
Abstract
Study Design
Retrospective cohort study.
Objective
The orthopaedic ability of traditional GR for severe EOS is limited. The proximal upper thoracic curve may progress during the lengthening procedure, which may lead to coronal imbalance and inhibit the longitudinal growth of the spine. In this retrospective cohort study, we investigated the clinical outcome of tandem GR.
Methods
We modified the traditional technique by using two groups of GR devices to control the major and the proximal upper thoracic curve, connected the two groups of GR in series, and named it tandem GR. The clinical and imaging outcomes of the new technique were evaluated and compared with traditional technique.
Results
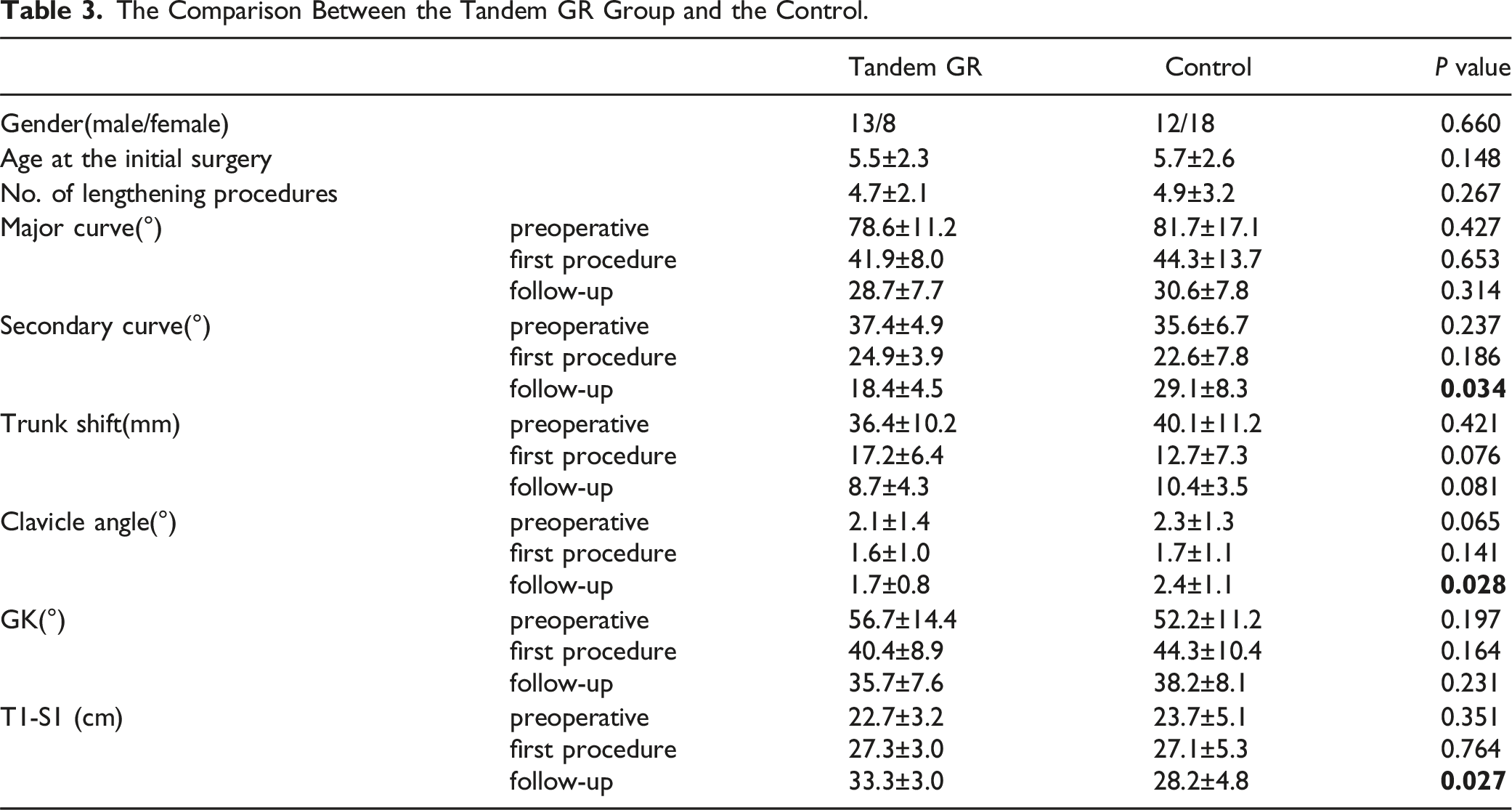
Twenty one patients were enrolled in the tandem GR group, and 30 patients were treated with traditional GR as the control. The baseline parameters were consistent between the two groups. In the tandem GR group, the secondary curve progressed from 24.9 ± 3.9° to 31.4 ± 3.2° (P = .006) in the procedure with the traditional GR and improved to 18.4 ± 4.5° (P = .001) after the switch. Meanwhile, the clavicular angle aggravated from 1.6 ± 1.0° to 2.6 ± .7° (P = .041), and improved to 1.7 ± .8° after changed to the tandem GR (P = .033). At the final of the follow-up, the secondary curve was higher in the control group (27.1 ± 8.3° vs 18.4 ± 4.5°, P = .034), the clavicle angle was 2.4 ± 1.1° in control and 1.7 ± .8° in the tandem GR group (P = .028), the T1-S1 height was 28.2 ± 4.8 cm in the control and 33.3 ± 3.0 cm in the tandem GR group (P = .027). The average growth rate was 1.0 ± .3 cm/year in the control and 1.2 ± .4 cm/year in the tandem GR group (P = .046).
Conclusion
Tandem GR can effectively improve the proximal upper thoracic curve progression during the treatment of EOS. Compared with the traditional GR, tandem GR can achieve better curve correction, better shoulder balance, and retains more capacity for longitudinal spine growth.
Introduction
During the treatment of severe early onset scoliosis (EOS) with a traditional growing rod (GR), good control of the major curve is always achieved. However, the proximal upper thoracic curve may progress during the lengthening process. In this article we also refer to it as secondary curve. Many studies have found that GR often improves after the first operation, but the secondary curve may progress over time.1,2 Wang et al 3 found that traditional GR can only control the progression of the major curve in severe EOS, and has a limited effect on coronal imbalance. Bjerke et al 4 conducted that significant correction of the main thoracic curve (>54%) with simultaneous “under-correction” (<52%) of the upper thoracic curve resulted in shoulder height imbalance. Because the proximal upper thoracic curve is always short and rigid, so far it is lacking of a reliable surgical method. 5 Therefore, upgrading the traditional GR technique is necessary to improve its orthopaedic effects.
EOS tends to show rapid progression, the annual progression ratio was 10-20° per year in patients with EOS.6,7 Studies conducted that after treatment with traditional GR, C7PL-CSVL (the distance between the C7 plumb line and the centre sacral vertical line) always increases by more than 20 mm.8-10 According to the experience of Flynn, 11 the improvement of the secondary curve with traditional GR is less than 50%. Li et al 12 conduct that shoulder elevation over 1 cm in the lengthening procedure is predictive of shoulder imbalance ≥2 cm after treatment of GR. Hence, the correction strategy of the proximal upper thoracic curve is closely related to the postoperative clinical outcome.4,13 In the past patients with secondary curve progression or shoulder imbalance always lack of effective coping method and premature termination of GR treatment, which may exacerbate coronal imbalance and inhibit longitudinal growth of the spine.
We modified the technique by using two sets of GR devices to control the major and secondary curves, and connected the two groups of devices in series. We named this tandem GR by referring to the concept of a series circuit in physics. When the secondary curve progressed, another set of devices was connected to the original device. It is expected that the distraction function of the newly added device can be directly applied to the secondary curve to achieve better curve correction. This study evaluated the clinical outcome of tandem GR and its orthopaedic effect on severe EOS.
Methods
A retrospective analysis was performed on patients treated for GR from January 2014 to December 2020. Before the study began, approval was obtained from the Institutional review board (IRB approval number 2014 -173). In addition, all guardians provided and signed an informed consent form.
Inclusion Criteria
1) Patients less than 10 years; 2) Cobb angle over than 60°; 3) follow-up time longer than 24 months; 4) patients undergoing surgery for the first time, no other invasive treatment was performed prior to GR treatment; 5) secondary curve progressed more than 10° during the 6-month follow-up period; 6) obvious shoulder imbalance (shoulder imbalance ≥ 2 cm) occurred in the lengthening procedure, and 7) no significant improvement in the secondary curve was observed by fluoroscopy during the lengthening procedure.
Patients who switched to tandem GR when the secondary curve progressed were enrolled in the tandem GR group. Further, patients who continued treatment with the traditional technique were enrolled in the control group.
During this period, 241 patients underwent treatment for GR at our institution. 51 cases met the inclusion criteria with the secondary curve progressed. Twenty-one patients were enrolled in the tandem GR group, and 30 underwent the traditional technique were assigned to the control group.
Methods of Surgery
The first step in the surgical procedure was the implantation of the traditional GR. We refer to the operational technique proposed by Akbarnia et al. 14 The placement of the proximal and distal screws depends on the whole-spine standing radiographs and bending images. The patient was placed in a prone position, soft tissue was removed along the spinous process to the facet joint, and pedicle screws in the proximal and distal anchor points were implanted. The cephalad and caudal exposures for insertion of screws is subperiosteal. The remaining area of exposure is subfascial to prevent spontaneous fusion. Typically, two pairs of screws are fixed at the proximal and distal ends. Two titanium rods with a pre-formed curve were passed through the muscle surface below the deep fascia and connected to the proximal and distal anchor points and connector, respectively. When the coronal imbalance was severe, additional screws were implanted in the apical region, and the offset vertebra was pulled to the midline.
When the proximal upper thoracic curve progression was observed and the patient was enrolled in the tandem GR group, the traditional GR was switched to the new technique. Another GR device was implanted at the cranial end of the original GR device during the next procedure. The original rod was truncated in the apex region of the proximal upper thoracic curve. Two additional new rods were connected to the original rod using connectors. In this way, the two sets of rods at the cranial end and the tail end are connected together in parallel along the central line. The balance of the shoulder and the correction of the secondary curve were observed by intraoperative fluoroscopy, and the curvature of the rod and the position of the connector were adjusted if necessary. It was equivalent to use two sets of GR to control the major curve and proximal upper thoracic curve respectively. We anticipated that the proximal upper thoracic curve would be corrected by the distraction of the newly added GR. Schematic diagram of the tandem GR technique is presented in Figure 1. Schematic diagram of tandem growing rod technique.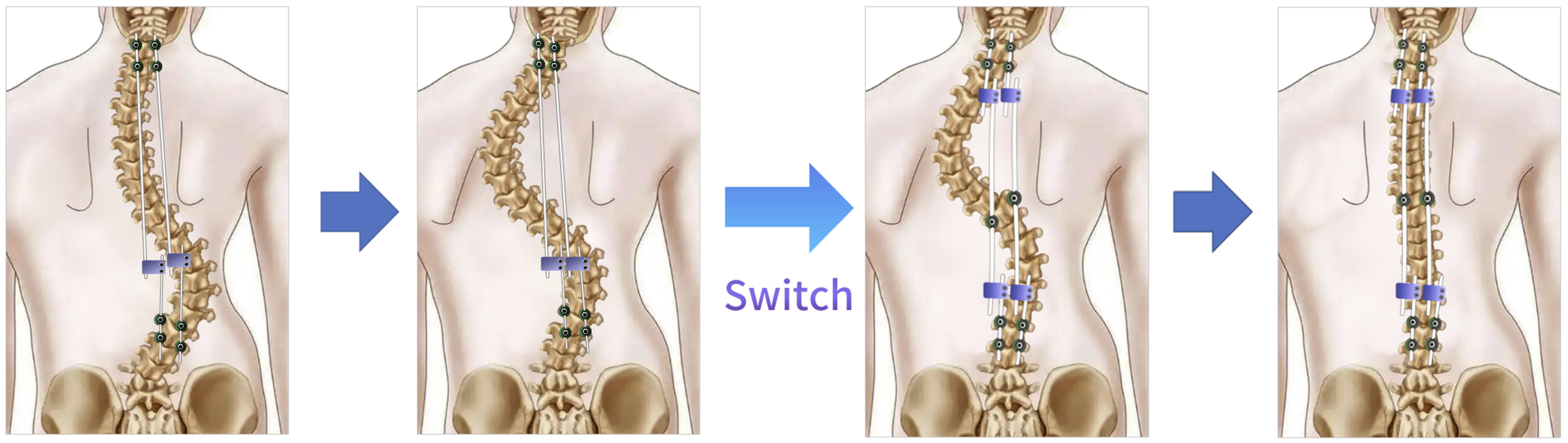
Radiographic Parameters
The fixed segments and Cobb angles of the major and secondary curves were recorded during the follow-up. Trunk shift represented the distance between the C7 plumb line (C7PL) and the centre sacral vertical line (CSVL). Global kyphosis (GK) represented the angle between the cephalad and caudal vertebral bodies with the maximum oblique angle in lateral spine X-rays. The angle of the clavicle represented the angle between the line of the highest point of the clavicle and the horizontal line. All the above parameters were recorded.
Complications
Complications in each group, such as infection, nerve injury, and implant-related complications, were recorded. The incidence of complications was compared between the two groups.
Statistical Analysis
Statistical analysis was performed using SPSS17.0. Measurement data are expressed as the mean ± standard deviation (x ± s). The t test of independent samples was used to compare the imaging parameters between the tandem GR group and the control group. The paired samples t test was used to compare the imaging parameters between the tandem GR at the different follow-up nodes. Statistical data were compared using the chi-squared test. P < .05 were considered statistically significant.
Results
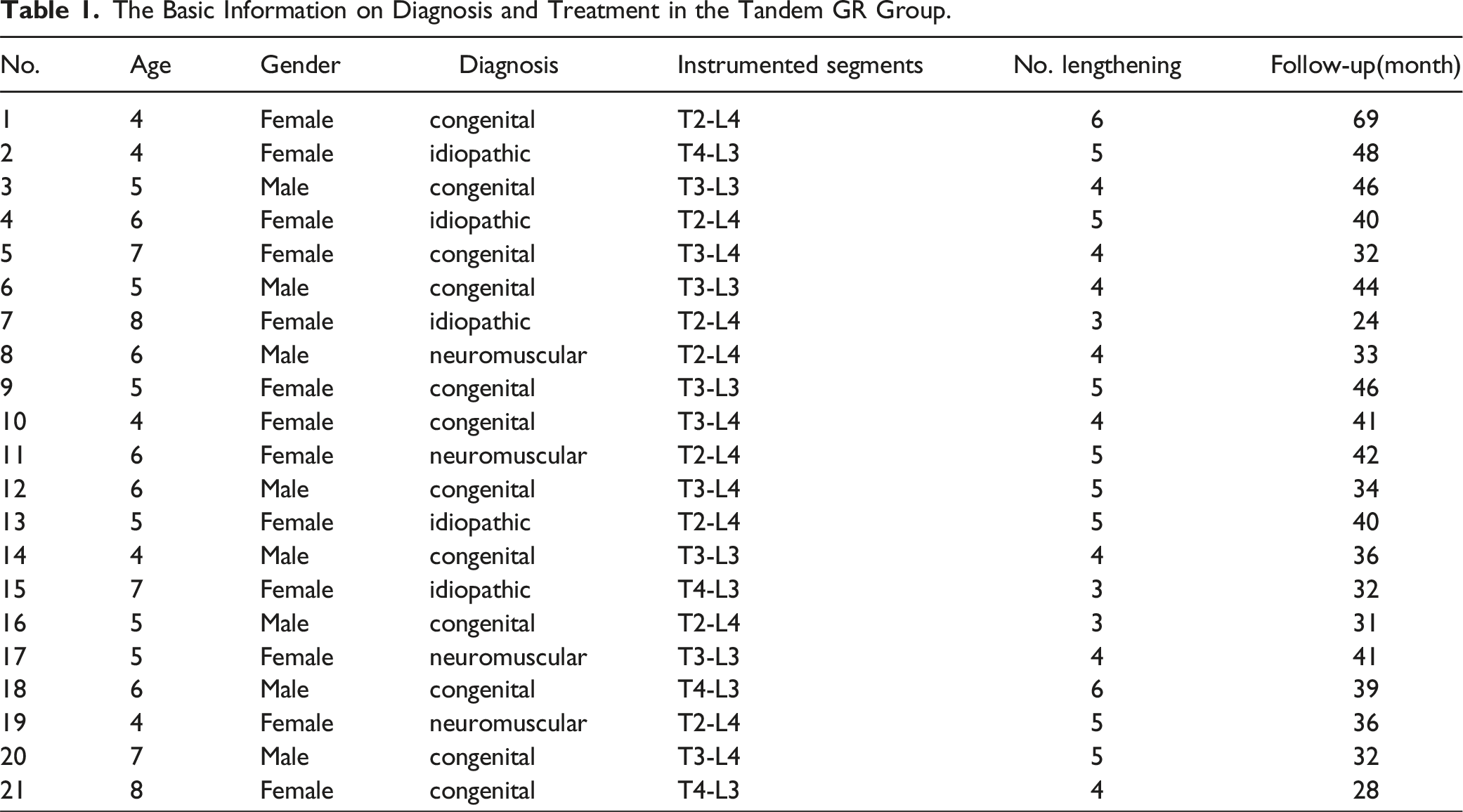
The Basic Information on Diagnosis and Treatment in the Tandem GR Group.
Preoperative and Postoperative Imaging Parameters of Patients in the Tandem GR Group.
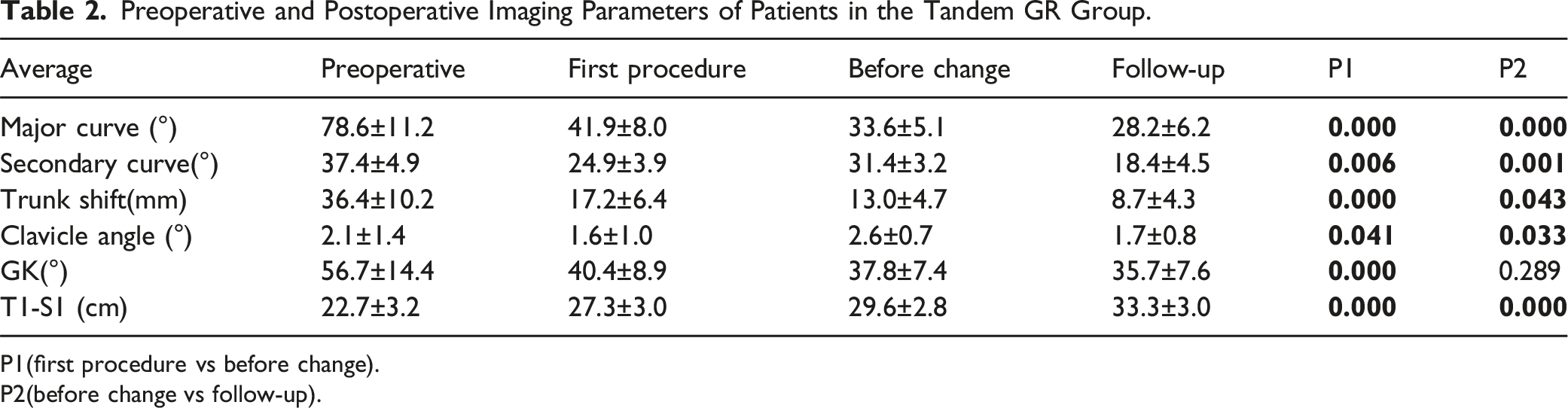
P1(first procedure vs before change).
P2(before change vs follow-up).
Then we studied the secondary curve and clavicular angle in the tandem GR group. The secondary curve progressed from 24.9 ± 3.9° to 31.4 ± 3.2°(P = .006) before switching to the tandem GR and improved to 18.4 ± 4.5° (P = .001) after the change. Meanwhile, the clavicular angle changed from 1.6 ± 1.0° to 2.6 ± .7° (P = .041) before switching to the tandem GR and improved to 1.7 ± .8° after the change (P = .033) (Table 2). These results suggest that the new technique can reverse the progression of the secondary curve and can maintain the balance of the shoulders.
In the control group, the major curve was 81.7 ± 17.1° before treatment, 44.3 ± 13.7° after the first operation, and 30.6 ± 7.8° at the end of the follow-up. The difference between the three points was significant (P = .000). The secondary curve was 35.6 ± 6.7° before treatment, 22.6 ± 7.8° after the first procedure, and 29.1 ± 8.3° in the follow-up. Moreover, the differences between the three points were significant. This indicates that the secondary curve was not been effectively corrected during the treatment procedure, and the last follow-up was worse than the first procedure. Trunk shift changed from 40.1 ± 11.2 mm preoperative to 12.7 ± 7.3 mm after the first operation and improved to 10.4 ± 3.5 mm at the end of the follow-up. T1-S1 height increased from 23.7 ± 5.1 cm to 27.1 ± 5.3 cm after the first operation and improved to 28.2 ± 4.8 cm at the follow-up, with an average growth rate of 1.0 ± .3 cm/year. And the mean number of lengthening was 4.2 ± .7. A comparison between the tandem GR group and the traditional GR group was made, and the imaging parameters showed no significant difference preoperatively and after the first procedure (P > .05). However, at the end of the follow-up, the secondary curve in control was higher than that in the tandem GR group (27.1 ± 8.3° vs 18.4 ± 4.5, P = .034), the clavicle angle in control was higher than that in the tandem GR group (2.4 ± 1.1° vs 1.7 ± .8, P = .028), and the T1-S1 height in control was lower than that in the tandem GR group (28.2 ± 4.8 vs 31.3 ± 3.0 cm, P = .027) (Figure 2). After conservation, the average growth rate was 1.0 ± .3 cm/year in the control and 1.2 ± .4 cm/year in the tandem GR group (P = .046) (Table 3). There was no difference the number of lengthening between the two groups (4.4 ± 1.1 vs 4.2 ± .7, P = .075). Compared with the traditional technique, tandem GR can effectively control the progression of the secondary curve, improve coronal balance, and allow the spine to retain better longitudinal capacity. (A) The Cobb angle of the major curve in the two groups during the follow-up. (B) The Cobb angle of the secondary curve in the two groups during the follow-up. (C) The clavicle angle in the two groups during the follow-up. (D) The T1-S1 height in the two groups during the follow-up. The Comparison Between the Tandem GR Group and the Control.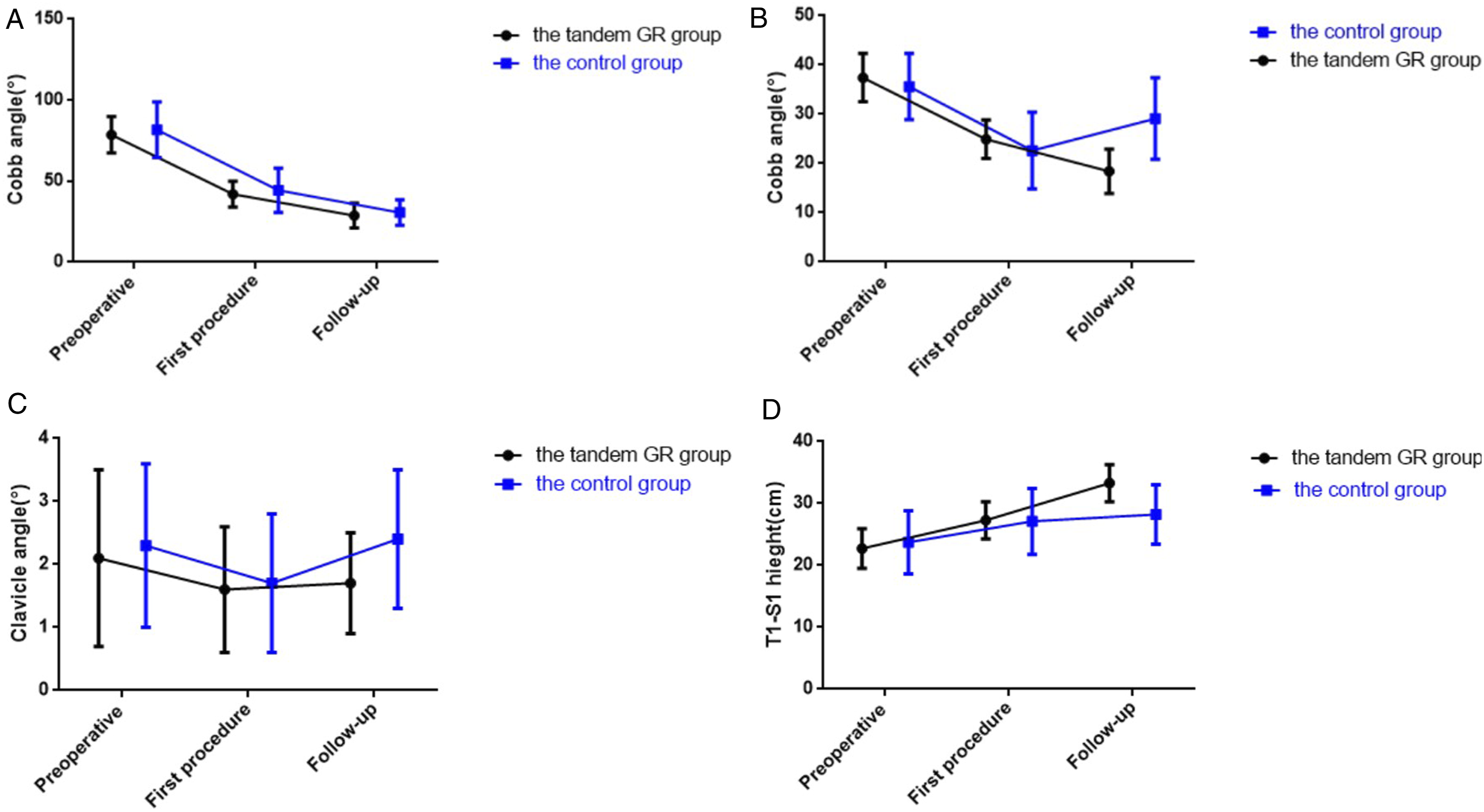
There were no significant differences in postoperative complications between the two groups. In the tandem GR group, two patients developed wound infections after lengthening, and the wound healed after debridement and drainage. One patient had a broken rod replaced during the next lengthening procedure. Further, two patients developed wound infections in the control group, and three cases experienced rod breakage. No nerve injuries or other complications were observed in either group.
Discussion
The purpose of GR is to control the progression of scoliosis while maintaining the growth capacity and mobility of the spine. However, some problems persist in the traditional technique, such as insufficient orthopaedic ability, poor secondary curve control, and a higher rate of unplanned reoperation.15-18 In this study, we developed a modified technique based on traditional GR. We modified the technique by using two sets of GR devices to control the major and secondary curves and connected the two groups of devices in series. Finally, our study confirmed that tandem GR can improve the proximal upper thoracic curve progression in the treatment of EOS.
The clavicular angle often changes during the multistep lengthening process, and the final result is unpredictable. Liu et al 8 found that early shoulder imbalance (OR = 19.500, P = .015) was an independent risk factor for final shoulder imbalance. Therefore, adjusting the shoulder balance during the lengthening procedure may improve the overall treatment effect. 19 The new technique provides a more powerful distraction effect and a more flexible adjustment strategy for the proximal upper thoracic curve. In this study, the clavicular angle improved from 2.6 ± .7° to 1.7 ± .8° after the switch. At the end of the follow-up period, the clavicular angle was smaller than the control. Both results verified the effectiveness of tandem GR in controlling shoulder balance.
The secondary curve is usually non-structural and has limited progression. However, some cases progress during the lengthening procedure. In this study, 51 secondary curve progression cases were included, accounting for 21% of all patients treated with GR. Skeletally immature patients, Cobb angle ≥44.5°, and double curves were risk factors for the progression of the secondary curve.20-22 Progression of the proximal upper thoracic curve may result in coronal imbalance and early termination of the GR, leading to premature spinal fusion or limited longitudinal growth of the spine. Before switching to the tandem GR, the secondary curve progressed from 24.9 ± 3.9° to 31.4 ± 3.2°(P = .006) and improved to 18.4 ± 4.5°(P = .001) after the change. This validates that tandem GR can effectively control the progression of the secondary curve.
The optimal age for GR is 5 to 10 years.23,24 In the past, it was often considered that the spine of children is in a period of slow development. 25 However, recent research suggests that scoliosis is also likely to progress between the ages of 5 and 10 years. 26 According to Lenz et al, 27 age of less than 10 years and multiple curves constituted patient-specific risk factors for curve progression. This is consistent with the clinical characteristics of the patients in our study, and the modified technique may be more appropriate in cases of severe malformations.
The proximal upper thoracic curve have continued exacerbation at the end of follow-up. The secondary curve progressed from 22.6 ± 7.8° to 29.1 ± 8.3° from the first procedure to the end of the follow-up in the control group, which means that in such a situation, the traditional GR cannot control the secondary curve (Figure 3(A)–(F)). Many studies have confirmed that in the major left thoracic and left lumbar curve types, initial minor curves progressed faster than major curves.28,29 Pizones et al
30
summarised the experience of GR in the treatment of EOS with curve progression, wherein 12 of 13 patients developed thoracic curve progression, all of whom had to stop GR treatment early and undergo osteotomy in the terminal surgery. (A) A 4-year-old boy with congenital scoliosis. This is the posterior-anterior X-ray images. (B) The lateral X-ray images before surgery. (C) After the first procedure with GR, and the secondary curve is 26°. (D) After the third lengthening, the curve progressed to 38°. (E) After switching to the tandem GR, the curve corrected to 22°. (F) At the last follow-up, the secondary curve is 16°.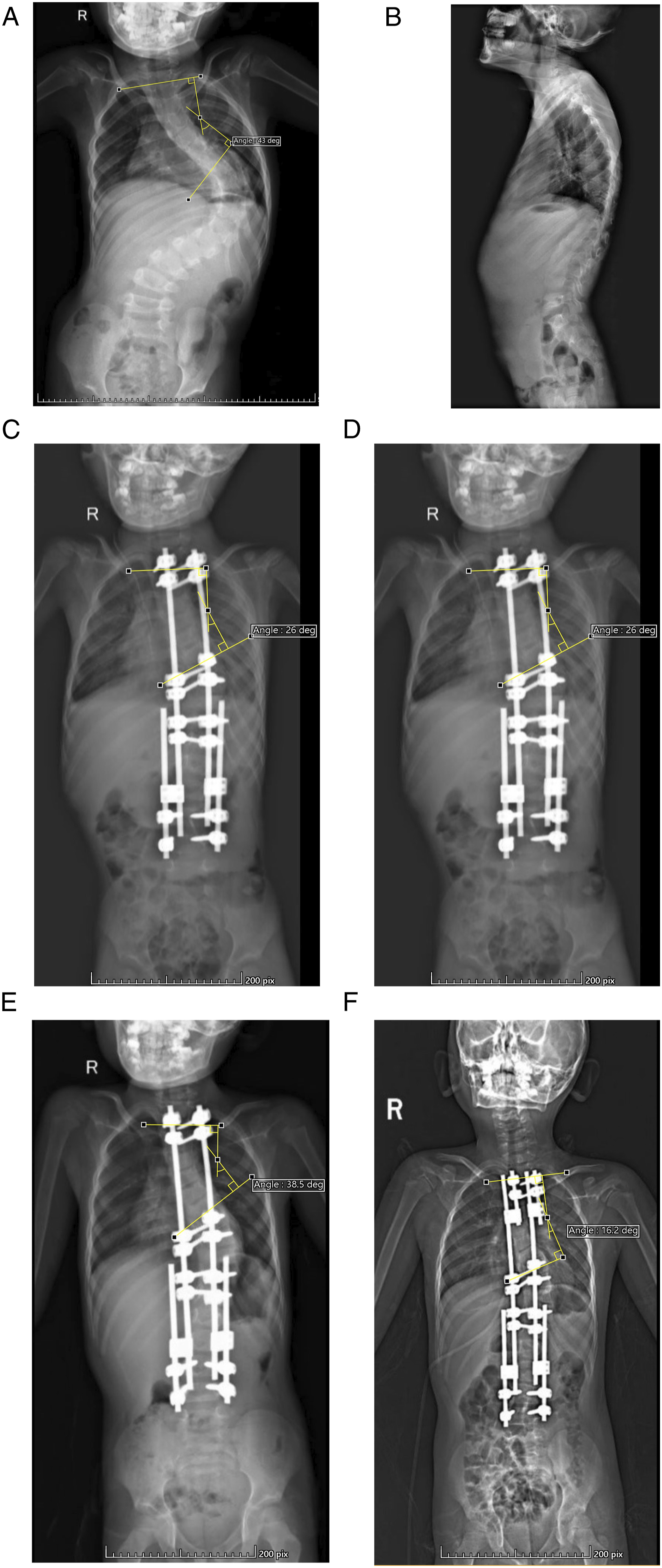
The height of TI-S1 in the tandem GR group was higher than that in the control group, which was an impressive finding. This may be due to the following two reasons: first, good control of the secondary curve may reduce the loss of spine height due to scoliosis. Second, the two sets of devices in the tandem GR group provided a greater tensile force when performing lengthening operations. Duisun et al 31 reported that bringing the apex in line with the GR increases the capacity for growth preservation, resulting in the largest height gain and better deformity control. This may partially explain our results. Urbanski et al 32 concluded that T1-S1 length was higher in the dual-rod group than in the single-rod group. They believe that an extra rod can lengthen the spine.
Tandem GR has many advantages over the traditional technique. Firstly, the curve correction ability is stronger. The principle of traditional technique is to apply traction between proximal and distal anchors joined by expandable rods. However, due to the limited power of distraction, it often only has a certain correction effect on the major curve.33,34 After the improvement, the effect of the distraction force equilibrium on the primary and secondary curves. Brooks et al 35 confirmed that the higher the correction rate, the better the terminal outcome. Secondly, the second device can be planted with a small incision rather than a complete replacement. In the past, the entire device out had to be taken out to adjust the GR. Thirdly, compared with the traditional technique, tandem GR allows the spine to retain better longitudinal capacity.
In this study, one patient in the tandem GR group and two patients in the control group developed implant-related complications. The rates of these complications were 4.8% and 6.7%, respectively, which were higher than that in previous studies. 36 Therefore, the higher complication rate may be related to all patients enrolled in this study having severe scoliosis. In addition, the mean age at initial surgery was only 5.5 years old, which means that the spine has more significant growth potential.
Our study still has limitations. Firstly, the number of cases enrolled was limited, and the clinical outcome of the technique was only preliminaries reported in this study. Secondly, all patients did not undergo terminal surgery. However, it is worth emphasising that at the end of the follow-up, the average age of the tandem GR cases was 9.1 ± 1.4 years old, which is close to the maximum age of GR. We believe this result is sufficient to prove the validity of tandem GR. Finally, with the progress of material science and manufacturing technology, the traditional GR device can be modified to achieve better curve correction and more flexible use strategies.
Conclusion
Tandem GR can effectively improve the proximal upper thoracic curve progression during the treatment of EOS. Compared with the traditional GR, tandem GR can achieve better curve correction, better shoulder balance, and retains more capacity for longitudinal spine growth.
Footnotes
Author Contributions
Weiran Hu and Xiaonan Wu, analysis of data, drafting and revising manuscript, and final approval. Guang Yang, design, acquisition, analysis of data, drafting and revising manuscript, and final approval. Haohao Ma, Hongqiang Wang, data collection and final approval. Yanzheng Gao, conception and design of work, drafting and revising manuscript, and final approval
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Henan Provincial Medical Science and Technology Tackling Program Joint Project (LHGJ20200047), the Henan Provincial Medical Science and Technology Tackling Program Provincial-Ministerial Co-construction Project (SB201901085), and the Henan Provincial Medical Science and Technology Tackling Program Provincial-Ministerial Co-construction Project (SBGJ2018076).
Data Availability Statement
All of the data are described in the manuscript. The datasets used and/or analyzed in the present study are available from the corresponding author upon reasonable request.