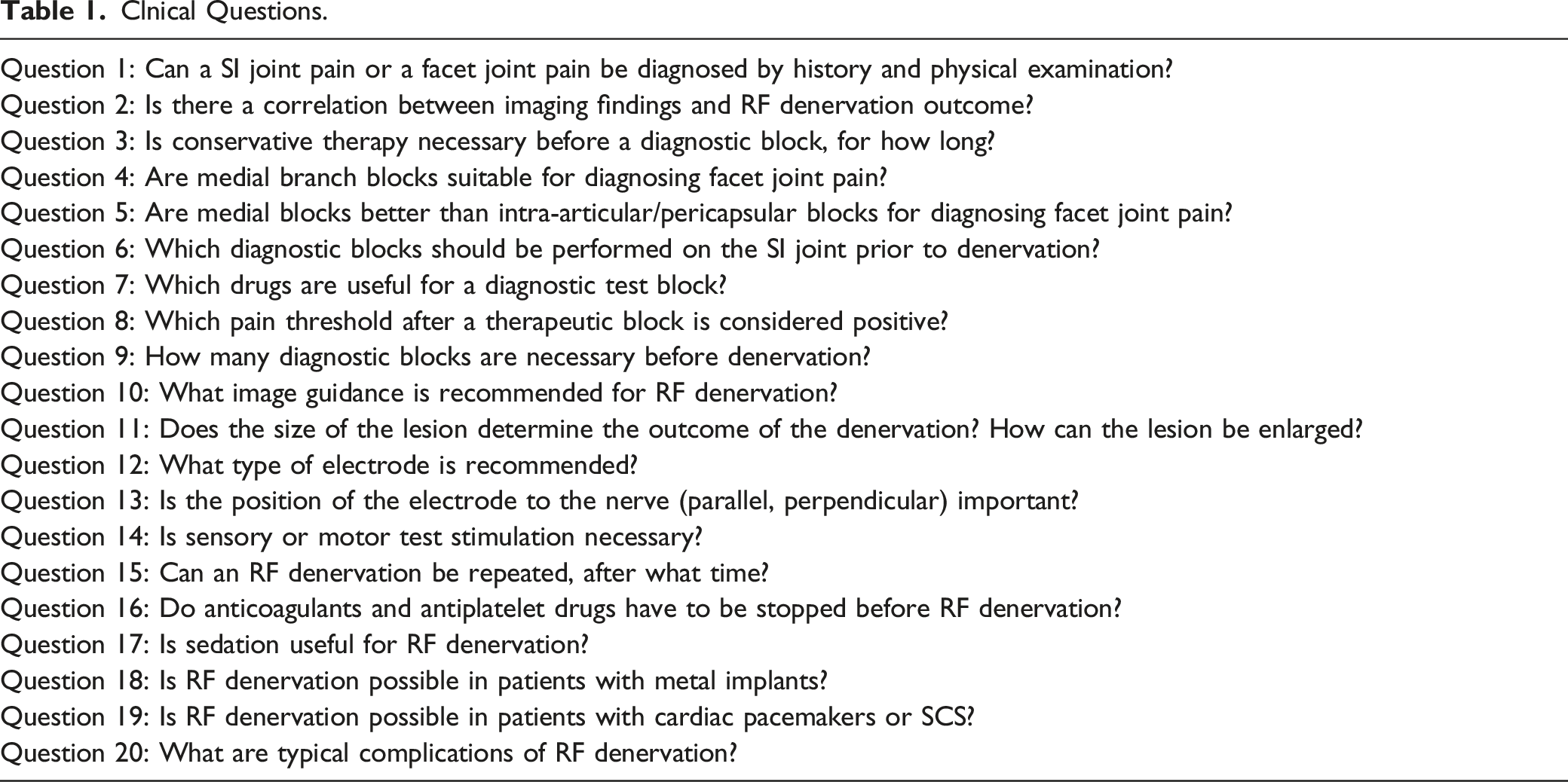
20 clinical questions were defined for guideline development, with 87.5% consensus achieved by committee members for one recommendation and 100% consensus for all other topics. Specific questions that were addressed included clinical history, examination and imaging, conservative treatment before injections, diagnostic blocks, the injected medications, the cut-off value in pain-reduction for a diagnostic block as well as the number of blocks, image guidance, the cannula trajectories, the lesion size, stimulation, repeat radiofrequency denervation, sedation, cessation or continuation of anticoagulants, the influence of metal hardware, and ways to mitigate complications.
Conclusion
Radiofrequency (RF) denervation of the spine and the SI joint may provide benefit to well-selected individuals. The recommendations of this guideline are based on very low to moderate quality of evidence as well as professional consensus. The guideline working groups recommend that research efforts in relation to all aspects of management of facet joint pain and SI joint pain should be intensified.
Keywords
Introduction
Pain originating from the joints of the spine is a frequent cause of pain and is classified as specific back pain. The structure of the facet joints in the spine is similar to other synovial joints which are richly supplied with nociceptors. 1 They can therefore be a source of pain in the cervical, thoracic, and lumbar spine. The sacroiliac joint is an amphiarthrosis, in combination with the posterior ligaments it is also a possible specific cause of pain.
The prevalence of facet joint pain in the lumbar spine varies in the literature, acknowledging the age dependency of specific anatomical structures causing pain. 2 Over the age of 55, the facet joints are the most common source of back pain, followed by the SI joint, since degenerative changes and arthrosis tend to increase with rising age.
These different prevalences can be explained, among other things, by the fact that it is difficult to identify facet joint pain with great diagnostic certainty. 3 History and clinical examination are important and useful in making the suspected diagnosis, but there is no single clinical test protocol that is pathognomonic for facet joint pain. 4 For the SI joint, the combination of several clinical tests can provide some diagnostic certainty. 5 Additionally, the correlation between degenerative findings in spinal imaging and pain is also poor.6,7
Nevertheless, it is important to prove a specific cause of pain with sufficient diagnostic certainty since RF denervation classifies as a therapeutic method for specific back pain. RF denervation is only indicated if specific facet joint pain or SI joint pain is confirmed. Test blocks are therefore performed with a local anesthetic to confirm the diagnosis. However, there are differences in the literature both in the technique of the test block and in the interpretation of the results. Intra-articular injections into the joint space or injections into the joint capsule are possible.8,9 Alternatively, the 2 nerves supplying the joint are blocked with local an anesthetic (medial branch block). 10 How much pain reduction is necessary for the test block to be considered positive is handled differently in the studies. As with any other test, there are false-positive and false-negative results. 11 To increase the diagnostic validity, a number of authors recommend to verify the result of the first test block by repeating it with local anesthetics of different durations (comparative block) or at least to perform a repeated block. 12
These diagnostic questions are relevant for the therapeutic options. The indication for RF denervation and the different approaches to test blocks have a significant impact on the subsequent denervation result. For this reason, questions on clinical history, physical examination, imaging, and diagnostic interventions were included in the guideline so that recommendations and statements are also made on these issues.
The idea of RF denervation is the interruption of the conduction of nociceptive information by coagulation of the afferent nerves (medial branch) of the facet joints. 13 The goal is to coagulate a reasonable length of the nerve because evidence exists that the length of the segment of nerve that was obliterated correlates with the duration of pain reduction after RF denervation. 14 The size of the lesion depends on the diameter of the electrode, the specific protocol of increasing reaching the target temperature and the target temperature itself, the duration of the application, the number of lesions and the cannula position. 15 It seems obvious that a parallel position of the electrode to the targeted nerve coagulates a longer distance than a perpendicular position. 16 Regarding all these parameters mentioned and also with regard to the electrode position to the nerve, there is no uniform procedure in the studies carried out to date.
Methods
Study Design
The guideline of the German Spine Society is based on a critical systematic review of the literature followed by a meta-analysis of evidence. The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach 17 was used for assessing the overall quality (strength) of evidence for a specific outcome. The quality of evidence is described as high, moderate, low, or very low, based on the confidence that the observed effect sizes reflect the true effect. 18
The final guideline was appraised using the Appraisal of Guidelines for Research and Evaluation II (AGREE II) criteria 19 to assess the validity of the guideline and the development process and to determine major areas of deficiency. Informed consent or Institutional Review Board approval is not necessary for a systematic literature review.
Work Process
The guideline was developed under the auspices of the “Deutsche Wirbelsäulengesellschaft” (DWG, German Spine Society). DWG is the largest specialist spine society in Europe with an interdisciplinary forum for basic researchers and those working in conservative and surgical treatment.
A representative multidisciplinary work group was assembled by invitation from relevant professional organizations and scientific associations. The working group was composed of orthopedic and trauma surgeons, neurosurgeons, an anesthesiologist, and a patient representative. They were involved in all parts of the process including formulating 20 clinical PICO questions (patient/intervention/comparator/outcome), 20 selecting literature, data extraction, rating the quality of evidence, and formulating recommendations. One in-person meeting and several webinars were used throughout the process. Three levels of recommendations were used: A: strong recommendation, B: weak recommendation and 0: open recommendation. If there was no evidence in the literature, an expert consensus (EC) was noted.
Finally, a modified Delphi pre-match was conducted by letter. All elected representatives were able to vote anonymously on the statements and recommendations. The final consensus conference took place under the neutral moderation of the Association of the Scientific Medical Societies of Germany (AWMF). The guideline was internally and externally appraised; results of these reviews, a summary of the final voting, as well as any substantial changes to the guideline were documented. Finally, the work was approved by the AWMF using Appraisal of Guidelines for Research and Evaluation II (AGREE II) criteria. 19
Systematic Review of Evidence
For each of the clinical questions, a systematic search strategy consisting of 3 consecutive steps was followed: Firstly, national and international guideline databases were searched for clinical guidelines regardless of the age of the guideline. Seven International, European and North American guidelines were evaluated.4,21-27 Secondly, the Cochrane Library was searched for systematic reviews. A review of RF denervation from 2015 28 was covered. The literature mentioned in this review was evaluated. Thirdly, Medline and the Cochrane Library were searched for randomized clinical trials (RCTs) and clinical observational studies. The date of the Cochrane review (2015) was used as the lower limit for the new search in step 3. The lead reviewer screened and retrieved titles and abstracts. Potentially eligible papers were then collected in full text and screened for inclusion or exclusion.
The overall quality of evidence was determined using methods outlined by the GRADE Working Group. 17 In general, the risk of bias, consistency, directness, precision, and publication bias were assessed across included studies for each critical or important outcome. The final overall quality of evidence expresses the confidence that the effect estimate lies close to the true effect: high confidence that the estimate reflects the true effect, moderate confidence, low confidence, or very low confidence; the true effect is likely to be substantially different from the estimated effect.
Results
Clnical Questions.
Question 1: Can a SI Joint Pain or a Facet Joint Pain be Diagnosed by History and Physical Examination?
Pain Maps Cervical Spine
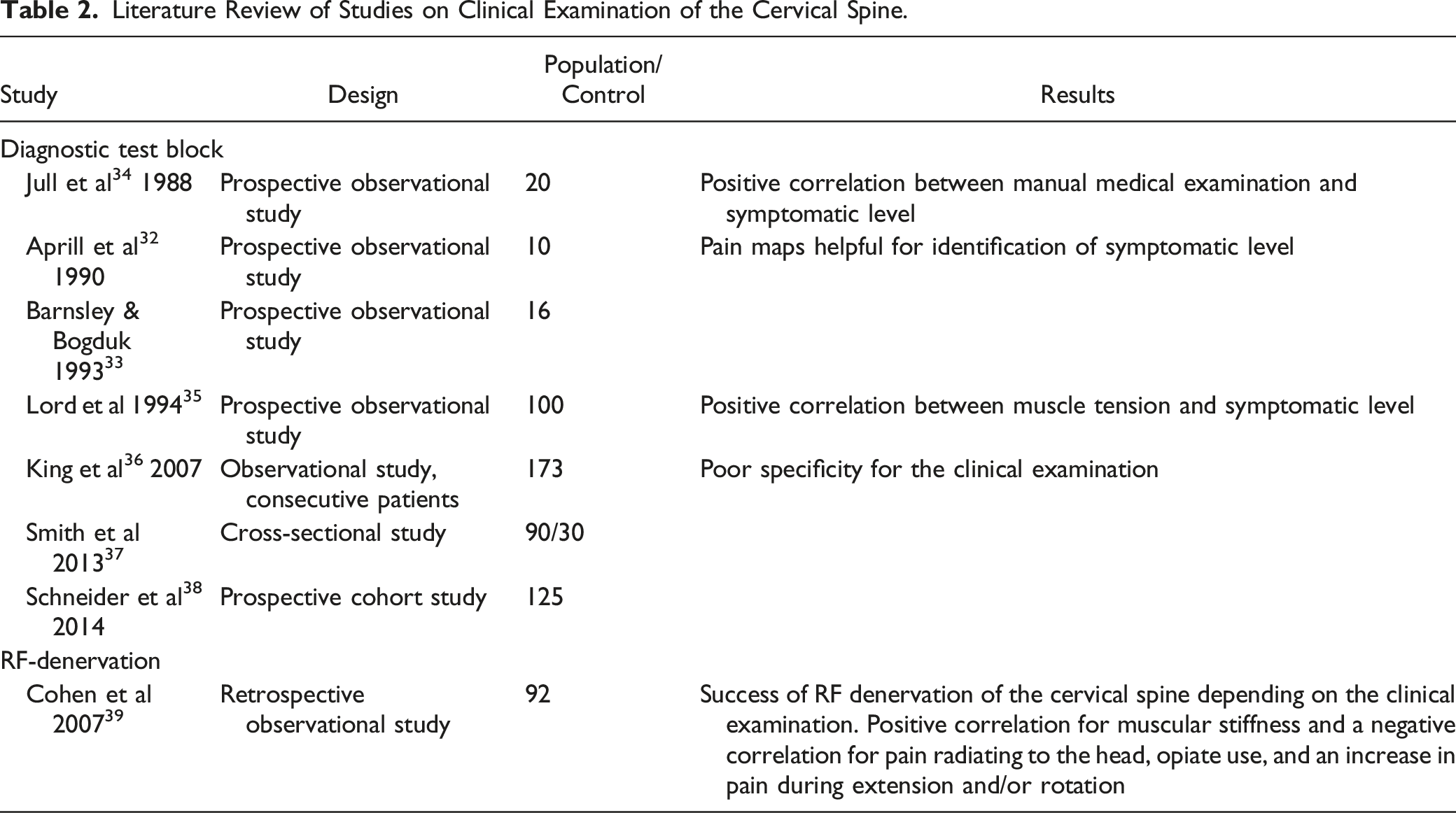
Two studies29,30 created pain maps for the individual levels of the cervical spine in volunteers after facet joint provocation. These results were confirmed by medial branch blocks in patients. 31 In 2 studies, the pain maps helped to identify the symptomatic joints.32,33
Examination Cervical Spine
Literature Review of Studies on Clinical Examination of the Cervical Spine.
Examination Lumbar Spine
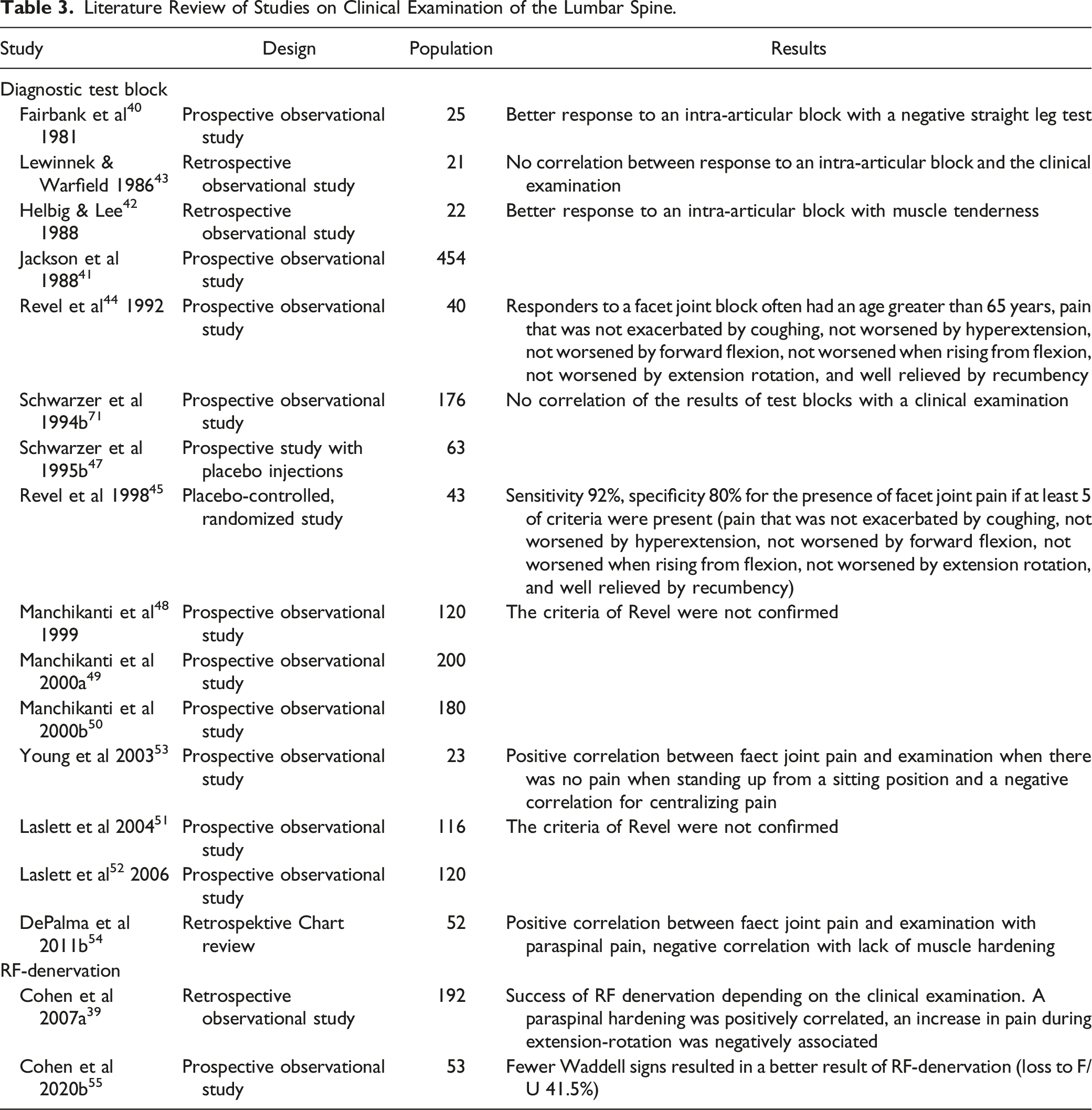
A better response to an intra-articular block at the lumbar spine was found with less leg pain,40,41 a negative straight leg test, 40 increased pain with flexion, 40 and with muscle tenderness.41,42 In contrast, Lewinnek and Warfield 43 found no correlation between response to an intra-articular block and the clinical examination.
Revel et al 44 found in responders to a facet joint block often an age greater than 65 years, pain that was not exacerbated by coughing, not worsened by hyperextension, not worsened by forward flexion, not worsened when rising from flexion, not worsened by extension rotation, and well relieved by recumbency. In a placebo-controlled, randomized follow-up study, 45 the sensitivity was 92% and the specificity 80% for the presence of facet joint pain if at least 5 of these criteria were present. Other studies could not find any correlation of the results of test blocks with a clinical examination46,47 and could not confirm the criteria of Revel either.48-52 Young et al 53 again found a positive correlation when there was no pain when standing up from a sitting position and a negative correlation for centralizing pain. In the study of DePalma et al 54 paraspinal pain was positively correlated, lack of muscle hardening was negatively correlated.
Literature Review of Studies on Clinical Examination of the Lumbar Spine.
Examination Sacroiliac Joint
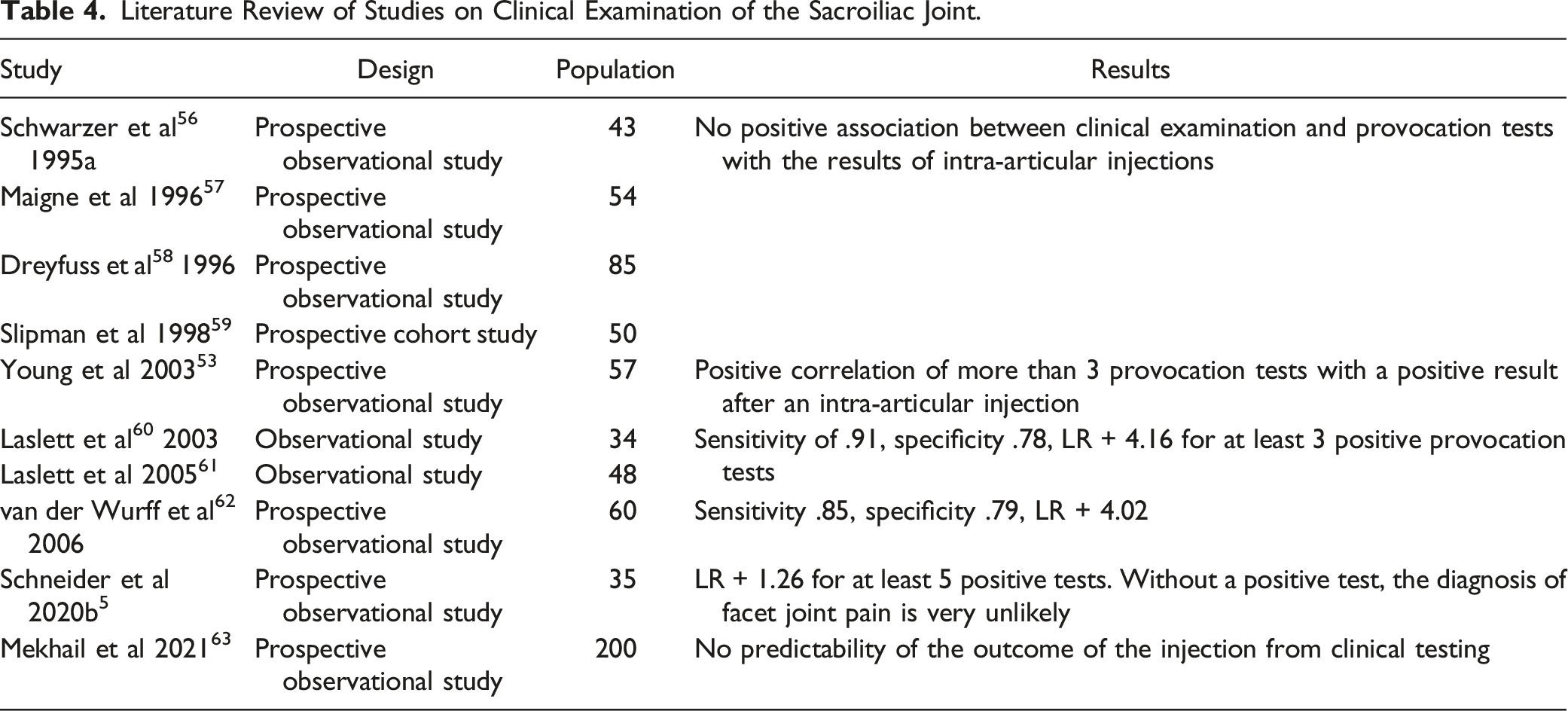
The first studies that compared the results of clinical examination tests and provocation tests of the SI joint with the results of intra-articular injections for the SI joint did not find any positive association.56-59 Later studies showed a positive correlation of more than 3 provocation tests with a positive result after an intra-articular injection. 53 Laslett et al 60 calculated a sensitivity of .91, a specificity of .78 and a positive likelihood ratio of 4.16 for at least 3 positive provocation tests and in a follow-up study 61 a sensitivity of .94, a specificity of 0.78 and a positive likelihood ratio of 4.29. In addition, pain of the SI joint can be ruled out if no test is positive. Similar results can also be found in the study of van der Wurff et al 62 (sensitivity .85, specificity .79, LR + 4.02).
Literature Review of Studies on Clinical Examination of the Sacroiliac Joint.
Existing Guidelines
Two guidelines4,22,23 recommend selecting the level at the cervical and lumbar spine based on the muscle tension at examination and on pain maps. One guideline
27
recommends 6 provocation tests for the SI joint. If none of these tests are positive, the SI joint can be ruled out as the cause of the pain. Recommendations and statements: 1.1 There are no symptoms or clinical investigations pathognomonic for the presence of cervical facet joint pain. (Quality of evidence: low) 1.2 Pain maps and the results of the segmental clinical examination should be used to identify the levels at the cervical spine for testing. (Recommendation: B, quality of evidence low) 1.3 There are no symptoms or clinical investigations pathognomonic for the presence of lumbar facet joint pain. There is a weak correlation to a positive result of a test block for paravertebral pain and tenderness. (Quality of evidence: low) 1.4 The results of the segmental clinical examination should be used to identify the levels at the lumbar spine for testing. (Recommendation: B, quality of evidence low) 1.5 Evidence is conflicting as to whether the combination of multiple clinical provocation tests (≥3 tests) can predict outcome of intra-articular SI joint injection. (Quality of evidence: very low) 1.6 In the absence of positive provocation tests, no test block should be carried out on the SI joint. (Recommendation: B, quality of evidence: low)
Question 2: Is there a Correlation Between Imaging Findings and RF Denervation Outcome?
X-Ray and CT
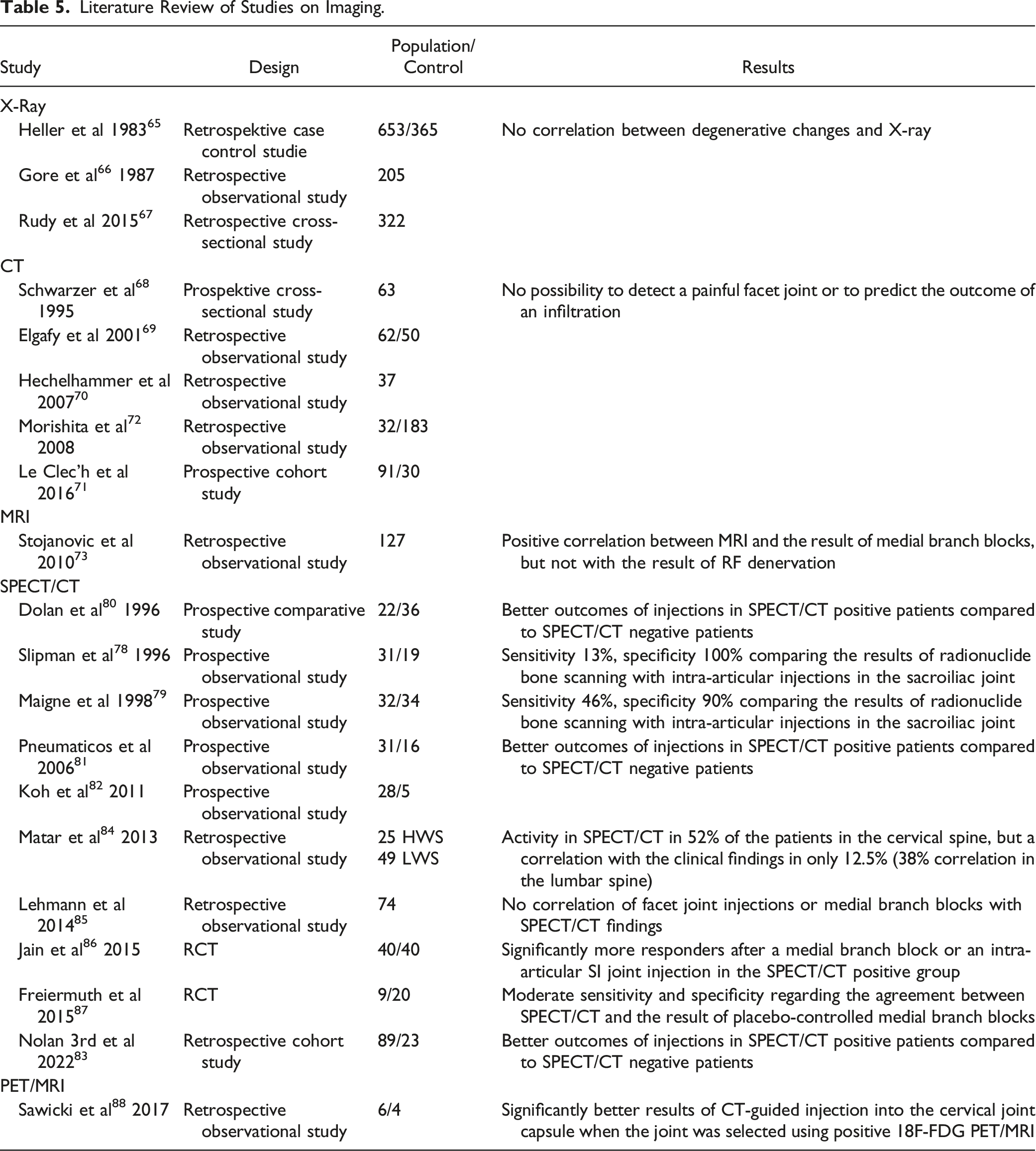
Since the 1980s, in many studies no correlation was seen between degenerative changes in the X-ray image and pain in the cervical or lumbar spine.65-67 Computed tomography (CT) is well suited for displaying the facet joints. Nevertheless, it is not possible to detect a painful facet joint or to predict the outcome of an infiltration68-72 with CT.
MRI
Stojanovic et al 73 found a positive correlation between magnetic resonance imaging (MRI) and the result of medial branch blocks, but not with the result of RF denervation. Also, Cohen et al39,74 found no correlation of MRI findings with the results of RF denervation of the cervical or lumbar spine. There is no study for the SIJ that compares MRI findings with results of injections. 75 It is assumed that MRI has a very low specificity regarding SI joint pain, since changes (eg, bone edema) are also often found in healthy subjects. 76 However, MRI is of great importance for diagnosing ankylosing spondylitis. 77
SPECT/CT
Two studies have compared the results of radionuclide bone scanning with intra-articular injections in the sacroiliac joint.78,79 Both studies found very low sensitivity (13% and 46%) with high specificity (100% and 90%). Several studies found better outcomes of injections in SPECT/CT positive patients compared to SPECT/CT negative patients.80-83 In contrast, Matar et al 84 showed activity in SPECT/CT in 52% of the patients in the cervical spine, but a correlation with the clinical findings in only 12.5% (38% correlation in the lumbar spine). Lehmann et al 85 found no correlation of facet joint injections or medial branch blocks with SPECT/CT findings.
Two randomized controlled trials show conflicting results. Jain et al 86 found significantly more responders after a medial branch block or an intra-articular SI joint injection in the SPECT/CT positive group. In contrast, Freiermuth et al 87 found only moderate sensitivity and specificity regarding the agreement between SPECT/CT and the result of placebo-controlled medial branch blocks, so that a SPECT/CT examination is not recommended for primary diagnostics.
PET/MRI
Literature Review of Studies on Imaging.
Existing Guidelines
One guideline
4
sees moderate evidence to use SPECT/CT to identify painful lumbar facet joints prior to medial branch block. However, another guideline
25
does not see sufficient evidence for or against the use of SPECT/CT to diagnose lumbar facet joint pain. There is weak evidence for a CT or an MRI to identify a painful facet joint in the lumbar spine.
4
For the cervical spine, the current evidence would not be sufficient to weigh the harms and benefits of imaging regarding the success of a cervical facet block; existing imaging should be considered for planning.22,23 Imaging is important in relation to the detection of other essential diseases,
24
but it is not required as a prerequisite for RF denervation.
21
Recommendations and statements 2.1 There is insufficient evidence to diagnose symptomatic facet joints or a symptomatic SI joint using imaging methods (X-ray, CT, MRI, SPECT, PET) alone. (Quality of evidence: low) 2.2 Imaging diagnostic procedures have no predictive value regarding the results of diagnostic blocks (intra-articular, medial branch block) or the result of RF denervation. (Quality of evidence: low) 2.3 Image diagnostic methods provide relevant information on differential diagnostic diseases (eg herniated disc, ankylosing spondylitis, infections, tumors). (Quality of evidence: low) 2.4 Existing imaging should be considered along with history and clinical examination findings when deciding which levels to treat. (Recommendation: B, quality of evidence: low)
Question 3: Is Conservative Therapy Necessary before a Diagnostic Block, for How Long?
There are currently no studies comparing RF denervation after conservative therapies of different duration. Likewise, there is no evidence for RF denervation in acute neck pain or acute low back pain. In all randomized studies that compared RF denervation with sham, chronic pain, and usually also explicitly previous conservative therapy for 2 months, 89 3 months,15,90-95 6 months,96-100 1 year 101 or even 2 years 89 are an inclusion criterion.
Existing Guidelines
The existing guidelines also recommend conservative therapy for at least 3 months.4,16,22–24 Recommendations 3.1 Chronic pain is a prerequisite facet joint testing and RF denervation. (Recommendation: A, quality of evidence: moderate) 3.2 Patients suspected of having a chronic pain disorder with somatic and psychological factors require interdisciplinary evaluation before an intervention. (Recommendation: EC)
Question 4: Are Medial Branch Blocks Suitable for Diagnosing Facet Joint Pain?
In this guideline, the terms medial branch and medial branch block are used for the medial rami C4 to C8 and the medial rami L1 to L4, but also for the third occipital nerve (TON) and the dorsal ramus L5, without these differences being explicitly pointed out in each case. The dorsal innervation of the SI joint is called lateral branch.
The validity of clinical tests is often validated by a reference examination (eg, laboratory values, histology, or imaging). Since pain is a subjective perception, there is no such reference value for medial branch blocks. Engel et al 102 tried to answer the question of diagnostic validity of medial branch blocks philosophically and were able to conclude that the 8 criteria they selected provide an axiomatic basis for diagnostic blocks in general and serve to show what empirical evidence needs to be gathered in order to validate a particular block.
It can be considered whether medial branch blocks are prognostic, predictive or diagnostic. Since studies on healthy volunteers have shown that facet joints can be pain generators 29 and that a medial branch block is specific33,103 and can protect against facet joint pain 104 the guideline uses the term diagnostic medial branch blocks.
A systematic review105,106 dealt with the diagnostic use of medial branch blocks. „Strong evidence“ was certified. Statement 4.1 Medial Branch Blocks are useful as a test block prior to RF denervation. (Quality of evidence: moderate)
Question 5: Are Medial Blocks Better than Intra-Articular/Pericapsular Blocks for Diagnosing Facet Joint Pain?
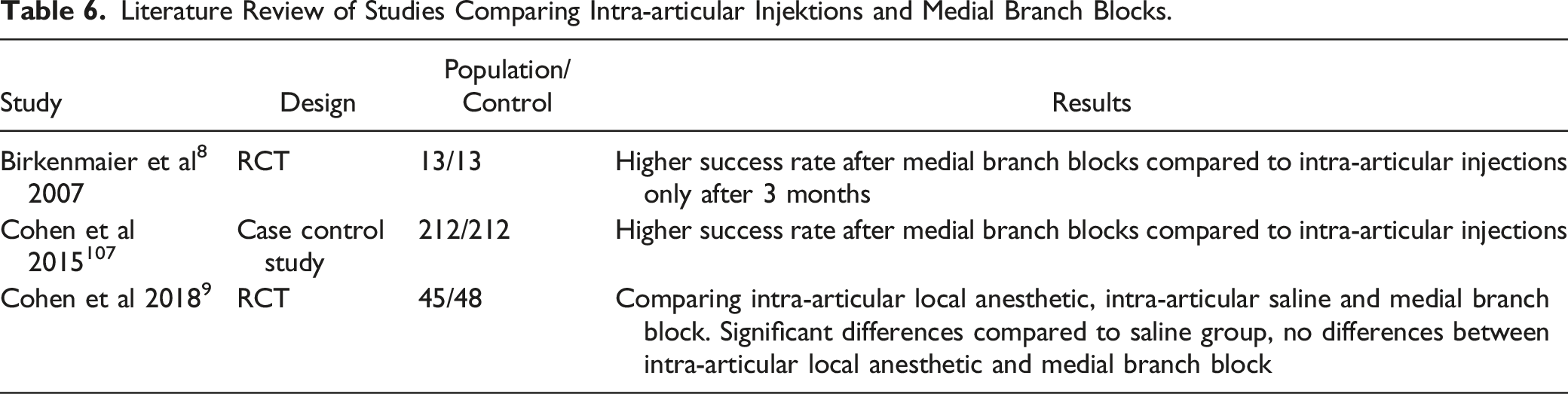
Literature Review of Studies Comparing Intra-articular Injektions and Medial Branch Blocks.
Existing Guidelines
All guidelines considered4,16,21 and the Greater Manchester EUR Policy Statement on Facet Injections
109
recommend performing medial branch blocks. Recommendation 5.1 Medial branch blocks should be performed as a test block prior to RF denervation. (Recommendation: B, quality of evidence: low)
Question 6: Which Diagnostic Blocks should be Performed on the SI Joint Prior to Denervation?
In the case of intra-articular test blocks, the target structure of an RF denervation (the lateral branches) is not tested. The dorsal pain generators (ligaments) are not included in the test. Another weakness of intra-articular injections as a diagnostic test is the lack of specificity. Fortin et al 110 were able to demonstrate that during arthrography of the SI joint in 61% of the joint injections, contrast medium was detectable outside the joint (dorsal foramina, superior recess closed to the L5 spinal nerve, ventral towards the lumbosacral plexus). In a cadaver study by Stelzer et al 111 a localization exclusively within the joint was found in only 50% of the joints after the injection of red latex under fluoroscopic guidance. In the other patients, injectate was found in the dorsal ligaments or intravenously. In a systematic review with evaluation according to the GRADE methods, 112 a false-positive rate of diagnostic intra-articular blocks of 19-22% was found. In 4-20% of the patients it was anatomically not possible to perform an intra-articular injection.
When using lateral branch blocks as a test block, the lateral branch is the target of the test injection and the RF denervation. However, the parts of the joint with a ventral innervation are not included in the test. Only 2 primary studies have examined lateral branch blocks. 113 A double-blind, randomized study on volunteers 114 was able to show that only 40% of the subjects were protected from provocative pain by intra-articular volume administration by a “single-site, single-depth” injection to the lateral branches. Target nerves were reached in only 36% of the injections. Thus, single-site, single-depth injections are not suitable for diagnostic or prognostic purposes. A “multi-site, multi-depth” technique was also developed in a double-blind, randomized, placebo-controlled follow-up study. 115 Either a local anesthetic or saline was injected to the medial branch L5 and the lateral branches at various sites around the foramen, followed by stimulation of the dorsal ligaments and the joint capsule. 70% of the patients with the local anesthetic but only 10% of the patients in the control group felt no pain. An anatomical study showed that 91% of the lateral branches were reached with this technique. Stout et al 116 studied the anatomy of the lateral branches in cadavers in relation to an ideal electrode position and determined positions for an RF electrode in which only 3% of the lateral branches are at the foramen S1, 1% at the foramen S2 and zero% at the foramen S3 are not reached. A denervation of the lateral branch L5 is also necessary. Vorobeychik et al 117 found that all patients after positive lateral branch blocks and successful RF denervation of the SI joint showed hypoesthesia in the area supplied by the cluneal nerves. It was concluded that the absence of hypoesthesia indicates an inadequate technique. It is thus possible to clinically check the quality of lateral branch blocks and RF denervation on the SI joint.
RCTs
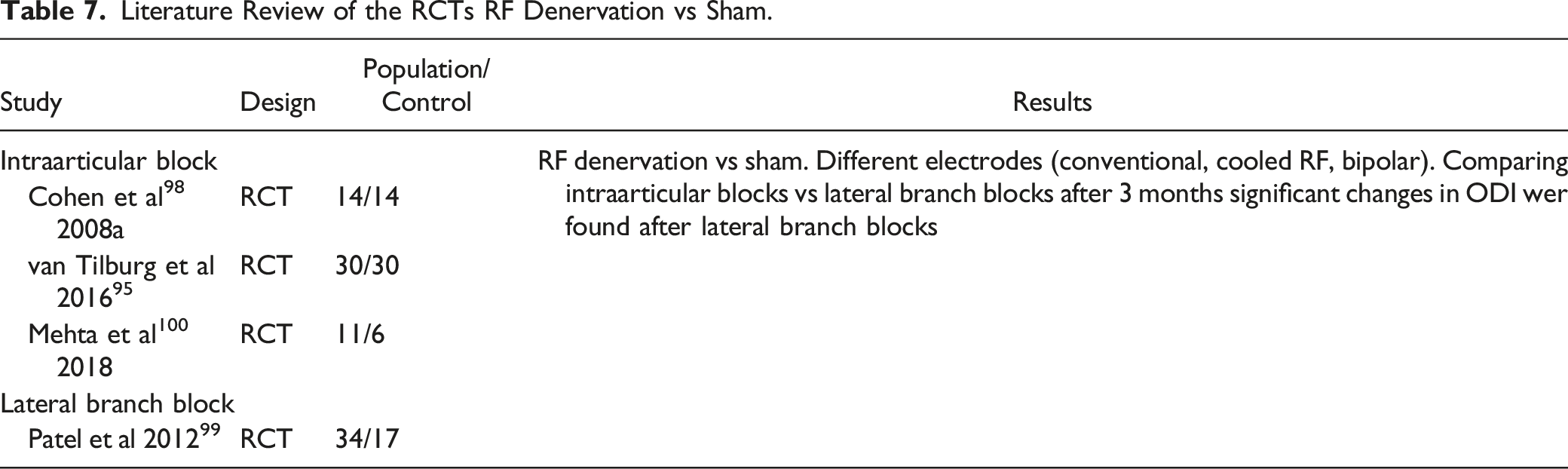
Literature Review of the RCTs RF Denervation vs Sham.
Existing Guidelines
The guidelines of the American Society of Pain and Neuroscience (ASPN) 27 recommend performing diagnostic lateral branch blocks using the “multi-side, multi-depth” technique. The North American Spine Society (NASS) 25 recommends RF denervation of the sacroiliac joint after 2 intra-articular test blocks. Studies regarding lateral branch blocks are necessary.
The review by Schneider et al 75 suggests initially performing a therapeutic intra-articular SI joint injection and, if unsuccessful, a lateral branch block for RF denervation. Also, in the RCT by Cohen et al 9 intra-articular, therapeutic injections were possible before the diagnostic test infiltration.
According to current knowledge, it seems useful to differentiate joint pain from pain in the dorsal (ligamentous) structures. Recommendations 6.1 Intra-articular injections can be used as the primary (therapeutic) intervention for SI joint pain. (Recommendation 0, Quality of evidence: very low) 6.2 An intra-articular injection with local anesthetic can be used as test prior to RF denervation of the sacroiliac joint. (Recommendation 0, Quality of evidence: very low) 6.3 Multi-site, multi-depth lateral branch blocks should be performed as test prior to RF denervation at the SI joint. (Recommendation B, Quality of evidence: very low)
Question 7: Which Drugs are Useful for a Diagnostic Test Block?
To reduce the number of false positive results, medial branch blocks are often performed as controlled medial branch blocks (the same local anesthetic is used), or with 2 local anesthetics of different durations of action (comparative medial branch blocks). Under strict test conditions, the medial branch block can only be considered positive if the patient reports a duration of pain reduction that corresponds to the duration of action of the local anesthetic. However, the pharmacological duration of action of the local anesthetics could not be confirmed in a clinical study. 118
Looking at the existing RCTs comparing RF denervation vs sham, different volumes were used for the medial branch blocks: .3 mL, 97 .5 mL,15,119 .75 mL 101 or 1.0 mL. 89 Cohen et al 120 compared .5 mL vs .25 mL volume for medial branch blocks and found (non-significantly) less aberrant contrast agent distribution at lower volume. There were no differences in pain reduction between the 2 groups. On cadavers, Wahezi et al 121 compared the distribution of .25 mL and .5 mL injectate on the lumbar spine. In both groups, the medial branch was adequately irrigated, but with .5 mL of injectate there was distribution in the muscles and distal branches of the dorsal ramus. Therefore, a volume of .25 mL was recommended for a specific medial branch block. Similar results in the comparison of .25 mL and .5 mL could also be shown for the cervical spine. 122
In a cadaver study with subsequent injections to the medial branches of volunteers, 103 the distribution of contrast medium at different puncture sites was examined in the CT. It was concluded that the administration of contrast medium prior to the injection of local anesthetic is necessary for the test block to be specific for the medial branch. Kennedy et al 123 investigated the frequency of intravascular injections in medial branch blocks. Intravascular contrast medium was detected in 19% of medial branch blocks. Without contrast medium, it is not possible to detect intravascular drug distribution and to avoid drug distribution to structures other than the medial branch. The possible side effects (allergic reaction to contrast media) must be considered.
Existing Guidelines
The SIS Practice Guidelines
16
recommend the use of long-acting and short-acting local anesthetics with comparative medial branch blocks. No more than .5 mL should be used, .3 mL is sufficient. Contrast agent is recommended under live fluoroscopy. The consensus guidelines4,92,101 recommend using less than .5 mL total volume for a medial branch block at the lumbar spine and even less than .3 mL total volume for the cervical spine. Both guidelines recommend the use of contrast media under live fluoroscopy. The British Pain Society technical guideline
26
recommends the use of levobupivacaine. The guidelines of the American Society of Interventional Pain Physicians (ASIPP)
24
recommend using less than .5 mL for medial branch blocks. Recommendations 7.1 Both a short-acting and a long-acting local anesthetic can be used for a diagnostic test block. (Recommendation: 0, quality of evidence: very low) 7.2 The volume used for a medial branch block should be less than .5 mL. (Recommendation: B, quality of evidence: low) 7.3 Contrast media should be used for diagnostic medial branch blocks. (Recommendation: B, quality of evidence: low)
Question 8: Which Pain Threshold after a Therapeutic Block is Considered Positive?
It can be assumed that strict test criteria (100% pain reduction) lead to better results of a subsequent RF denervation. However, there will be patients with false-negative test blocks who, given these strict criteria, would be deprived of a potentially effective therapy.
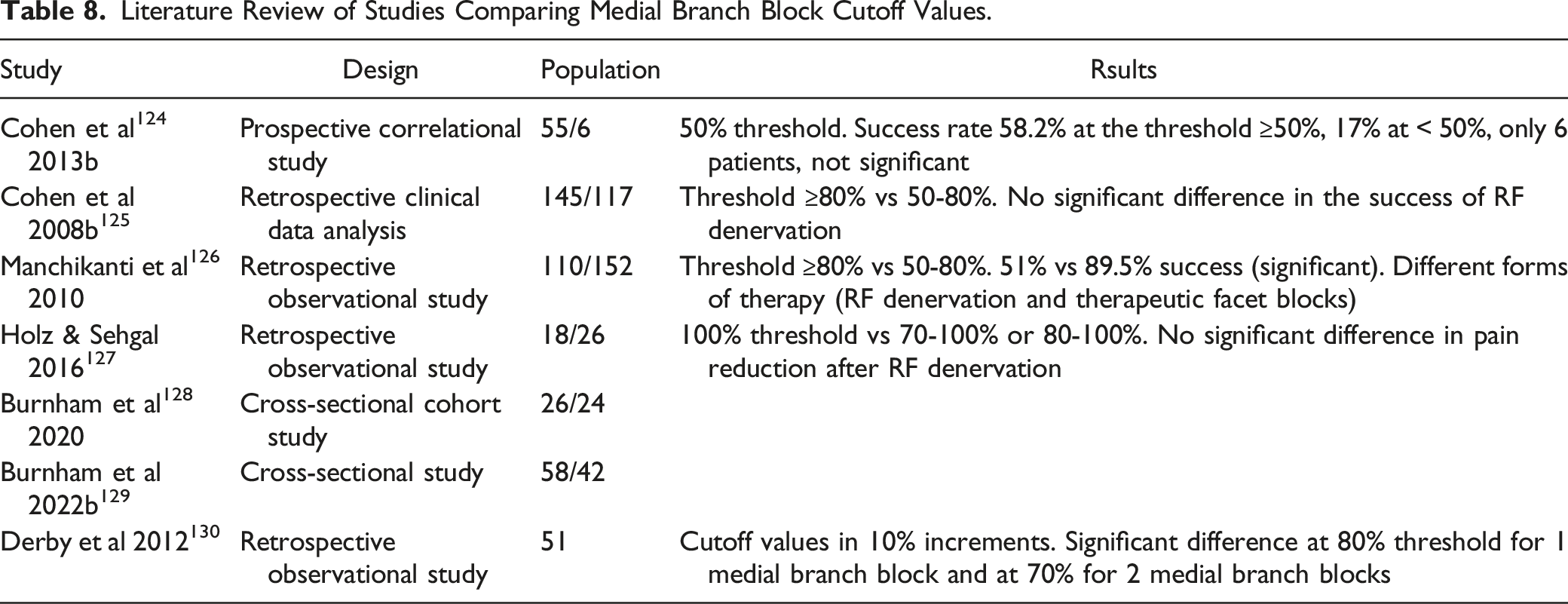
Cohen et al 124 chose 50% as the threshold in a prospective study, but patients who reported less than 50% pain reduction after medial branch block but were satisfied with the pain reduction were also treated with RF denervation. The success rate was 58.2% at the threshold ≥50% and 17% at < 50%, however, due to the small number of cases (6 patients), the difference is not significant.
Two studies compared a threshold of ≥80% with a threshold between 50 and 80%. Cohen et al 125 found no significant difference in the success of RF denervation. Manchikanti et al 126 reported 51% vs 89.5% reported success in both groups; this difference is significant, although different forms of therapy (RF denervation and therapeutic facet blocks) were used in both groups.
A threshold of 100% was compared with a threshold of 70-100% and 80-100% in 3 studies (cervical and lumbar spine).127-129 In all studies, the difference in pain reduction after RF denervation was not significant.
Literature Review of Studies Comparing Medial Branch Block Cutoff Values.
Existing Guidelines
The SIS Practice Guidelines
16
recommend ideally using 100% pain reduction of index pain as a positive result of a medial branch block, but at least 80%. The consensus guidelines4,22,23 recommend that ≥50% pain reduction be rated as positive. The Comprehensive Guidelines of the American Society of Interventional Pain Physicians (ASIPP)
24
recommend a threshold of ≥80% for the lumbar spine and ≥80% or 100% for the cervical spine. The North American Spine Society (NASS)
25
sees no evidence for or against the 50% threshold in its guideline. Recommendation 8.1 A threshold of 50% pain reduction after a medial branch block should be used for the test block to be considered positive. (Recommendation: B, quality of evidence: low)
Question 9: How Many Diagnostic Blocks are Necessary Before Denervation?
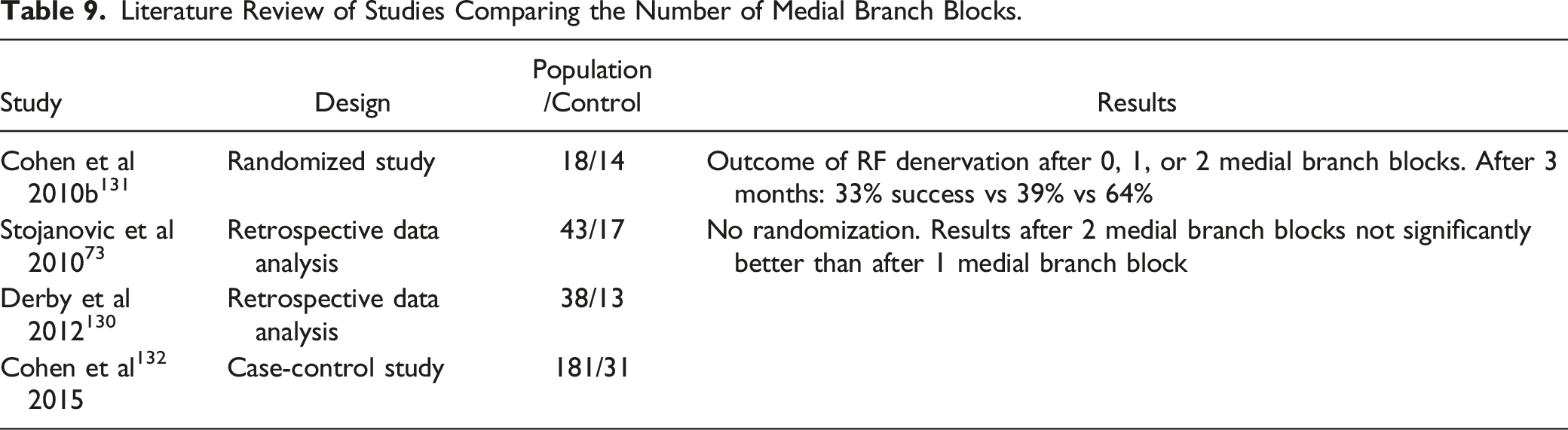
Comparing the RCTs RF comparing denervation to sham, which used either 1 or more than 1 medial branch block as an inclusion criterion, only individual studies per endpoint with small patient numbers can be found. More significantly better results are found when using more than 1 medial branch block.
Literature Review of Studies Comparing the Number of Medial Branch Blocks.
Existing Guidelines
The SIS Practice Guidelines
16
recommend conducting controlled medial branch blocks, ideally as comparative medial branch blocks. The Comprehensive Guidelines of the American Society of Interventional Pain Physicians (ASIPP)
24
also recommend performing 2 diagnostic medial branch blocks. However, the NICE Guidelines
21
recommend a single medial branch block prior to RF denervation. Likewise, with the justification “maximize access to care”, only 1 medial branch block is recommended in the consensus guidelines.4,22,23 Recommendation 9.1 Prior to RF denervation, two diagnostic medial branch blocks with a positive response should usually be performed. (Recommendation: B, quality of evidence: low)
Question 10: What Image Guidance is Recommended for RF Denervation?
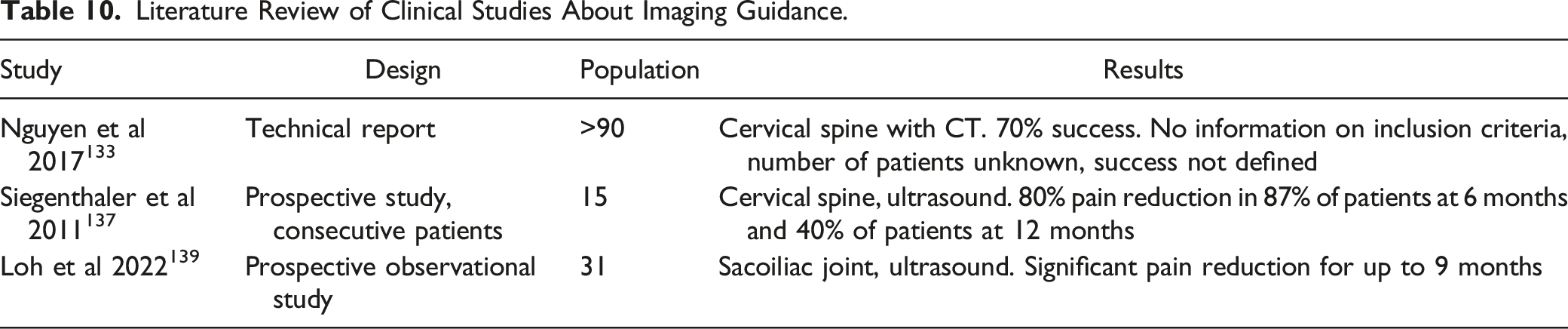
One study 133 dealt with RF denervations in the cervical spine using computed tomography. There is no information on the inclusion criteria and the number of patients, but 70% success is reported, although success was not defined in more detail.
A cadaver study 134 examined the needle position in CT vs fluoroscopy on 10 specimens. Under CT guidance, the tip of the electrode often failed to reach the nerve and the needle had less contact area to the medial branch compared to fluoroscopy. The authors concluded that computed tomography should not be used for RF denervation. In a follow-up study, 135 the technical feasibility of a parallel needle position with a corresponding puncture angle in computed tomography was demonstrated on 10 cadavers. 54.6% of the needles met the requirement of maximum parallelism and proximity to the medial branch.
Literature Review of Clinical Studies About Imaging Guidance.
Existing Guidelines
The consensus guidelines4,22,23 recommend the use of fluoroscopy for RF denervation of the lumbar or cervical spine. All RCTs were performed with fluoroscopy. Recommendation 10.1 RF denervation should be performed with fluoroscopy. (Recommendation: B, quality of evidence: very low) 10.2 The diagnostic test block (medial branch block and lateral branch block) should be performed with the same imaging as the later RF denervation. (Recommendation: B, quality of evidence: very low)
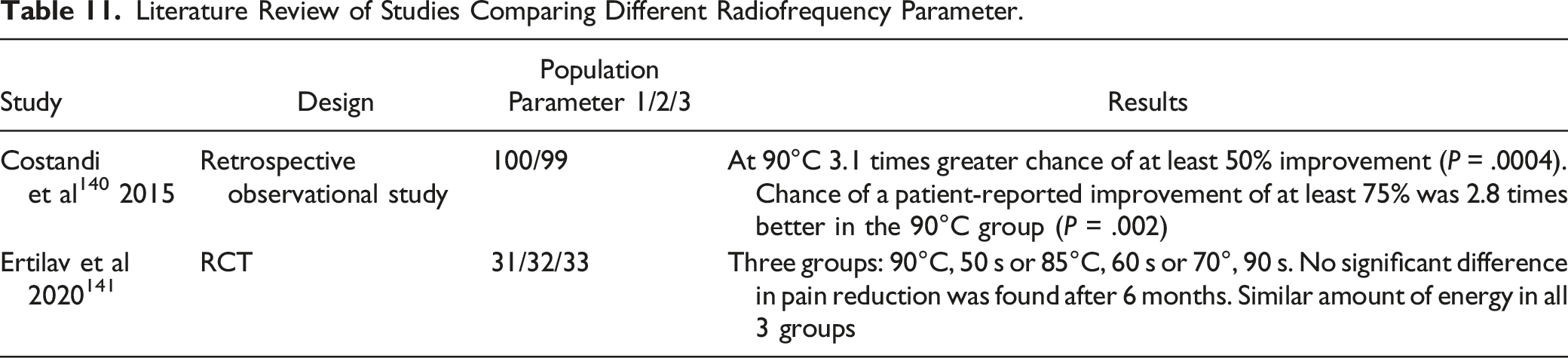
Question 11: Does the Size of the Lesion Determine the Outcome of the Denervation? How can the Lesion be Enlarged?
Literature Review of Studies Comparing Different Radiofrequency Parameter.
Existing Guidelines
The consensus guidelines for the cervical and lumbar spine4,22,23 suggest that a larger lesion increases the probability of medial branch neurotomy and that a larger lesion increases the duration of pain reduction. The SIS Practice Guidelines
16
recommend a temperature of 80 °C-85°C and a duration of denervation of 60-90 s. Multiple lesions (2-3) are also recommended depending on the diameter of the cannula and the length of the active tip. The British Pain Society technical guideline
26
recommends an 18 G cannula with a 10 mm curved active tip and a temperature of 80°C for 120 s with 2 lesions per nerve. The guidelines of the American Society of Pain and Neuroscience (ASPN)
27
recommend 60 °C-80°C for 60-90 s at the cervical spine and 60-90 s at the lumbar spine. Recommendations and statements 11.1 It can be assumed that a larger lesion leads to a longer-lasting reduction in pain. (Quality of evidence: low) 11.2 A temperature of 75-90°C should be used for denervation with conventional electrodes. (Recommendation: B, quality of evidence: very low) 11.3 A lesion duration of between 60 s and 120 s is recommended when using conventional electrodes. (Recommendation: EC) 11.4 A large diameter of the cannula of at least 18G is recommended when using conventional electrodes. (Recommendation: EC) 11.5 An active tip length of 10 mm is recommended for conventional electrodes in the lumbar spine and SIJ, on the cervical spine a length of 5 mm is also possible. (Recommendation: EC) 11.6 When using conventional electrodes, multiple lesions per medial branch or lateral branch are recommended. (Recommendation: EC)
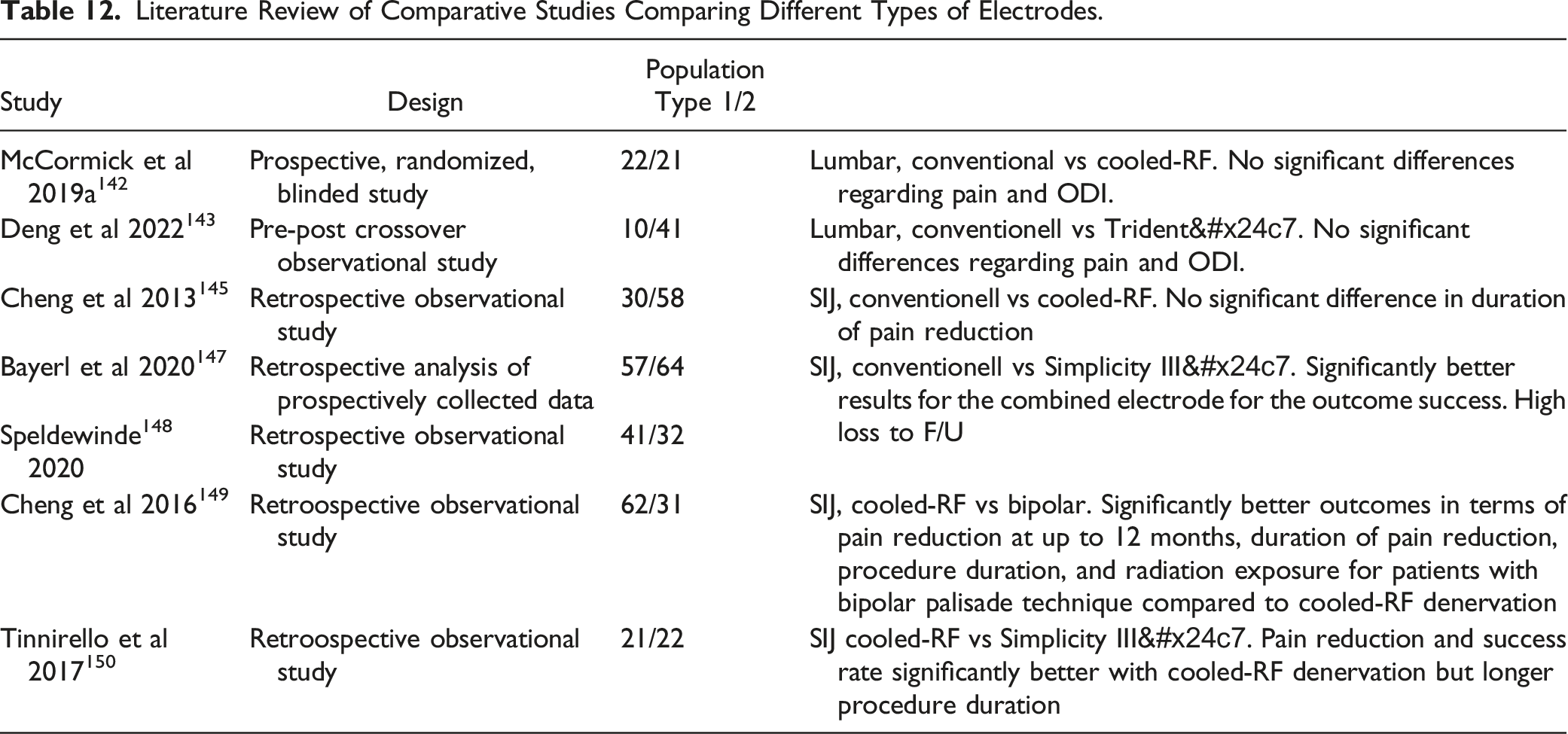
Question 12: What Type of Electrode is Recommended?
A conventional monopolar electrode was used in all RCTs at the lumbar or cervical spine comparing RF denervation vs sham. Two observational studies142,143 examined the results of different electrode types for the lumbar spine. A conventional electrode was compared to a cooled-RF or to an electrode with 3 active parts of the tip. There were no significant differences regarding pain and ODI. In a systematic review with meta-analysis, 144 no significant differences were found between conventional RF denervation and cooled RF denervation regarding pain reduction.
Literature Review of Comparative Studies Comparing Different Types of Electrodes.
Existing Guidelines
Without considering different types of electrodes, the North American Spine Society (NASS)
25
recommends in its guideline cooled RF in patients with proven SI joint pain. The guidelines of the American Society of Pain and Neuroscience (ASPN)
27
recommend a bipolar technique or cooled-RF electrodes for SI joint denervation. Statement 12.1 Based on the available evidence in the literature, a recommendation for or against the use of a certain type of electrode cannot be given for denervations of the cervical, lumbar, or sacroiliac joints. (Quality of evidence: very low)
Question 13: Is the Position of the Electrode to the Nerve (Parallel, Perpendicular) Important?
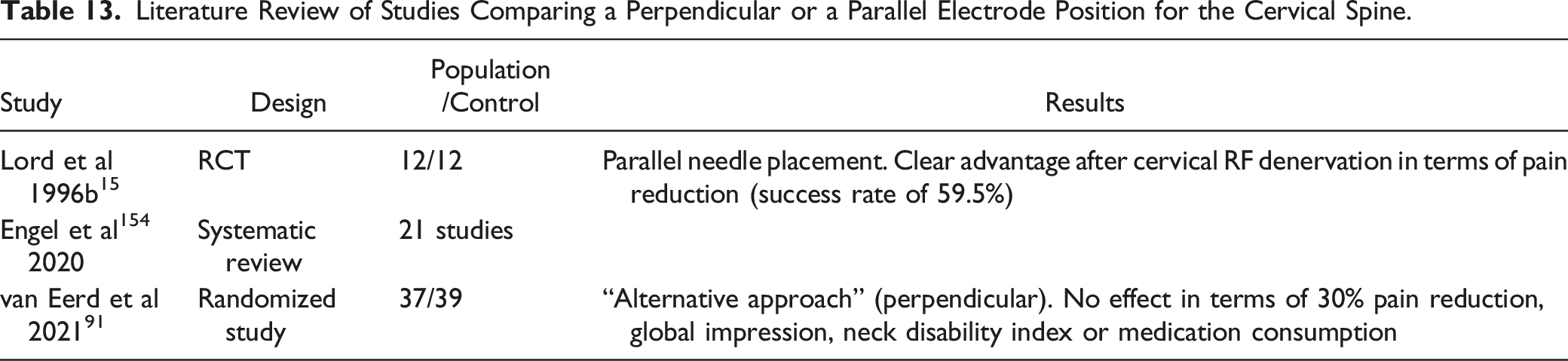
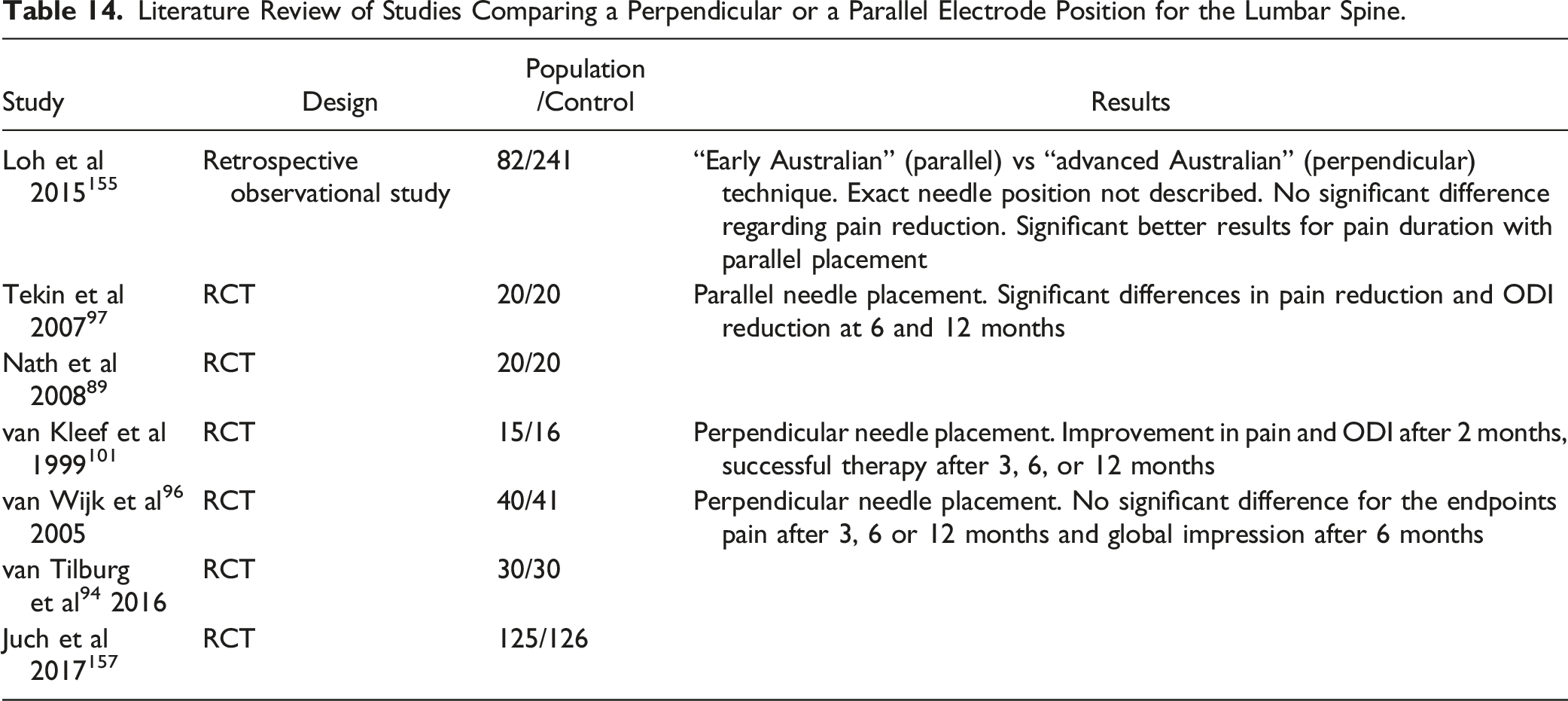
Currently, there are 2 dominant techniques in the literature regarding needle guidance in RF denervation, which differ primarily in the angle at which the electrode is inserted. In 1 technique, (curved) electrodes are placed tangentially to the medial branch so that contact to the nerve occurs along the long side of the non-insulated electrode tip. Compared to the medial branch block, a much flatter puncture angle is required for RF denervation. 151 This is called a parallel needle position. 152 The other technique uses a needle direction like that of the medial branch block, so that the needle tip contacts the nerve perpendicular.
The results of studies using the parallel technique should therefore be distinguished from the results of studies using the perpendicular technique. When comparing both techniques, only the conventional electrode is taken into account, since the distribution of the heat field in relation to the extent distal to the tip is different with other electrode types (eg, cooled-RF). 153
Cervical Spine
Literature Review of Studies Comparing a Perpendicular or a Parallel Electrode Position for the Cervical Spine.
Lumbar Spine
Literature Review of Studies Comparing a Perpendicular or a Parallel Electrode Position for the Lumbar Spine.
Existing Guidelines
The consensus guidelines for the cervical spine22,23 recommend a parallel needle position via a posterior or oblique posterior approach for conventional electrodes. The Consensus Guidelines for LWS
4
also recommend a parallel electrode position. The guidelines of the American Society of Pain and Neuroscience (ASPN)
27
recommend choosing a sagittal and oblique approach to the cervical spine to denervate a long part of the nerve. A parallel needle position is required for the lumbar spine. Recommendations 13.1 When using a conventional electrode in the cervical spine, a parallel needle position should be selected via a posterior or oblique posterior approach, if necessary, with a curved needle. (Recommendation: A, quality of evidence: moderate) 13.2 On the lumbar spine, a parallel needle position should be selected when using a conventional electrode. (Recommendation: B, quality of evidence: low)
Question 14: Is Sensory or Motor Test Stimulation Necessary?
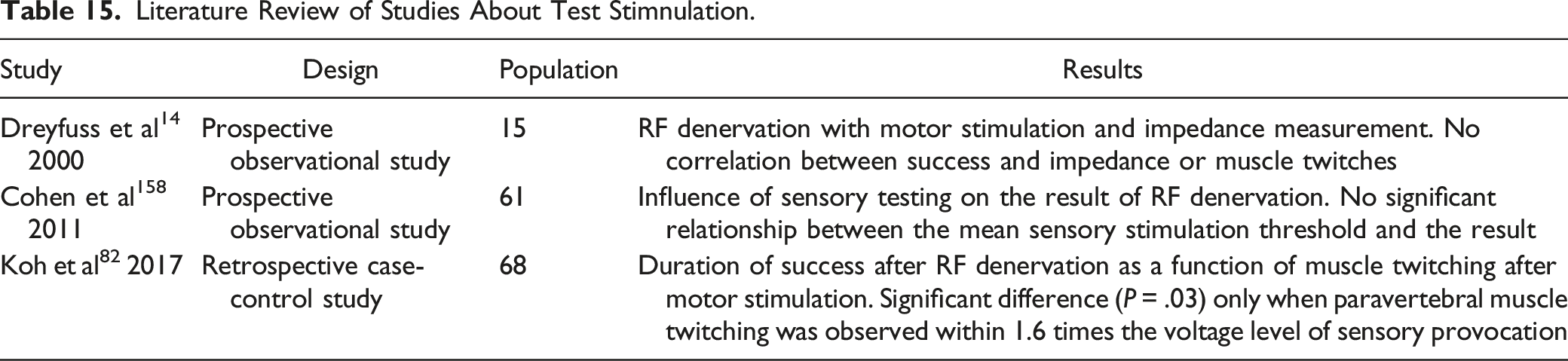
Literature Review of Studies About Test Stimnulation.
Existing Guidelines
The SIS Practice Guidelines16,159 do not recommend sensory or motor testing, but instead localize the electrode according to anatomical landmarks in multiplanar fluoroscopy. A warning is given against motor stimulation without adequate imaging. The Consensus Guidelines4,22,23 recommend sensory and motor testing for the cervical and lumbar spine. In the British Pain Society technical guideline,
26
sensory testing is recommended, but not motor testing. The guidelines of the American Society of Pain and Neuroscience (ASPN)
27
recommend both sensory and motor testing of the lumbar spine. Recommendation 14.1 Sensory and motor stimulation can be performed to provide information on the safety and proximity of the electrode to the nerve in addition to orientation to the anatomical landmarks in the fluoroscopic image. (Recommendation: 0, quality of evidence: moderate)
Question 15: Can an RF Denervation be Repeated, After What Time?
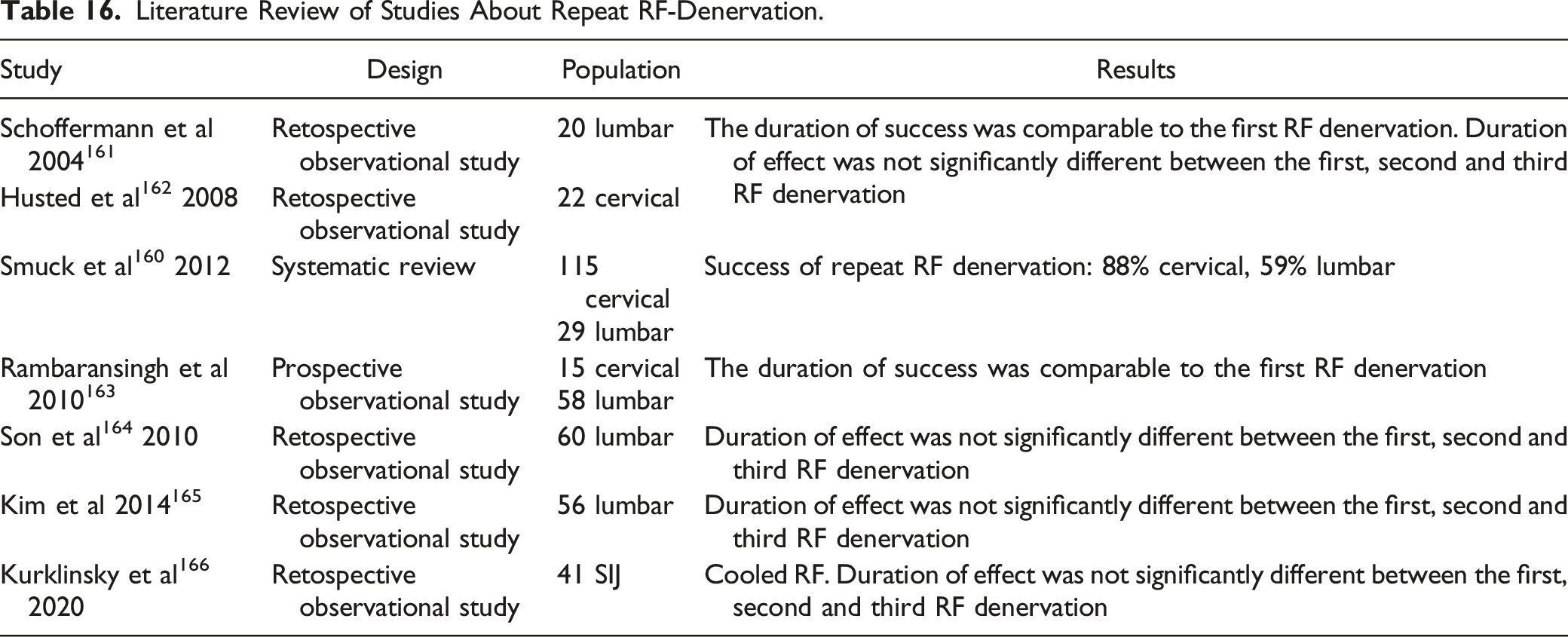
In a systematic review, 160 repeated RF denervation in the cervical spine was successful in 88% of patients and in 59% of patients in the lumbar spine. Success was defined as minimum 50% pain reduction for at least 3 months. The duration of success was comparable to the first RF denervation. Further studies confirmed these results.161-163 No significant differences in pain reduction were found with first, second, or third RF denervation. The duration of the effect was also not significantly different between the first, second and third RF denervation.161,162,164,165 Similar results were also described for repeating a cooled-RF on the SI joint. 166
A review 160 examined the results of a second RF denervation after an unsuccessful first denervation and found a success rate of only 38%. Lord et al 167 found a success rate of only 33% for repeated application after a short-term success <90 days after the first application. If the first RF denervation was unsuccessful, the repeat success rate was zero%.
Literature Review of Studies About Repeat RF-Denervation.
Existing Guidelines
The NICE Guidelines
21
advise caution in recommending repeat RF denervation until more long-term data are available. The consensus guidelines
4
recommend repeat RF denervation for the lumbar spine for patients who have experienced at least 3 (or preferably 6) months of success after the first RF denervation. The Consensus-Guidelines for the cervical spine22,23 also recommend repetition after a response for at least 3 months, but no more frequently than twice a year. The guidelines of the American Society of Pain and Neuroscience (ASPN)
27
recommend repeating the cervical spine after 6 months at the earliest. Recommendations 15.1 After successful RF denervation with at least 50% pain reduction for at least 3 months, another RF denervation should be offered, if the same pain recurs. (Recommendation: B, quality of evidence: low) 15.2 If a technically correct RF denervation was unsuccessful (less than 50% pain reduction or shorter than 3 months of effect), no repeat RF denervation of the same medial branches should be performed. (Recommendation: B, quality of evidence: low) 15.3 If the same pain recurs after the first successful RF denervation, no further test blocks should be carried out before another RF denervation. (Recommendation: B, quality of evidence: low)
Question 16: Do Anticoagulants and Antiplatelet Drugs have to be Stopped Before RF Denervation?
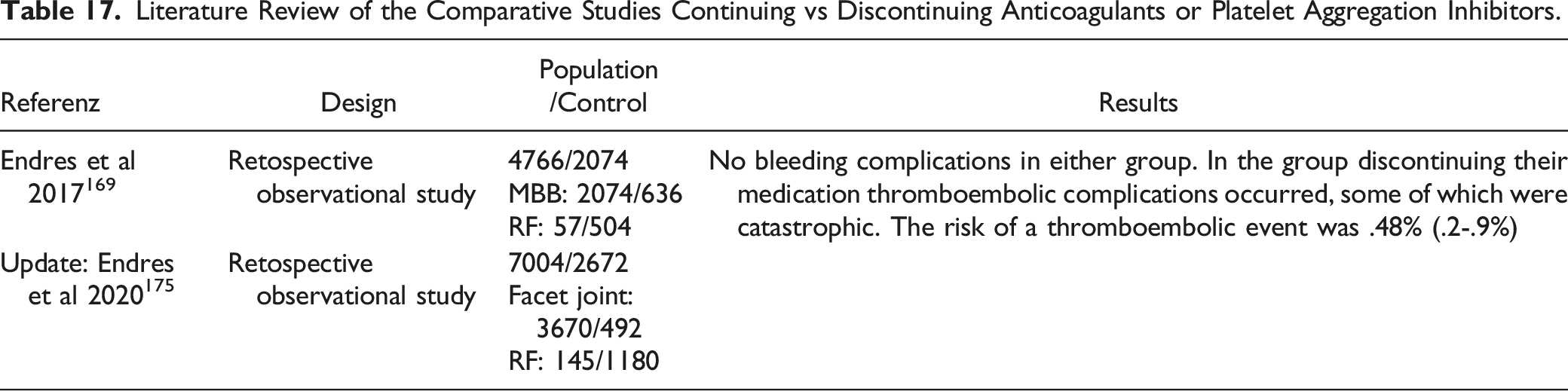
No relevant bleeding complications after RF denervation have been described in the literature.168–171 In contrast, thromboembolic complications after discontinuation of anticoagulants or platelet aggregation inhibitors are found in the literature. Although the risk is rather low, complications can be serious and even fatal. 169
Several observational studies have evaluated the risk of bleeding events in patients on anticoagulants/antiplatelets. Goodman et al 172 performed 197 interventions in 74 patients under medication without a relevant bleeding complication. Van Helmond et al 173 observed a hematoma at the puncture site of an RF denervation in one of 467 patients with medication. Ehsanian et al 174 saw no bleeding event in cervical and lumbar medial branch blocks and RF denervations with continued medication.
Endres et al169,175 conducted a comparative study in which 1 user performed interventions when continuing the medication and 1 user performed interventions when discontinuing anticoagulants or platelet aggregation inhibitors. There were no bleeding complications in either group. Only in the group of patients who had discontinued their medication thromboembolic complications occurred, some of which were catastrophic. The risk of a thromboembolic event is .48% (.2-.9%). A myocardial infarction after discontinuation of antiplatelets for lumbar RF denervation was reported by Galbraith et al. 176
Literature Review of the Comparative Studies Continuing vs Discontinuing Anticoagulants or Platelet Aggregation Inhibitors.
Existing Guidelines
The guidelines of the American Society of Regional Anesthesia and Pain Medicine, the European Society of Regional Anesthesia and Pain, the American Academy of Pain Medicine, the International Neuromodulation Society, the North American Neuromodulation Society, and the World Institute of Pain
177
have lumbar RF denervation classified as a low-risk procedure (when performed with image guidance), cervical spine denervation as a medium-risk for a bleeding complication. For medium-risk interventions, it is recommended to decide on preparations with acetylsalicylic acid based on risk assessment, discontinue Coumarin and new oral anticoagulants. Discontinuation of preparations containing acetylsalicylic acid is not recommended for low-risk interventions, but a case-by-case decision is made for oral anticoagulants. The SIS Practice Guidelines
16
generally recommend not stopping the medication. However, the risk of bleeding should be individually weighed against the risk of a thromboembolic complication, with the latter risk being classified as higher.
178
For the cervical spine, it is recommended to examine the imaging regarding anatomical variants in the course of the blood vessels before an intervention.159,171 Whether anticoagulants or platelet aggregation inhibitors should be discontinued should be determined in an individual case together with the patient, considering that complications were only seen in the group of patients after discontinuation of the medication. It should always be considered not to perform an intervention on the cervical spine if the risk seems too high. Recommendations 16.1 There is no evidence that continuing medication with anticoagulants or platelet aggregation inhibitors leads to a clinically relevant increased risk of bleeding. (Quality of evidence: low) 16.2 Anticoagulants or antiplatelet agents should not be discontinued prior to RF denervation of the lumbar spine or sacroiliac joint, the risk and benefit always being a case-by-case basis. (Recommendation: B, quality of evidence: low) 16.3 In the case of RF denervation of the cervical spine, an individual risk/benefit assessment should be made for each individual patient regarding continuation or discontinuation of anticoagulants or platelet aggregation inhibitors. (Recommendation: B, quality of evidence: low)
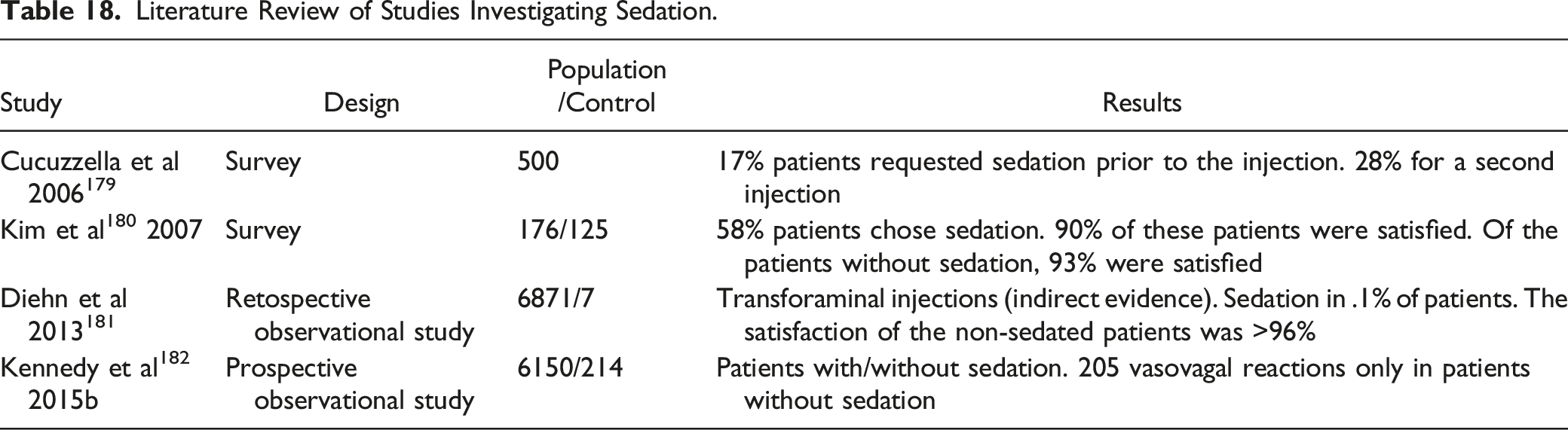
Question 17: Is Sedation Useful for RF Denervation?
Literature Review of Studies Investigating Sedation.
Existing Guidelines
The SIS Practice Guidelines
16
do not recommend sedation as routine and require that the patient be always responsive when RF denervation occurs. The NICE guidelines
21
state that RF denervation can be performed under light sedation. The American Society of Interventional Pain Physicians (ASIPP) Comprehensive Guidelines
24
state that moderate sedation can be used. The American Society of Anesthesiologists
183
issued a statement on anesthesiologic care during pain therapy interventions. In general, local anesthetic is sufficient. However, if sedation is given, the patient should be responsive to report changes in pain or sensory disturbances. Light sedation is recommended for most interventions; moderate sedation (“conscious sedation”) would be an option for RF denervation, which requires the patient to lie still for an extended period of time. Recommendation 17.1 Responsive sedation can be used for RF denervation. (Recommendation: 0, quality of evidence: low)
Question 18: Is RF Denervation Possible in Patients with Metal Implants?
Literature Review of Studies With an RF Denervation in Patients With Metal Implant.

In a FactFinder,
158
the SIS recommends avoiding direct contact of the electrode with the metal. Existing axial imaging should be evaluated. The consensus guidelines
4
recommend using multiplanar fluoroscopic images for the LWS and avoiding direct contact of the electrode with the metal. The consensus guidelines for the cervical spine22,23 also recommend multiplanar imaging under fluoroscopy and a more posterior approach to avoid direct contact with the metal. Recommendation 18.1 A multiplanar fluoroscopic view should be used to view the implant and electrode, avoiding direct contact of the electrode with the metal. (Recommendation: B, quality of evidence: low)
Question 19: Is RF Denervation Possible in Patients with Cardiac Pacemakers or SCS?
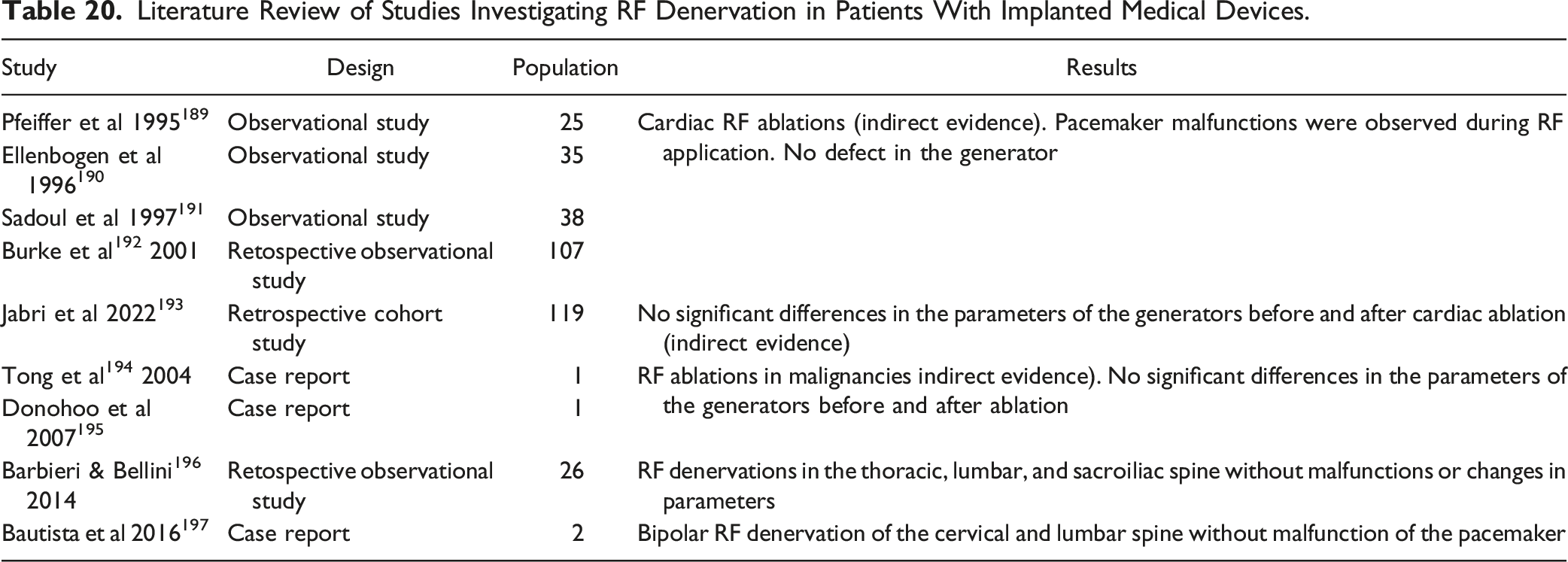
Electromagnetic fields can lead to malfunctions in implanted devices such as cardiac pacemakers, defibrillators or brain or spinal cord stimulators.187-189 There are several observational studies that have examined cardiac RF ablations (indirect evidence) in patients with pacemakers or defibrillators.189-192 In all studies, pacemaker malfunctions were observed during RF application. In some cases, the pacemaker had to be reprogrammed after the ablation. However, there was never a defect in the generator. A current retrospective cohort study 193 could not observe any significant differences in the parameters of the generators before and after cardiac ablation. Case reports on RF ablations in malignancies also show similar results.194,195
Literature Review of Studies Investigating RF Denervation in Patients With Implanted Medical Devices.
Existing Guiedlines
The American Society of Anesthesiologists guideline
198
recommends keeping the high-frequency electric field as far away from the pacemaker electrodes as possible. The consensus guidelines4,22,23 also recommend a distance of at least 15 cm between the neutral electrode and pacemaker electrodes. The SIS recommends close cooperation with an experienced cardiologist even before the RF denervation.
199
Recommendations 19.1 RF denervation in patients with an implanted pacemaker or defibrillator should be done in close collaboration with a cardiologist. (Recommendation: A, quality of evidence: very low) 19.2 The neutral electrode should be placed in such a way that the electrical field between the lesion electrode and the neutral electrode does not affect the pacemaker/defibrillator. (Recommendation: B, quality of evidence: very low) 19.3 An implanted neurostimulator should be turned off for the duration of RF denervation. (Recommendation: EC)
Question 20: What are Typical Complications of RF Denervation?
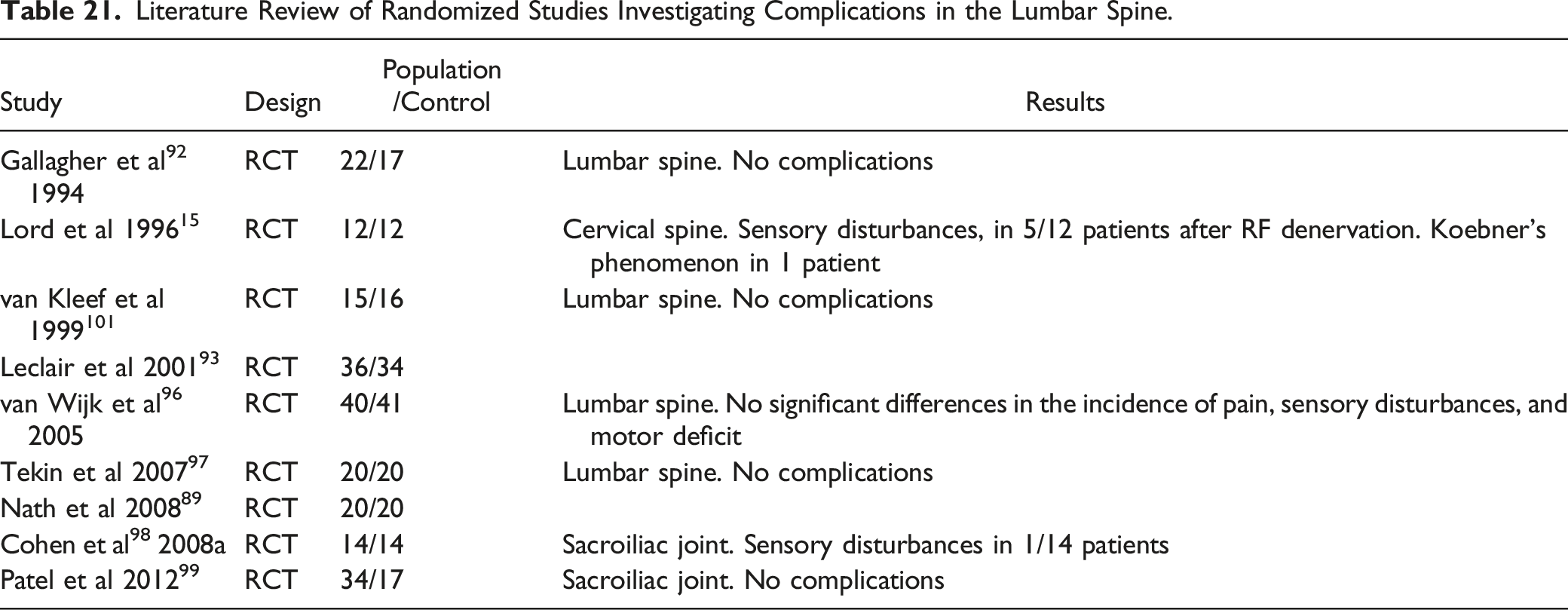
Literature Review of Randomized Studies Investigating Complications in the Lumbar Spine.
Literature Review of Observational Studies Investigating Complications in the Lumbar Spine.

The studies show that prolonged pain is the most common complication after RF denervation96,200 followed by sensory disturbances.15,96,98 Neuropathic pain has already been described by Bogduk 202 in a case report. In the case of denervation of the “Third Occipital Nerve” (TON), ataxia is mentioned as a typical temporary side effect,203,204 and temporary sensory disturbances or dysesthesia 203 are described in many patients. In a study by Gazelka et al 205 neuralgia after RF denervation of the TON was reported in 12 of 64 patients without neurological deficits.
Dreyfuss et al 206 were able to demonstrate diffuse atrophy of the multifidus muscle in 5 patients after 17 to 26 months after unilateral RF denervation. However, the 3 blinded radiologists were only able to correctly identify the side and level of the lesion in 1 patient. Clinical consequences of the atrophy were not found. Smuck et al 207 found no significant difference in the area of the multifidus muscle or negative changes in the facet joints in 27 patients after RF denervation, but increased degeneration of the intervertebral discs. Another study 208 examined the proportion of fat tissue in the multifidus muscle before and at least 6 months after RF denervation. A difference in relation to fatty degeneration could not be determined.
Skin burns due to the lesion extending too far, 209 the neutral electrode 210 or a malfunction of the RF generator 211 are conceivable and described as case reports in the literature.212,213 There may be an increased risk with cooled-RF due to the larger lesion 214 and with strip electrodes. 209
Injuries to the lumbar spinal nerves are rare. A single case report describes radicular L5 pain and sensory disturbances after RF denervation.
215
Bogduk et al.
216
describe 2 unpublished spinal cord injuries after cervical RF denervation, 1 with the development of Brown-Séquard syndrome and 1 infarction with probably coagulation of an artery supplying the spinal cord in the foramen. Donohue and White
217
describe a thoracic spinal cord change after an RF denervation of the thoracic spine, without being able to clarify the mechanism of the injury. Recommendations and statements 20.1 Serious complications are very rare after RF denervations (only single cases in the literature). (Quality of Evidence: low) 20.2 It is important to include existing imaging (particularly MRI) for anatomical variants (eg, course of the vertebral artery) in planning for RF denervation of the cervical spine. (Recommendation: EC) 20.3 It is important to inform patients prior to RF denervation of the possibility of a transient increase in pain or of prolonged pain and dysesthesia. Pain that lasts longer than 2 weeks is very rare. (Recommendation: EC)
Discussion
Unlike standards that offer little room for deviation, guidelines tend to be more flexible and allow for variations based on physician judgment and unique patient characteristics. For areas of medicine with there is a lack of high-quality clinical trials to guide treatment and a consensus regarding best practices, the development of inclusive guidelines becomes even more important.
A multidisciplinary expert group formulated a national clinical guideline for RF denervation of the facet joints and the SI joint. These guidelines were developed to serve as a roadmap for physicians who treat cervical, lumbar, and sacral joint pain and for interested patients. There can be wide variations in the conclusions of experts from different specialties on the effectiveness of pain management procedures. Reasons for incongruities include conscious and unconscious bias, differences in patient selection and in the technical implementation of the RF denervation.
Strengths of this national clinical guideline include the interdisciplinary chairmanship by the German Spine Society (DWG), the rigorous adherence to the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach for assessing the overall quality of evidence, and the rigorous adherence to relevant scientific standards. Furthermore, the guideline working group were composed of clinicians and academic researchers with a range of professional backgrounds, as well as relevant professional societies. Finally, the guidelines were peer-reviewed by the Association of the Scientific Medical Societies of Germany (AWMF) who provided detailed comments which resulted in revisions and clarifications prior to release of the final report. All participating organizations approved the document.
The main weakness of this work relates to the limited scientific evidence for some recommendations due to the lack of published clinical trials in some areas; therefore, the recommendations are mostly based on low quality of evidence. We chose 20 key questions to address in these guidelines, but this list is by no means exhaustive. In many cases, the answers to the questions we addressed will be controversial because there are gaps in the literature. Areas of controversy include all aspects of lumbar facet joint arthropathy, such as the value of history and physical examination and imaging, how to perform and interpret diagnostic injections, and technical aspects of the RF denervation.
Conclusion
Clinical trials evaluating RF denervation are characterized by widely disparate outcomes, and there is enormous variation in selecting patients and performing procedures. A multidisciplinary working group developed a national clinical guideline for RF denervation of the spine and the SI joint in adult patients. These multi-society guidelines have been developed to improve outcomes, enhance safety, and minimize unnecessary tests and procedures.
The recommendations are based on limited evidence or on consensus but are well aligned with recommendations from similar international guidelines. The guideline working groups strongly recommend that research efforts in relation to all aspects of the management of LBP and RF denervation be intensified.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Potential conflicts of interest have been declared by all involved partners and made publicly available on the webpage of The Association of the Scientific Medical Societies of Germany (AWMF): ![]() . No member of the guideline developing group had a high risk of conflict of interest.
. No member of the guideline developing group had a high risk of conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.