
Abstract
Study Design
prospective multicenter study.
Objectives
Active apex correction (APC) is posterior tethering technique for correction of early onset scoliosis (EOS) via reverse modulation at the apex. Active apex correction has been increasingly used worldwide. This study aimed to assess short-term outcomes of multicenter study with ≥2 years of APC on spine length, curve correction, complications, unplanned surgeries, and proposed low crankshaft phenomena incidence.
Methods
Prospective multicenter study including 24 EOS patients treated by APC; involves inserting and compressing pedicle screws on convex side of apex proximal and distal to most wedged vertebra allowing apex modulation according to Hueter-Volkmann law. Excluded patients with <2 years follow-up whom APC was not primary surgery.
Results
Mean age 85.97 ± 32.43 months, 71% congenital scoliosis, mean follow-up 35.54 ± 12.36 months. At final follow-up, statistically significant improvement in Cobbs angle (∆ = 23.96%, P < .0001), spinal length T1-T12 (∆ = 12.83%, P < .0001), T1-L5 (∆ = 13.41%, P < .0001) but not in apical vertebral translation (AVT) albeit clinical improvement (∆ = 7.9%, P = .36) compared to preoperative measurements. Comparing immediate postoperative measurements to >2 years follow-up, statistically significant improvement in spinal length T1-T12 (∆ = 6.03%, P = .0002) and T1-L5 (∆ = 6.26%, P < .0001) but not in Cobbs angle (∆ = 4.93%, P = .3) or AVT (∆ = 14.77%, P = .25). 9 complications requiring 3 unplanned surgeries recorded in all patients including 2 broken rods, 2 adding-on and 4 screw dislodgement.
Conclusion
Active apex correction is a novel technique that has been incorporated in several countries as treatment modality for EOS. Short-term outcomes are promising in terms of clinical improvement, complication rates and decreased need for multiple operations or unplanned surgeries.
Keywords
Introduction
Early onset scoliosis (EOS) is defined as a deformity in the spine of a growing child that develops before the age of 10 years.1,2 The spinal deformity, regardless of etiology, produces chest wall rotation that obliterates lung space. The treatment of EOS aims to halt and correct deformity while preserving spinal growth and maximizing thoracic volume to allow cardiopulmonary growth and avoid respiratory compromise and cardiac diseases.1-3 Initial treatment consists of non-operative methods (bracing and/or corrective casting) which are used to delay or avoid the need for spinal surgery. However, treatment is challenging in rapidly progressive curves and hence surgical ‘growth-friendly’ corrective techniques is often necessary.1,4,5
Multiple surgical techniques have been devised in aim to maintain a mobile growing spine while preserving lung growth and at the risk of minimal complications. 6 Traditional growing rods (TGR) are the most frequently used technique in EOS management; however, it requires lengthening procedures repeatedly every 6 months and is as such accompanied by higher complication rates and costs.3,7 As a result, several methods have been recently described and introduced to overcome the need of repeated reoperation, including magnetically controlled growing rods (MCGR) and the SHILLA growth guidance system.3,8
SHILLA technique is a one-time posterior based technique controlling the apex through fusion but has 2 major disadvantages: High incidence of loss of correction as a result of the Crankshaft or adding-on, and need for osteotomies, putting screws on the concave side of the curve apex and the potential associated complications.9,10 At 5-year follow-up, McCarthy and his group noticed that 62% of the patients treated with SHILLA developed crank shafting and a shift in the apex of the fused primary curve.
10
Active apex correction (APC) is a modification of the SHILLA technique proposed to overcome the aforementioned disadvantages and is as such deemed desirable.
6
Active apex correction is a hybrid of guided-growth and compression-based philosophies for management of growing-spine deformity. APC replaces the apical fusion of a traditional SHILLA with a unilateral compression applied via pedicle screws on the convex side which halts the growth of the most wedged vertebrae on convex side and allow the ratio of concave-to-convex height to increase overtime, thus reducing the vertebral wedging at the apex of the curve (Figure 1). Biomechanically, it allows for an active compression-based intervention at the apex of the curve in accordance with Hueter-Volkmann law,
11
alongside passively restrained guided-growth height allowance of the entire scoliotic curvature that will decrease the incidence of crank shafting. Active apex correction also avoids the need for pedicle screw fixation on the concave side, thus circumventing the need for risky osteotomies and reducing precious surgical time. Schematic showing key differences in the established SHILLA procedure and the modified APC approach used in this study, used with permission.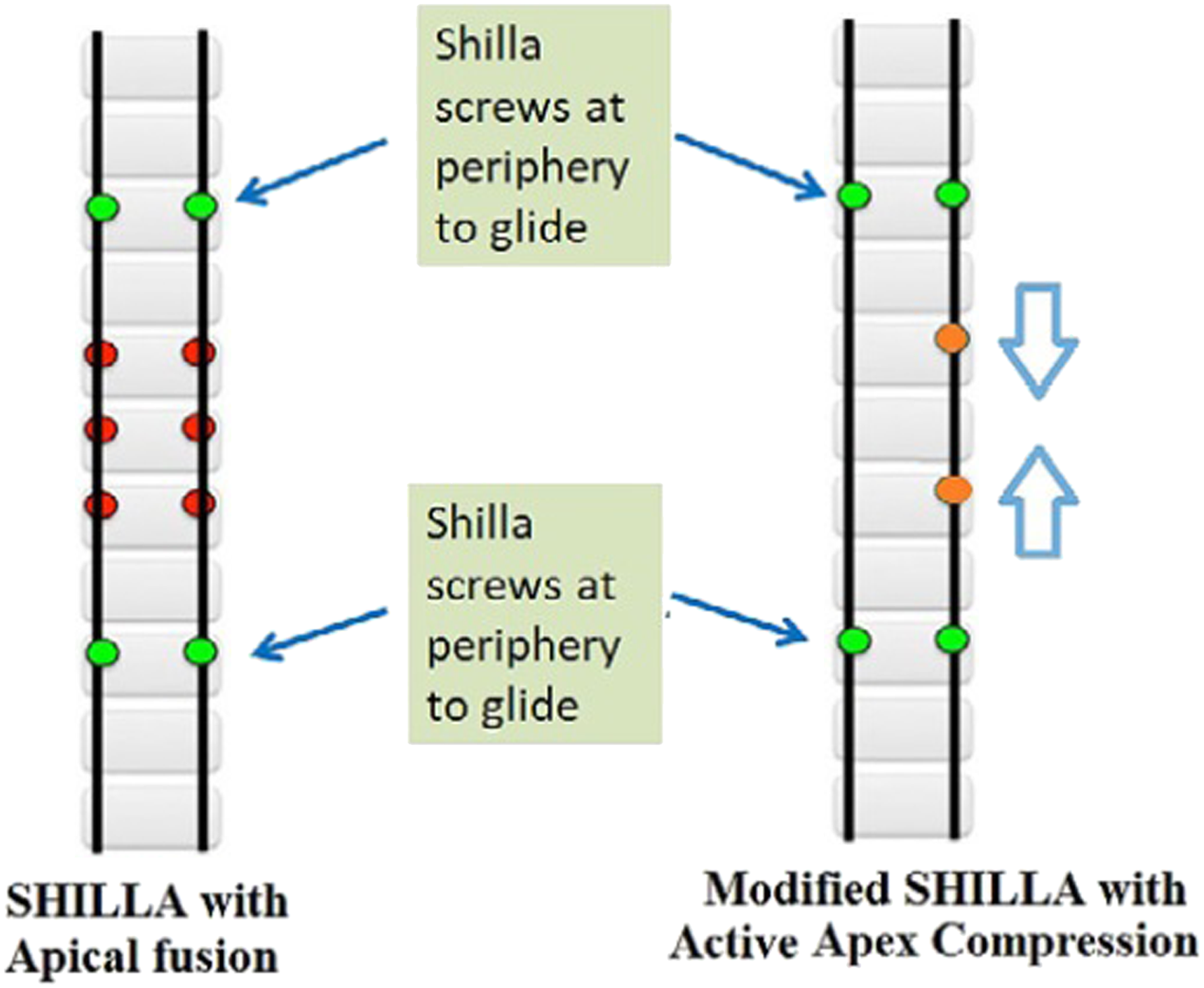
Active apex correction has been increasingly used worldwide in Jordan, Palestine, Egypt, Pakistan, India, Vietnam, Italy, USA among other countries. Few recent studies have been reported on the efficacy of this novel technique on correction of scoliotic curve characteristics on the short-term and the equivalency of the outcomes as compared to other correction methods.9,12 Nonetheless, there exists no procedure with no risks and hence the aim of this multicenter study was to assess the short-term outcomes (≥2 years) following APC on spine length gain, curve correction, complications, unplanned surgeries, and the proposed low incidence of crankshaft phenomena.
Methods
Cohort Demographic and Spinal Parameters at Surgery and at ≥ 2-Year Follow-Up Quantifying the Extent of Deformity and Subsequent Correction.
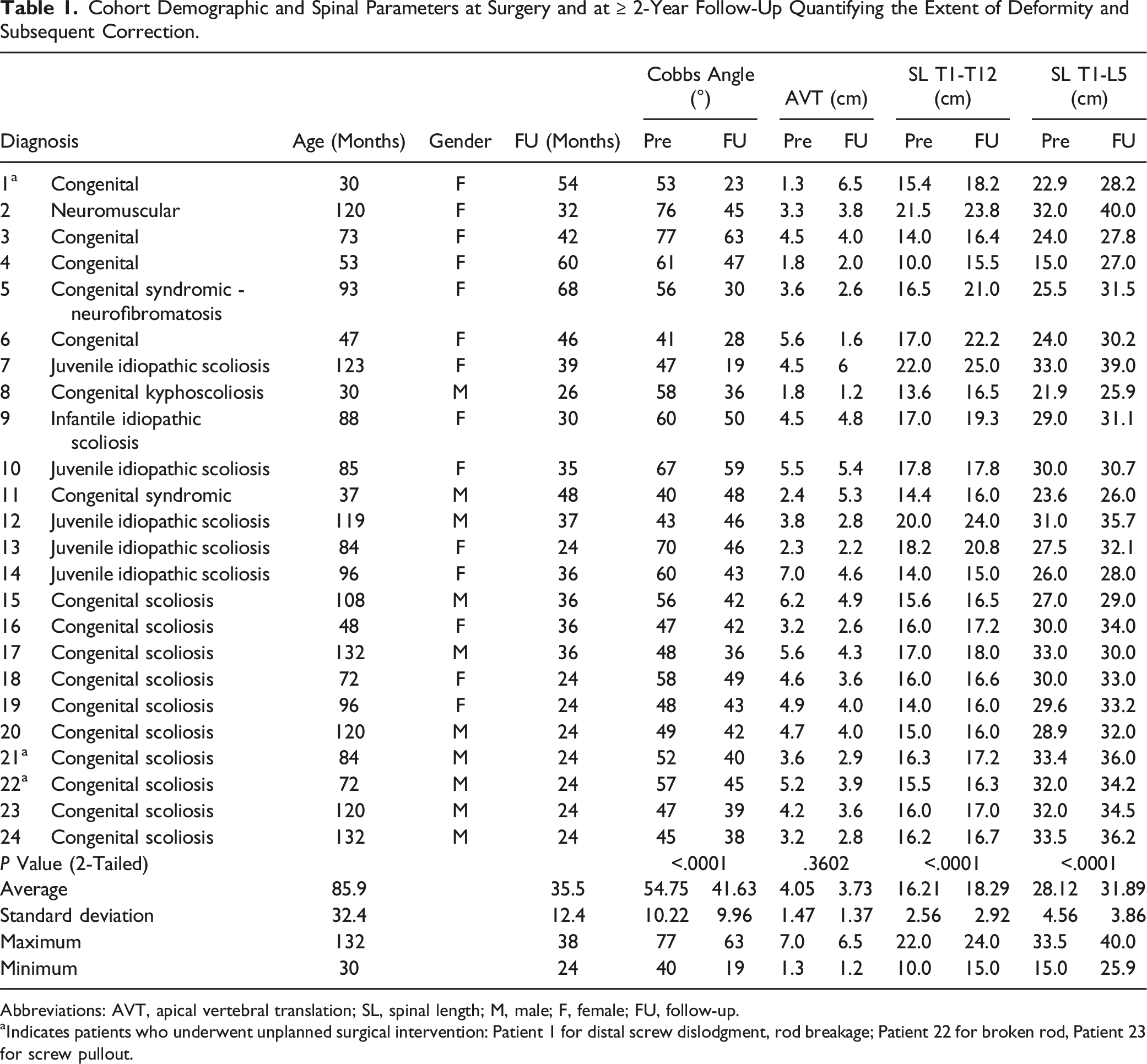
Abbreviations: AVT, apical vertebral translation; SL, spinal length; M, male; F, female; FU, follow-up.
aIndicates patients who underwent unplanned surgical intervention: Patient 1 for distal screw dislodgment, rod breakage; Patient 22 for broken rod, Patient 23 for screw pullout.
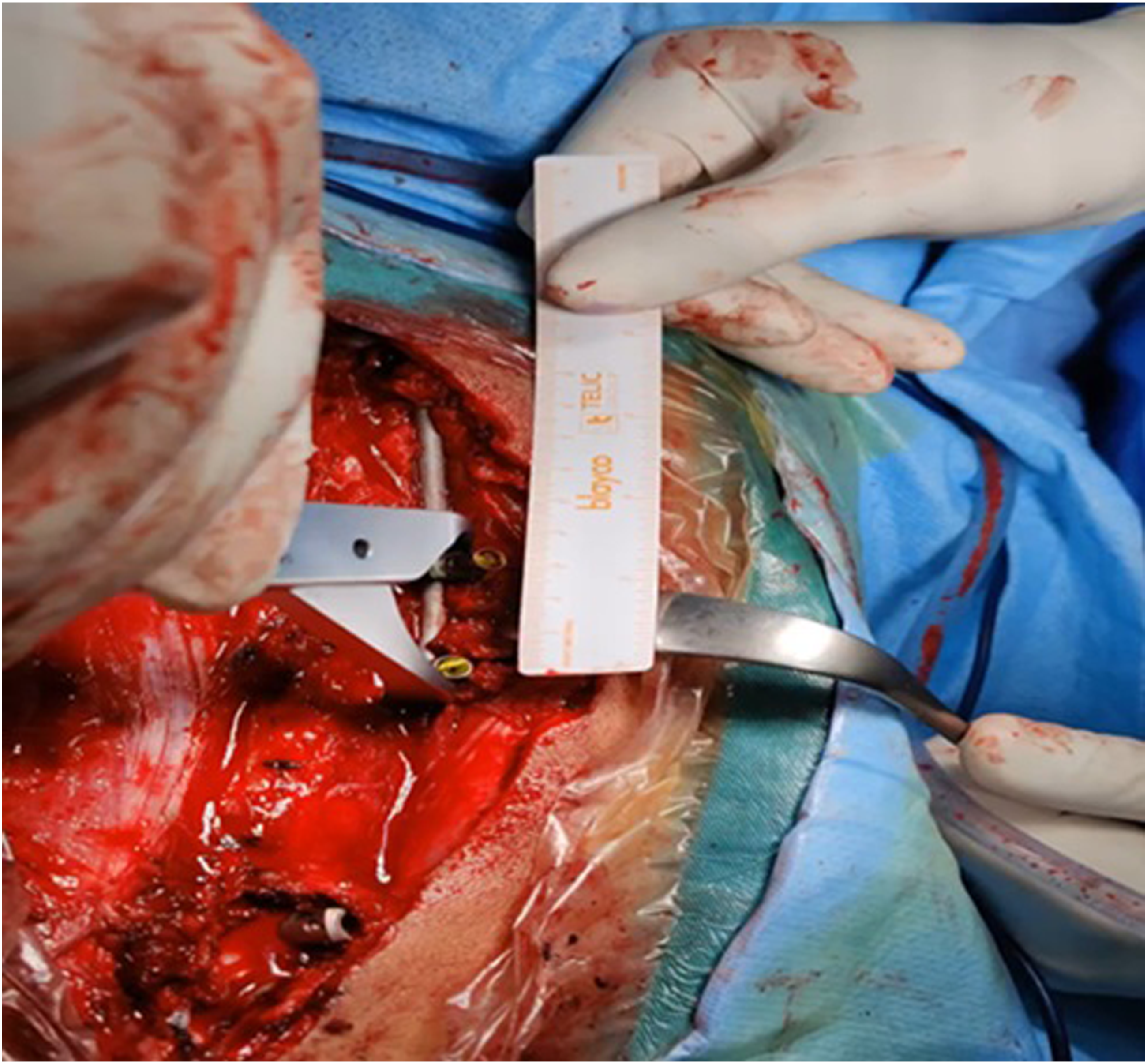
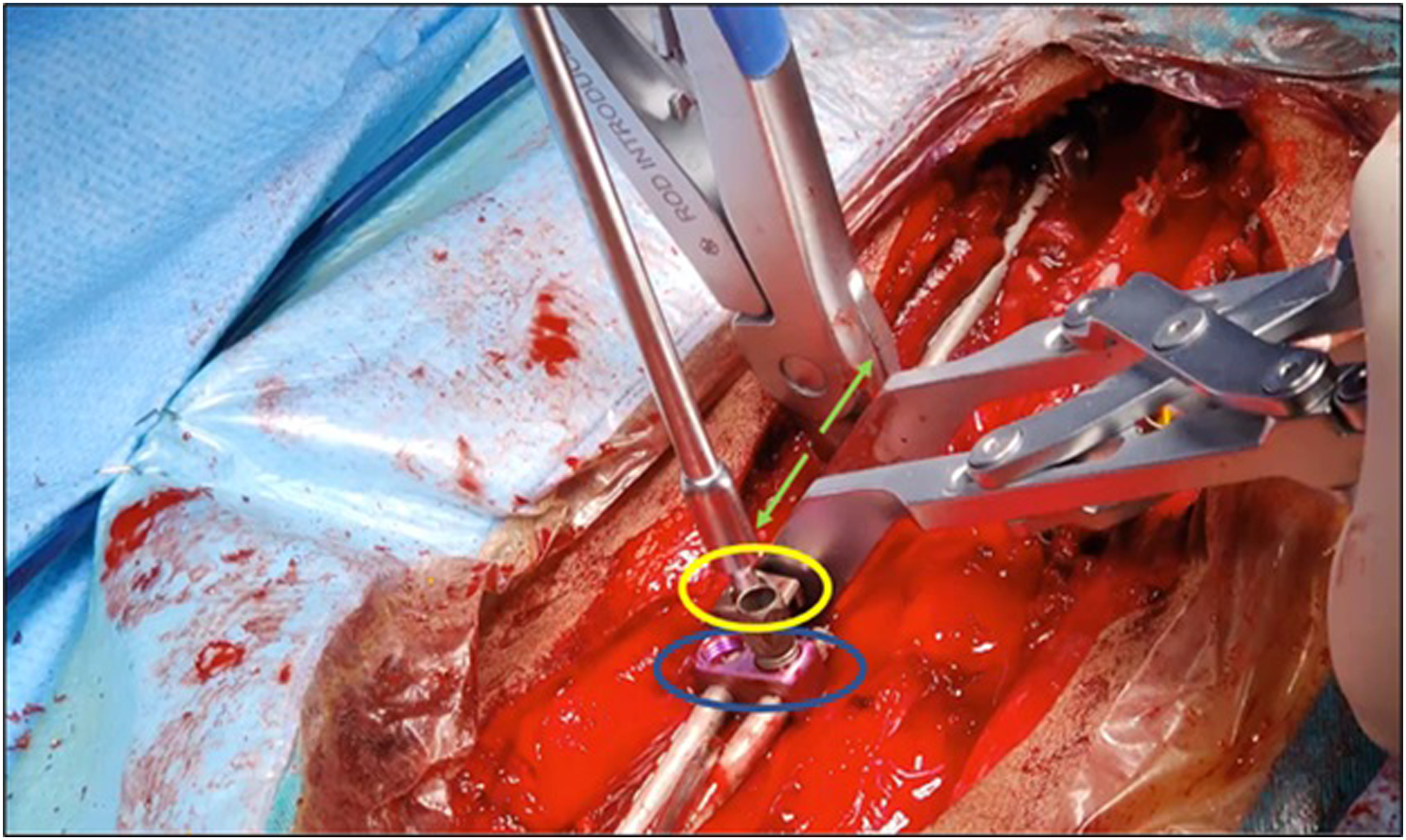
Active apex correction is a modified version of the traditional SHILLA technique (Figure 1). The surgical procedure was performed with the patient in prone position. Extraperiosteal exposure was done for the 2 proximal and distal vertebrae planned for instrumentation and the convex side of the 3 levels at the apex. After putting pedicle screws or hooks proximally and pedicle screws distally, putting tethered pedicle screws on the convex side of the apex one vertebra above and one below the most wedged vertebra (Figure 2). Tethered rod should be 5.5 titanium or 4.75 Cobalt Chrome (CC) connecting the tethered screws, and connecting the tethered rod with the proximal and distal anchors either directly or through dominos. Compression of the tethered screws was done slowly with precautions so as not to dislodge the screws (Figure 3). The connection with the rod connected to proximal or distal anchors by dominos. Dominos need to be locked at the tethered rod level, unlock the other rod for gliding with at least 4 cm to have a potential of 4 years self-gliding. On the concave side, the rods attached to proximal and distal anchors relate to dominos with unlocked one hole for self-gliding (Figure 4). Distraction is to be done with a barrier proximal to the unlocked domino to prevent the gliding rod from gliding backwards. Closure was done after irrigation; no drains were used. All surgeries were performed under intraoperative neuromonitoring and C-arm. Postoperatively, none of the patients used a cast or brace. Intra-operative depiction of the implant construct used in the APC technique. The screws at the tethered levels on the convex side are shown in yellow. Method of measurement of displacement of the tethering screws, quantifying compression done during the APC. Surgical intervention involving distraction on the concave side (green arrows). One part of a cross link (yellow) was added proximal to the unlocked part of the domino (blue). Post distraction, the cross-link piece (which can be replaced with a screw head) is locked to prevent the rod sliding to go proximally.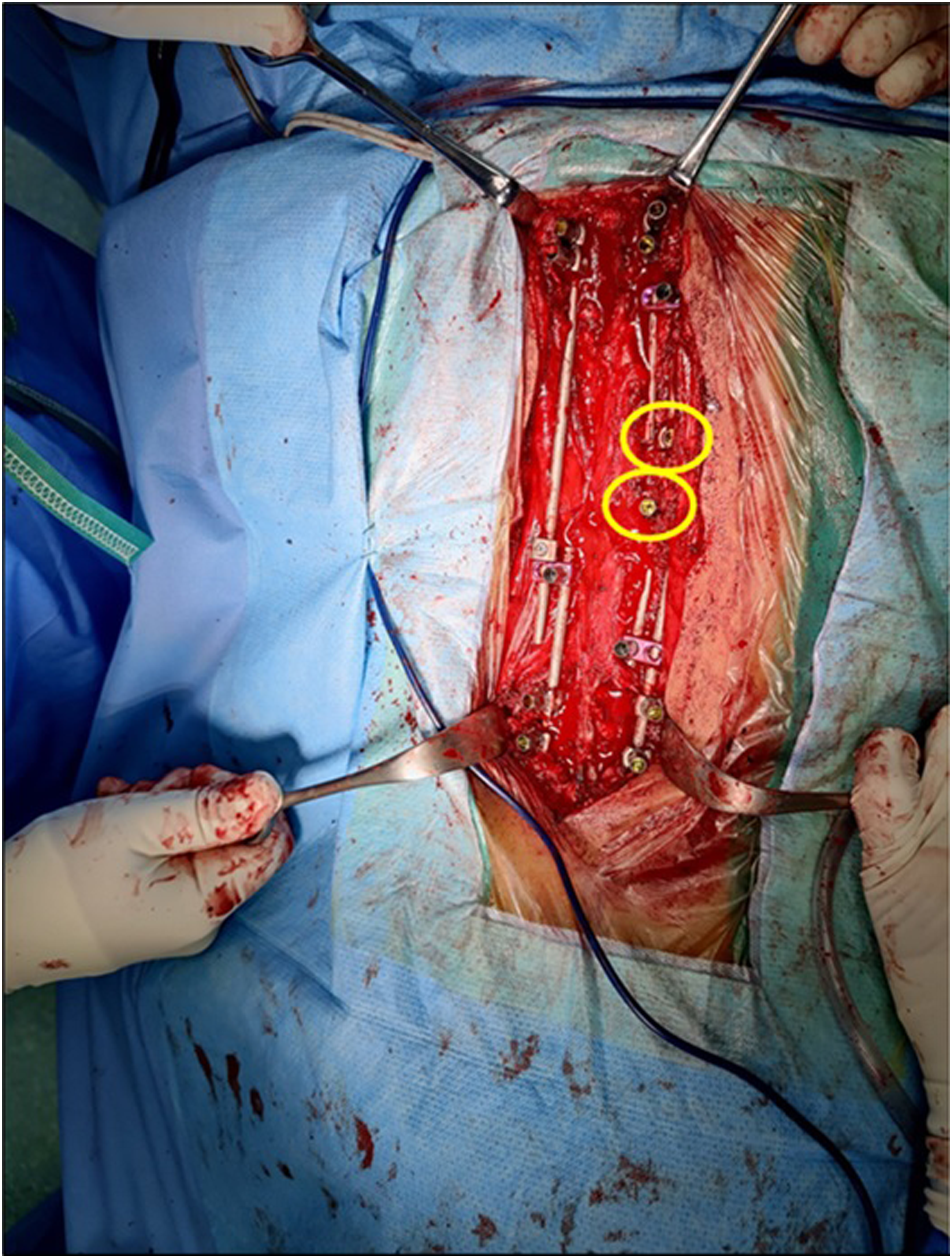
All patients included were followed for a minimum of 24 months. Data on demographics, curve characteristics including Cobbs angle, apical vertebral translation (AVT), spinal length T1-T12 and T1-L5 were recorded at presentation and at follow-up using computed tomography (Figure 5). The curve Cobbs angle was measured in the coronal view from the superior vertebra to inferior endplate of an inferior vertebra. Apical vertebral translation was measured as the distance between center of thoracic (or lumbar) apical vertebra and the C7 plumb line (or central sacral vertical line). Spinal length included T1-T12 and T1-L5 segments spine segments. In addition, data on complications and number of surgeries, planned and unplanned, were also collected. Comparison of Radiographic images at pre-operative (L) and post-operative (R) time points in a patient undergoing APC. The most wedged vertebra (green) seen on pre-operative AP radiograph is used to identify apical region during surgical planning. Post-operative image indicates control of apex via compressive remodulation through screws above and below the most wedged vertebra on the convex side.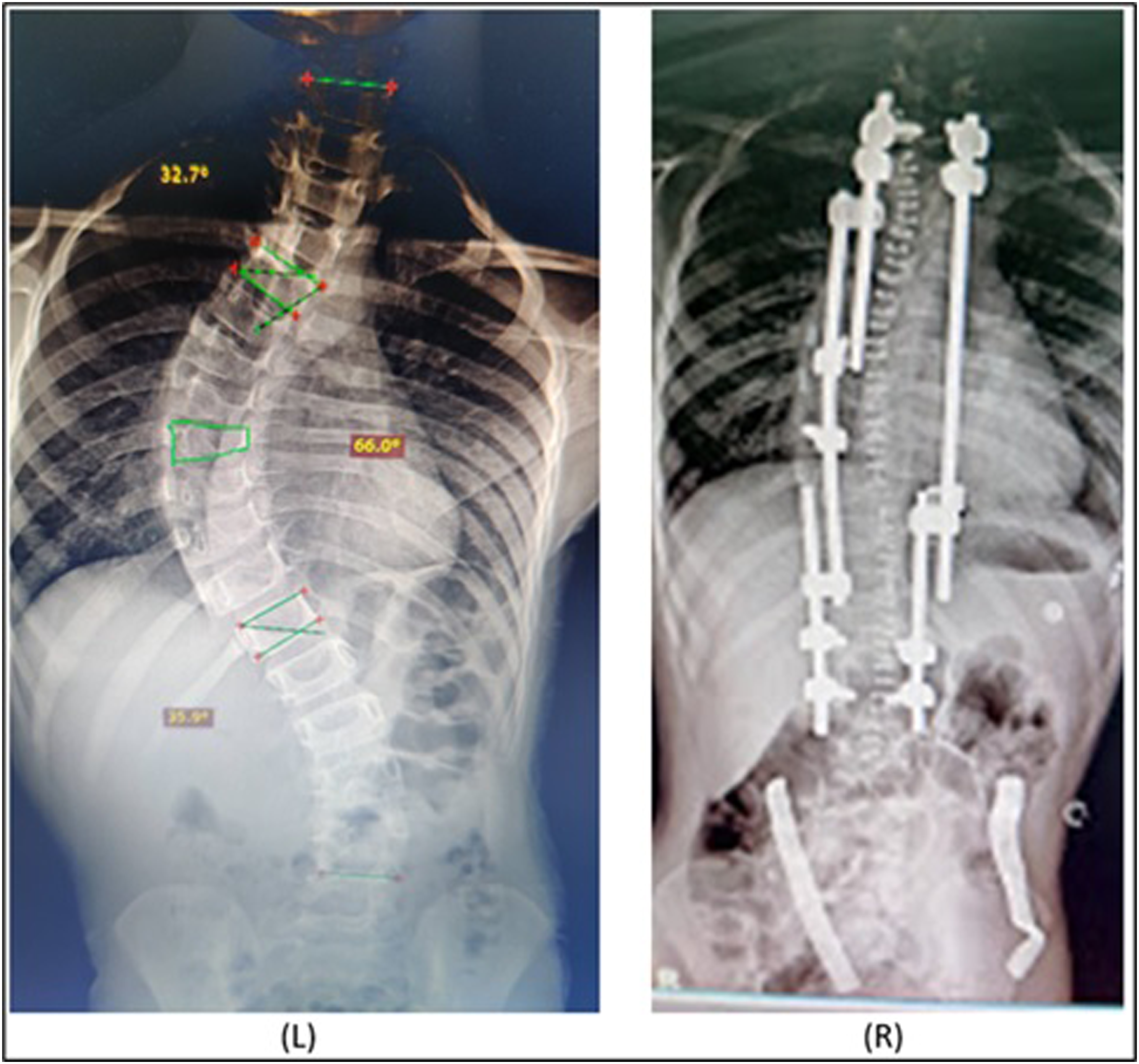
This study was approved by the Institutional Review Board (IRB) at Palestine Polytechnic University (number: KA/41/2023). There were no new implants to be inserted that needed an informed consent, as such it was deemed exempt from this requirement. Data was analyzed using Microsoft Excel. A general descriptive analysis of the data was initially performed. Continuous data were reported as mean and standard deviation (SD). Categorical variables were reported as absolute numbers and percentages. Paired t-tests were used to analyze the magnitude of change between preoperative and postoperative states. Results with P < .05 were considered statistically significant.
Results
The study included 24 patients with EOS treated by APC as an index surgery and followed up for a minimum of 2-year; mean follow-up time was 35.54 ± 12.36 months. Mean age was 85.97 ± 32.43 months with 17 (71%) classified as congenital scoliosis. Cohort data are represented in Table 1.
Percentage of Change in Curve Characteristics at Preop, and at Minimum of 2 Years Follow-Up Post Active Apex Correction.
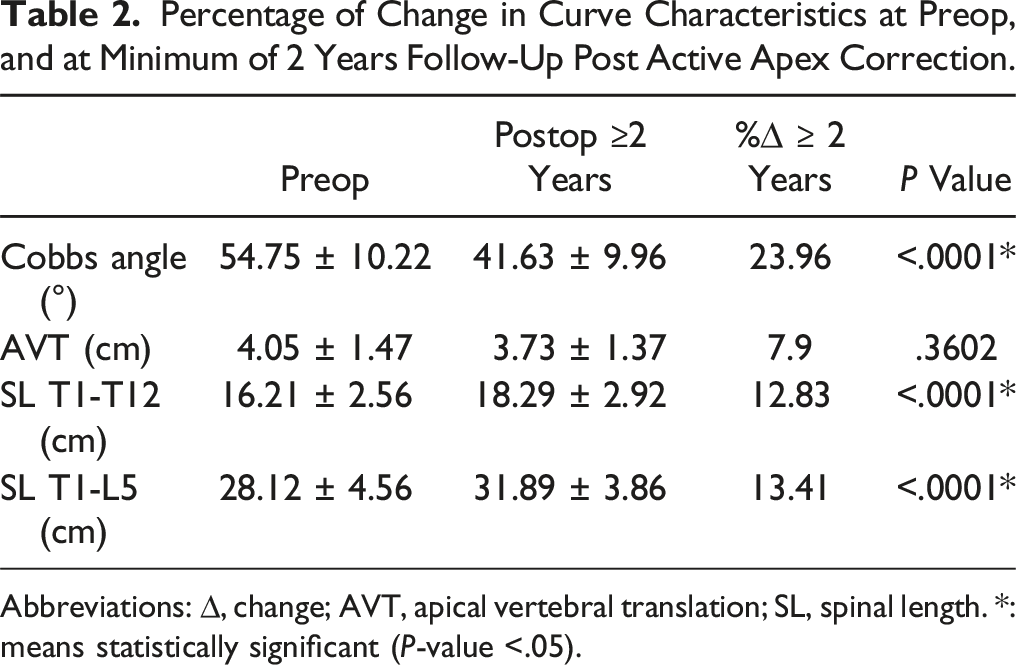
Abbreviations: ∆, change; AVT, apical vertebral translation; SL, spinal length. *: means statistically significant (P-value <.05).
Percentage of Change in Curve Characteristics at Initial Follow-Up and at Minimum of 2 Years Follow-Up Post Active Apex Correction.
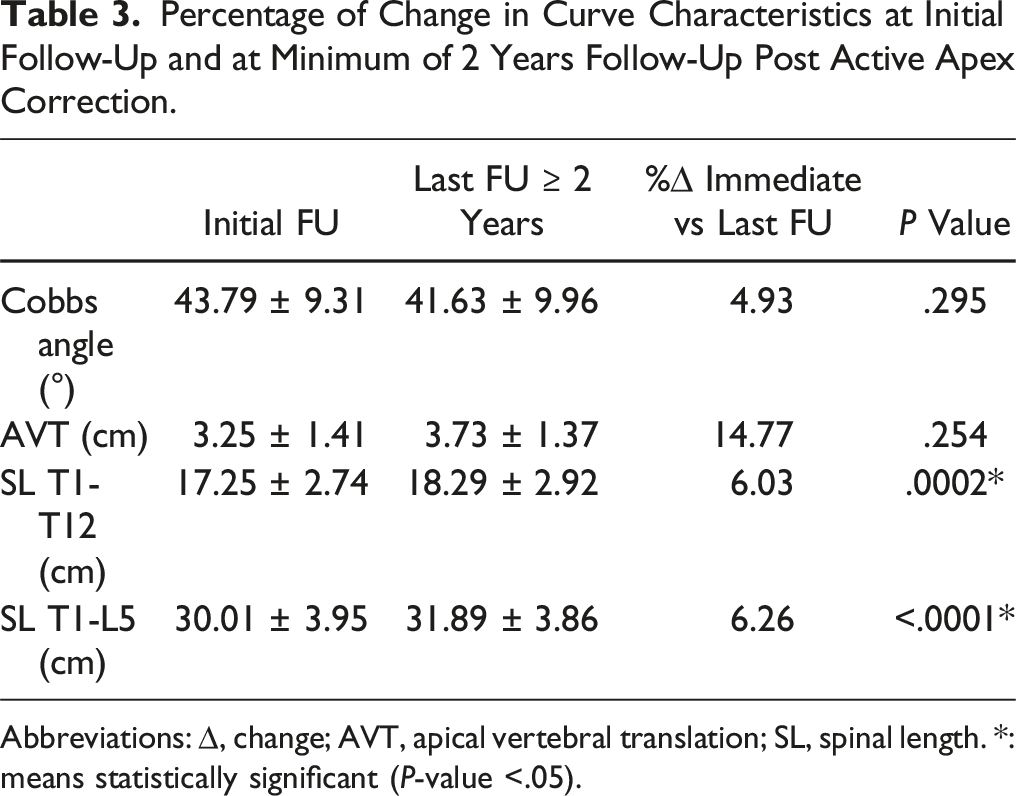
Abbreviations: ∆, change; AVT, apical vertebral translation; SL, spinal length. *: means statistically significant (P-value <.05).
Biomechanical Complications.
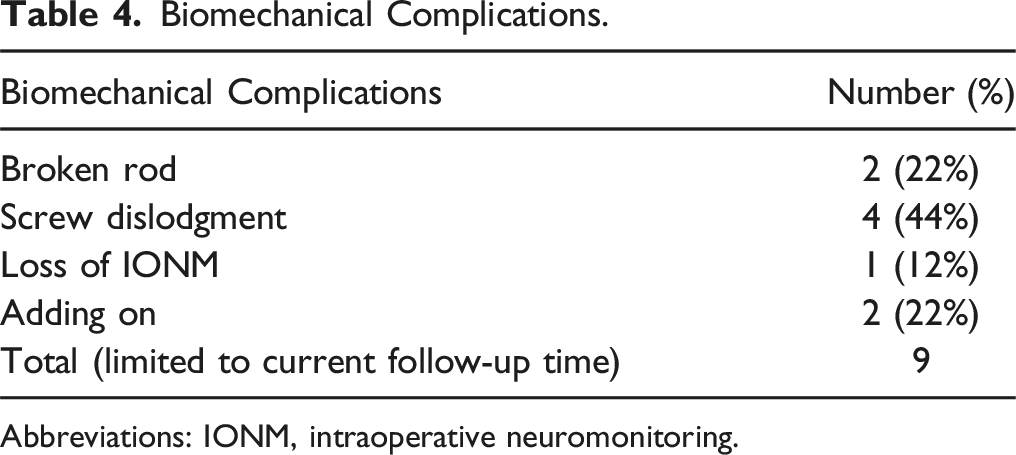
Abbreviations: IONM, intraoperative neuromonitoring.
Subgroup Analysis Based on Etiology of Scoliosis: Percentage of Change in Curve Characteristics at Minimum of 2 Years Follow-Up Post Active Apex Correction Compared to Preoperative and to Initial Follow-Up.
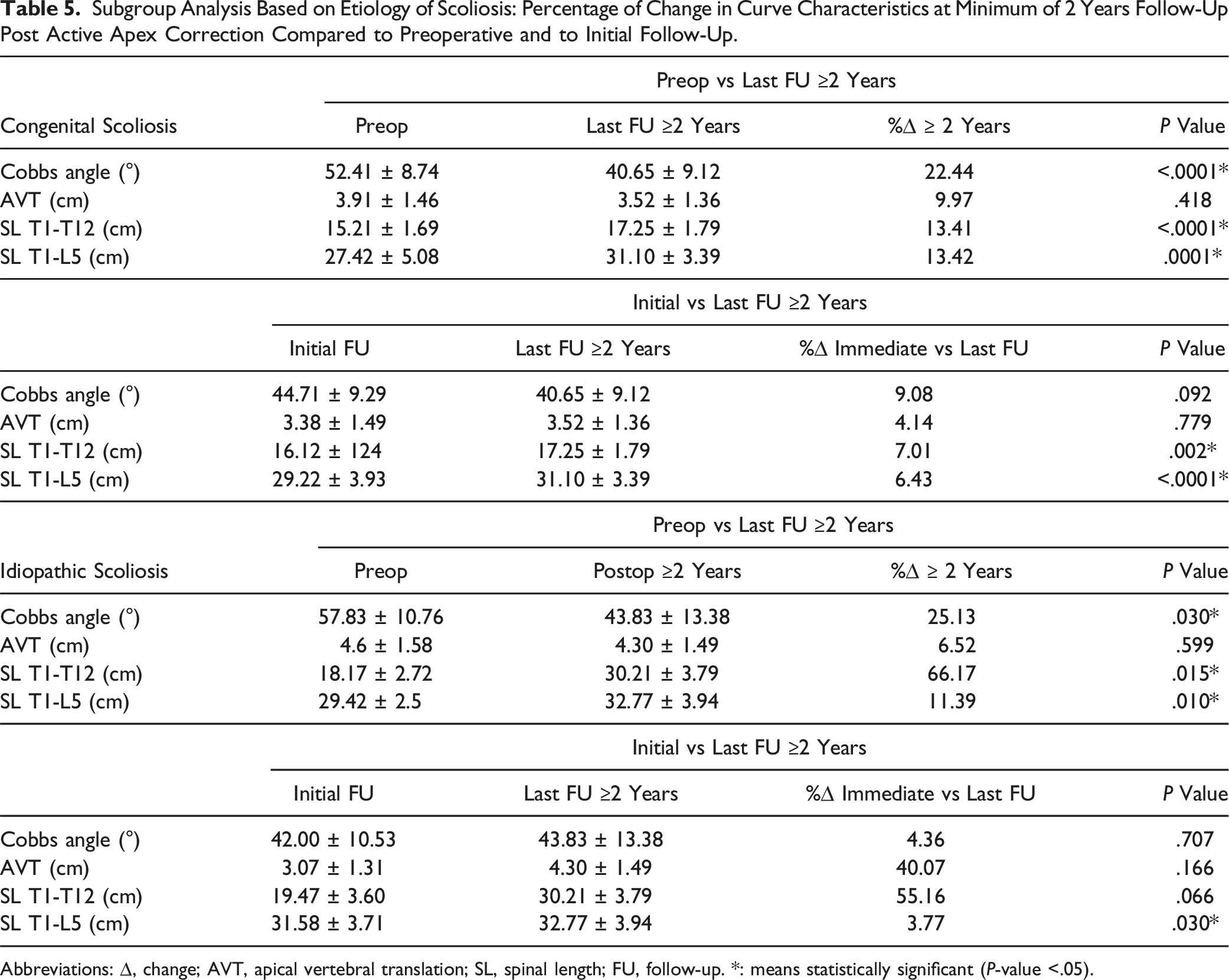
Abbreviations: ∆, change; AVT, apical vertebral translation; SL, spinal length; FU, follow-up. *: means statistically significant (P-value <.05).
Subgroup Analysis Based on Cobbs Angle: Percentage of Change in Curve Characteristics at Minimum of 2 Years Follow-Up Post Active Apex Correction Compared to Preoperative and to Initial Follow-Up.
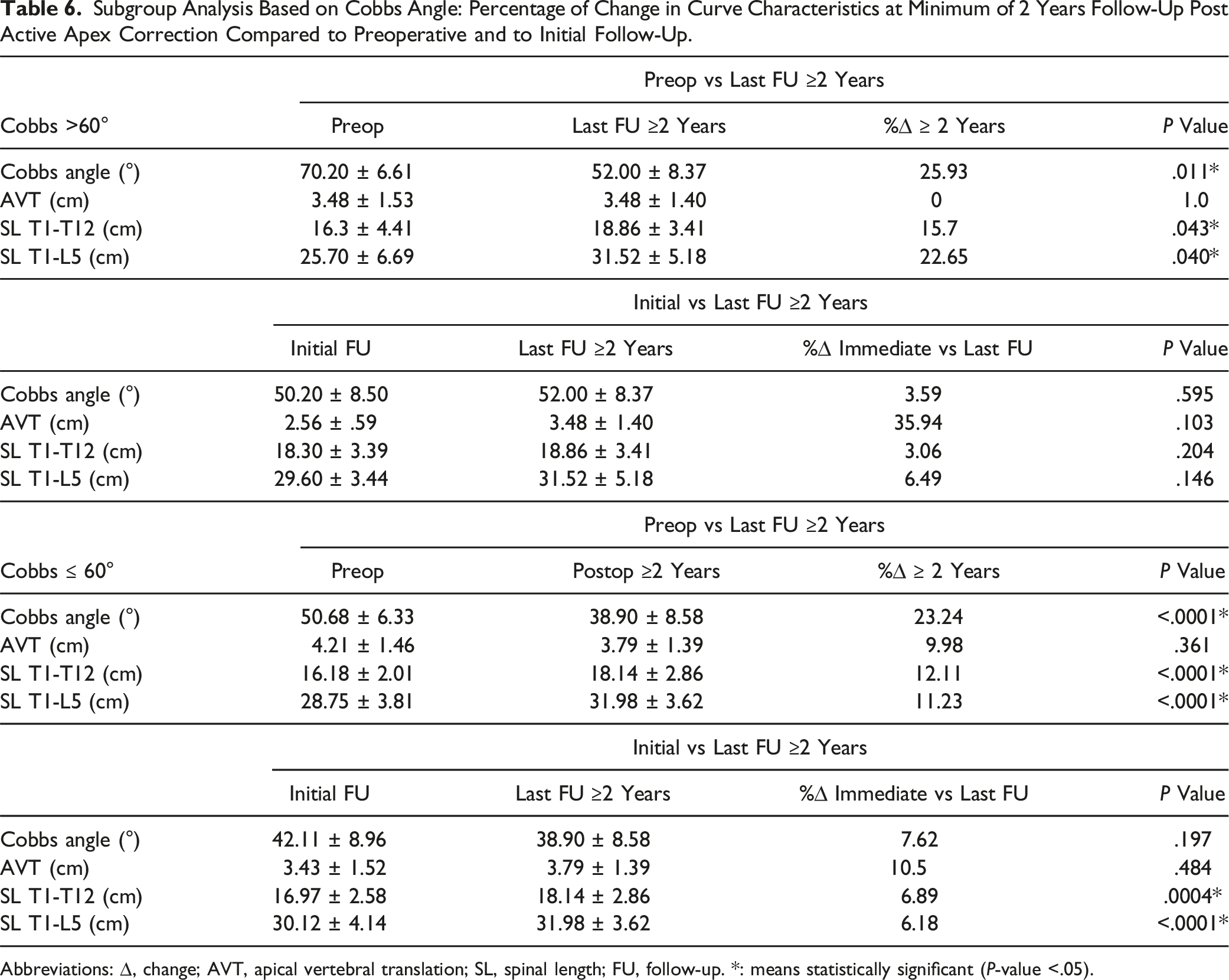
Abbreviations: ∆, change; AVT, apical vertebral translation; SL, spinal length; FU, follow-up. *: means statistically significant (P-value <.05).
Discussion
Early onset scoliosis, as defined by Scoliosis Research Society, includes children <10 years of age having spinal deformities which according to etiology can be classified into congenital, neuromuscular and idiopathic. 6 The spine serves the role of maintaining posture, facilitating rotation and movement. As such, a disturbance of the curvature results in compromise of the spine morphology and its role in daily activities, and when it happens at a young age result in obliteration of space available for cardiopulmonary growth. 13 Hence the management of EOS, in contrary to adolescent idiopathic scoliosis, is considered lifesaving and can vary from bracing and casting as conservative measures to various surgical interventions.
As the curve progresses beyond 40° and conservative approaches fail to maintain a decent life, EOS patients are advised to seek surgery to improve life quality and expectancy. Initially posterior fusion with maximal correction was the treatment of choice for spine deformity. However, spinal growth restriction and lung growth restrictions resulted in high morbidity that led to a transition towards spine growth preservation techniques that aim to correct deformity, preserve growth and mobility at a low complication rate. 6 The difficulties of dealing with EOS patients include heterogenicity, associated comorbidities, higher complications than idiopathic spine deformity, the multidisciplinary approach, and the expenses of the implants.
TGR is distraction-based system popularized by Akbarnia that corrects the curve by frequent distractions every 6 months but the main disadvantages include planned and unplanned operations associated with recurrent anesthesia, increased risk of wound complications and infection in addition to financial burdens.14,15 MAGEC is similar to TGR in theory but the distractions are done transcutaneously every few months; the main drawbacks are high cost of the operation and equipment needed, possible mechanical complications and unplanned surgeries, and metallosis.16,17 SHILLA was developed by McCarthy as guided growth-based technique to control apex of curve as to guide spinal growth and to decrease the number of frequent reoperations. It is done by correction and fusion of 3-4 levels around the apical vertebra with proximal and distal sliding of the rods guiding growth. 6 This technique was found to be accompanied by an increased risk of unplanned surgeries from loss of correction secondary to crank shafting, adding on, screw pull-out and rod breakage and complications associated with osteotomies performed on the concave side of the curve.10,18,19 Henceforth, a modification of SHILLA was needed in effort to overcome the latter disadvantages.
APC technique was developed 13 years ago and has recently gained international attention. It is sought to dynamically modify the apex of the curve via reverse modulation by placing screws posteriorly in a tethering fashion above and below the most wedged vertebra with compression on the convex side. The immediate benefit of APC as a modification of the SHILLA technique is the avoidance of risky osteotomies, inserting screws on the concave side of the apex, that in addition to being more economical for underprivileged patients especially in low- and middle-income countries by having more choices to use implants from different companies since there is no specific implant or instrument that would be needed beside regular ones. Using 2 screws in the apex instead of 6 make the surgery easier, less costly, and less risky. It is preferable to assess the pedicles by CT scan to put the appropriate screw in the apex which is usually from 4-5.5 screws (the rod is always 4.75 CC or 5.5 tetanium) with the length to get at least 80% of the body to get the best purchase. We try to put the screw through Wiltse technique with extraperiosteal exposure avoiding as possible the soft tissue disruption and increase the non-fusion process, with apex correction through compression, rotation, medial translation, which will go with the geometry of the corrected spine, reducing the stress discontinuity and avoiding a junctional area between the apex and the non-instrumented spine above and below, which might be the main reason for the decreased incidence of crankshaft phenomena, rod fracture, beside the good correction post operatively. The long-term benefit hypothesizes that the main concept of controlling the apex through modulation, rather than fusion, would preserve spinal growth including the apex unlike stopping the growth by fusing the apex posteriorly with continuous growth anteriorly which will increase the possibility of the Crankshaft and implant related complications. The radiographs in Figure 6 clearly show sliding of the rods due to guided growth which is seen through the position of proximal rods with respect to screw and rib-hooks at 1 year following APC. Comparison of Radiographic images at post-operative (L) and 1-year follow-up (R) time points in a patient undergoing APC. Position of proximal rods with respect to screw(red) and rib-hook (yellow) indicate sliding of rods due to guided-growth.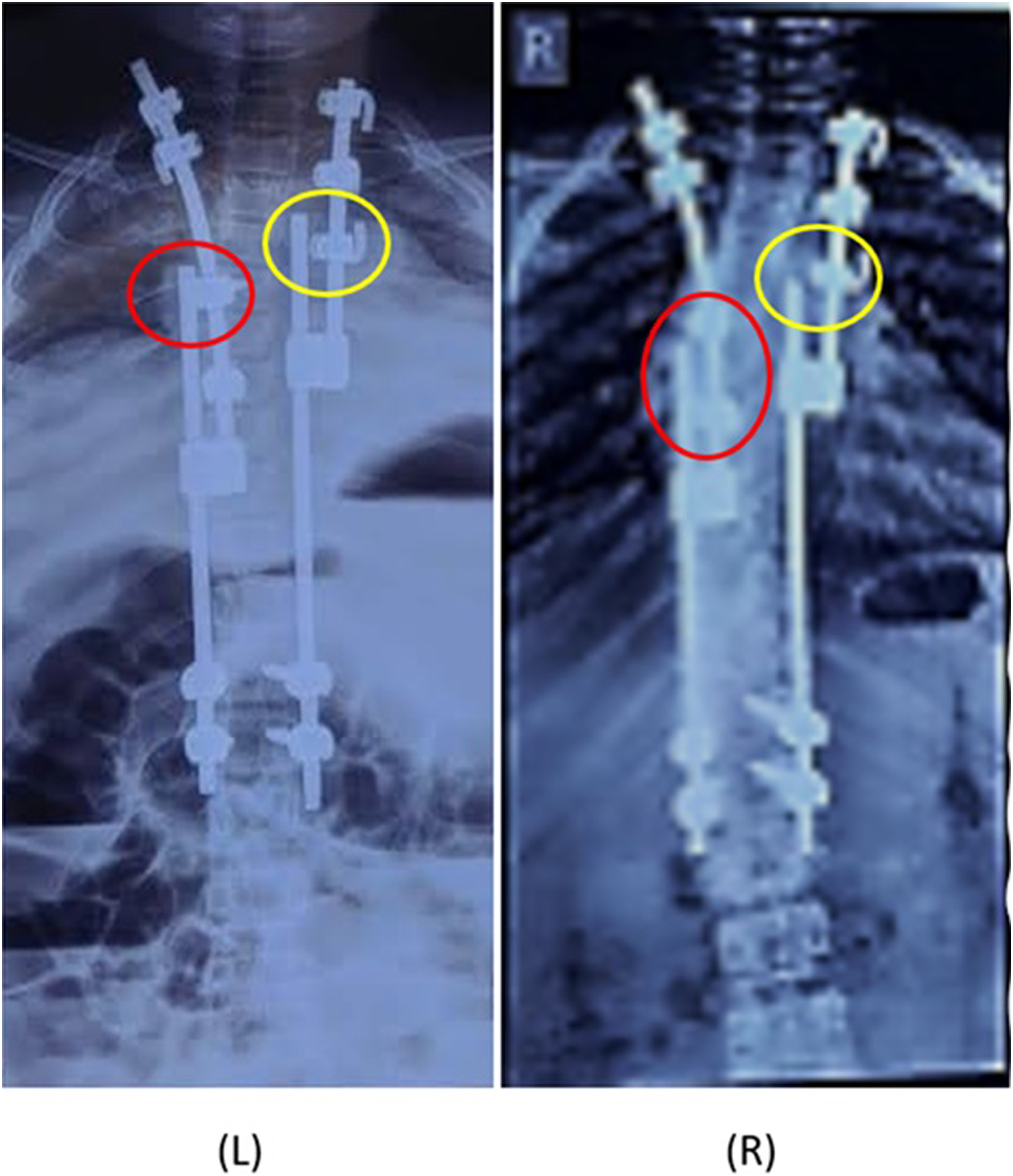
This is the first multicenter study presenting the 2-year outcomes of surgical correction of early onset scoliosis primarily using active apex correction technique. We found statistically significant improvement in curve characteristics postoperatively when compared to baseline, mainly Cobbs angle, spinal length gain but not apical vertebral translation albeit noticeable clinical improvement. Similarly, when compared to immediate postoperative correction, there was a statistically significant improvement in spinal length gain as well, but not apical vertebral translation or Cobbs angle. At ≥2 years post-APC, the study at hand found decrease in Cobbs angle (54.75° ± 10.22° to 43.79° ± 9.31° immediately to 41.63° ± 9.96° at final follow-up) and increase in spinal length from T1-T12 (16.21 ± 2.56 cm to 17.25 ± 2.74 cm to 18.29 ± 2.92 cm at final follow-up) and T1-L5 (28.12 ± 4.56 cm to 30.01 ± 3.95 cm to 31.89 ± 3.86 cm at final follow-up) along with radiographic decrease in AVT (4.05 ± 1.47 cm to 3.25 ± 1.41 cm) at immediate follow-up with a mild increase to 3.73 ± 1.37 cm at >2 year follow-up. Further subgroup analysis of etiology of EOS and Cobbs angle, showing improvement in spinal parameters postoperatively indicates that that APC as a method of correction and spinal growth preservation shows promising outcomes at least 2 years post-correction and maintenance of improvements when compared to immediate follow-up. Previous studies have showed that modulation of wedged vertebra was noticed at follow-up with gradual correction of curvature without need of osteotomies or auxiliary anterior approaches.
12
Other studies comparing APC to other established EOS correction technologies found equivalent outcomes. As reported by Dimeglio, the spine grows on an average of 2.2 cm/year during first 5 years which decreases to 1 cm/year between 5 and 10 years of age.6,20 In our study, the spinal height gain was found to be 1.1 ± .49 mm/month which is similar to previously reported spinal length gain for APC (1.2 ± 1.6 mm/month) and TGR (.8 ± .5 mm/month).
12
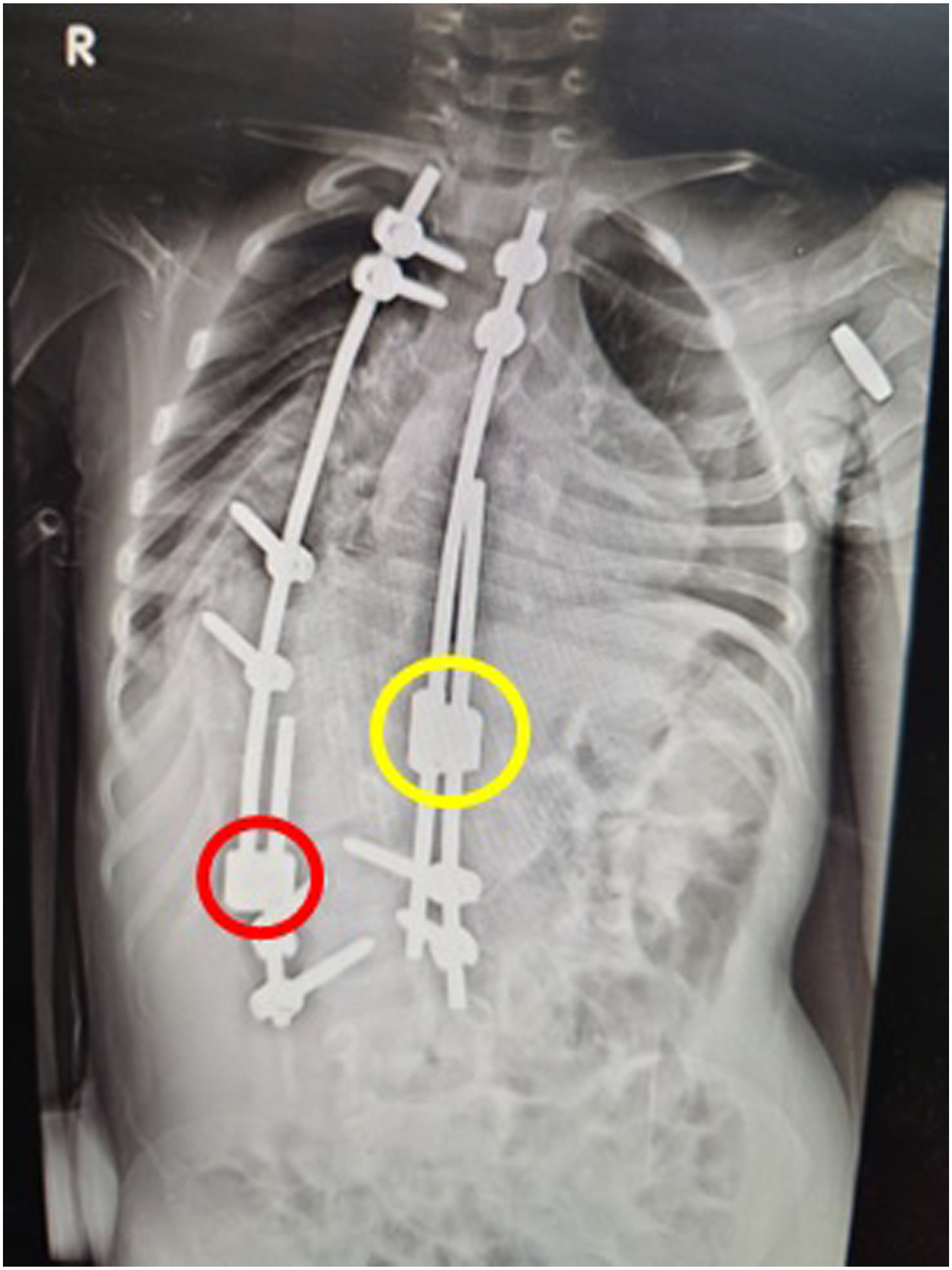
Figures 7-9 show the clinical and radiographic correction of the spine of a 4-year-old boy with syndromic right sided scoliotic deformity using APC technique. A preoperative radiograph (on right) and clinical appearance (on left) of a 4-year-old boy with severe right-sided syndromic scoliotic deformity. Postoperative radiograph showing the treatment of the scoliotic deformity using APC. Yellow/red (concave/convex sides, respectively) circles identify the sliding units of this modified SHILLA construct. Postoperative (day 2) portrait of the clinical improvement and correction of the appearance of the upper body of the same child following APC.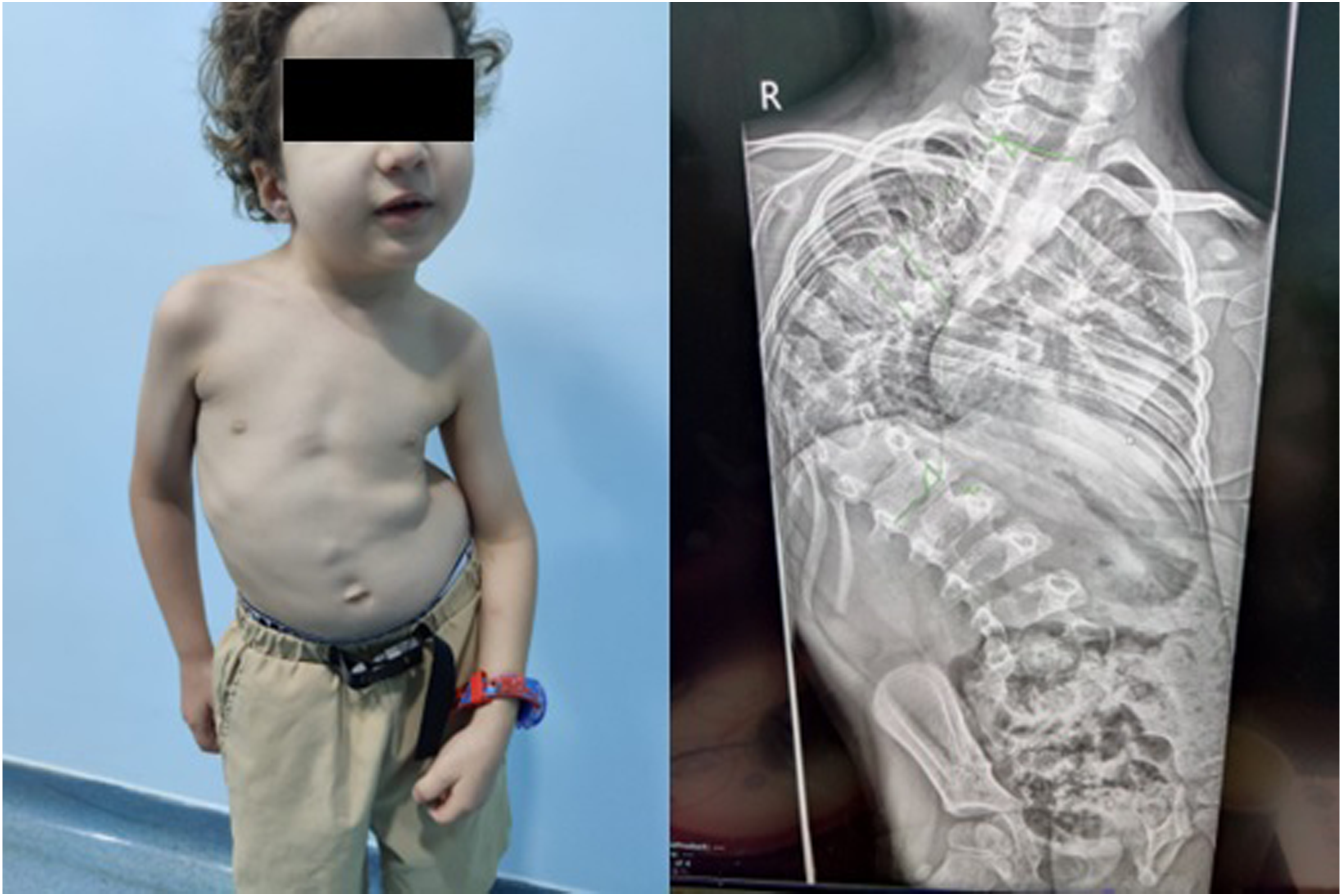

Previous studies reported that biomechanical complications were higher in TGR as compared to APC. 12 Nine biomechanical complications requiring 3 unplanned surgeries were reported in our cohort: screw dislodgment (n = 4), broken rod (n = 2), adding on (n = 2), loss of intraoperative neuromonitoring (n = 1). It is noteworthy that during the follow-up period, none of the patients developed a Crankshaft which is considered a major complication of SHILLA technique. 19 The latter finding is considered an advantage of APC as a modification of the SHILLA, 9 but might as well be attributed to need of longer follow-up.
It is of paramount importance to acknowledge that treatment of spinal deformities and EOS is complex. The latter is reflected in the diversity of complications, their high rates and the fact that they might not show until several years after the operation. 21 A review by Latalski et al found that the most frequent complications were implant related and that incidence of complications can be underestimated; they found that 54% of the patients required unplanned surgeries which accounts for 15% of all surgeries. 4 Another study showed that 50% of patients undergoing SHILLA procedure had implant-related complications postoperatively with 66% needing unplanned surgery. 18 Wilkinson et al also showed 29% implant related complications following SHILLA over 5-year follow-up period. 10 Implant related complications include rod displacement or breakage, screw pull-out, screw-rod loosening, deep and superficial infections, among others.10,18 MCGR, on the other hand, is associated with higher costs and with a high complication profile approaching 42.4% in some studies and 33% rate of unplanned revisions. MCGR-related complications included distraction failure, implant/screw failure, anchor pullout, wound infection and dehiscence and junctional kyphosis.22,23
There are several limitations to this study. First and foremost being the number of patients given that this is a modification of SHILLA procedure and is still a novel technique. Second, we did not quantify the amount of compression applied and how its magnitude affects reverse modulation. To date, there are no randomized controlled trials or prospective studies comparing APC to equivalent corrective surgical techniques (MCGR, SHILLA) in terms of outcomes, hence an evidence-based recommendation of which surgical modality is better is still lacking. All available outcomes are short- and medium-term and still there exists no long-term outcomes which are yet to be investigated. It is true APC serves the purpose of spinal correction and preserve growth, however and as a surgical intervention, it comes with a range of complications that might interfere with the treatment course and require revision.
Conclusion
Although treatment of EOS is still challenging, evolution of knowledge and equipment presents hope and a beacon of opportunity for these patients. APC is a novel technique that has been incorporated in several countries as a treatment modality for EOS and found to be effective in reverse modulating apex wedging. Short-term outcomes are promising in terms of clinical improvement, complication rates and decreased need for multiple operations or unplanned surgeries. Future longer-term studies are indeed needed for better understanding of the clinical and radiographic outcomes and their sustainability, establish safety and efficacy along with complications profile associated with the procedure.
Footnotes
Authors Contributions
All authors listed have contributed to conception and design. AH and AA critically wrote, read and revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AA discloses consultancy from Tria Spine, consultancy from Proximie, Committee chair at SICOT, Committee member at SRS, NASS, AO spine. The rest of the authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.