
Abstract
Study Design:
A retrospective study.
Objective:
To determine if active remodulation in the apex of the curve is possible in scoliosis and kyphoscoliosis patients, using a modified SHILLA; active apex correction (APC) technique for guided growth.
Method:
Twenty patients with either scoliosis or kyphoscoliosis underwent a modified SHILLA approach, where instead of apical fusion, APC was applied. In this modified technique, the most wedged vertebra was selected followed by insertion of pedicle screws in the convex side of the vertebrae above and below the wedged one. The convex and concave heights of the wedged and control vertebrae were recorded at the time of the surgery and at follow-up duration, both using computed tomography.
Results:
The wedged vertebra demonstrated in average a 17% (P = .00014) increase in the proportion of concave to convex heights ratio, whereas the control vertebra did not show any relative change in the wedged vertebra heights at the follow-ups.
Conclusion:
APC, instead of apical fusion in SHILLA remodulates the apex vertebra, which may in turn help mitigate loss of correction on long term due to crankshafting and adding-on.
Keywords
Introduction
Growth guidance technique using SHILLA is 1 of the 2 most widely used posterior-based growth friendly techniques for curve correction and halting the progression of deformity in children with scoliosis or kyphoscoliosis. 1,2 SHILLA has the advantage of being one-time surgery and is technologically less demanding compared with MAGEC rods. 3 -6 However, there are still 2 major disadvantages of using SHILLA: loss of correction and need for osteotomies, that has made its use in par with distraction-based system. To elaborate, substantial percentage of patients undergoing SHILLA technique experience loss of correction via crankshafting or adding-on (eg, distal migration). 7 -9 In addition, the need for osteotomies on the concave side has the potential of severe complications. Therefore, any modified SHILLA technique that could eliminate the loss of correction and complications related to the need of osteotomies on the concave side is very desirable.
Based on previous studies using staples and anterior tethering, exemplifying the well-known phenomenon of Hueter Volkmann principle, we too hypothesize that the wedging of the deformed vertebra in immature scoliosis can be corrected through apex compression (using pedicle screws as levers) on the convex side to reverse the progressive asymmetric growth of that vertebra, and thereby actively reducing the wedge angle. 10 -12 This nonfusion SHILLA procedure, active apex correction (APC), is performed by placing pedicle screws on the convex side, above and below the wedged vertebrae. The pedicle screws are then compressed before final tightening, to artificially create a compensatory pressure on the vertebral body by thus gradually allow its remodulation (reverse modulation) and reduction in the wedging over time. In contrast to the regular SHILLA approach, the addition of APC could mitigate or reduce future loss of correction, and also eliminates the complications related to the need of osteotomies (no screw is required at the concave side of the apex) as a procedural byproduct.
Method
Institutional review board approved this study. The study consisted of 20 patients with either scoliosis or kyphoscoliosis undergoing an index surgery or revision surgery and demonstrating a clear radiographic evidence of vertebral wedging at the apex. In the subgroup of congenital scoliosis, these patients had both malformation and malsegmentation with unilateral bony bar. All patients were younger than 8 years with Risser less than or equal to 2, and the major Cobb’s angle more than 40°. Refer to Table 1 for further patient details at surgery and during follow-up.
Diagnoses, Age at Surgery, Gender, Follow-up Duration, and Spinal Parameters Quantifying the Extent of Deformity.
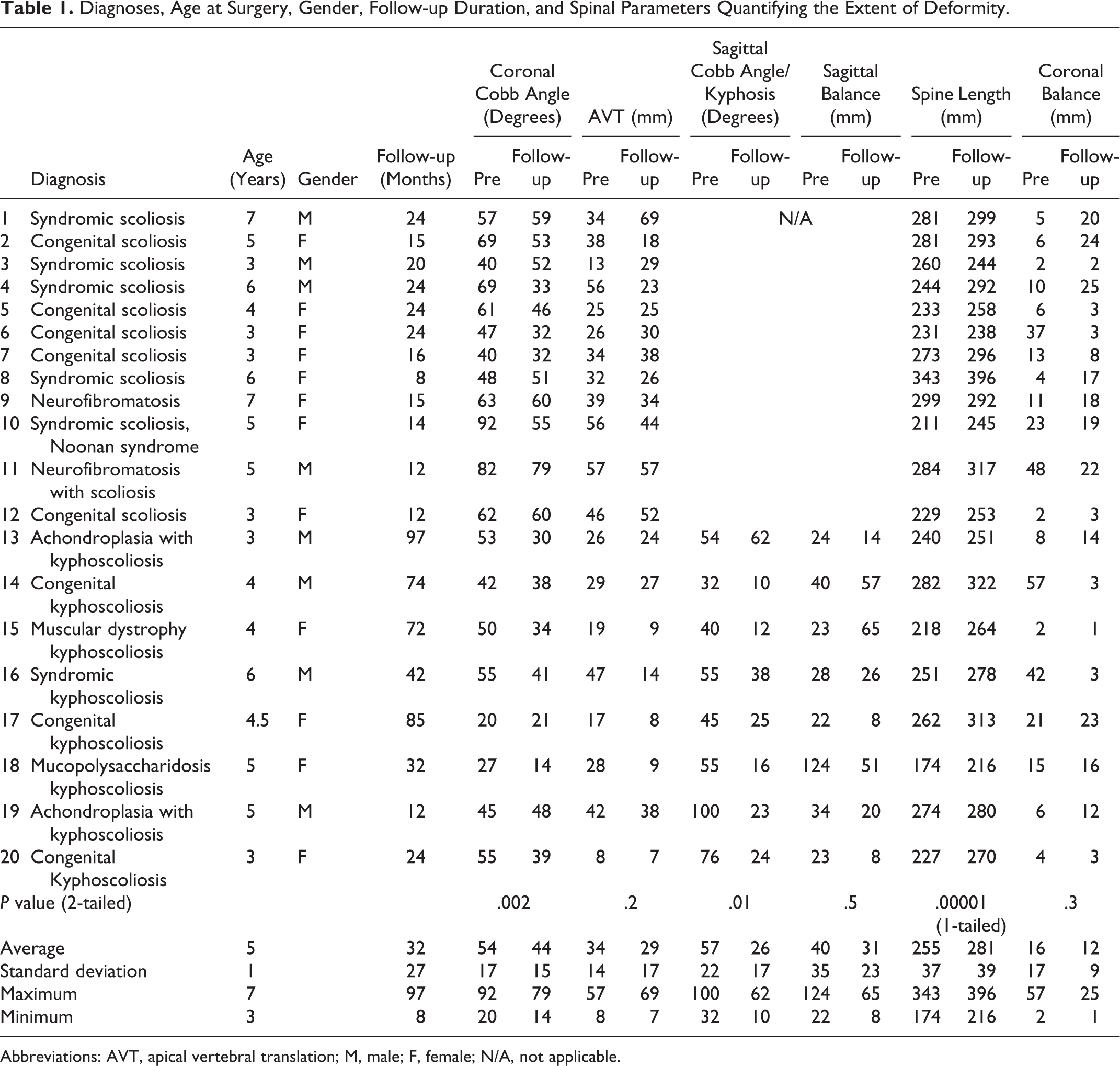
Abbreviations: AVT, apical vertebral translation; M, male; F, female; N/A, not applicable.
The surgical procedure involved was a modified version of to SHILLA (Figures 1 and 2), either using rod to screw (SHILLA screws from Medtronics) sliding mechanism or the analogous rod to domino (4.5-mm rod in 5.5-mm domino) sliding mechanism. In this modified technique, the most wedged vertebra was selected followed by insertion of pedicle screws in the convex side of the vertebrae above and below the wedged one. No screws were put on the concave side of the apex. All surgeries were performed under intraoperative neuromonitor and C-arm. Additionally, no cast or brace were used for these patients postoperatively. The technique was extraperiosteal except for the convex side of the apical (and wedged) vertebrae, where we put screws for compression. The rods and domino remained subfacial, to avoid prominence. The patients were followed for a period of at least 8 months. The convex and concave heights of the wedged vertebra were recorded at the time of the surgery and at follow-up, both using computed tomography. For comparison, a control vertebra was chosen, whose physical dimensions were in par with the wedged vertebra to record the normal growth rate of the particular duration of follow-up and age. The main difference between a wedged vertebra and the control vertebra was the compression forces being applied at the convex end (including congenital subgroup) for the wedged vertebra, with the expectations of reducing local longitudinal growth rate. In the control group no such forces were applied.
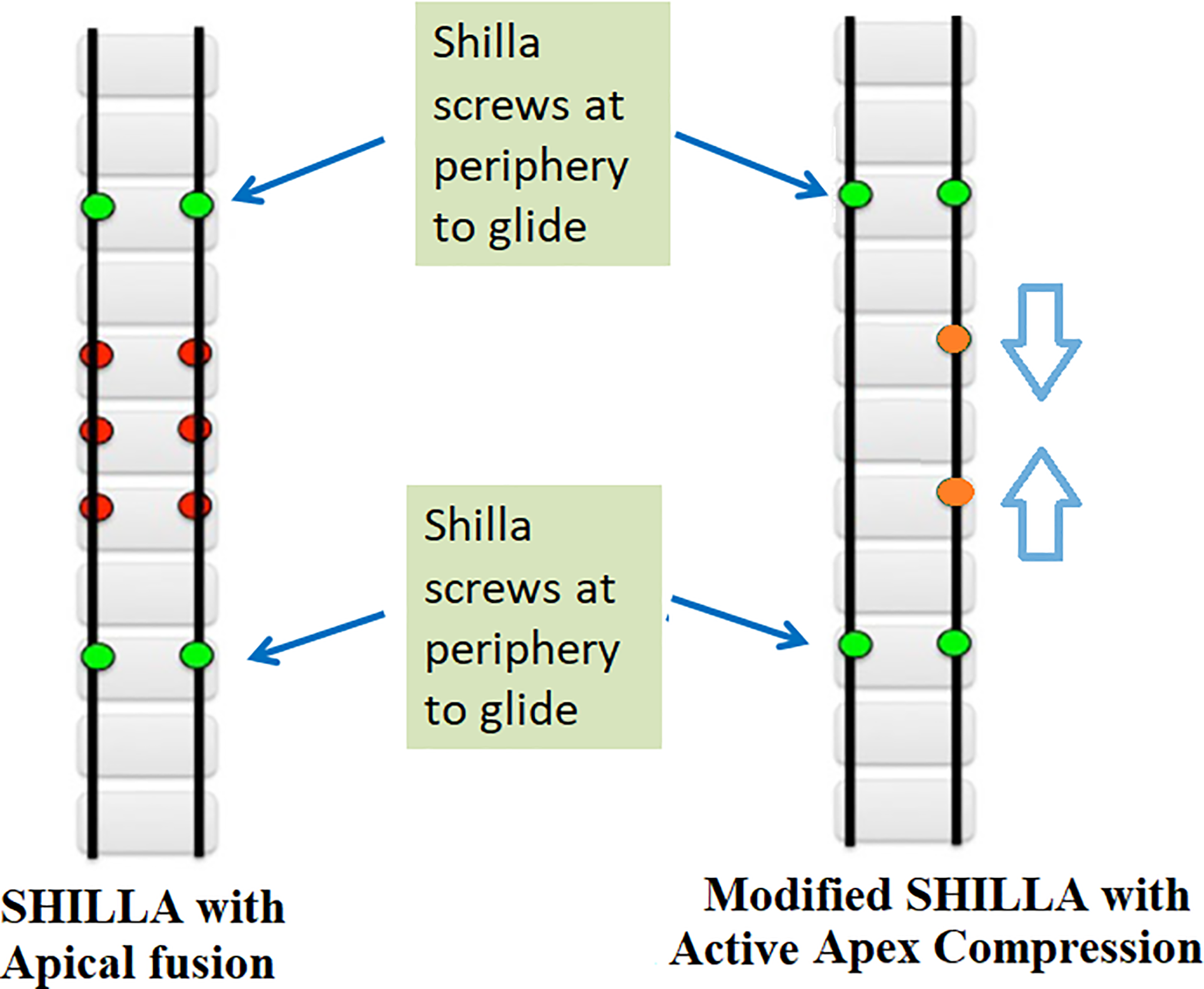
Schematic showing key differences in established SHILLA procedure and the modified SHILLA approach used in this study.
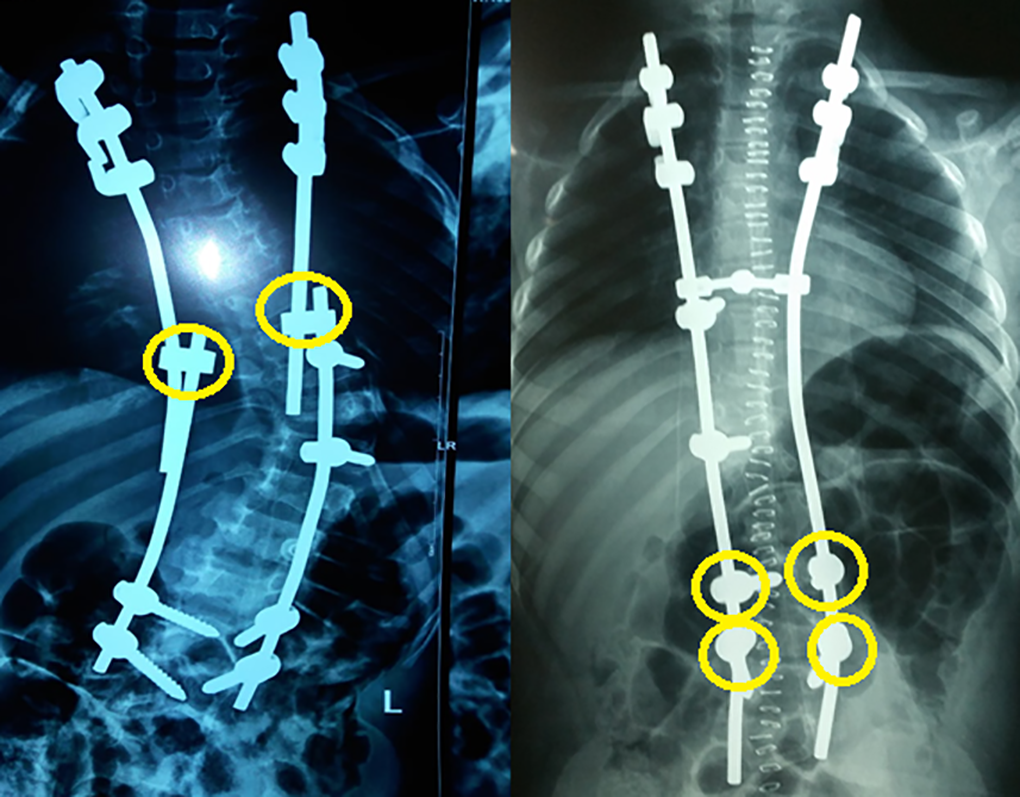
Radiographs of 2 patients exemplifying the 2 types of, but analogous, modified SHILLA procedure. (Left) The modified SHILLA approach using dominos (4.5-mm rod in 5.5-mm domino hole) for sliding with growth. (Right) The modified SHILLA approach using pedicle screw-rod clearance for sliding with growth. Yellow circles identify the sliding units of this SHILLA construct for sustenance of overall longitudinal growth of the spine until puberty.
Results
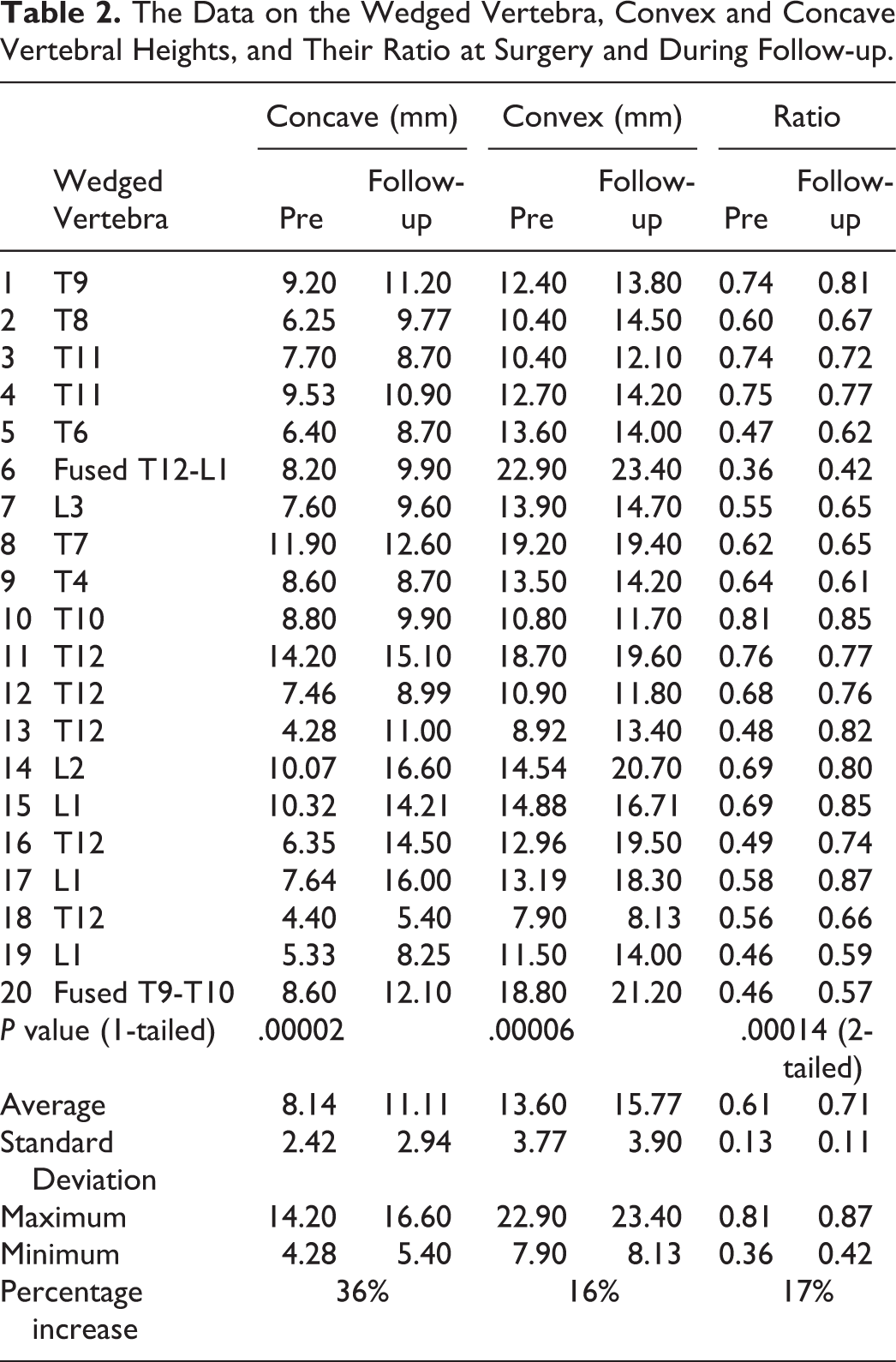
The wedged vertebra under apex compression demonstrated an average increase of 17% (P = .00014) in the proportion of concave to convex heights ratio. However, as expected, the control vertebra did not show any lateral deviance in the height at the follow ups. Table 2 presents data array on the wedged vertebra, concave and convex vertebral heights, and their ratio at surgery and during follow-up. The concave end of wedged vertebra increased by an average of 36%, whereas the convex side showed an increase of 16%. Table 3 presents data array on the control vertebra, convex and concave vertebral heights, and their ratio during surgery and at follow-up. Both the concave and convex ends of the control vertebra increased by an average of 17%.
The Data on the Wedged Vertebra, Convex and Concave Vertebral Heights, and Their Ratio at Surgery and During Follow-up.
The Data on the Control Vertebra, Convex and Concave Vertebral Heights, and Their Ratio at Surgery and During Follow-up.
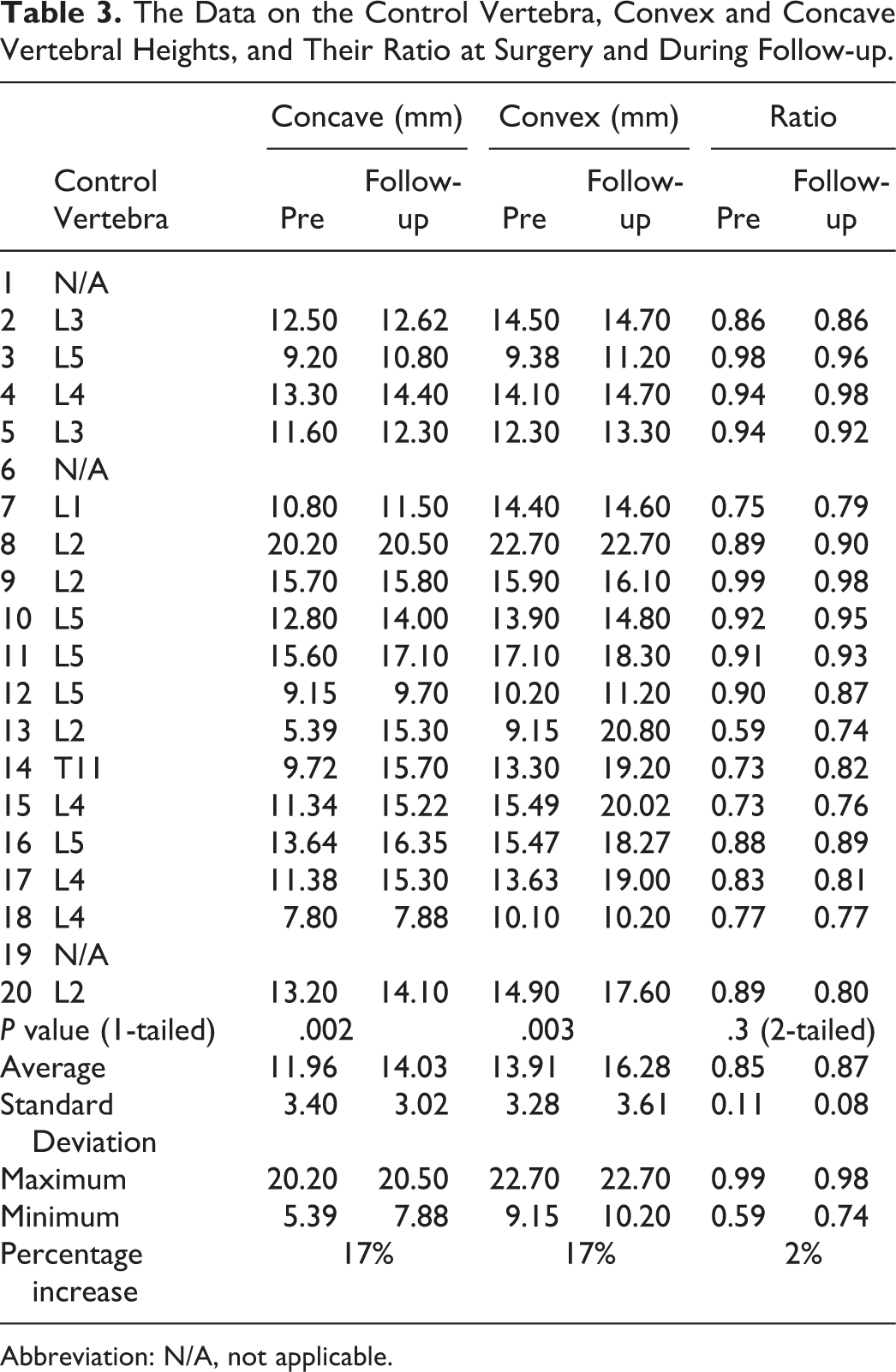
Abbreviation: N/A, not applicable.
Discussion
Crankshaft phenomena has been well described by Dubousset as a major complication in growing spine management. 7,8 The long-term goals of selecting this procedure is to assess if active remodulation of the apex is possible, and if so, whether it would avoid crankshaft effect or distal migration. The study presents preliminary data on apex vertebral growth remodulation post modified SHILLA procedure. Instead of apical fusion, apex compression was applied at the wedged vertebra. This in addition to allowing a foundation for fixation at the apex, traditionally sought for controlling the curve, also seeks to dynamically modify the peak of the curve. The immediate benefits of the procedure alone are avoidance of risky osteotomies required to insert screws at the concave end of the apex, and more economical surgery (putting 2 screws instead of 6 at the apex of the curve) for underprivileged patients globally with no added risk over SHILLA. 13,14 Furthermore, in presence of more than one curve, this procedure is still applicable, whereas the SHILLA technique may not be as practical. Biomechanical complications included dislodgment of iliac screws (1), proximal hook dislodgment (1), iliac screw and rod loosening (1), rod fracture (1) and proximal junctional kyphosis (1). The subject of this study was to estimate the reverse modulation as a result of this intervention, that is, APC. The results did show correction in the wedging of the vertebra due to APC, in contrary to a static fusion at the apex, which have been shown to cause continued growth of deformity and thus crankshafting or adding-on. Nevertheless, a less varied cohort with equal follow up duration in patients undergoing this procedure is required to establish its efficacy in mitigating or reducing crankshafting or distal migration. Although, we do see reduction in wedging, it is still not clear if it was a result of convex-only fixation without fusion at the apex or due to apex compression of the wedged vertebra on the convex side.
There are several limitations to the current study, first and foremost being the number of patients. Given a major deviation from the established SHILLA procedure, it was a prudent measure to limit this procedure to a few and perform a close follow up. However, given these results we are confident to carry on an open enrollment of patients with scoliosis and kyphoscoliosis. The second shortcoming of the study is that we didn’t quantify the amount of compression being applied, and how the magnitude of compression or lack of it altogether affects the reverse modulation in practice. We intend to quantify that in future either via direct measurement or virtual setup employing Hueter Volkmann principle where a patient-specific kinetic model could be used to determine the forces based on the height gain in a given period. 15 -20
Yet with all these shortcomings, the study demonstrates the possibility of safely and effectively reverse modulating the wedging at the apex using a modified SHILLA technique, and in theory has the potential to mitigate crankshafting or adding-on.
Conclusion
The result of this study provides clinical evidence of reverse vertebral modulation at the apex of the curve in patients with scoliosis and kyphoscoliosis, when modifying the traditional SHILLA technique with APC.
Footnotes
Authors’ Note
The device(s)/drug(s) is/are approved by the Food and Drug Administration or approved by corresponding national agency for this indication.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. AA reports royalties from Paradigm Spine, Joimax, consultancy from Spinal Balance, editorial board membership from Clinical Spine Surgery and Spine, outside the submitted work. The other authors (LA, AAA) have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.