
Abstract
Study Design:
Systematic review and meta-analysis.
Objective:
To investigate the effect and safety of acupuncture for the treatment of chronic spinal pain.
Methods:
MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, the WHO Clinical Trial Registry, and the US National Library of Medicine clinical trial registry were searched from January 1, 2000, to November 1, 2019. Randomized controlled trials (RCTs) involving patients with chronic spinal pain treated by acupuncture versus sham acupuncture, no treatment, or another treatment were included.
Results:
Data was extracted from 22 RCTs including 2588 patients. Pooled analysis revealed that acupuncture can reduce chronic spinal pain compared to sham acupuncture (weighted mean difference [WMD] −12.05, 95% confidence interval [CI] −15.86 to −8.24), mediation control (WMD −18.27, 95% CI −28.18 to −8.37), usual care control (WMD −9.57, 95% CI −13.48 to −9.44), and no treatment control (WMD −17.10, 95% CI −24.83 to −9.37). In terms of functional disability, acupuncture can improve physical function at immediate-term follow-up (standardized mean difference [SMD] −1.74, 95% CI −2.04 to −1.44), short-term follow-up (SMD −0.89, 95% CI −1.15 to −0.62), and long-term follow-up (SMD −1.25, 95% CI −1.48 to −1.03).
Conclusion:
In summary, compared to no treatment, sham acupuncture, or conventional therapy such as medication, massage, and physical exercise, acupuncture has a significantly superior effect on the reduction in chronic spinal pain and function improvement. Acupuncture might be an effective treatment for patients with chronic spinal pain and it is a safe therapy.
Introduction
Chronic spinal pain carries a heavy price tag in the world.1-5 The annual personal health care spending of chronic spinal pain was about 87.6 billion, which ranks third behind diabetes and heart disease treatment. 6 It is the leading reason for visits to licensed acupuncturists, and many medical acupuncturists consider acupuncture an effective treatment for chronic spinal pain. 7
Currently, the voice of whether acupuncture should be used to treat spinal pain is disharmony. The National Institute for Health and Care Excellence (NICE), the American College of Physicians (ACP), and the Danish Health Authority (DHA) give inconsistent recommendations on the use of acupuncture for low back pain treatment. The ACP strongly recommends that clinicians and patients initially select the nonpharmacologic treatment (including acupuncture), 7 while the NICE and DHA do not recommend acupuncture as a conventional treatment for patients with low back pain.8,9 The Royal Dutch Society for Physical Therapy guidelines do not recommend acupuncture for treating neck pain; however, the Italian Society of Physical and Rehabilitation Medicine guidelines recommend acupuncture for pain relief of subacute and chronic neck pain.10,11 These recent guidelines give conflicting results, so it is important to update our knowledge about whether we can use acupuncture for treating chronic spinal pain.
In this article, we review the research landscape to determine the efficacy of acupuncture for chronic spinal pain. First, we conduct a comprehensive systematic review to summarize available clinical studies. We then calculate the effect size using meta-analysis methods. Finally, we construct an evidence mapping to visually present the different clinical studies about the effect of acupuncture for treating chronic spinal pain.
Methods
Study Registration
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement 12 (Supplementary File 1) and has been registered on a platform previously (PROSPERO CRD42019120665).
Literature Search
We searched MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, the World Health Organization Clinical Trial Registry (http://apps.who.int/trialsearch/Default.aspx), and the US National Library of Medicine Clinical Trial Registry (https://clinicaltrials.gov/) from January 1, 2000, to November 1, 2019. The search strategy was based on the guidance in the Cochrane handbook. The keywords and medical subject heading (MeSH) terms included “chronic low back pain” OR “chronic neck pain” OR “lumbago” OR “back pain” OR “neck pain” OR “sciatica” AND “acupuncture” OR “electro-acupuncture” OR “manual acupuncture” OR “fire needling” OR “auricular acupuncture” OR “scalp acupuncture” OR “abdominal acupuncture” OR “warm acupuncture.” There were no restrictions on language or publication period. This search strategy was applied to all the electronic databases. Two authors (JFH and XQZ) read and screened the titles and abstracts to identify eligible trials according to the inclusion criteria; the full text was reviewed if necessary. Any discrepancies were resolved by discussion with the third author (DC).
Study Selection
Inclusion
(1) Prospective randomized controlled trials (RCTs) design to evaluate the use of acupuncture to treat chronic spinal pain; (2) participants with chronic neck pain, chronic low back pain, or sciatica for more than 3 months; (3) sample size >20 participants; and (4) mixed population trials if separate data was reported for participants with chronic spinal pain.
There was no restriction on sex, age, or symptom intensity. Any type of acupuncture was included in our study, such as acupuncture, electro-acupuncture, fire needling, auricular acupuncture, abdominal acupuncture, warm acupuncture, and bee venom acupuncture. Control interventions included usual care, no treatment/waiting list control, sham acupuncture/placebo, or pharmacological therapies.
Exclusion
(1) Non-RCT design; (2) patients with acute infection, acute injury, spinal deformity, vertebral compression fractures or tumor, or cauda equina syndrome; (3) no aimed data; (4) comparison of 2 types of acupuncture; (5) evaluation of postoperative analgesia using acupuncture in participants with spinal pain; and (6) follow-up time <2 weeks after treatment session was completed.
Outcomes
The primary outcome was pain intensity, which was measured by the Visual Analogue Scale (VAS; range 0 to 100) and Numerical Rating Scale (NRS; range 0 to 10). 13 Secondary outcomes were assessed by the Oswestry Disability Index (ODI; range 0 to 100) and Roland Morris Disability Questionnaire (RMDQ; range 0 to 24). 14 In addition, adverse events caused by interventions were recorded. We defined “postintervention” as the assessment conducted on the same day after the last treatment and “follow-up” as the first assessment conducted on a different day after the last treatment.
Data Extraction and Quality Assessment
Two authors (JFH and XQZ) extracted general information (name and year of publication, date of extraction, title of study and author’s publication details), study characteristics, eligibility criteria, interventions, outcome measurements, duration, adverse events, results and the type of intervention, independently using a data extraction form. Any disagreement was discussed and finally decided on by the third author (DC). According to the guidelines of the Cochrane Handbook of Systematic Reviews of Interventions, 15 the Cochrane Collaboration’s tool was used to assess the risk of bias in the included RCTs. This tool consists of 7 factors: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias. Then the reviewers summarized the assessments and categorized the bias into 3 levels: low, high, and unclear risk of bias. The risk of bias was assessed independently. Any disagreements were resolved by discussion or consultation with the third author (DC). Whenever necessary, the original authors of the studies were contacted for missing data or additional information.
Evidence Mapping
We built an evidence map to visualize the results of included RCTs. The x-axis represents the effect of acupuncture for pain or disability grouped into 3 categories: no effect, unclear or mixed effect, and positive effect. We defined evidence of no effect as there was evidence that acupuncture had no impact on spinal pain compared with control group. We defined evidence with unclear or mixed effect as there was not enough or multiple conflicting evidence to show the effect of acupuncture. We defined evidence of positive effect as there was clear and enough evidence to draw the conclusion that acupuncture was more effective than control group.
Statistical Analysis
We divided outcomes into 4 groups, according to follow-up time: follow-up period <2 weeks as immediate term; follow-up between 2 weeks and 3 months as short term; follow-up between 3 months and 6 months as medium term and follow-up ≥6 months as long term. Then, we conducted subgroup analyses based on the type of chronic spinal pain (chronic low back pain, chronic neck pain, and sciatica), type of acupuncture (acupuncture, laser acupuncture, electro-acupuncture, auricular acupuncture, etc), type of control group (sham acupuncture, no treatment, usual care or medication), and risk of bias (low risk of bias, unclear risk of bias, and high risk of bias).
In our study, “usual care” was defined in the context of each individual intervention and consisted of routine physiotherapy, massage, or back exercise therapy. The meta-analysis was performed with Stata software (version 12.0; StataCorp). For continuous outcomes, the weighted mean difference (WMD) or standardized mean difference (SMD) with 95% confidence intervals (CIs) was calculated if different measurement scales were used. Dichotomous outcomes were analyzed using relative risks (RRs) with 95% CIs. Considering the ineluctable heterogeneity, we used the random-effect model to provide a more conservative estimate of effect for all pooled analysis. If the data was not suitable for quantitatively combination, we provided a systematic narrative synthesis with the information presented in the text to summarize and explain the characteristics and findings of the included studies. Then funnel plots were used to assess publication biases, and Duval and Tweedie’s nonparametric trim-and-fill method was used to explore potential publication bias. 16 For heterogeneous data, sensitivity analysis with a random model was used to remove one study and evaluate whether the other results were markedly affected.
Results
Study Identification and Selection
Details of the selection process are shown in the PRISMA flow chart (Figure 1). In summary, 1861 studies were manually screened by title and/or abstract, of which 1534 records were deemed irrelevant. The remaining 327 records were retrieved in full text. However, 224 records are not randomized clinical trials, 38 records are lacking outcomes, 23 records have incorrect study design, 14 records contain inappropriate interventions, and 4 records are case reports. In total, 24 RCTs were included in the systematic review,17-40 22 records were included in the meta-analysis,17-30,33-40 but the other 2 records did not provide complete data or relevant outcomes and were excluded.31,32
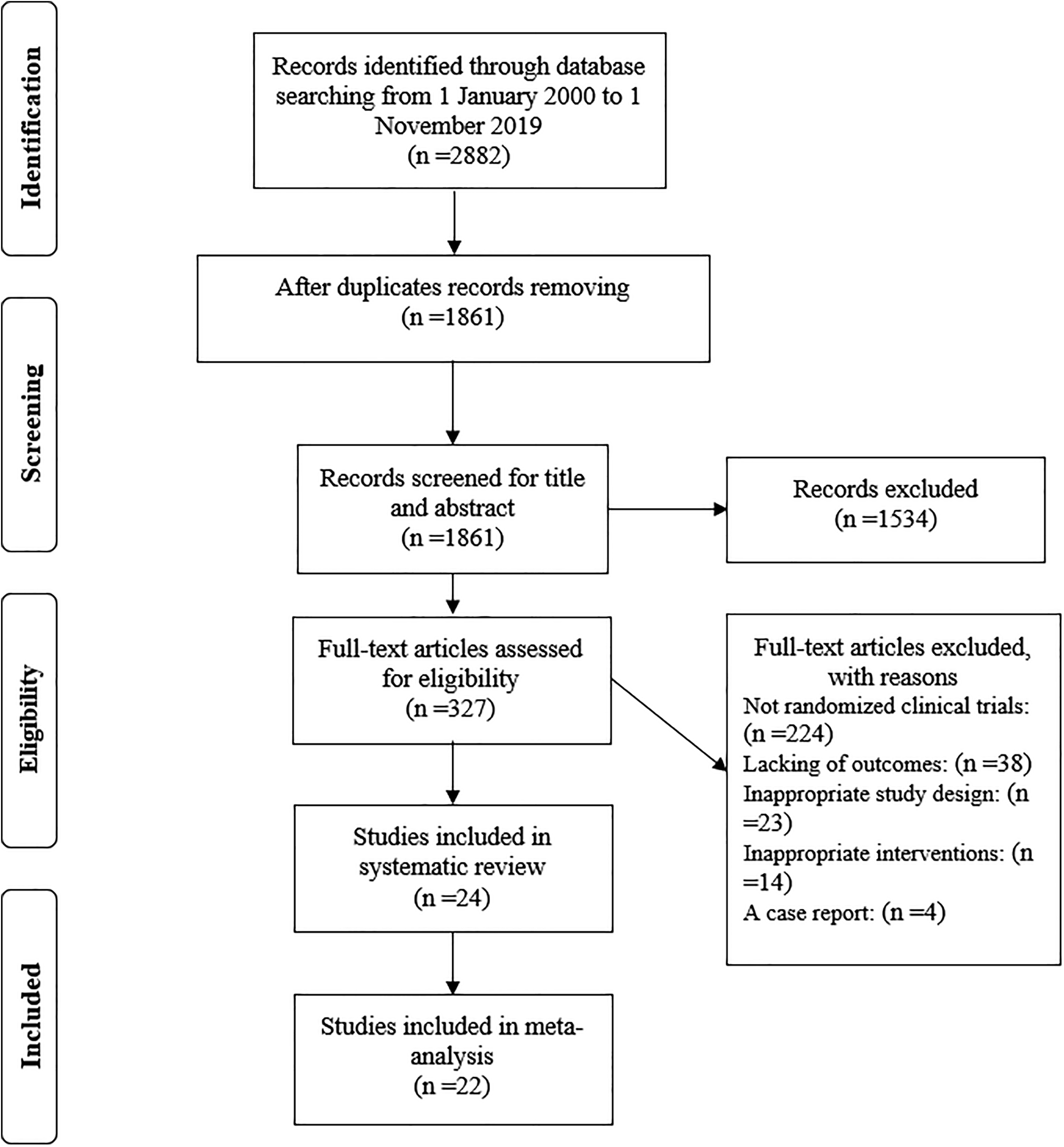
Flow diagram for study identification, screening, eligibility assessment, and inclusion.
Study Characteristics
A descriptive summary of the studies included in the review is shown in Tables 1 and 2. Sixteen records involved standard acupuncture with needle stimulation, 5 records involved laser/electro-acupuncture, 2 records involved auricular acupuncture, and 1 record involved bee venom acupuncture. The duration of interventions ranged from 1 treatment to 8 weeks of treatment. The follow-up time ranged from 2 weeks to 1 year after the final treatment. In many studies, the pain was considered the primary outcome, while disability and adverse events were considered as secondary outcomes. The outcomes of most studies were measured using the VAS or NRS, the ODI, the RMDQ, and adverse event incidence rates.
Demographic Characteristics of Patients of Included Studies.
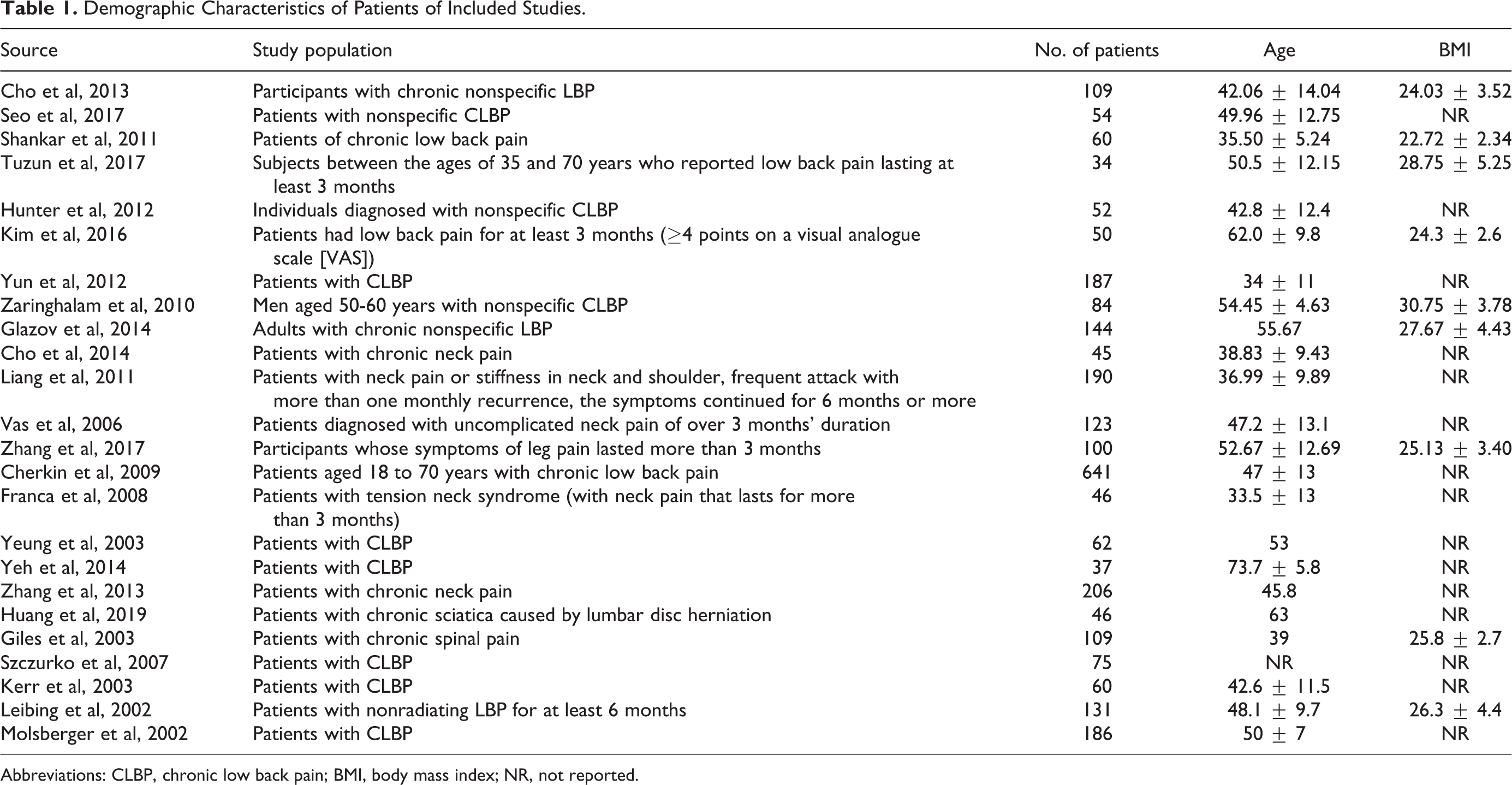
Abbreviations: CLBP, chronic low back pain; BMI, body mass index; NR, not reported.
The Study Design of Included Studies.
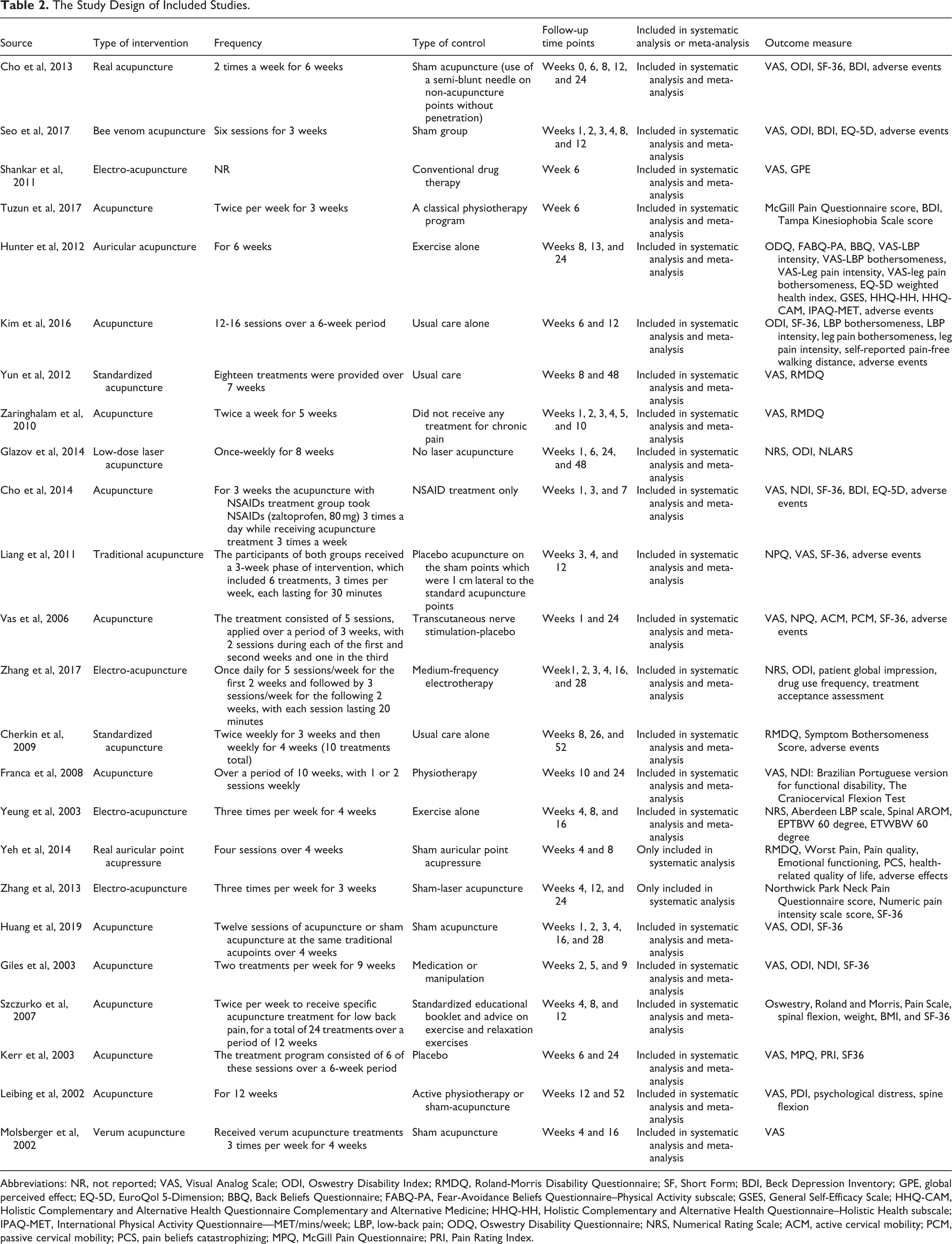
Abbreviations: NR, not reported; VAS, Visual Analog Scale; ODI, Oswestry Disability Index; RMDQ, Roland-Morris Disability Questionnaire; SF, Short Form; BDI, Beck Depression Inventory; GPE, global perceived effect; EQ-5D, EuroQol 5-Dimension; BBQ, Back Beliefs Questionnaire; FABQ-PA, Fear-Avoidance Beliefs Questionnaire–Physical Activity subscale; GSES, General Self-Efficacy Scale; HHQ-CAM, Holistic Complementary and Alternative Health Questionnaire Complementary and Alternative Medicine; HHQ-HH, Holistic Complementary and Alternative Health Questionnaire–Holistic Health subscale; IPAQ-MET, International Physical Activity Questionnaire—MET/mins/week; LBP, low-back pain; ODQ, Oswestry Disability Questionnaire; NRS, Numerical Rating Scale; ACM, active cervical mobility; PCM, passive cervical mobility; PCS, pain beliefs catastrophizing; MPQ, McGill Pain Questionnaire; PRI, Pain Rating Index.
Evidence Mapping
For chronic neck pain, 4 RCTs showed enough evidence to support the positive effect of acupuncture compared with control group, while 2 RCTs pointed that acupuncture may facilitate patients’ rehabilitation but need larger size studies to prove the effect. For chronic low back pain, 9 RCTs supported the positive effect of acupuncture, while 5 RCTs showed conflicting results and 3 RCTs lacked evidence to show the positive effect of acupuncture. As for sciatica, 2 RCTs pointed the positive effect of acupuncture, whereas 1 RCT did not have enough evidence to show the effect of acupuncture (Figure 2).
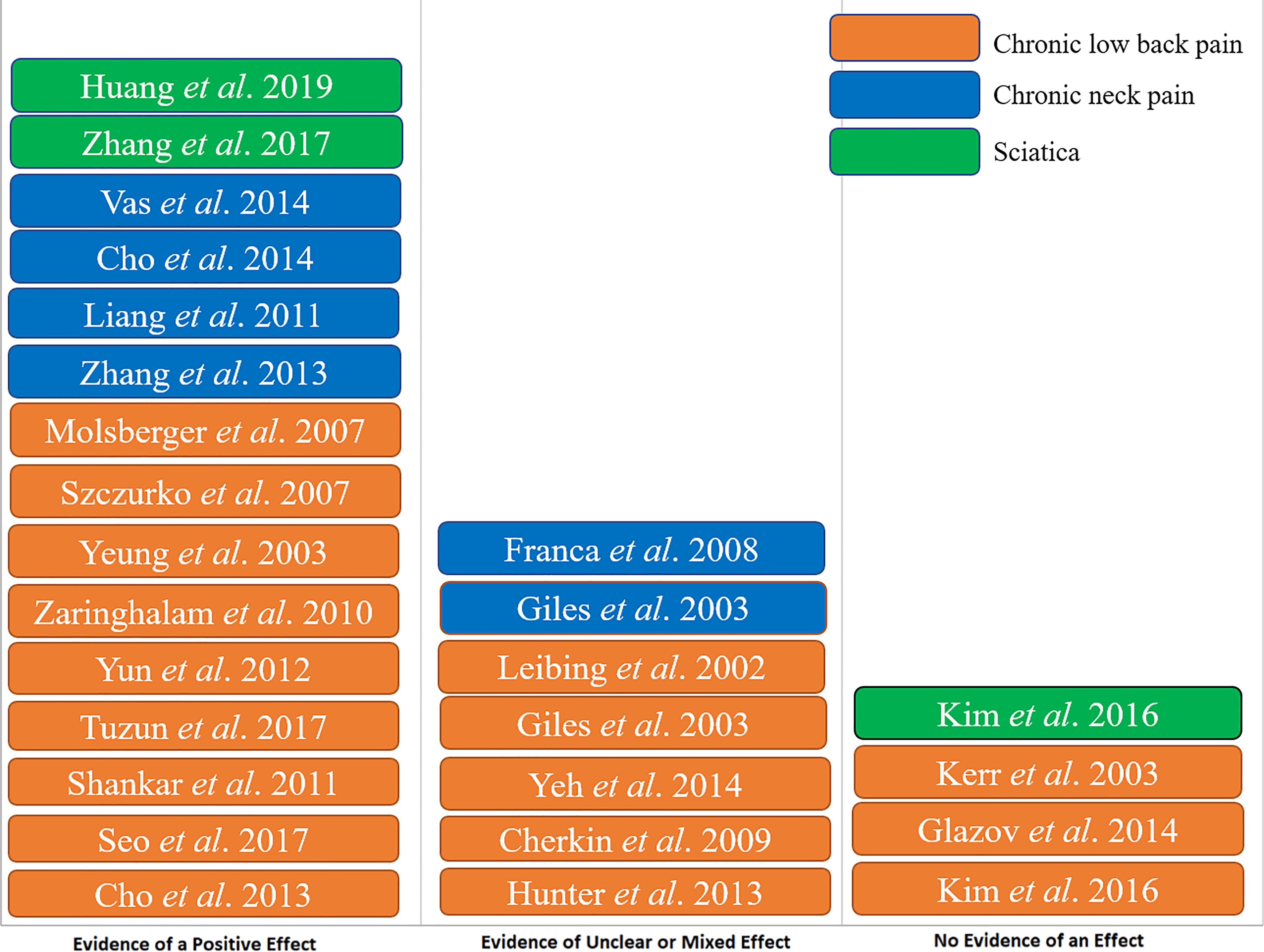
Evidence map synthesizing the strength of the evidence of acupuncture for spinal pain.
Methodological Quality
An overview of the risk of bias assessment of the included studies is shown in Table S1. Fourteen studies had a high risk of bias, 5 studies had a low risk of bias, and 5 studies had an unclear risk of bias. All studies fulfilled or partly fulfilled the requirements of allocation concealment, selective outcomes, incomplete outcome data, and other sources of bias. Eight studies were considered to have a high risk of bias because of a lack of the blinding of the participants and personnel.
Pain Intensity
Pooling of all included trials revealed that acupuncture, compared to control treatments, reduced chronic neck pain (WMD −16.60, 95% CI −27.37 to −5.83, I2 97.6%, low-quality evidence, including 6 studies and 522 patients), chronic low back pain (WMD −12.33, 95% CI −15.23 to −9.44, I2 91.6%, moderate-quality evidence, including 13 studies and 1259 patients), pain from sciatica (WMD −11.94, 95% CI −13.22 to −10.67, I2 0%, high-quality evidence, including 3 studies and 196 patients) in the immediate-term (Figure 3A, including 20 studies and 1931 patients).17-24,26-28,32-40 Mean differences in the efficacy of acupuncture for chronic spinal pain treatment at immediate-term (A), short-term (B), medium-term (C), and long-term (D) follow-up. Immediate-term = follow-up ≤2 weeks; short term = follow-up >2 weeks but ≤3 months; medium-term = follow-up >3 months but <6 months; long-term = follow-up ≥6 months.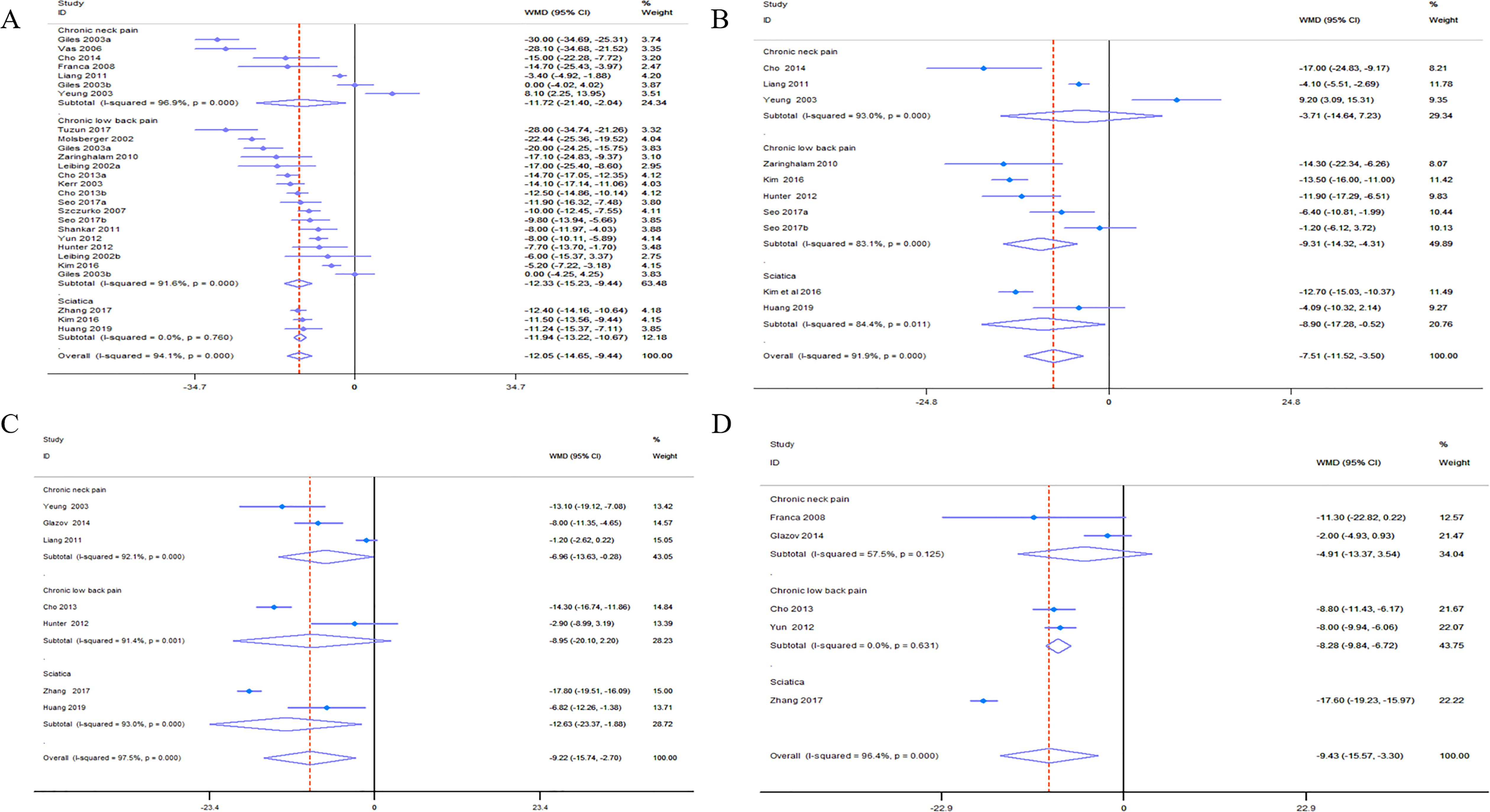
For short-term outcomes, acupuncture had a significant effect on the reduction in chronic low back pain (WMD −9.31, 95% CI −14.32 to −4.31, I2 83.1%, moderate-quality evidence, including 4 studies and 319 patients) and pain from sciatica (WMD −8.90, 95% CI −17.28 to −0.52, I2 84.4%, moderate-quality evidence, including 2 studies and 96 patients). However, acupuncture showed a limited effect on the reduction in chronic neck pain (WMD −3.71, 95% CI −14.64 to 7.23, I2 93.0%, low-quality evidence, including 3 studies and 297 patients; Figure 3B, including 9 studies and 605 patients).18,21,22,24,26,27,34,35
For medium-term outcomes, acupuncture had a relatively smaller effect on the reduction in chronic neck pain (WMD −6.96, 95% CI −13.63 to −0.28, I2 92.1, moderate-quality evidence, including 3 studies and 369 patients) and chronic low back pain (WMD −8.95, 95% CI −20.1 to 2.20, I2 91.4%, low-quality evidence, including 2 studies and 161 patients) than that observed for immediate-term outcomes and had a significant effect on sciatica treatment (WMD −17.80, 95% CI −19.51 to −16.60, I2 93.0%, moderate-quality evidence, including 2 studies and 146 patients; Figure 3C, including 7 studies and 639 patients).17,21,25,27,29,34,35
In the long-term, acupuncture, compared to the control treatments, had only a modest effect on the reduction in chronic neck pain (WMD −4.91, 95% CI −13.37 to 3.54, I2 57.5%, low-quality evidence, including 2 studies and 190 patients) and chronic low back pain (WMD −8.28, 95% CI −9.84 to −6.72, I2 0%, high-quality evidence, including 2 studies and 296 patients) and a significant effect on sciatica treatment (WMD −17.60, 95% CI −19.23 to −15.97, I2 0%, moderate-quality evidence, including 1 study and 100 patients; Figure 3D, including 5 study and 692 patients).17,23,25,29,33
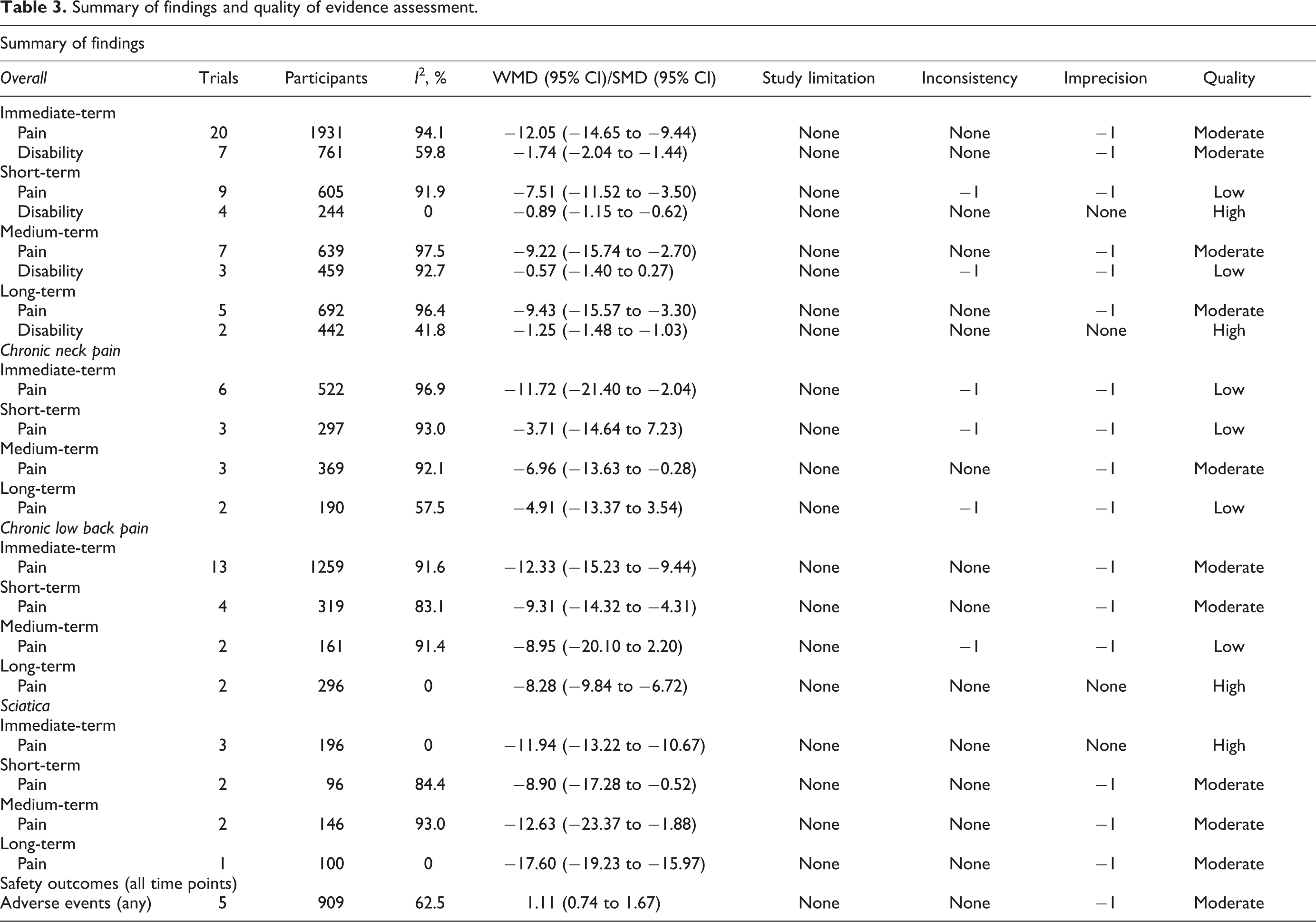
A detailed summary of the above findings and the GRADE assessment is shown in Table 3.
Summary of findings and quality of evidence assessment.
Subgroup Analysis of the Primary Outcome
Next, we then sub-analyzed the outcomes of different types of acupuncture and of acupuncture versus sham acupuncture, no treatment, medication, and usual care (physiotherapy programs, exercise, electrotherapy, etc) and the risk of bias. For pain reduction, the results show that normal acupuncture had greater effects (WMD −14.97, 95% CI −18.33 to −11.62, I2 95.6%, moderate-quality evidence, including 16 studies and 1634 patients) than other styles of acupuncture in the immediate-term. Acupuncture had the greatest effect when compared to medication (WMD −24.62, 95% CI −36.55 to −12.68, I2 96.1%, moderate-quality evidence, including 3 studies and 214 patients) and had relatively good effects when compared to usual care (WMD −9.57, 95% CI −13.48 to −9.44, I2 92.9%, moderate-quality evidence, including 11 studies and 919 patients), sham acupuncture (WMD −12.05, 95% CI −15.86 to −8.24, I2 94.8%, moderate-quality evidence, including 8 studies and 976 patients), and no treatment (WMD −17.10, 95% CI −24.83 to −9.37, I2 0%, moderate-quality evidence, including 1 study and 84 patients). Additionally, we found that trials assessed as having a high risk of bias (WMD −13.45, 95% CI −17.23 to −9.66, I2 96.2%, moderate-quality evidence, including 14 studies and 1379 patients) found greater effects of acupuncture treatment than trials assessed as having a low risk of bias (WMD −11.99, 95% CI −13.94 to −10.03, I2 44.6%, high-quality evidence, including 4 studies and 432 patients), but smaller effects than trials assessed as having an unclear risk of bias (WMD −14.51, 95% CI −17.25 to −11.78, I2 0%, high-quality evidence, including 3 studies and 190 patients; Table 4).
Secondary exploratory analyses for pain.
Abbreviations: WMD, weighted mean difference; CI, confidence interval.
Functional Disability
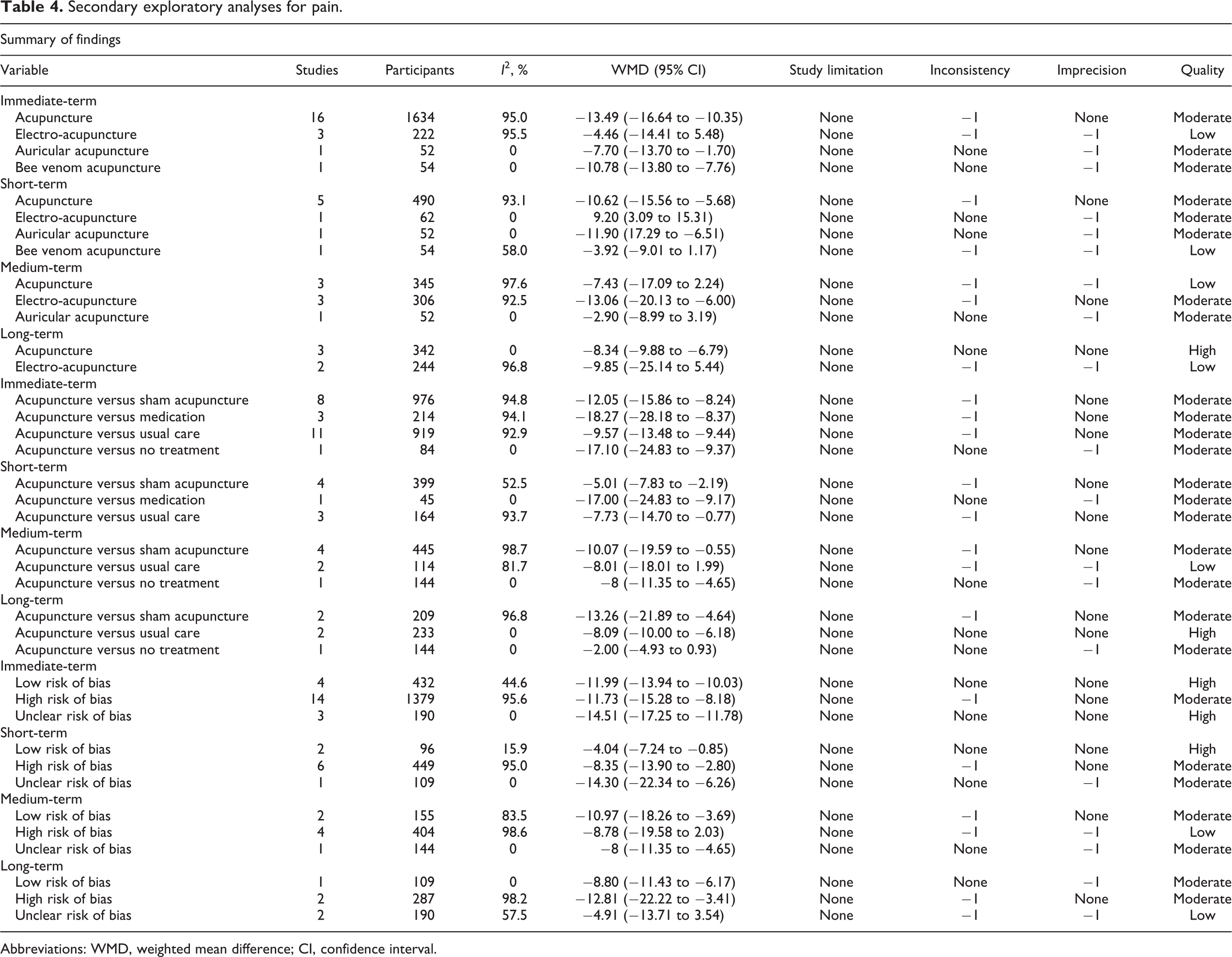
Seven studies measured functional disability: 4 used the ODI to measure disability outcomes,18,22,25,35 and the others used the RMDQ.23,24,30 The effect of acupuncture, compared to the control treatment, on the treatment of function limitation was −1.74 at immediate-term follow-up (95% CI −2.04 to −1.44, I2 59.8%, moderate-quality evidence; Figure 4A, including 7 studies and 761 patients),18,22-24,30,35,37 −0.89 at short-term follow-up (95% CI −1.15 to −0.62, I2 0%, high-quality evidence; Figure 4B, including 4 studies and 244 patients),18,22,24,35 −0.57 at medium-term follow-up (95% CI −1.40 to 0.27, I2 92.7%, low-quality evidence; Figure 4C, including 3 studies and 459 patients),25,30,35 and −1.25 at long-term follow-up (95% CI −1.48 to −1.03, I2 41.8%, high-quality evidence; Figure 4D, including 2 studies and 442 patients).23,30
Standard mean differences in the efficacy of acupuncture on disability during chronic spinal pain treatment at immediate-term (A), short-term (B), medium-term (C), and long-term (D) follow-up. Disability was measured by the ODI or RMDQ scale. Immediate-term = follow-up ≤2 weeks; short-term = follow-up >2 weeks but ≤3 months; medium-term = follow-up >3 months but <6 months; long-term = follow-up ≥6 months.
Safety
Six trials provided information on adverse events. There was no difference in adverse event rates between acupuncture and other treatments (RR 1.11, 95% CI 0.74 to 1.67, I2 62.5%, moderate-quality evidence; Figure 5, including 5 studies and 909 patients).17,18,22,27,41 No trials reported data on serious adverse events during acupuncture treatment. The most frequent adverse events were temporarily worsened pain and needle pain at the acupuncture site, which can decrease quickly after a short period of rest.
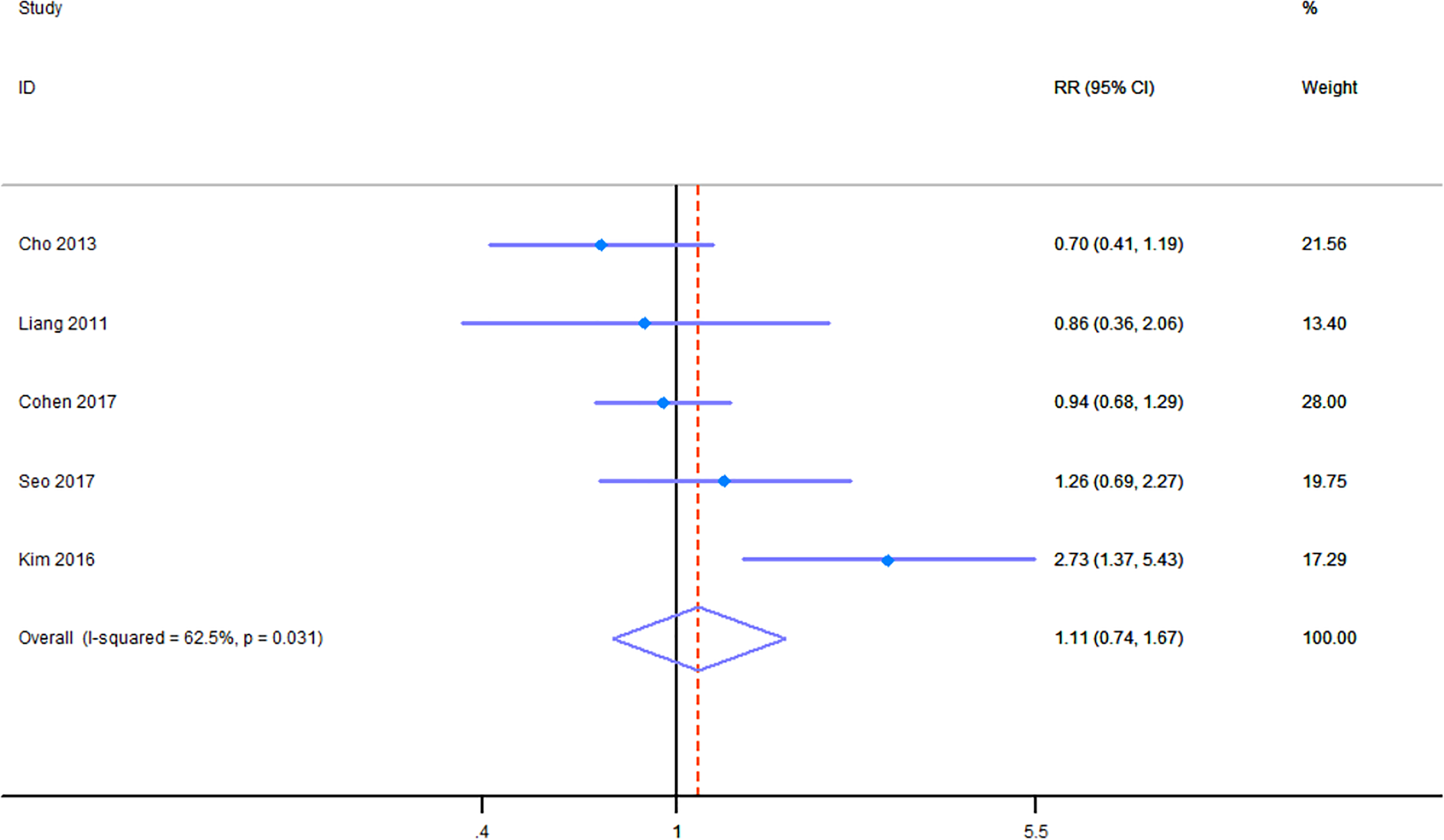
Forest plot of the results of the meta-analysis of the risk ratio.
Publication Bias and Sensitivity Analysis
The funnel plots, which were generally symmetrical, indicated that there was no significant publication bias for each outcome measure (Figure S1). We used the trim-and-fill method, which imputes artificial studies to achieve symmetry of the funnel plot, to estimate the adjusted risk ratio for publication bias. The trim-and-fill method showed that no additional artificial studies needed to be included in the meta-analysis to generate a symmetrical funnel plot, so there was no potential publication bias (Figure S2).
Sensitivity analysis was used to evaluate the effects of each individual study. The outcome suggested that the results are relatively robust (Figure S3).
Discussion
Chronic spinal pain, a major public health problem in many countries, causes tremendous pain in patients and seriously affects the quality of life. To date, the recommendations of acupuncture for spinal pain are inconsistent.7-9 In our study, 22 RCTs were included in the meta-analysis to evaluate the effectiveness of acupuncture in treating chronic spinal pain. The results of the included studies suggest that acupuncture can significantly relieve pain when compared with sham acupuncture17,18,27,29,35 or other common treatments,20,23,28 and acupuncture combined with other interventions is better than the intervention alone.21,22,24,26,34 Some studies have shown that acupuncture can significantly improve the function of chronic spinal pain patients.30,33 In addition, other studies indicated that acupuncture is a feasible and safe therapy for reducing chronic spinal pain.19,31 However, Zhang et al pointed out that no long-term benefit could be demonstrated for acupuncture. 32 Our findings indicate that acupuncture can reduce pain in the immediate term and short term.
For patients with chronic low back pain, our analysis shows that acupuncture had an excellent ability to reduce pain in the immediate term and short term. Xu et al defined long-term follow-up as follow-up after 4 weeks to 1 year and noted that acupuncture is effective at providing long-term relief from chronic low back pain. 42 To assess the follow-up more accurately, we defined 4 different follow-up terms: immediate-term (<2 weeks), short-term (≥2 weeks and <3 months), medium-term (≥3 months and <6 months), and long term (≥6 months). We found that the effect on pain reduction drops dramatically in the medium term, which may seriously affect patients’ daily lives and reduce confidence in this therapy. For patients with chronic neck pain, the effect on pain relief decreases considerably in the short term and medium term. Moffet et al showed that acupuncture may alter brain chemistry by changing the release of neurotransmitters and neurohormones, thus affecting the parts of the central nervous system related to sensation and involuntary body functions. 43 The disappearance of the effect might be due to the reduction in these neurotransmitters and neurohormones. For patients with sciatica, acupuncture has a stable effect on pain relief. Our findings are important for the clinical application of acupuncture in the management of chronic spinal pain. Additionally, previous studies indicated that acupuncture is not more effective than other treatments.44-46 However, in contrast to these earlier findings, we found that acupuncture is significantly more effective than other treatments including medication therapy, massage, physical exercise, and other usual treatments. Moffet et al indicated that acupuncture is not statistically significantly different from sham acupuncture for pain reduction and that sham acupuncture is efficacious for pain relief. 47 However, our results show that acupuncture is more effective than sham acupuncture and that sham acupuncture may have an effect on the reduction in chronic spinal pain. Therefore, future studies may concentrate on researching non-penetrating acupuncture and its mechanism.
Our findings show that the effects of acupuncture are smaller on physical function improvement than on pain reduction. Lehmann et al indicated that acupuncture cannot immediately improve physical function after the end of the treatment sessions. 48 However, we found that acupuncture can improve the function of patients with chronic spinal pain in the immediate and short term. Tsukayama et al showed that acupuncture may not improve physical function at intermediate follow-up, which was similar to our findings that the effect of acupuncture on physical function improvement will not persist at medium-term follow-up. 49
Melchart et al noted that the incidence of minor adverse reactions was 91 per 10 000 treatments, and the incidence of major adverse reactions was 6 per 1 000 000 treatments. 50 MacPherson et al 51 and White et al 52 showed that the incidence of minor adverse events was approximately 0.1%, and no major adverse reactions were observed. All of these outcomes suggest the safety of acupuncture, which is consistent with our findings. In our study, no major adverse events were reported in the trials included in the meta-analysis and the RR of minor adverse events was 1.11 (95% CI, 0.74 to 1.67). In general, compared to sham acupuncture, medication, usual care, and no treatment, acupuncture affected pain reduction and functional limitations.
Previous studies have indicated that cognitive behavioral therapy (CBT) and mindfulness-based stress reduction, compared with usual care, can significantly reduce back pain and functional limitations in both the short and long term.53-56 However, Sterling et al noted that there is no obvious evidence to determine whether psychological treatments alone are effective for chronic neck pain. 57 Also, NICE advised that psychological therapies should be used only as part of multimodal treatment options that are effective for reducing pain and disability and improving work status.58,59 Therefore, psychological therapy should be combined with physical treatment. 57 Lifestyle factors such as stress, sleep problems, depression, smoking, alcohol use, and obesity play important roles in the reduction in chronic spinal pain.60-62 Therefore, addressing any lifestyle problems can lead to a long-term decrease in chronic spinal pain. 63 In general, acupuncture may be more effective than CBT or multimodal treatment in the immediate term at reducing chronic spinal pain, while CBT or multimodal treatment may be more effective in the long-term management of spinal pain.
Previous studies have indicated that 50% of patients recover quickly in 2 to 3 weeks after good-quality first-line care (education, reassurance, and analgesic medicines), so providing nonpharmacological therapies to all patients is unnecessary and wasteful of health care resources.3,64 Besides, nonpharmacological therapies should be emphasized more in the management of chronic pain than acute pain.65-67 Providing advice, reassurance, and exercise instruction for patients with chronic spinal pain is also a first step, and first-line treatment recommended by many studies.68-71 Education in combination with physiotherapy is more effective than education or physiotherapy alone.72,73 Therefore, education combined with exercise and physiotherapy should be the first-line treatment for any case of acute or chronic spinal pain. However, for those who are not responding to first-line treatments or who are still functionally disabled by pain after first-line treatment, multimodal treatment, and nonpharmacological therapy, such as spinal manipulation, massage, acupuncture, and yoga, may be better choices for pain management.9,57,59 If one is not responding to nonpharmacological therapy, pharmacological treatment is recommended. 71 However, for those who do not respond to conservative care, have common degenerative spinal changes or persistent and disabling symptoms or have symptomatic spinal stenosis, surgery should be considered as an optimal solution.3,74 Generally, specific treatments should be personalized for different patients.75,76
Strengths
The strengths of our review are that we strictly followed the PRISMA recommendations, including the use of GRADE to appraise the quality of the evidence. In addition, past reviews studied the effect of acupuncture on only chronic low back pain, chronic neck pain, or sciatica.77-81 We comprehensively analyzed the 3 most common spinal pain to conduct a more thorough evaluation of the effects of acupuncture on various forms of spinal pain, and to include different forms of acupuncture. We also provided valuable information on pooled treatment effects for specific patients, including those with chronic neck pain, chronic low back pain, and sciatica. Moreover, we conducted subgroup comparisons including acupuncture versus sham acupuncture, acupuncture versus medication, acupuncture versus usual care and acupuncture versus no treatment to investigate the effect of acupuncture compared with those of sham acupuncture and other treatments. Compared with medication, no treatment, or usual care, acupuncture demonstrated a significant improvement in pain relief. However, the effectiveness was minimal when compared to that of sham acupuncture, which means that sham acupuncture can also reduce chronic spinal pain. A previous study reported that the underlying principle of acupuncture involves the release of neurotransmitters; however, no studies have shown whether neurochemical effects are dependent on specific acupuncture points. Our findings indicate the need for further study to clarify whether acupuncture works through specific acupuncture points. This observation may support further study of noninvasive acupuncture, which may be a promising therapy. Noninvasive acupuncture may have similar effects as normal invasive acupuncture but can avoid many adverse events such as pain and bleeding.
Limitations
Our study has some limitations. First, our meta-analysis results have significant heterogeneity, which may have been caused by the different forms of acupuncture used and the differing quality of the included studies. Second, most of the trials had only immediate-term and short-term follow-up data and a relatively small sample size. Third, because of the nature of acupuncture treatment, blinding of patients is difficult. Therefore, blinding of both patients and investigators was not properly conducted in many studies, which led to the low quality of most included RCTs. More high-quality RCTs with larger sample sizes should be conducted.
Conclusions
In summary, compared to no treatment, sham acupuncture, or usual therapy, acupuncture has a significantly superior effect on the reduction in pain and functional limitations for patients with chronic spinal pain. Our results suggest that acupuncture is also a safe therapy. Patients with chronic spinal pain might benefit from acupuncture therapy.
Supplemental Material
Supplemental Material, prisma_checklist - Can Acupuncture Improve Chronic Spinal Pain? A Systematic Review and Meta-Analysis
Supplemental Material, prisma_checklist for Can Acupuncture Improve Chronic Spinal Pain? A Systematic Review and Meta-Analysis by Jin-Feng Huang, Xuan-Qi Zheng, Dong Chen, Jia-Liang Lin, Wen-Xian Zhou, Hui Wang, Zongshi Qin and Ai-Min Wu in Global Spine Journal
Supplemental Material
Supplemental Material, supplement_1 - Can Acupuncture Improve Chronic Spinal Pain? A Systematic Review and Meta-Analysis
Supplemental Material, supplement_1 for Can Acupuncture Improve Chronic Spinal Pain? A Systematic Review and Meta-Analysis by Jin-Feng Huang, Xuan-Qi Zheng, Dong Chen, Jia-Liang Lin, Wen-Xian Zhou, Hui Wang, Zongshi Qin and Ai-Min Wu in Global Spine Journal
Footnotes
Author Contributions
JFH, ZSQ, and AMW designed the study. JFH and XQZ performed a systematic search of the literature. JFH, XQZ, DC, LJL, WXZ, and HW screened potential articles and acquired data for analysis. JFH, XQZ, and DC evaluated the methodological quality and performed statistical analysis and interpretation of data. JFH and XQZ drafted the paper. ZSQ and AMW critically revised the draft manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Natural Science Foundation of China (81 501 933), Zhejiang Provincial Natural Science Foundation of China (LY14H060008), Zhejiang Provincial Medical and Health Technology Foundation of China (2018KY129), Wenzhou Leading Talent Innovative Project (RX2016004), and Wenzhou Municipal Science and Technology Bureau (Y20170389). The funders had no role in the design, execution, or writing of the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.