
Abstract
Study Design
A multicenter retrospective study.
Objectives
To determine the rate of Apex facet fusion in children with Early Onset Scoliosis treated surgically with the Active Apex Correction (APC) technique.
Methods
Seventeen patients were treated with the APC technique as index surgery for Early Onset Scoliosis with more than 1 year of follow-up. A 3D CT scan was done to determine the facet fusion rate in the deformity’s apex controlled with posterior tethering.
Results
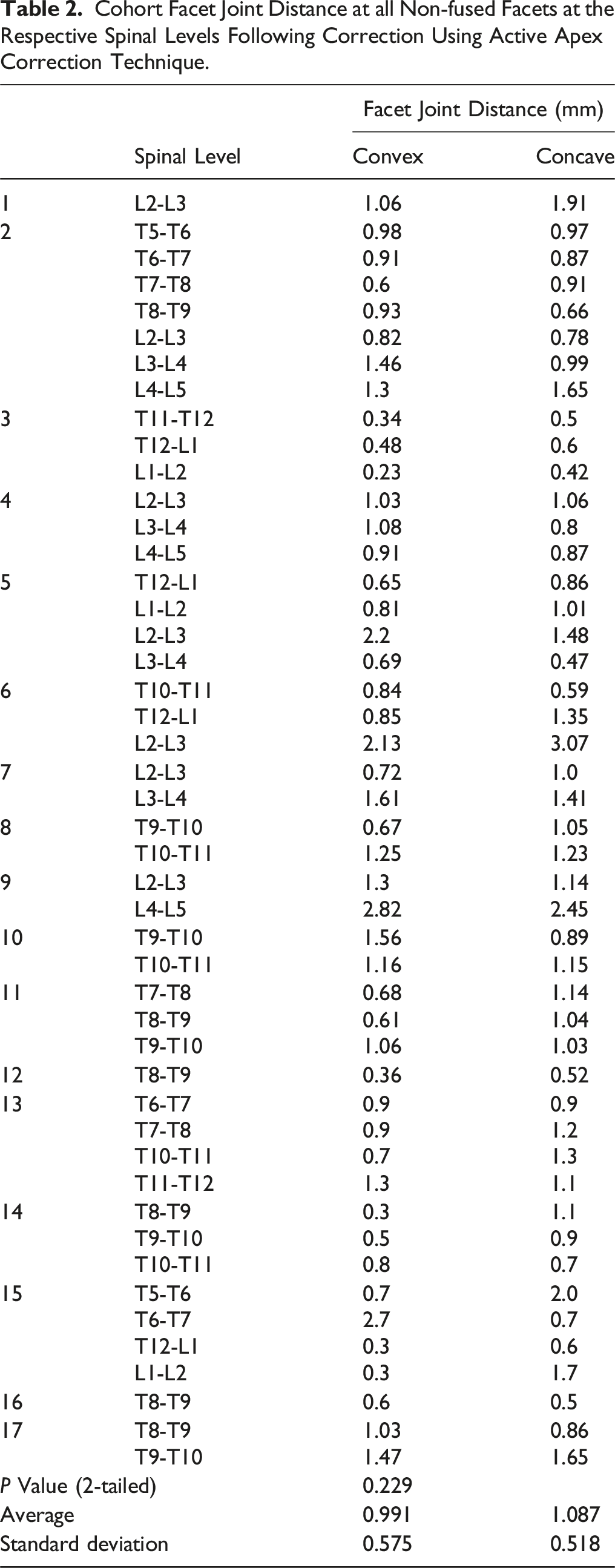
The average follow-up time was 26.4 months (12-56), Average age at index surgery was 81.2 months (30-132), and average number of surgeries done 1.3. Apical vertebrae studied for facet fusion were the 3 vertebrae in the apex in each patient that were subjected to posterior tethering according to the APC technique. In total they were 86 apical vertebrae (172 Facets studied with 86 convex side, 86 concave side). Our observations showed that 29 facet joints were fused (16% of the total facets studied),15 were on the convex, 14 on the concave side (no statistically significant difference). Regarding the facet joint distance in the non-fused facets was 0.99 mm on the convex side and 1.08 mm on the concave side with no statistical significance difference.
Conclusion
APC for Early Onset Scoliosis achieves apical growth modulation and control utilizing posterior tethering without inducing fusion. This study demonstrated that APC is an effective non-fusion technique through the low incidence of facet fusion levels at the Apex, limiting the crankshaft phenomena seen in cases with apex control through arthrodesis.
Keywords
Introduction
Management of progressive Early Onset Scoliosis (EOS) poses a surgical challenge to the pediatric Spine surgeon. Growth friendly surgery has been proposed to manage this complex spectrum of patients allowing spine and lung growth while controlling the deformity. 1 Growth friendly implants can be classified according to their mode of action into : distraction-based, compression-based and growth guidance techniques. 2
Guided growth techniques have gained popularity in the management of Early Onset Scoliosis (EOS) over the last decade. The SHILLA system induced an apical fusion while allowing the rest of the spine to grow through the sliding mechanism in its specific screws. 3 However, the maintenance of the spine growth with the SHILLA technique has been questioned recently. 4 In addition to other complications namely crankshaft and rod breakage. 5
The Active Apex Correction (APC), a hybrid posterior tethering strategy featuring replacing a traditional SHILLA with apex non-fusion and growth modulation through unilateral compression, translation, and rotation on the convex side associated with distraction on the concave side, has been shown to be safe and effective for Early Onset Scoliosis. 6 The rate of facet fusion in the APC technique has not been well investigated. The main purpose of this study is to investigate the rate of facet fusion, especially at the 3 apical and peri-apical vertebrae when implementing APC technique.
Methods
This is a multicenter retrospective study that was done for patients who were treated with APC technique as the index surgery for Early Onset Scoliosis children with more than 1 year follow up. Seventeen patients were included in this study from 6 pediatric spine centers in 6 different countries (8 congenital, 5 Idiopathic, 2 syndromic, 2 neuromuscular). All patients enrolled had a minimum 1 year follow up with a 3D CT scan determining the rate of facet fusion in the Apex of the deformity treated with posterior tethering. To note, CT scan is not routinely performed on every patient undergoing APC, but was patient-specific depending on progress in their case requiring CT imaging. The current study is a retrospective study and all investigations were done regardless of the study, as such informed consent was not required and was deemed exempt from this requirement.
APC is performed by placing pedicle screws on the convex side, above and below the most wedged vertebrae (Figure 1). The screws are compressed onto each other before the final tightening to induce compressive forces that would allow the modulation of the wedged vertebra over time.
7
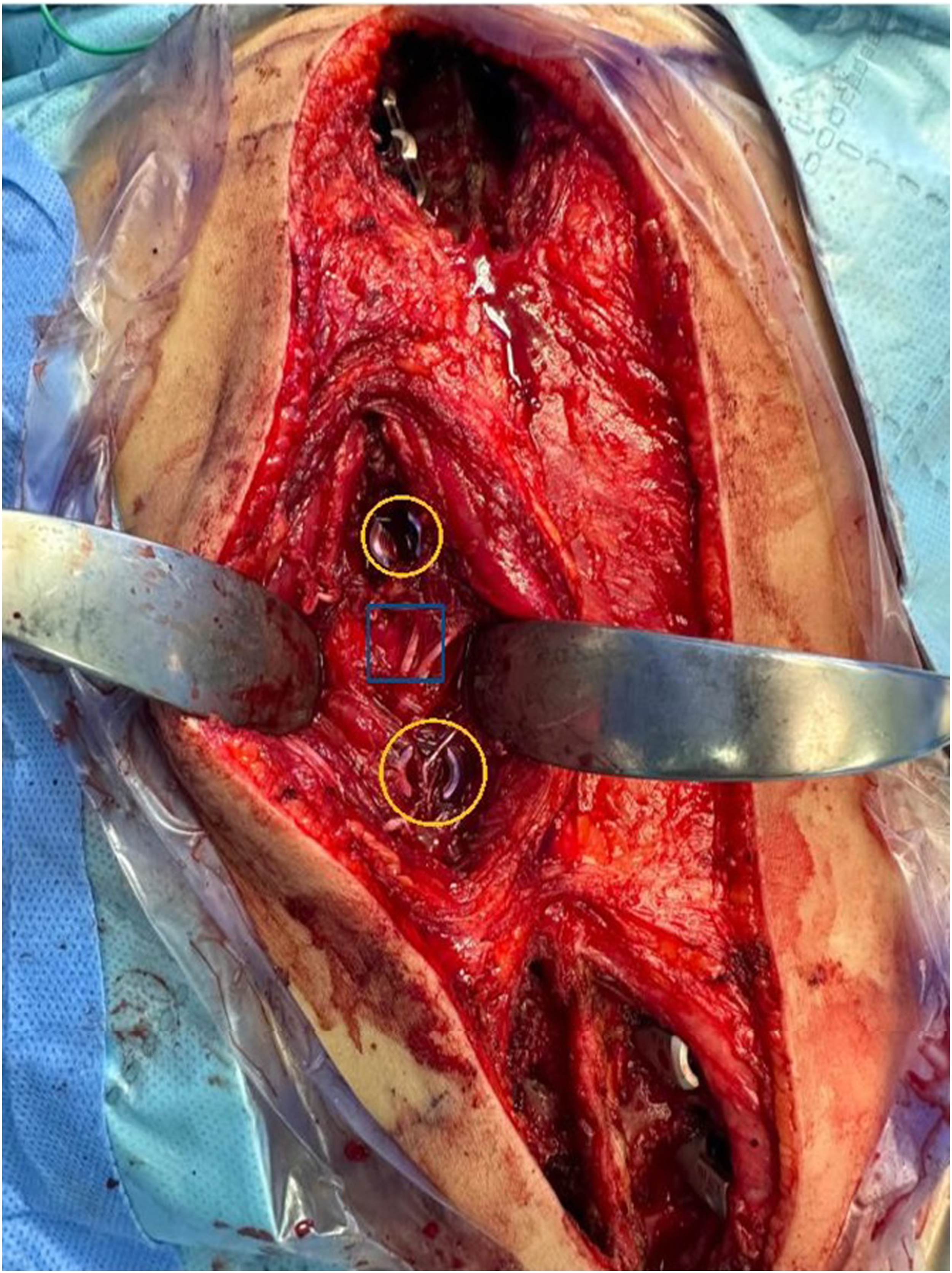
All patients went through a specific procedure related to putting the screws in the apex. We try to put the screw through Wiltse Approach with extraperiosteally exposure avoiding as possible the soft tissue disruption and increase the non-fusion process (Figure 2), with apex correction through compression, rotation, medial translation, which will go with the geometry of the corrected spine, reducing the stress discontinuity and avoiding a junctional area between the apex and the non-instrumented spine above and below, which might be the main reason for the decreased incidence of crankshaft phenomena, rod fracture, beside the good correction postoperatively.
8
All other details of the APC technique are done according to the previously published publications.6-10 Postoperative complications were recorded. Preoperative xray of a 5 years old child with major lumbar curve with T12 most wedged and laterally displaced vertebra. A: preoperative xray with T12 (enlightened with blue color) with the screws placed on the convex side of T11 and L1 (enlightened in orange). B: Post operative xrays in coronal and sagittal views putting tethering screws T11, L1 (enlightened in orange) with the most wedged vertebra T12 (enlightened in blue), with the rods to slide (enlightened in green), and proximal and distal anchors (enlightened in red). Tethered pedicle screws (enlightened in orange) are put in the convex side of the apex through Wiltse technique; the most wedged vertebra (enlightened in blue) is not exposed, besides the exposure is only for the proximal and distal anchors without soft tissue disruption in between.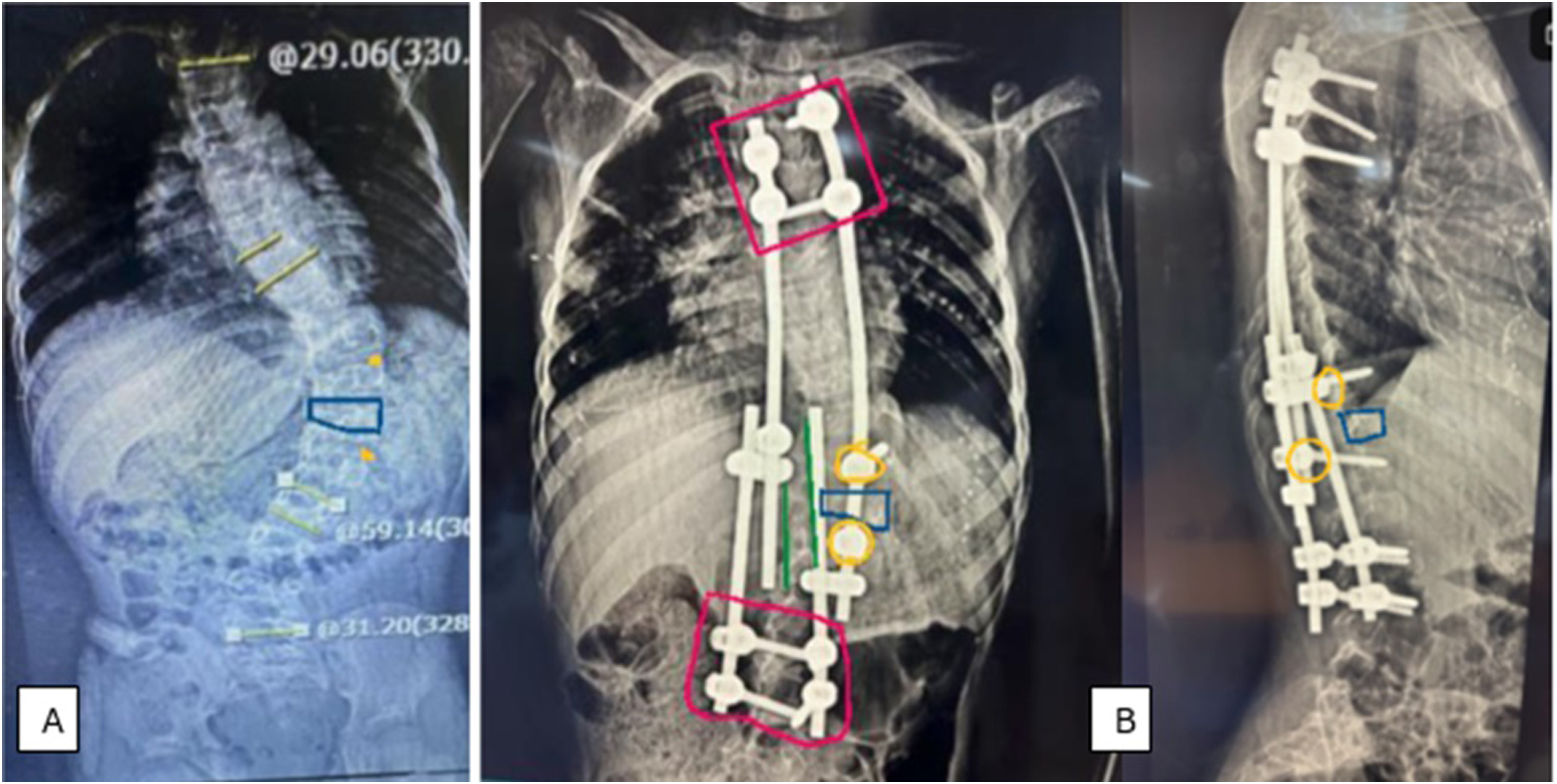
Careful analysis of the facet distance was done and recorded in the axial CT cuts that were exactly perpendicular to the facet joint line (Figure 3). The facet was considered unfused if there was a preserved facet joint line space. If there was no facet distance identified, the facet was considered fused. An example for checking the facet fusion through CT scan. The most wedged vertebra was T7, with the apex including T6,7,8; pedicle screws were put on the convex side T6 and T8. A: T6-T7 facet joints. B: T7-T8 right concave side. C: T7-T8 left convex side.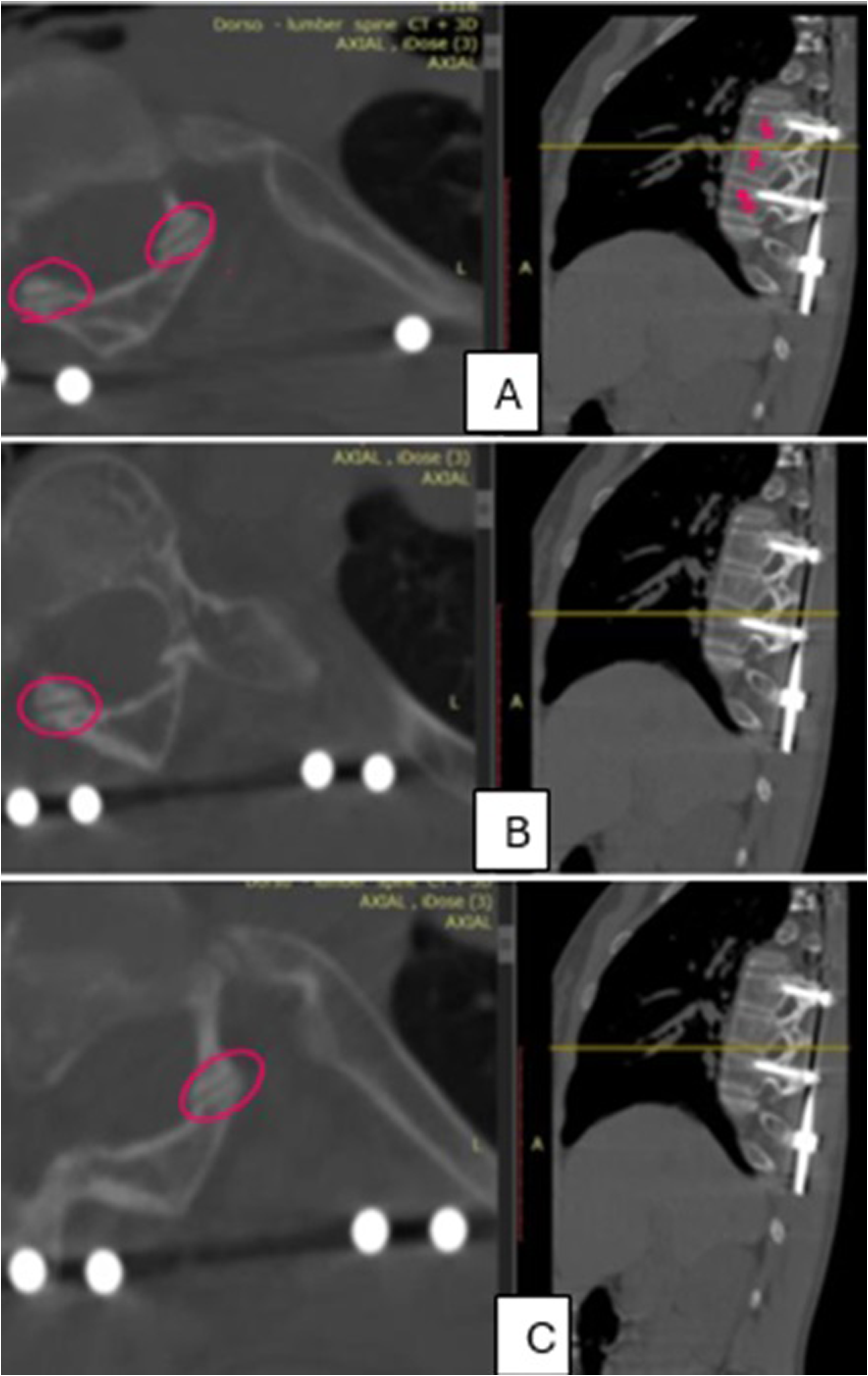
This study was approved by the Institutional Review Board (IRB) at Palestine Polytechnic University (number: KA/41/2024). The current study is a retrospective study that did not require an informed consent, as such it was deemed exempt from this requirement. Data was analyzed using Microsoft Excel. A general descriptive analysis of the data was initially performed. Continuous data were reported as mean and standard deviation (SD). Categorical variables were reported as absolute numbers and percentages. Paired t-tests were used to analyze the magnitude of change between preoperative and postoperative states. Results with P < 0.05 were considered statistically significant.
Results
17 patients with EOS underwent surgery with Active Apex Correction (APC) technique as an index surgery in 6 pediatric spine centers in 6 different countries with minimum 1 year follow up. All of them had 3D-CT scan done at the last follow up visit. The average follow-up time was 26.4 months (range: 12-56 months), Average age at index surgery was 81.2 months (range: 30-132), and average number of surgeries done was 1.3.
Cohort Spinal Parameters at Surgery and at the Last Follow-up Quantifying the Extent of Deformity and Subsequent Correction.
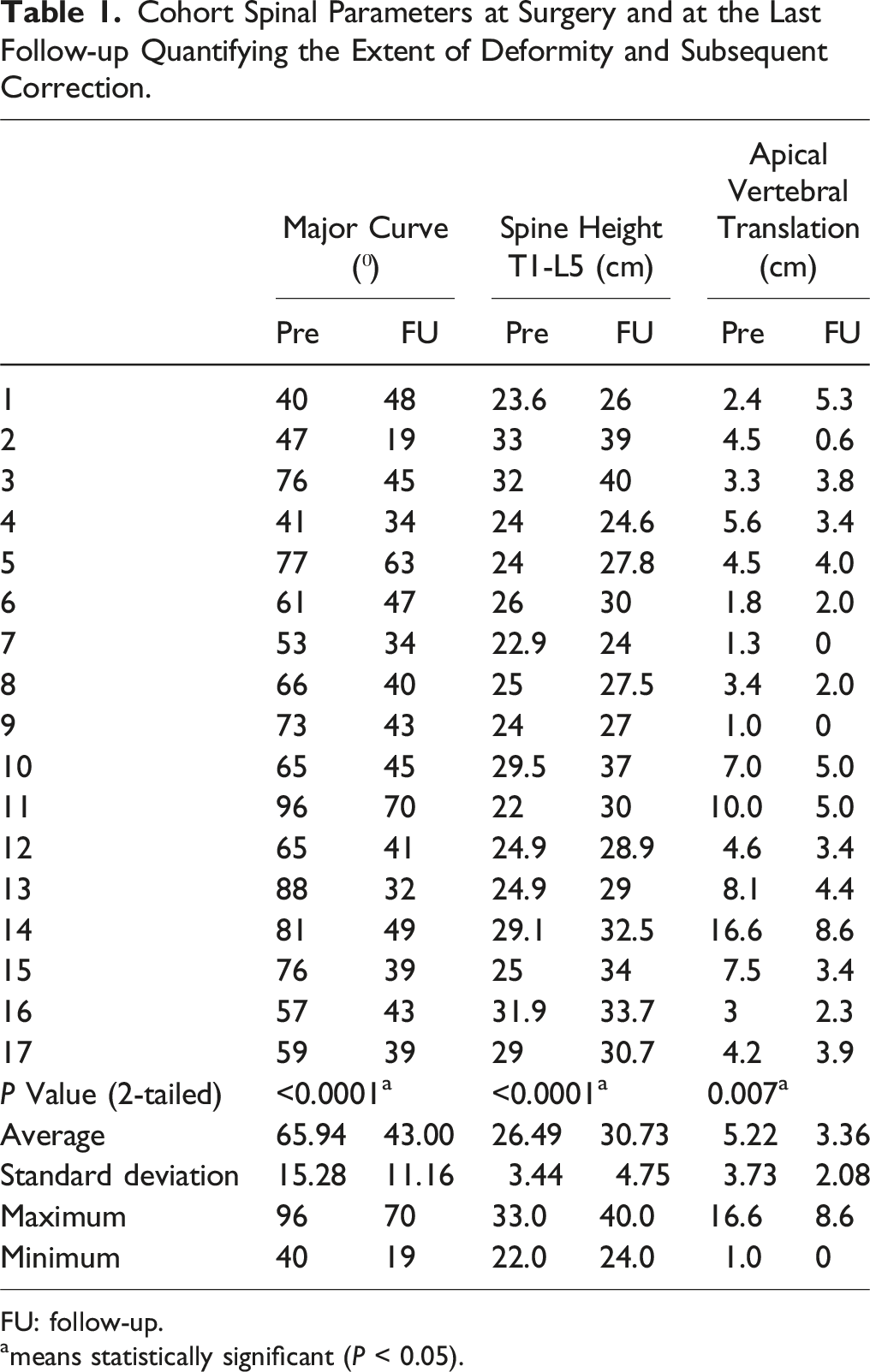
FU: follow-up.
ameans statistically significant (P < 0.05).
Cohort Facet Joint Distance at all Non-fused Facets at the Respective Spinal Levels Following Correction Using Active Apex Correction Technique.
Discussion
The main corner stone in surgical management of EOS is controlling the spinal deformity while allowing spinal growth. 11 Optimizing spinal growth is of crucial importance in growing children as it has a direct impact on their pulmonary functions and their quality of life as adults. 12 Growth friendly surgeries are classified based on the forces the implants impose on the spine into compression-based, distraction-based and guided growth. 2
SHILLA is a popular technique described by McCarthy with spine guided growth technique through correction and fusion of the apex of the major curve (usually 3-4 levels) and rod sliding through the SHILLA screws in the proximal and distal anchors. 3 This technique was found to be accompanied by high incidence of crankshaft and adding on, rod breakage, screws pullout, beside complications related to osteotomies done in the apex.4,13
A modification of the SHILLA was done to overcome the complications related to this technique. The APC technique is a hybrid method that was developed since 2008 that modifies the apex through reverse modulation by imposing compression forces on the convex side of apical vertebra while guiding the spinal growth through sliding rods. 7
This study aimed to investigate the incidence of apical non-fusion through posterior tethering with the APC technique. The main concept of apical control (usually 3 vertebrae) without fusion is posterior tethering by putting screws on the convex side above and below the most wedged vertebrae, with minimal facet exposure, avoiding subperiosteal dissection, and minimal soft tissue disruption (Wiltse approach).
Our assumption is that this technique will correct the apex through modulation according to Hueter Volkmans law which will be a true non fusion technique, minimizing the incidence of Crankshaft phenomena accompanied with the Apex fusion as in SHILLA. Since the main fusion process in scoliosis is facet fusion, our hypothesis is that most of the apical facets will not fuse. The facet joint line distance measured on axial cuts of the CT scan was used as a surrogate indicating non-fusion at the apical and peri-apical levels as previously outlined in Yamada’s et al study. 14 The presence of a visible facet joint line distance indicated that this level still has maintained growth potential and was not inadvertently fused (Figure 3).
We did 3D CT scan for the cases gone through APC as index surgery, studied the facet joints of the 3 levels of each apex in the major curve (concave and convex sides) that went through posterior tethering with APC technique. This study suggests that the APC technique is protective against the crank shaft phenomenon as it did not induce fusion at the apical levels while controlling the spinal deformity. The relatively small percentage of inadvertently fused facets in the APC technique (16%) in this study is a promising sign in solving 1 of the major drawbacks of surgical intervention in EOS, contrary to the traditional Shilla technique3 where apical vertebra are intentionally fused. Additionally, the distinctive apical control ability of the APC technique outperforms the distraction-based techniques as they lack the ability to control the apex. 15
Moreover, this study is an extra step in analysing the effectiveness of the APC in controlling the spinal deformity in EOS patients while allowing spinal growth. The correction of the coronal cobb angle was significant and comparable to the other different techniques 16 without the need for multiple surgeries or having to deal with different problems of the MAGEC rods.17,18 The optimization of spine growth as well was similar to normal values19,20 and equivalent to the results of distraction-based surgeries.21,22
This is the first study to our knowledge to evaluate 1 of the growth friendly techniques in terms of facet fusion as a surrogate for long term success in maintaining spinal growth. It is a very logical concept, but it has not been studied before. Limitations of this study include the retrospective nature of this research, the heterogenicity of types of EOS treated, relatively low number of patients included, and the lack of long term follow up. However, as the APC technique has been recently described, there is no long term follow up data yet, but this study is a step on the way evaluating the technique and its potential benefits in management of a complex group of patients. We hope future studies will include more patients with a longer follow up.
Conclusion
APC for Early Onset Scoliosis offers patients apical correction associated with modulation and non-fusion technique, clearly demonstrated with low incidence of facet fusion levels at the Apex, limiting the crankshaft phenomena seen in cases resulting in arthrodesis at apical levels.
Footnotes
Author Contributions
All authors listed have contributed to conception and design. AA critically wrote, read and revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AA discloses consultancy from Proximie, Committee chair at SICOT, Committee member at SRS, NASS, AO spine. The rest of the authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.