
Abstract
Study Design:
Retrospective study.
Objectives:
This study retrospectively evaluates the outcome of the surgical treatment of early-onset scoliosis with proximal clawing rib fixation in hybrid growing-rod constructs. The study examines spinal deformity correction with spinal growth maintenance, and the complications associated with this technique.
Method:
A hybrid rib construct surgery with serial lengthening was utilized for the treatment of 71 patients. Mean age at surgery was 66.6 months and mean time for follow-up was 43.9 months.
Results:
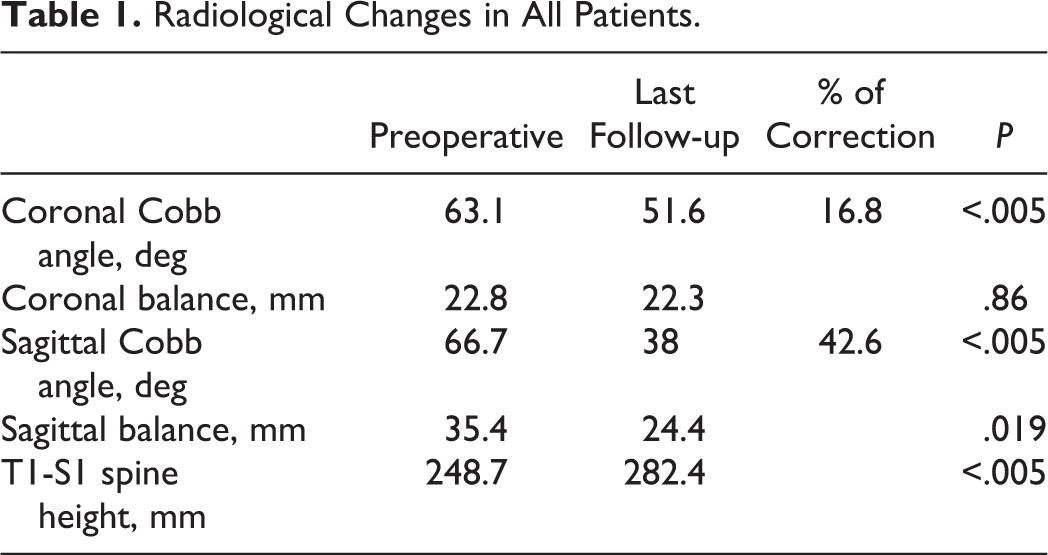
The coronal Cobb angle in patients fell from 63.1° preoperatively to 51.6° at the last follow-up, with a correction of 16.8%. The sagittal Cobb angle fell from 66.7° preoperatively to 38° at the last follow-up, with a correction of 42.6%. Coronal balance fell from 22.8° preoperatively to 22.3°, and sagittal balance fell from 35.4 mm preoperatively to 24.39 mm. T1-S1 spine height increased from 248.7 mm preoperatively to 282.4 mm, with a mean change of 1.13 cm per year. No neurological complications were detected.
Conclusion:
Surgical management for early-onset scoliosis using proximal clawing rib fixation technique is a good choice in terms of safety, ease of placing the proximal anchors, ability to use more than one form of instrumentation, and a lower complication rate.
Introduction
Early-onset scoliosis (EOS) is a complex pathology that comprises a variety of etiologies, including idiopathic, neuromuscular, syndromic, and congenital types, with onset occurring before the age of 10 years. Ideally, the surgical management of EOS has the objectives of achieving the optimal pulmonary function and spine length, with minimal hospitalizations, complications and family burden. 1
Technological developments have significantly improved the growth-friendly spinal implants. Safety and efficacy of growth-friendly techniques in the treatment of EOS in addition to improvements in the quality of life have been documented in the literature. 2 -5 Different proximal anchoring implants are typically used in distractive based ones, including rib hook anchors, and spinal-based screws. However, there is limited data in the literature about the biomechanical and clinical outcomes of each.
In this article, we demonstrate our own experience in the treatment of EOS through a fusionless surgical construct that involved the use of distractive-based system of dual rods attached to proximal clawing rib-hooks anchors, and distal spine/pelvic screws. The modified rib hook technique demonstrated here indicates a reasonable amelioration of construct stability, correction of coronal scoliosis and kyphosis curves, with minimal complications aside from its unparalleled unique role in correcting kyphotic deformities. The implication is that proximal clawing rib hook anchors are a favorable biomechanical and clinical implant in EOS.
Method
This was a retrospective study of 71 children who underwent spinal growing rod implantation surgery from 2008 to 2015, for which institutional review board approval was obtained. The inclusion criteria were children who had growing rod implants with proximal clawing hook anchors for surgical treatment of EOS, with a minimum of 2 years of follow-up from index surgery. The exclusion criteria were children who had proximal spine anchors other than clawing rib hooks and or with less than 2 years of follow-up.
The retrospective review included age at initial surgery, diagnosis, coronal and sagittal Cobb angle, levels instrumented, type of instrumentation, number of surgeries, number of lengthenings, implant metal type, rod diameter, anchor types, and complications.
Of the 71 patients with EOS, 64 had scoliosis or kyphoscoliosis while 7 had kyphosis. The mean age at surgery was 66.6 months and the mean follow-up period was 43.9 months.
Surgical Technique
Preoperatively, multidisciplinary involvement is vital to address any possible associated medical and surgical problems, in addition to optimizing nutritional status. In addition, full anteroposterior and lateral views x-rays are needed for surgical planning, with spine MRI to evaluate the presence of spinal pathology.
The operation is performed under general anesthesia, with the patient in the prone position. A straight longitudinal midline incision is performed from T2 downward. Then, the attached edge of the trapezius and rhomboidus major is dissected extraperiosteally and distracted laterally. Erector spinae muscles are also distracted laterally and exposed to the rib extraperiosteally.
Laminar hooks are used as anchors preferably beginning from second rib, placing at least 5 hooks according to Miller and Vitale 6 for better stability of the anchors proximally. The hooks are put in clawing fashion with 2 proximal hooks facing downward and 1 or 2 distal hooks facing upward (demonstrated in Figure 1) to increase the stability proximally specially with thoracic kyphosis. 7 (Figure 1).
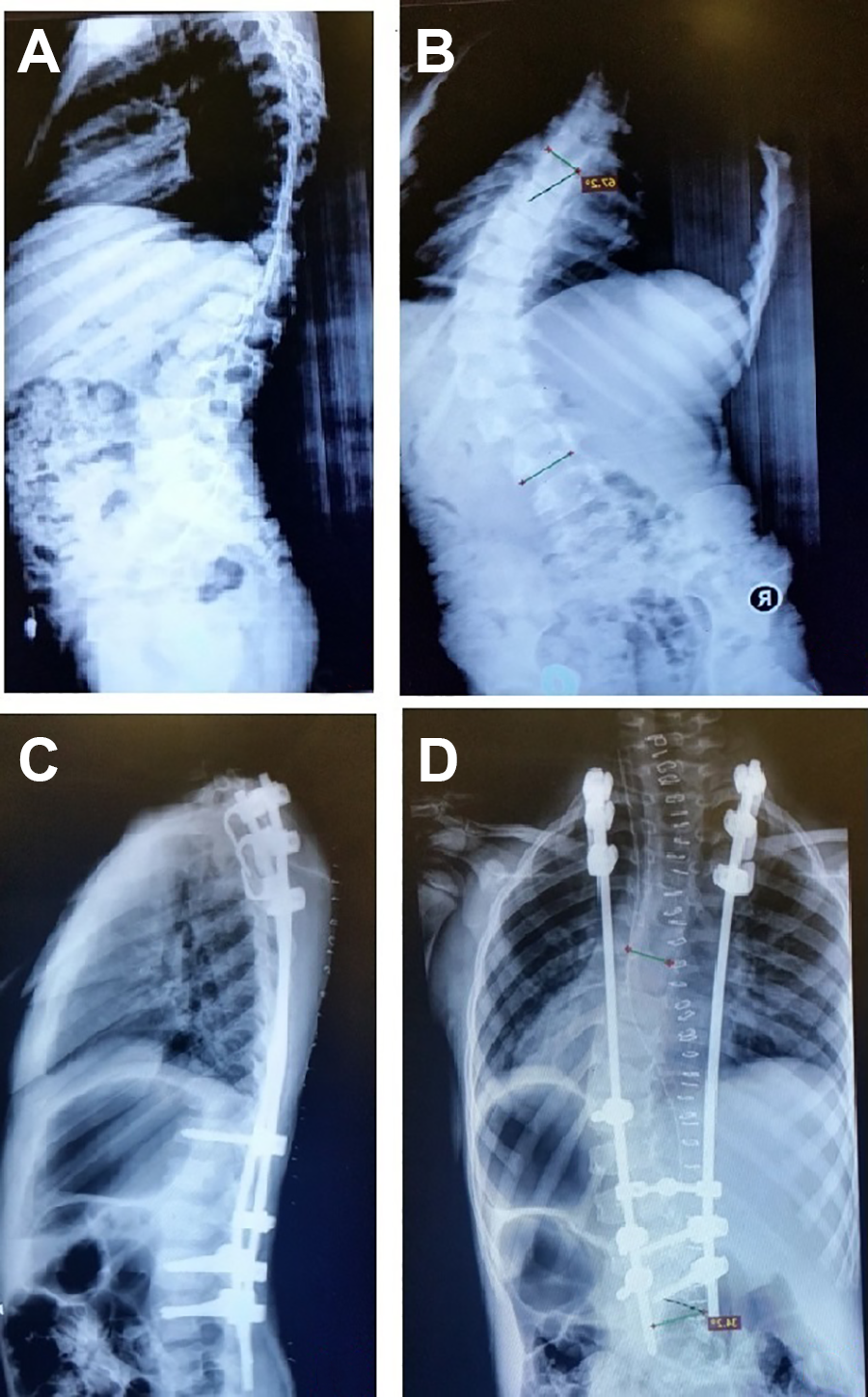
(A and B) Preoperative anteroposterior and lateral x-rays for early-onset scoliosis. (C and D) Postoperative x-rays for proximal fixation with 3 clawing hook construct beginning with second rib with the proximal 2 hooks facing downward and the distal one facing upward.
Distally, screws are put in the lumbar spinal segment or the iliac part. An appropriately determined length, 4.5 titanium rod, is selected, contoured to maintain the adequate sagittal planes in the thoracic and lumbar regions locked with all the anchors. Correction is maintained through the cantilever effect, especially in kyphosis, which prevents the possibility of hook dislodgment. Two centimeters of the rod is preserved and locked distal to the distal anchors for future lengthening. C-arm and neuromonitoring need to be used in all cases.
Mobilization is not restricted postoperatively, and postoperative lengthening is performed every 6 to 9 months. The lengthening procedure includes the following steps. First, the rods are lengthened by unlocking and distracting the distal screws distally (through the previously preserved 2 cm), which usually takes 1 or 2 lengthening times. Then, the rods were changed distally, and the proximal rod was engaged with the distal one by domino for lengthening. The incorporation of Dominos is done in lengthening surgeries but not in the first “index” surgery; this is because we think that correction is best done in the 1st surgery by using the rod without dominos. The patients need full-length spine radiographs in the coronal and the sagittal views standing or sitting preoperatively, postoperatively, and in follow-up sessions.
Results
In patients who had scoliosis/kyphoscoliosis deformity, preoperatively, the coronal Cobb angle was 63.1° and fell to 51.6° at last follow-up; with 16.8% correction. In patients who had kyphosis, Cobb angle was 66.7° and fell to 38° at the last follow-up; with 42.6% correction.
Sagittal balance was 35.4 mm and fell to 24.39 mm at the last follow up, while coronal balance fell from 22.8° preoperatively to 22.3° at the last follow-up.
The T1-S1 spine height of all patients averaged 248.7 mm preoperatively and rose to 282.4 mm at the last follow-up, with a mean change of 1.13 cm per year (Table 1).
Radiological Changes in All Patients.
Complications
Our experience with rib-based proximal clawing hook anchors revealed that out of 71 patients with EOS, 24 (33%) had 44 complications: 2 incidents of broken rod, 1 urinary tract infection, 1 domino movement, 9 distal screw dislodgment, 6 superficial skin infection postoperatively, 6 proximal hook dislodgments, 5 screw or rod protrusion through skin, 1 dislodgement of proximal screw after final fusion, 1 rib fracture, 1 shoulder bursitis, and 1 superior mesenteric artery syndrome.
The best results were idiopathic ones (8 cases with no complications) while the worst were neuromuscular (8 out of 11 cases, or 73%).
Complications were most common in kyphosis cases with 5 out of the 7 cases (71%) experiencing complications.
Discussion
The proper surgical treatment and continuous follow-up of EOS is crucial for correcting the spinal deformity and preventing catastrophic consequences related to cardiopulmonary functions. With the evolution of many fusionless surgical techniques, the main constructs introduced were distraction based and growth guided systems.
In fusionless surgical techniques, proximal implants bear the entire mechanical load during the treatment period, increasing the risk of implant failure compared to spinal fusion in adolescent idiopathic scoliosis. 6
Applying pedicle screws in proximal thoracic vertebrae can be challenging with abnormal morphology in these vertebrae. 6 Additional concerns of pedicle screws use in young children arise from their smaller pedicular anatomy and suboptimal bone quality.
Vitale et al 16 report a comparison between 73 patients with EOS who had rib-based proximal anchors and 33 who had spine-based proximal anchors. After an average follow-up of 1.16 years, no significant difference in spinal curve correction (29% vs 36% correction) was found between rib and spine anchor groups. 16 Despite this, many publications documented biomedical and clinical advantages of the rib hook construct. 7
The main biomechanical advantage is due to motion at rib hook interface. This makes the system less rigid and decreases the incidence of autofusion, with one-fourth less risk of rod breakage compared with spine anchors. 13 Clinical advantages are related to the easiness of putting the hooks proximally with better soft tissue coverage without the need of fluoroscopy. These distraction devices are neurologically safer and decrease the incidence of upper thoracic segment fusion (T1-3) done in traditional growing rods systems. 5,6,11,12
Clawing proximal rib construct technique results for 2 cases with thoracic kyphosis was first published in 2012 with good results. 7
In this study, we demonstrate our experience in the treatment of EOS through the same proximal anchor’s technique.
Our construct uses a distractive-based system of dual rods attached to proximal clawing rib-hooks anchors, and distal spine/pelvic screws. The hooks were placed in clawing fashion with 2 proximal hooks facing downward and 1 or 2 distal hooks facing upward, increasing the stability proximally and especially with thoracic kyphosis.
We realize that the results of the spine correction are comparable to other studies regarding the correction of scoliosis curve. However, this modified hybrid rib construct allows for a simultaneous correction of scoliosis and kyphosis curve. The reduced correction rate in scoliosis curve can be accepted since we are preventing curve progression in EOS, in comparison to correction with fusion in adolescent idiopathic cases.
Though EOS with kyphosis may worsen with continuous distraction, 17 using this technique yields statistically significant correction of kyphosis and sagittal balance. The mean kyphosis was corrected by 42.6%, from approximately 67° to 38°. This is likely due to better soft tissue coverage, which decreases implant prominence, and better fixation points (at least 6) in clawing fashion (Figure 2). The technique further produces better rib fixation than transverse process or lamina in weak bones, which are quite common in these patients (Figure 2).
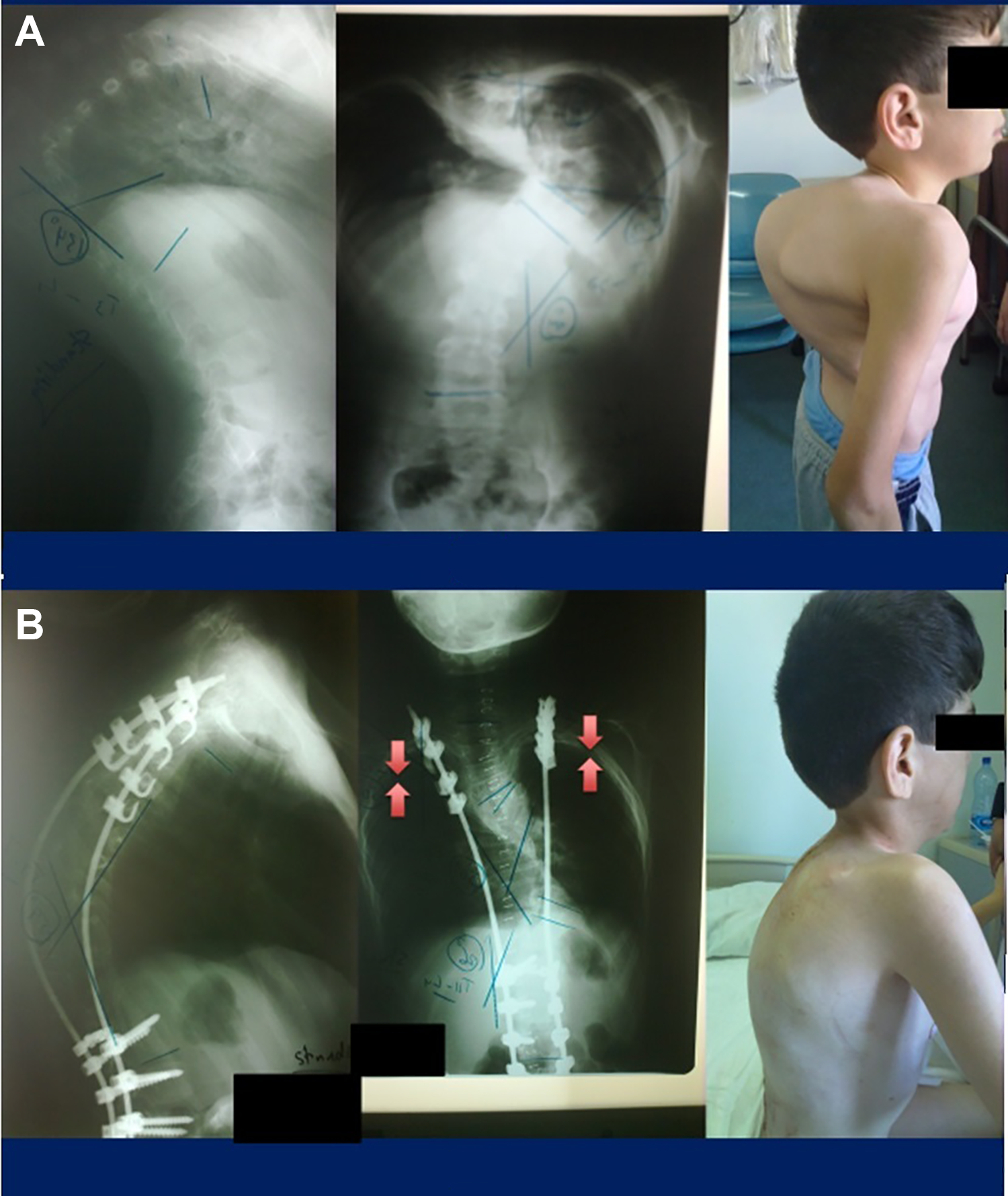
(A) Preoperative picture and x-rays of severe kyphoscoliosis in a 9-year-old child. (B) Postoperative correction of severe thoracic kyphosis from 134° to 59° by hook rib clawing with cantilever effect.
The results further indicate that there was no significant difference in the results of the 3 and 4 rib constructs, which corresponds with Vitale et al 16 point about putting 5 anchors. For this reason, we switched to 3 rib constructs in each side in the same clawing fashion, with 2 hooks proximally facing downward and a distal hook facing upward
The EOS surgical treatment has a wide range of well-known complications. Studies have reported the rate of complications in growing implants to be between 0.38 and 1.19 per patient. 2,3,8 -10 Rib-based distraction devices share many complications with other growth friendly implants, and have additional unique problems such as rib fracture, brachial plexus injury, chest wall problems and rib fusion. 17
Acknowledging complications in our study, only 44 complications occurred in 71 patients, representing a complication rate of 61.9%. This compares favorably with the 23 complications in 10 patients (complication rate of 230%) in standard dual growing rods as reported by Sankar et al 14 and is similar to the rate of 13 complications in 23 patients (57%) in patients treated with standard dual growing rods as reported by Akbarnia et al. 3 Furthermore, rod breakage occurred in 2.8% for this technique, compared to 28.9% in spine-based construct according to Yamaguchi et al. 13 Regarding the implant related failure, 16 dislodged implants occurred with a dislodgment rate of 22.5% compared with 50.1% in growing rod surgery as reported by Liang et al. 15
With regard to complications regarding the etiology, the neuromuscular cases are the highest in complications. We believe this is related more to the general condition of the patients than to the type of anchors (Table 2).
Data Regarding the Etiology.

The highest rate of complications is in kyphotic deformity related to the curve type, but it is accepted acknowledging the severity of the curve and the good correction (Table 3).
Data Regarding Deformity Type.

The study has some limitations, despite the good number of patients with more than 3 years of follow-up. It is a single center study with limited follow-up time, which might not be reflective of the true complication rate in the long run, especially for graduate patients. Furthermore, bending tests were not performed for most of the patients, which does not give the effect of flexibility of the curve on the results. Finally, we do not possess data about the pulmonary function progress for these children because of the lack of facilities and human resources that are needed for this type of study.
Conclusion
The 3-4 rib construct in clawing fashion technique would be a good choice for early onset scoliosis surgical management. Advantages include safety, ease of putting the proximal anchors, ability to use more than one form of instrumentation, and a relatively low complication rate. These findings may advocate the use of proximal rib hook anchors over the use of spinal-based screws in patients with EOS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.