
Abstract
Study Design
Retrospective analysis of an administrative dataset.
Objective
This study aims to investigate changing practice over a six-year period in the use of repeated lumbar facet joint injections/medial branch blocks in England.
Methods
Patient data were extracted from the Hospital Episodes Statistics database for the period 1st April 2015 to 31st March 2021 for the index lumbar injection and for repeat lumbar injections performed within one year of the first. The exposure of interest was two injections within 180 days or three within one year. Patients aged <17 years and where the body site was listed as cervical, thoracic or sacral were excluded.
Results
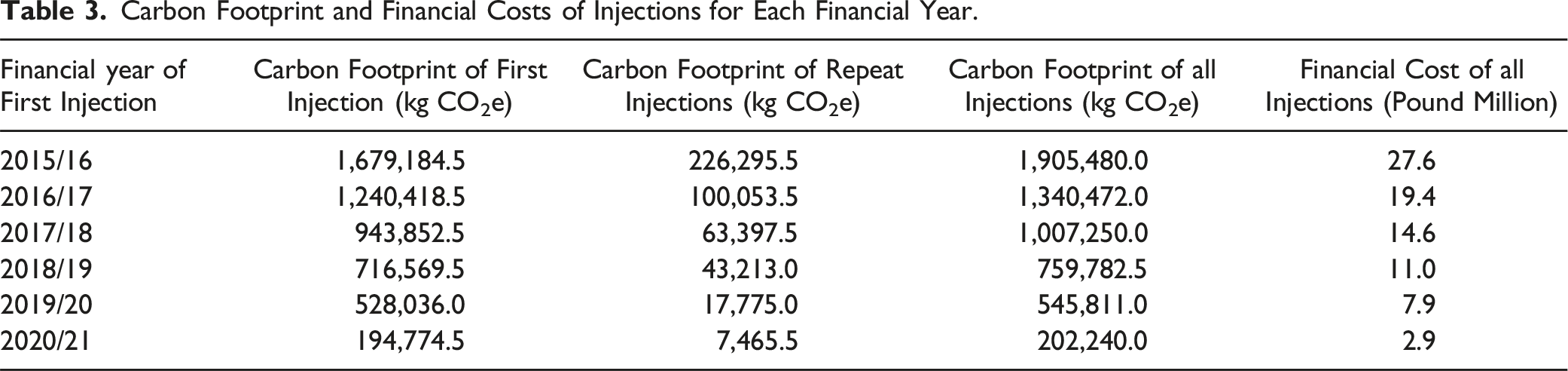
Data were available for 134,249 patients of which, 8,922 (6.6%) had either two injections within 180 days or three injections within one year. First injections fell from 42,511 in 2015/16 to 13,368 in 2019/20 as did the number of repeat injections: 4,018 to 424 for the same period. If all years had the same carbon footprint as 2019/20, 2.8 kilotons of CO2e would have been saved over the five years, enough to power 2,575 average UK homes for 1 year. The financial cost of injections decreased from £27.6 million in 2015/16 to £7.9 million in 2019/20.
Conclusions
The number of patients having repeated lumbar injections has decreased over time but has not been eliminated. More work is needed to educate patients and clinicians regarding alternative and more effective treatments.
Introduction
Low back pain is a common problem worldwide affecting people of all ages, ethnicities, demographic background and sex. It is a common cause of disability in people of working age; the worldwide prevalence of back pain in 2019 was 568 million cases, 1 and in Great Britain in financial year 2021-22, there were 202,000 self-reported cases of work related musculoskeletal disorders affecting the back. 2 A number of these cases resolve without the need for any medical intervention, but for those who have ongoing symptoms, multiple treatment methods are utilised to manage the pain.
In England, guidance for the management of low back pain and radicular pain has been available since 2014 in the form of the National Back Pain and Radicular Pain (NBPRP) Pathway. 3 This pathway has been implemented and was updated in 2016 to incorporate guidance on the management of back pain from the National Institute for Health and Care Excellence (NICE), who have endorsed the pathway.
Despite this guidance being available and supported by NICE, National Health Service (NHS) England’s Getting It Right First Time (GIRFT) programme report into spinal services published in January 2019 showed that there was still marked variation across England with regard to the management of non-specific low back pain and, in a number of centres, the guidance was not being followed. 4 One of the recommendations from both the NBPRP pathway and NICE guidance 5 was to stop performing facet joint injections (FJI) as a treatment for patients presenting with non-specific low back pain as there was a lack of evidence of clinical benefit. It was proposed to instead offer diagnostic medial branch block injections (MBB) and if these were successful in reducing pain, radiofrequency denervation to be offered and performed later. However, the GIRFT report and a recent systematic review highlighted that FJI are still being performed with some patients having multiple injections within one year for the treatment of non-specific low back pain.4,6
As well as the injections being shown to be of limited clinical benefit, repeat injections use financial and human resources and produce unnecessary carbon emissions, countering the NHS’s aim of achieving net zero carbon emissions by 2040. 7 The aim of this study was to investigate changing practice over a six-year period in the use of repeat lumbar FJI and MBB in England and the associated carbon production and financial implications.
Methods
Study Design
This was a retrospective analysis of administrative data from the Hospital Episode Statistics (HES) database. The HES database is collected by NHS Digital and includes data for NHS hospital activity in England. It is collated by clinical coders at each Trust.
Ethics
The presentation of data follows current NHS Digital guidance for use of HES data for research purposes. 8 Consent from individuals involved in this study was not required for analysis of this administrative dataset.
Data Extraction
Setting
All NHS hospitals in England are run by a trust with each trust covering a geographically defined catchment area of varying physical size and population. A single trust typically runs between one and four large secondary or tertiary care hospitals. Since 1st July 2022, NHS trusts in England have been grouped into 42 geographically based Integrated Care Boards (ICBs) with each incorporating multiple hospital trusts. 7
Time Period
The study covers all procedures performed between 1st April 2015 to 31st March 2021 for the first (index) lumbar FJI/MBB for each patient during the study period with follow up for repeat injections up to 31st March 2022. Data for first injections during the year from 1st April 2021 to 31st March 2022 were extracted separately to evaluate the impact of stopping most elective activity for periods during the year from 1st April 2020 to 31st March 2021 due to the COVID-19 pandemic. 9 One year follow up data were not available for these patients and so these data were not part of the main dataset.
Inclusion and Exclusion Criteria for Index Procedure
We identified FJI and MBB using the Office of Populations Censuses and Surveys Classification of Interventions and Procedures version 4 (OPCS-4) code V544 (injection around spinal facet of spine) which is the code for both procedures. The body site was identified as lumbar where the OPCS-4 codes Z665 (lumbar vertebra), Z675 (lumbar intervertebral joint) or Z073 (spinal nerve root of lumbar spine) were used. Where no body site was listed, injections were assumed to be in the lumbar region. This decision was made following discussions with clinical coding colleagues who suggested that as around 80% of all injections were in the lumbar region, clinicians would almost always list the body site if it was non-lumbar (being relatively uncommon). Thus, missing data would be disproportionately in the lumbar region. The number of missing values for body site is listed in the results section.
Patients were excluded where: 1. The patient was aged <17 years. 2. The body site was listed as Z071 (spinal nerve root of cervical spine), Z072 (spinal nerve root of thoracic spine), Z078 (specified spinal nerve root NEC), Z079 (spinal nerve root NEC), Z661 (axis), Z662 (atlas bone), Z663 (cervical vertebra), Z664 (thoracic vertebra), Z668 (specified vertebra NEC), Z669 (vertebra NEC), Z671 (atlanto-occipital joint), Z672 (atlantoaxial joint), Z673 (cervical intervertebral joint), Z674 (thoracic intervertebral joint), Z676 (lumbosacral joint), Z677 (sacrococcygeal joint), Z678 (specified intervertebral joint NEC) or Z679 (intervertebral joint NEC).
The first injection for each patient was identified as the index injection. Injections for the same patient in the year following the index injection were then recorded. The data extraction process is summarised in Supplementary material Figure S1.
Exposure
The exposure of interest was two injections within 180 days (6 months) or three within one year.
Outcomes
The following outcomes were considered. 1. Spinal surgery by way of facet joint denervation within one year of the first injection (OPCS-4 codes: V485, V486, V487, V488, V489 (denervation of spinal facet joint of vertebra, with lumbar vertebra specified or no vertebral site specified). 2. The carbon footprint of FJI/MBB. This was calculated using data from Greener NHS. The carbon factor for a generic surgical procedure has been estimated as 35.1 kgCO2e and the carbon factor for return patient travel as 4.4 kgCO2e giving a combined carbon factor of 39.5 kgCO2e for each injection.10,11 Values are also presented as carbon equivalents to power an average home in the UK with electricity for a year using a conversion factor of 1098.9 kgCO2e per home per year.12,13 3. The financial cost of FJI/MBB. The cost of each injection was calculated based on the 2020/21 National Tariff Payment System reference cost for ‘denervation or injection around spinal facet, for pain management’ (Health Resource Group code AB16Z) of £572 per injection.
14
Other Data Extracted
Data were extracted for each injection in relation to hospital trust, ICB responsible for the patient’s Lower Super Output Area (LSOA) of residence, financial year of admission, patient age in years, sex, Charlson Comorbidity Index (CCI) and Index of Multiple Deprivation (IMD) quintile for the patient’s LSOA residence. There were 32,844 LSOAs in England in 2011 each with a population of between 1,000 and 3,000 people.
Data Management and Statistical Analyses
Data were analysed using standard statistical software: Microsoft Excel (Microsoft Corp, Redmond, WA, USA), Stata (Stata Corp LLC, College Station, TX, USA) and Alteryx (Alteryx Inc, Irvine, CA, USA).
Age was non-normally distributed on visual inspection, with a bimodal appearance, with peaks at 50-54 years and 68-72 years and a left skew. Thus, age data were summarised using the median and inter-quartile range (IQR). All other data were categorical and were summarised using frequency and percentage. Data were aggregated at an ICB rather than a trust level when considering variation across organisations. This was due to a large number of injections that were funded by the NHS being delivered by independent sector providers and skewing the data. Since ICBs were defined by the patient’s residence, reporting by ICB is more meaningful.
When comparisons of the data were made between financial years, 2019/20 rather than 2020/21 was used as the final year, due to the fall in patient numbers during 2020/21 as a result of suspending elective surgery during the COVID-19 pandemic.
Funnel plots are presented for the variation in subsequent injections per 100,000 of the ICB background population. Given the rarity of subsequent injection in the background population, control limits are calculated based on the assumptions of a Poisson distribution.
Results
The data extraction process is summarised in Supplementary material Figure S1. Prior to exclusion of patients with a recorded body site other than lumbar, a dataset of 167,313 patients were identified. Exclusion of 33,064 (19.8%) patients with a non-lumbar body site gave a final dataset of 134,249 patients who underwent a first lumbar FJI/MBB during the study period. Of these, 118,479 (88.3%) had a lumbar body site recorded and 15,770 (11.7%) had no body site recorded.
A total of 8,370 patients had a repeat injection (two injections in total) within 180 days and 2,678 patients had two repeat injections (three injections in total) within one year; 2,126 (79.4%) of those with three injections within one year had their second injection within 180 days and so appeared in both groups. Therefore, 8,922 (6.6%) patients had either two injections within 180 days or three injections within one year. An additional 13,217 (9.8%) patients had a subsequent injection between 181 days and one year but did not have a third injection within one year and so did not meet the exposure of interest criteria.
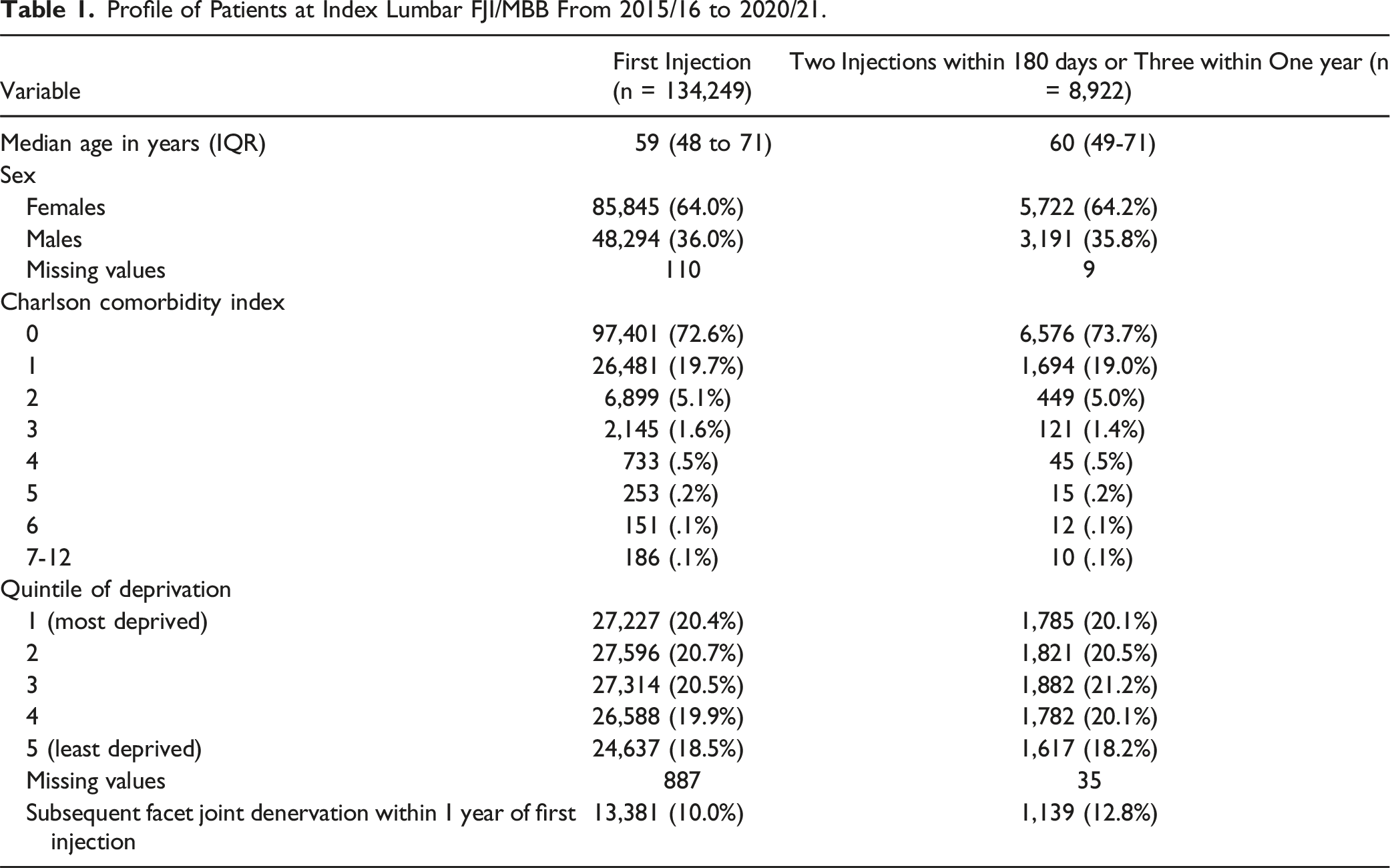
Profile of Patients at Index Lumbar FJI/MBB From 2015/16 to 2020/21.
Change in Proportion of Patients and Outcomes Over the Six-Year Study Period.
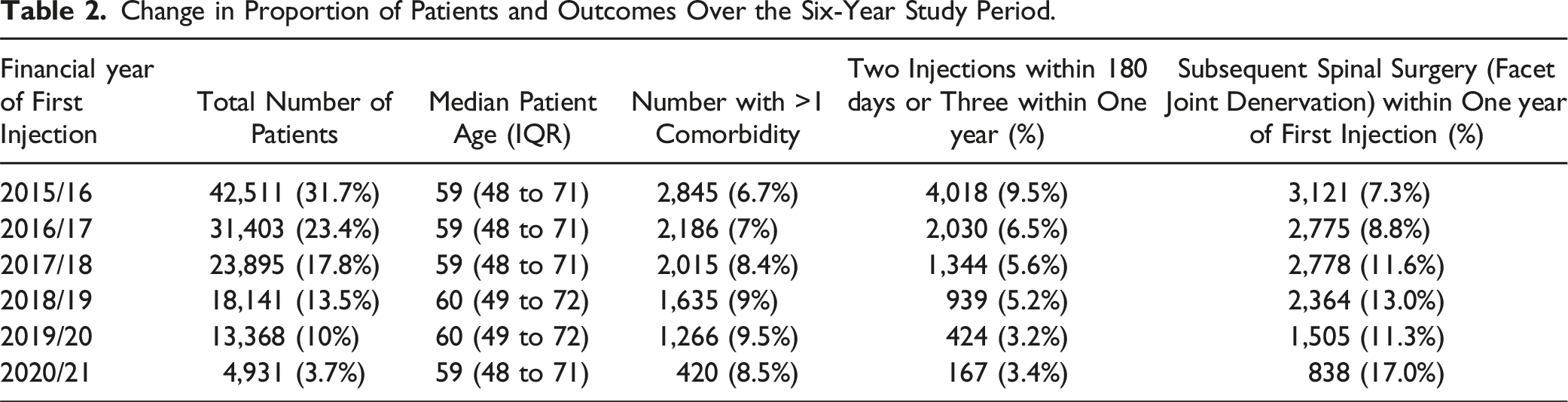
The number of first injections fell substantially over the study period; by 2019/20 the number of first injections was only 31.4% of that in 2015/16. There was a very large proportional fall in patient numbers from 2019/20 to 2020/21 (36.9%), with numbers likely influenced by the COVID-19 pandemic. The number of first injections was 10,341 for 2021/22 (see Supplementary material Figure S2), an increase of activity from 2020/21, but continuing the longer-term downward trend relative to earlier years. The fall in the absolute number of patients with a repeat injection was greater than the fall in first injections: 10.6% of the 2015/16 total by 2019/20. Although median age was consistent over the study period the proportion of facet joint denervations performed within one year increased steadily.
The procedures were performed across all 42 ICBs in England and the number of patients with a first and repeat FJI/MBB per 100,000 background population for each ICB in 2015/16 and 2019/20 are shown in Figures 1 and 2 respectively. Number of first injections per 100,000 population for each Integrated Care Board in England for 2015/16 and 2019/20 (Integrated Care Boards anonymised for confidentiality). Number of patients with a repeat injection per 100,000 population for each Integrated Care Board in England for 2015/16 and 2019/20 (Integrated Care Boards anonymised for confidentiality).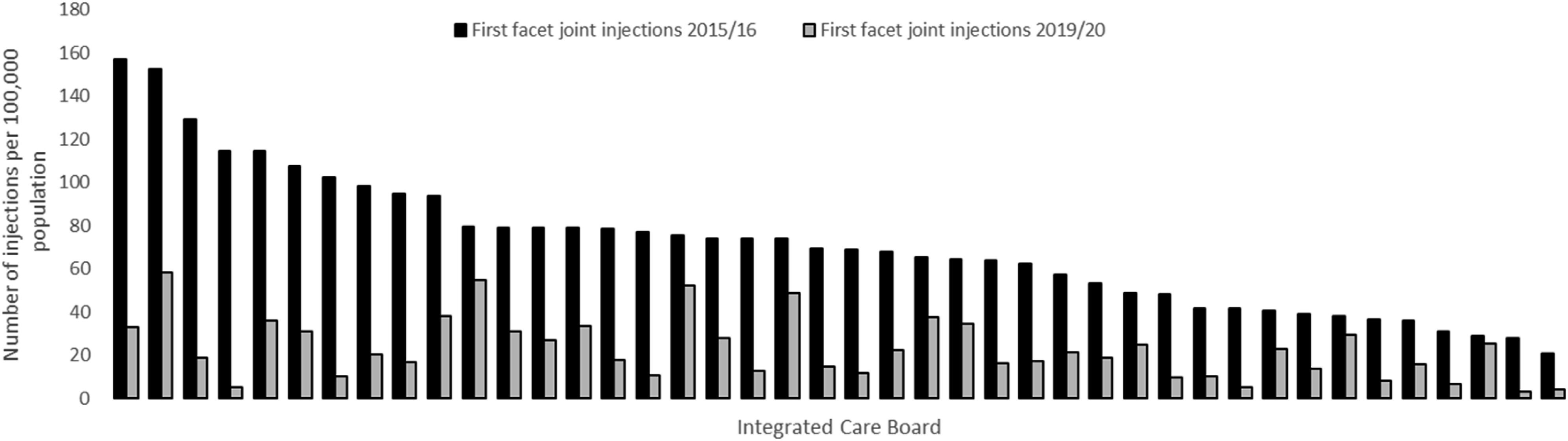
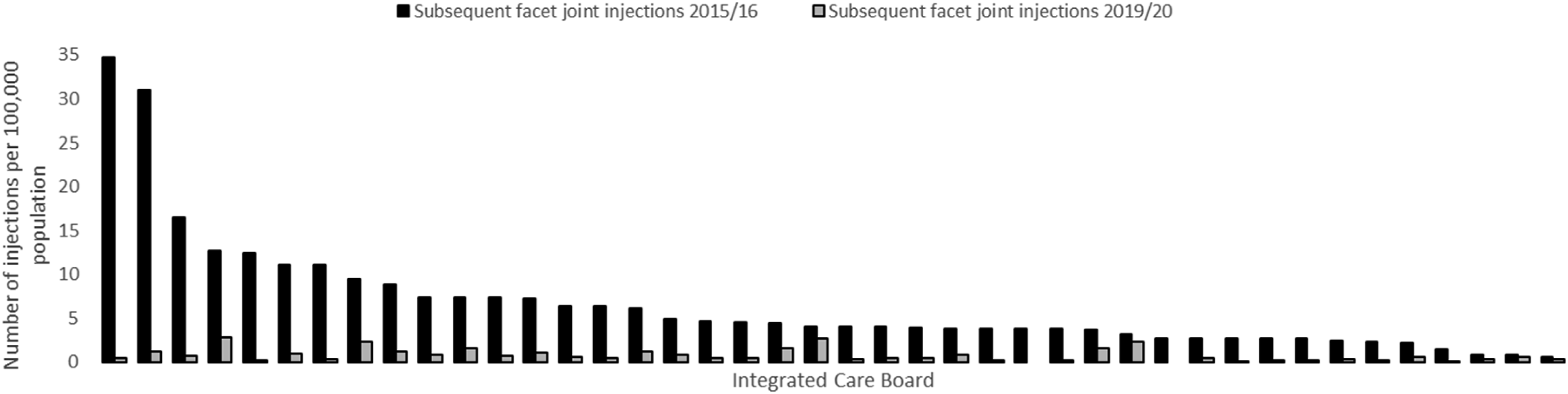
There was substantial variation in the number of first spinal injections per head of population across ICBs in 2015/16, from 157.4 to 20.9 per 100,000. Repeat injection rates per 100,000 population varied from 34.8 to .6 in 2015/16. All ICBs had a fall in the number of patients with a first and repeat injection from 2015/16 to 2019/20. In 2019/20, two ICBs performed no repeat injections and only eight ICBs performed repeat injections on more than 20 patients in the specified time frame. The number of subsequent injections per 100,000 background population for each ICB during 2015/16 and 2019/20 are presented as funnel plots in Supplementary material Figure S3 and Figure S4 respectively. Although some datapoints fall above the control limits during 2019/20, those that do are much closer to the control limits than was seen during 2015/16.
Carbon Footprint and Financial Costs of Injections for Each Financial Year.
Discussion
Our study provides evidence of a sustained reduction in the use of lumbar FJI/MBB in England over the study period, with a particularly dramatic fall in the use of repeat spinal injections. The observed changes also had a positive impact on both the financial costs to the NHS and the carbon footprint associated with FJI/MBB.
The recommendations from the NBPRP Pathway and NICE appear to be being followed, although the practice of repeat injections has not completely stopped. The NBPRP pathway encourages patients to rely less on medical management of their pain and use other treatments including combined psychological and physical rehabilitation which includes physiotherapy and behavioural therapy. Encouraging a less medicalised treatment pathway could result in a reduced incidence of back pain due to better patient education and release clinicians to participate in activities that are more effective.
Around two-thirds of patients were female, and the average patient was of working age, consistent with the profile of people reporting low back pain globally. 1 The vast majority of patients were free of comorbidity. Although the number of patients receiving a first FJI/MBB fell substantially over the study period, their age and comorbidity profile changed little. However, there was a proportional increase in use of denervation surgery over time, suggesting that those still receiving FJI/MBB were those most likely to require surgical intervention. It is also possible that the use of facet joint denervation has increased over the study period as a result of this change in practice. We do not present data to support or refute this possibility, although further investigation of change in practice due to the changes reported here is merited.
As we get closer to 2040 when the NHS is aiming to achieve net zero emissions, it is imperative that all procedures are assessed for their sustainability credentials as well as their clinical and cost effectiveness. We calculated a potential carbon reduction related to FJI/MBB of nearly 3 kilotons CO2e but this value could have been even higher if the guidance had been followed from 2015/16 onwards which would have been a positive step for the NHS and the planet.
The reduction in injections performed over the study period resulted in a saving of £19.7 million when the 2019/20 costs were compared to the 2015/16 costs, highlighting that focussing on clinical effectiveness can have financial benefits. Full compliance with the recommendations from the NBPRP, NICE and GIRFT would have resulted in greater financial savings which could have been utilised to fund alternative and more effective treatments for back pain.
Although our data and results are specific to practice in England, reviews of international guidelines for the management of non-specific low back pain from Europe and the United States have come to similar conclusions to those of the NBPRP, NICE and GIRFT in recommending against the use of lumbar FJI/MBB.15-18 Specific carbon and financial costs relating to lumbar FJI/MBB in other countries were not available for comparison but based on our findings, it is reasonable to assume that both would be reduced if the number of procedures performed was also reduced regardless of the nature of the health care funding model used.
Our study has several strengths. We used the most recent HES dataset available to us and accessed data on all initial lumbar FJI/MBB conducted within the NHS in England across a six-year period. As such, we were able to identify repeat injections and subsequent surgery at trusts other than the trust which performed the index injection. Cases included in our dataset should be representative of all NHS adult patients receiving lumbar FJI/MBB in England, and they will be broadly similar to patients in many countries with a similar health care model to the UK.
Our study also has some limitations. Due to our inclusion criteria, we did not include all the subsequent injections that were performed over the study period and as such, we accept that the carbon and financial savings that we have identified are likely to be an underestimation of the true savings that have accrued.
The final year of study for the initial injection, 2020/21, coincided with multiple lockdowns in England due to the COVID-19 pandemic resulting in a reduction in injections that year and subsequent reductions in second and third injections in the following year. As a consequence, we used the year 2019/20 when comparing changes over time. Data for 2020/21 are presented to evaluate the impact of the COVID-19 pandemic and data on first injections for 2021/22 are also presented to assess the degree to which patient numbers rebounded following the restarting of elective services. The higher number of first injections during 2021/22 may partly reflect an attempt to reduce post-pandemic waiting lists. It would be interesting to explore whether the number of FJI/MBB continue to decline in the future.
We acknowledge that the dataset does not include information on the different referral pathways used across England and the lack of detailed data relating to some aspects of clinical presentation also limited the extent to which we could investigate the impact of these important potential confounders. Although the HES database includes data for all patient episodes, some data entry inconsistencies have been noted, mostly with regard to differences in clinical coding practice across trusts.19,20 Data accuracy is also a concern, although there is no ‘gold standard’ dataset against which to compare the criterion validity of HES. Finally, the HES dataset contains only limited data on patient outcomes. Data on patient quality of life and other patient reported outcomes would be valuable, allowing a deeper understanding of how service delivery impacts on patient outcomes and experience.
Conclusions
There has been a reduction in the number of repeated spinal injections performed in England for low back pain and this is in line with the recommendations from NICE and GIRFT. More work to inform, educate and implement the NBPRP pathway is required to sustain this pattern and change back pain management in England for good.
Supplemental Material
Supplemental Material - Trends Over Time in the Use, Carbon Footprint and Costs of Facet Joint Injections and Medial Branch Blocks to Manage Lumbar Pain in England: Retrospective Analysis of an Administrative Dataset
Trends Over Time in the Use, Carbon Footprint and Costs of Facet Joint Injections and Medial Branch Blocks to Manage Lumbar Pain in England: Retrospective Analysis of an Administrative Dataset by Elizabeth Ojelade, Jacob Koris, Maria Van-Hove, William K. Gray, Tim W. R. Briggs, and Mike Hutton in Global Spine Journal
Footnotes
Acknowledgments
We acknowledge NHS Digital for permission to use their data in this report and the Greener NHS team for invaluable advice and support. We also thank all staff within individual NHS trusts who collected and entered the data used in this study. The study protocol was not pre-registered.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TWRB has received payment for expert testimony as part of medicolegal practice, works for NHS England as the National Director for Clinical Improvement and Elective Recovery, works as Chair of the Getting It Right First Time Programme and is a shareholder in Naitive Technologies Ltd. There are no conflicts of interest from the remaining authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent to Participate
Informed consent was not sought for the present study because it was an analysis of routine clinical data.
Ethical Statement
Data Availability Statement
This report does not contain patient identifiable data. Data in this report are anonymised. The underlying HES data cannot be made available directly by the authors as the data were obtained under licence/data sharing agreement from NHS Digital. HES data are available from NHS Digital upon application. 21
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.