
Abstract
Study Design
Retrospective Cohort Study.
Objectives
The objective of this study was to assess the impact of diet liberalization on short-term outcomes in patients undergoing anterior interbody lumbar fusion (ALIF).
Methods
A retrospective review was performed for patients undergoing ALIF at our tertiary care center institution from 2010 to 2022. Electronic medical records were reviewed for demographics, surgical characteristics, and 90-day postoperative outcomes.
Results
We included 515 patients in this study with 102 patients receiving a full diet on the same day as their operation. All other patients had a delay of at least 1 day (average 1.6 days) until a full diet was provided. This group was found to have a higher rate of postoperative ileus (10.2% vs 2.9%) and urinary retention (16.0% vs 3.9%). The readmission rate and percent of patients presenting to the emergency department within 90 days postoperatively were similar. On multivariate regression analysis, same-day, full-diet patients had decreased odds of developing urinary retention (OR = .17) and a shorter length of hospital stay (Estimate: −.99). Immediate full diet had no impact on the development of ileus (OR: .33).
Conclusions
An immediate postoperative full diet following an anterior approach to the lumbar spine was not found to be associated with an increased risk of postoperative ileus in patients deemed appropriate for early diet liberalization. Moreover, an early full diet was found to reduce length of hospitalization and risk of postoperative urinary retention. Reconsideration of postoperative diet protocols may help optimize patient outcomes and recovery.
Introduction
Anterior lumbar interbody fusions (ALIF) provide surgeons with powerful lordosis correction and indirect decompression opportunities, but the approach comes with the potential risk for injury to the nearby vascular and visceral structures. Inherent with this technique is the risk of postoperative ileus (POI), reported between 3% and 6%, and colonic perforation due to proximity of intra-peritoneal structures. 1 After an ALIF, some surgeons prefer to prescribe patients a stepwise progression of clear liquid diet, soft diet, and then full diet. In contrast, some surgeons prefer to clear patients for a full diet in the immediate postoperative setting. To date, there has been limited evaluation on the impact of early full diet vs a restricted diet and its effect on postoperative outcomes following ALIFs.
One of the most critical portions of the postoperative period for enhanced patient recovery centers around patient nutrition. However, a large percentage of the literature discussing nutritional optimization focuses on preoperative screening and prevention of malnutrition as opposed to postoperative recommendations.2-4 The Enhanced Recovery After Surgery (ERAS) initiative provides evidence-based and multidisciplinary perioperative care pathways aimed at decreasing the stress of surgery, optimizing physiologic function, and facilitating recovery. However, there exists a paucity of literature on ERAS protocols specific to spine surgery. Recommendations regarding nutrient content, and timing before and after surgery are evolving and not yet standardized.2,3,5
The purpose of the current study is to evaluate postoperative outcomes and complications, such as POI, length of stay (LOS), and urinary retention (POUR) based on diet status following anterior lumbar surgery. The findings of this study may serve to contribute to new spine specific ERAS protocols which can help surgeons and patients plan for optimization of the postoperative recovery period.
Materials and Methods
Following Institutional Review Board approval (Thomas Jefferson University, Office of Human Research Institutional Review Board, Approval #19D.508), a retrospective review was performed for all patients undergoing anterior lumbar interbody fusion (ALIF) and subsequent posterolateral fusion (PLF) or posterior lumbar decompression and fusion (PLDF) by 1 of 9 fellowship-trained spine orthopaedic surgeons from 2011 to 2022. Informed consent was waived by the IRB due to the retrospective nature of the study. Procedures occurred at 1 of 3 hospitals within a large, urban, academic hospital system. Patients were identified based on Current Procedural Terminology code 22558 for an anterior interbody fusion of the lumbar spine. Patients at least 18 years of age who underwent primary single or multi-level ALIF for degenerative spine disease were included in the study All ALIFs were performed via a retroperitoneal approach with an access surgeon assisting in exposure of the spine. Patients undergoing revision ALIF, surgical intervention for trauma, infection or malignancy, staged anterior and posterior procedures, and interbody fusions through a lateral approach were excluded from the study.
Electronic medical records for all patients meeting inclusion criteria were retrospectively reviewed for demographics (age, sex, body mass index (BMI), race, and ethnicity), comorbidities (Charlson Comorbidity Index (CCI), smoking status, and diabetes mellitus), prior abdominal and/or lumbar spine surgeries, surgical indications, and operative information (surgical duration and levels fused and decompressed). Prior gynecologic (ie, hysterectomy) surgeries were included within prior abdominal surgery given their association with postoperative adhesions and POI.6,7 Patients were divided into 2 cohorts based on postoperative diet: a control group who did not receive oral nutrition on the day of surgery and whose diet was advanced in a stepwise progression from clear to liquids to full diet, based on ability to pass flatus and tolerate oral diet (“Delayed Diet” group), and a study group whose diet was immediately liberalized postoperatively with oral nutrition appropriate for the patient’s medical comorbidities (“Full Diet” group). Length of stay (LOS), postoperative complications both in hospital and within 90 days of surgery, readmissions, emergency room visits, and revision surgeries were documented for each cohort. Consistent with previous literature, postoperative ileus was defined based on clinical diagnosis after consult for nausea, vomiting, or abdominal pain with confirmation on radiograph. 8 Patients had intraoperative foley catheters that were pulled on POD 1. POUR was identified by straight catheterization after surgery due to post void residual volume (PVR) of >400 mL, similar to previous literature. 9
Bivariate statistical analysis was performed between the “Delayed Diet” and “Full Diet” groups. Categorical variables were analyzed by Chi-Square or Fisher's Exact test while continuous variables were analyzed by t test or Mann-Whitney U test. Multivariate logistic regression analyses were performed for predictors of POUR and POI. Multivariate linear regression was performed for predictors of length of hospital stay. All statistical analyses were performed using R Studio Version 4.0.2 (Boston, MA).
Results
Patient Demographics.
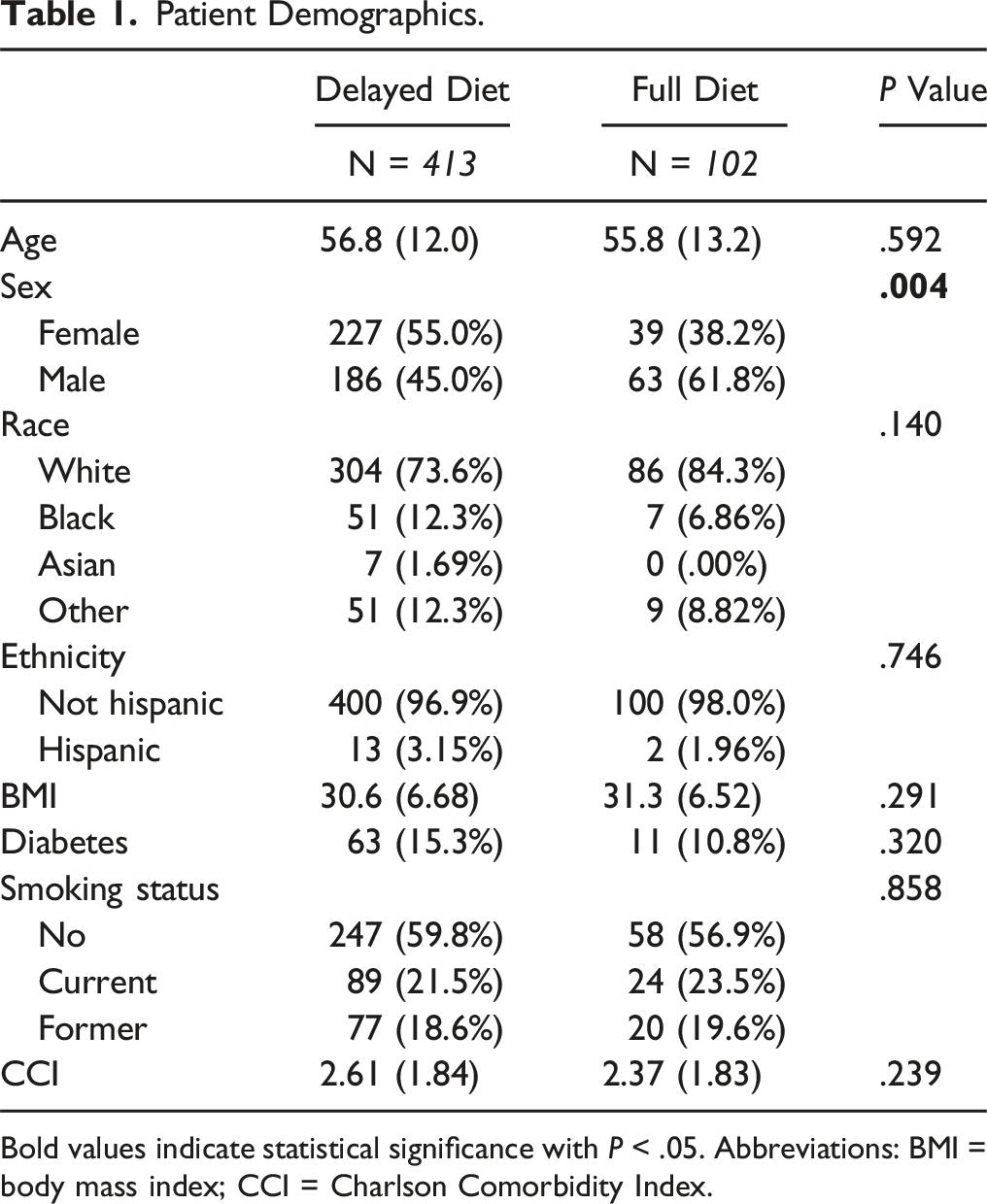
Bold values indicate statistical significance with P < .05. Abbreviations: BMI = body mass index; CCI = Charlson Comorbidity Index.
Surgical Characteristics.
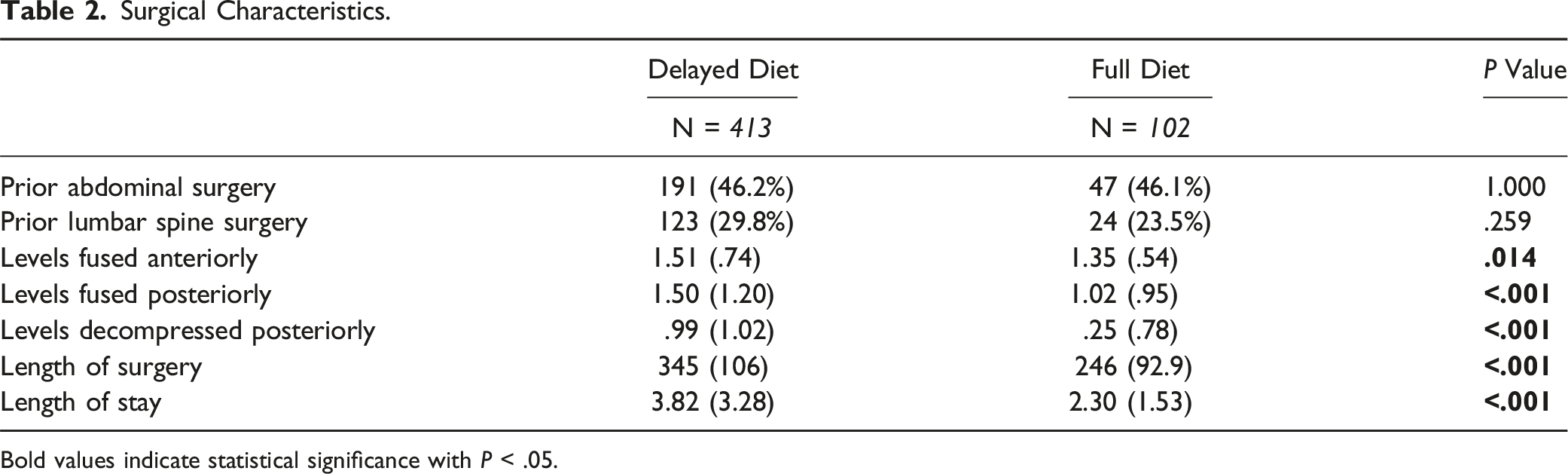
Bold values indicate statistical significance with P < .05.
Dietary Information.
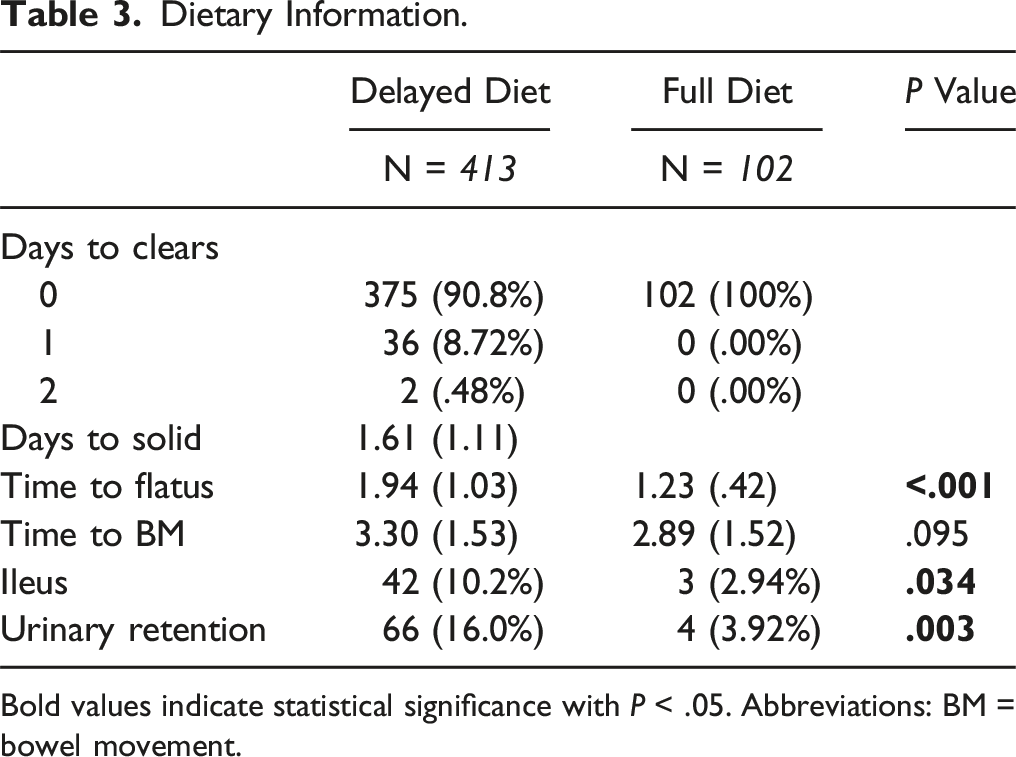
Bold values indicate statistical significance with P < .05. Abbreviations: BM = bowel movement.
90-day Postoperative Complications.
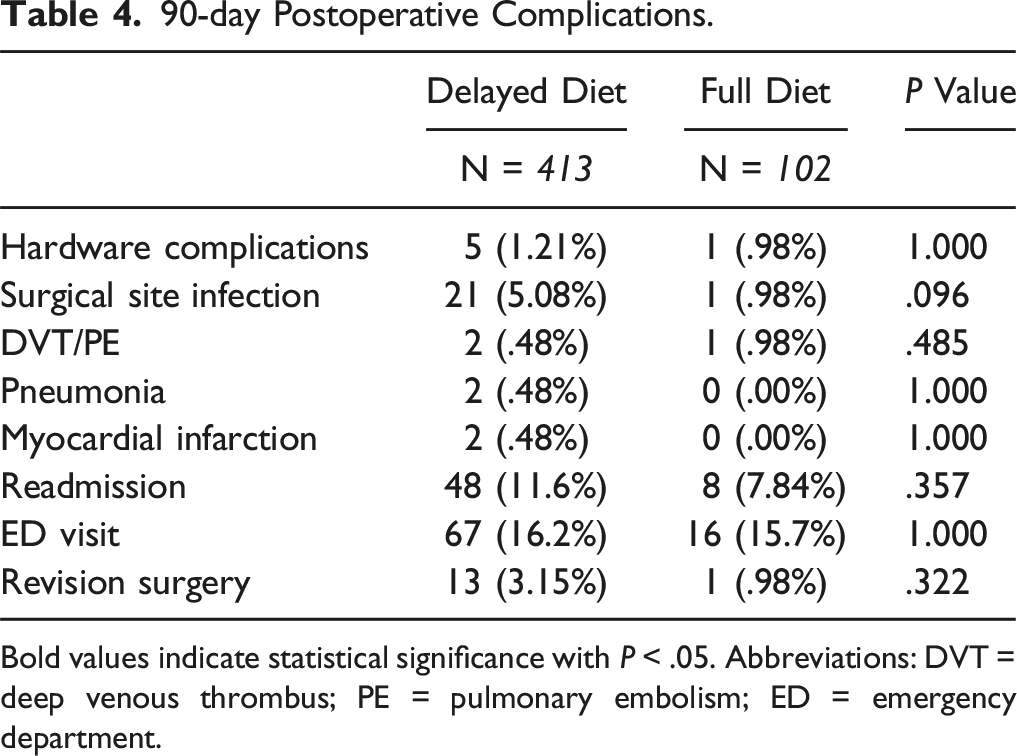
Bold values indicate statistical significance with P < .05. Abbreviations: DVT = deep venous thrombus; PE = pulmonary embolism; ED = emergency department.
Multivariate Regression Analysis.
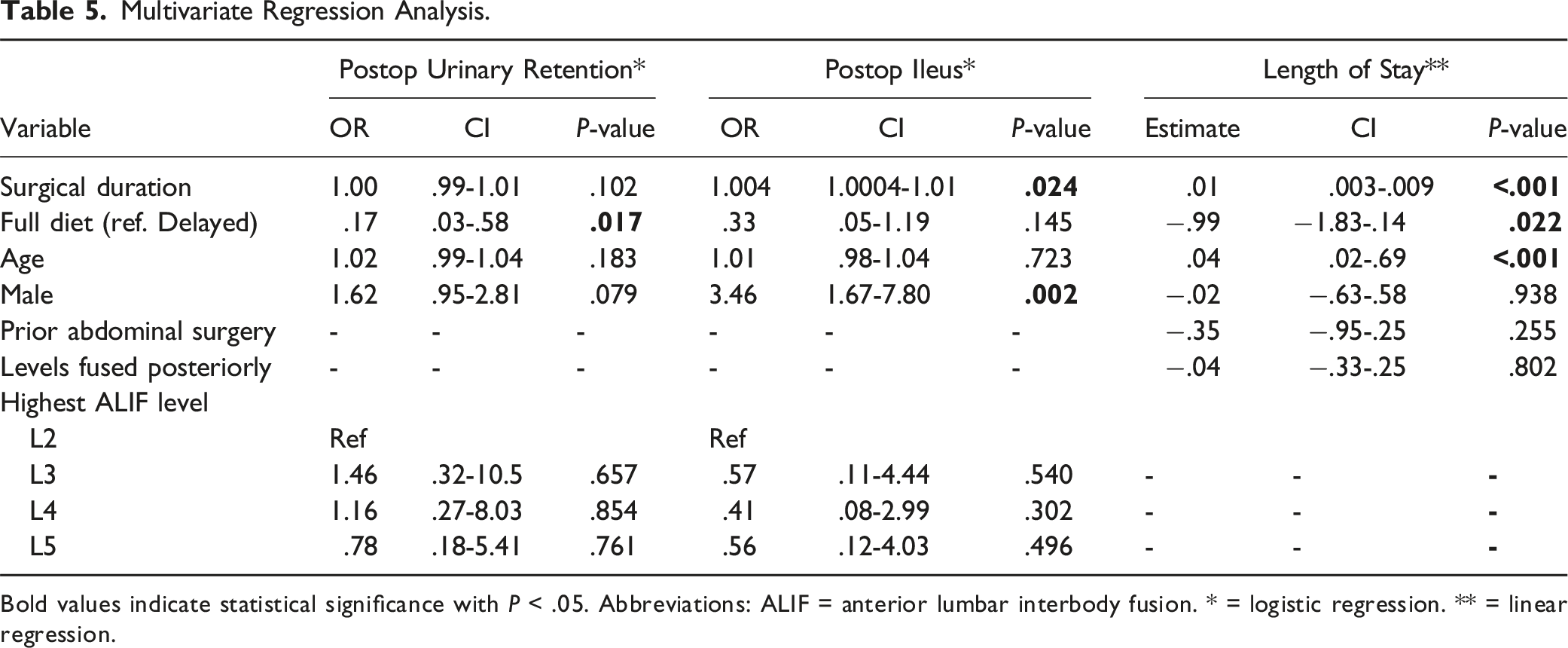
Bold values indicate statistical significance with P < .05. Abbreviations: ALIF = anterior lumbar interbody fusion. * = logistic regression. ** = linear regression.
Discussion
Currently, there is limited literature investigating postoperative diet following an anterior approach to the lumbar spine. The primary concern with initiating a normal diet in the immediate postoperative period is that patients undergoing an anterior approach may be at a higher risk for developing postoperative ileus (POI). 10 However, there is no literature associating immediate full diets with POI or other postoperative complications. Despite this, many surgeons still elect for postoperative diet restriction out of convention. The current study found that an immediate full postoperative diet was not associated with an increased rates of POI but it did significantly contribute to both decreased LOS and decreased rates of POUR.
Postoperative ileus is a multifactorial complication arising from intestinal manipulation. 11 Direct or indirect stimulation of the bowel during the anterior approach can in theory lead to an inflammatory cascade, inhibitory neural activation, and release of neurohumoral peptides which all contribute to impaired intestinal contractility.10-12 Rates of prolonged POI in patients undergoing abdominal surgery has been estimated to be around 9%, with rates of POI reported as high as 15.4% in patients undergoing colorectal surgery in a multicenter prospective study conducted by Venara et al13-15 Prior studies have estimated the rates of POI after ALIFs at 2% to 35.4% with institutional data and 4.9% to 7.5% in database reviews. Our study found a comparable POI rate of 8.7%1,10,16-18 Patients who develop POI had significantly longer LOS and higher cost of hospitalization, which further highlights the incentive to reduce rates of POI.10,16
Though conventional practice has emphasized restriction of oral intake postoperatively to allow the bowels to recover, this is at odds with more recent literature stating that enteral nutrition significantly lowers the incidence of POI after surgery.11,19 A central tenant of the Enhanced Recovery after Surgery (ERAS) protocol, which has shown improvement in postoperative recovery across numerous surgical subspecialties, is early resumption of oral intake after abdominal or colorectal surgery. 20 A study performed in a community hospital found significant reduction in POI from 13.2% to 2.5% in patients undergoing colorectal surgery after ERAS implementation. 21 In patients undergoing extensive rectal surgery, Boelens et al. found that those receiving enteral nutrition had significantly lower rates of POI and faster times to initial stool passage compared to those receiving parenteral nutrition. 11 Additionally, in 426 patients undergoing posterior thoracolumbar fusion, Deng et al. demonstrated that postoperative diet restriction of liquids and solids greater than 9 hours increased the risk of developing POI. 19 This is likely the result of immediate enteral nutrition dampening the inflammatory response to intestinal manipulation, thereby decreasing hypomotility. Our multivariate regression results echo this sentiment and suggest that immediate diet liberalization has no association with development of POI after ALIF in our cohort.
Patients undergoing ALIFs at more cranial levels may theoretically be at an increased risk of developing POI due to greater bowel manipulation, as surgery at more cephalad levels necessitates increased manipulation for adequate exposure of the spinal column. 12 Previous literature has demonstrated that lumbar spinal fusion of 3 or more levels significantly increases the risk of POI as compared to fewer fusion levels; however, interbody fusion of more cranial levels of the lumbar spine in isolation has not previously been shown to impact development of POI. 10 Our regression analysis similarly did not find the most cranial level to be an independent risk factor of POI. instead, only male sex (OR: 3.46) and surgical duration (OR: 1.0004) were found to be associated.
Given that postoperative diet restriction postpones solid food intake and tolerating a full diet is a prerequisite of discharge, an immediate postoperative full diet may affect hospital LOS. Early oral intake was found to shorten LOS by nearly a full day in 1 prospective trial of patients undergoing major abdominal gynecologic surgery. 22 A recent review of 6 randomized controlled trials also found shorter hospital stays in women who had early oral intake after abdominal gynecologic surgery, with no difference in nausea, vomiting, or development of postoperative ileus. 23 In the spine literature, implementation of ERAS in 114 patients undergoing transforaminal lumbar interbody fusion found a 1 day decrease in LOS compared to controls; however, this study did not specifically isolate early oral intake as the agent of change. 24 Our study demonstrated that immediate liberation of diet was associated with a decrease in LOS by 1.35 days. Other factors evaluated in the study that contributed to increased LOS were older age and duration of surgery.
Previous studies do not directly evaluate postoperative diet and POUR, but they do demonstrate that POUR is associated with numerous other operative and demographic factors. In a retrospective study of 397 patients undergoing elective spine surgery, an increased incidence of POUR was seen with longer operative times and increasing age. 25 Multiple studies also support advanced age as risk factors for POUR following general orthopaedic surgery, 26 elective lumbar spine surgery 27 and thoracic surgery.28,29 Sung et al. included 15,681 patients undergoing various orthopaedic procedures and found age (OR: 1.035) and male sex (OR: 1.522) to be associated with POUR. 26 Conversely, the retrospective study performed by Altschul et al. found, after controlling for BPH, an increased incidence of POUR in females compared to males. 25 Our own results found advanced age, male sex, and surgical duration were not independent risk factors for POUR. However, unlike the other studies which did not address postoperative diet, we found that immediate liberation of diet was shown to be protective against developing POUR (OR = .17). These findings may indicate that the same inflammatory cascade that can impair normal bowel function and cause ileus may contribute to urinary retention as well and further research will be needed to better understand this relationship.
Our study has several limitations which are mostly inherent to its retrospective design. First, the “Delayed Diet” group did not adhere to a strict dietary protocol other than postponing solids until at least postoperative day 1. Diet was advanced based on tolerance and time to passing flatus. We doubt this would meaningfully impact our results as we were comparing immediate liberalization of diet to any delay in diet postoperatively. This also represents a realistic control as diet advancement is typically based on these markers. Bowel regimens are standardized across all patients but medications may be titrated as necessary by the managing team based on postoperative course, which may introduce bias into our study. Pain management with opioid medication is also variable across our patient population, which could be a confounder. Postoperative mobilization information was not factored into this study and may represent a confounding factor. Finally, the retrospective nature of this study allows selection bias to influence our results; however, we utilized a multivariate regression model to control for potential confounders such as surgical duration, highest ALIF level, and levels fused. We are unable to report patient-reported outcomes due to the low response rate of our study population and lack of long-term follow up.
Conclusion
An immediate postoperative full diet following an anterior approach to the lumbar spine was not found to be associated with an increased risk of postoperative ileus in patients deemed appropriate for early diet liberalization. Moreover, an early full diet was found to reduce length of hospitalization and risk of postoperative urinary retention. Although more evidence is needed to support these finding, a reconsideration of postoperative diet protocols may help optimize patient outcomes and recovery. Future, prospective, randomized studies would be beneficial to mitigate selection bias and potentially identify which patients would be appropriate for early diet implementation after anterior lumbar interbody fusion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.