
Abstract
Study Design
Retrospective observational radiographic analysis.
Objective
Determine how single level lumbar interbody fusion (LIF) alters segmental range of motion (ROM) at adjacent levels and decreases overall ROM.
Methods
This study included 54 patients who underwent single-level anterior (ALIF, 39%), thoraco-LIF (TLIF, 26%), posterior LIF (PLIF, 22%), or lateral LIF (LLIF, 13%) (L2-3/L3-4/L4-5/L5-S1: 4%/13%/35%/48%). Segmental ROM from L1-2 to L5-S1 and the overall lumbar ROM (L1-S1) were assessed from preoperative and postoperative flexion-extension radiographs. K-means cluster analysis was used to identify ROM subgroups.
Results
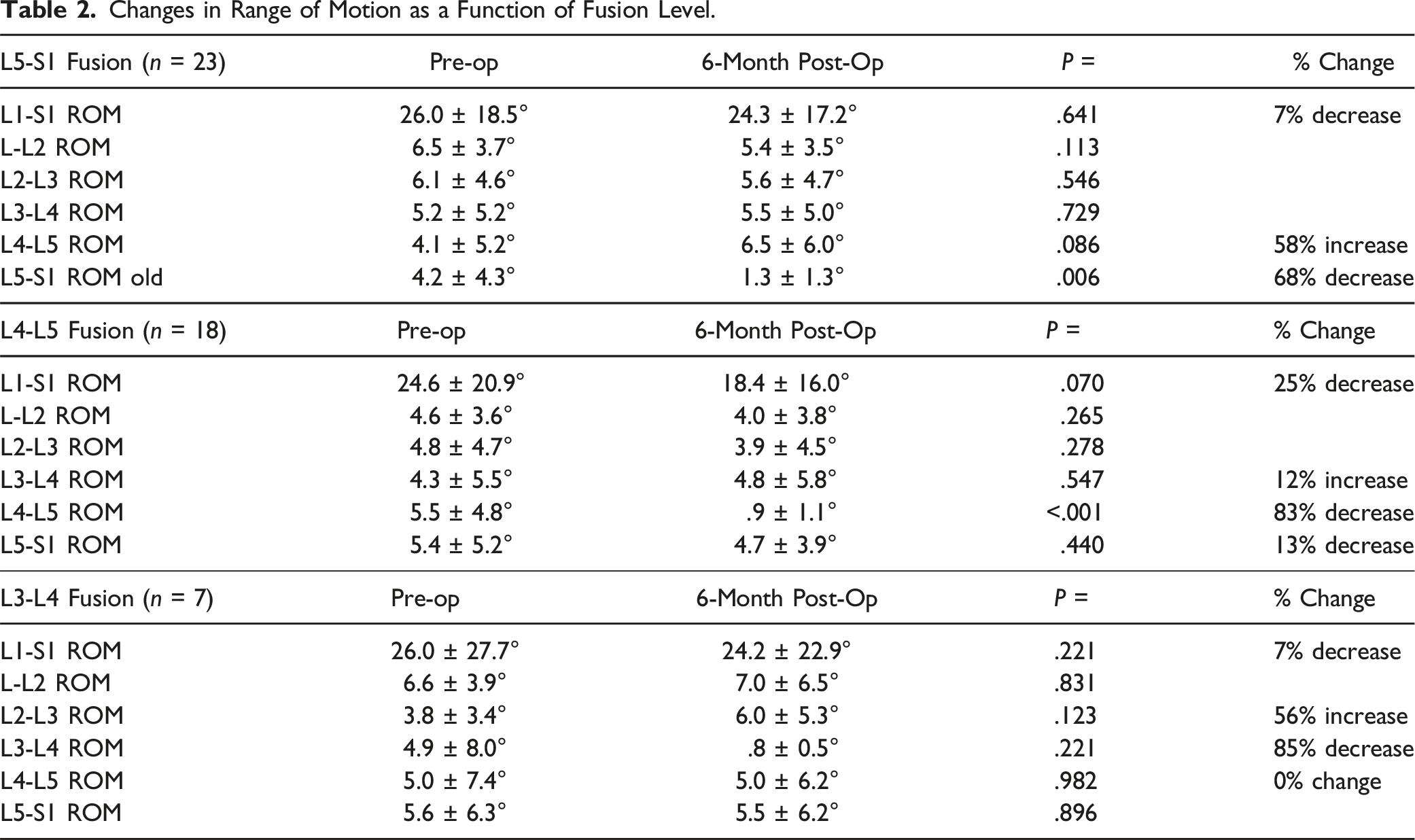
The overall L1-S1 ROM decreased 14% (25.5 ± 20.4° to 22.0 ± 17.2°, P = .104) postoperatively. ROM at the fusion level decreased 77% (4.8 ± 5.0° to 1.1 ± 1.1°, P < .001). Caudal adjacent segment ROM decreased 12% (5.2 ± 5.7° to 4.6 ± 4.4°, P = .345) and cranially ROM increased 34% (4.3 ± 5.0° to 5.7 ± 5.7°, P = .05). K-cluster analysis identified 3 distinct clusters (P < .05). Cluster 1 lost more ROM and had less improvement in patient-reported outcomes measures (PROMs) than average. Cluster 2 had less ROM loss than average with worse PROMs improvement. Cluster 3 did not have changes in ROM and better improvement in PROMs than average. Successful fusion was verified in 96% of all instrumented segments with >6 months follow-up (ROM <4°).
Conclusion
Following single-level L IF, patients should expect a loss of 3.3°, or 14% of overall lumbar motion with increases in ROM of the cranial segment. However, specific clusters of patients exist that experience different relative changes in ROM and PROMs.
Introduction
Lumbar interbody fusion (LIF) is a common and effective surgical treatment for multiple degenerative pathologies of the lumbar spine, including spondylolisthesis, degenerative disc disease, and many others. 1 While multiple different techniques for interbody fusion exist, all of which have reported advantages and disadvantages,2-4 they all share a common pitfall: fusing vertebral levels in this highly-mobile region of the spine can lead to changes in biomechanics and range of motion (ROM).
The lumbar spine plays a complex role in weight-bearing and maintaining ROM through the spine. 5 In general, flexion-extension ROM is greatest in the caudal levels of the lumbar spine (L4-5, L5-S1), while lateral bending is greatest in the central lumbar levels (L2-3, L3-4, L4-5).5,6 Given the complex configuration of this region, subtle changes in the anatomic and kinematic arrangement of the lumbar spine have the ability to disrupt the balance between stability and flexibility that is required for normal function. While alterations in this relationship have long been known to be associated with the natural process of ageing and gradual degenerative changes in the spine, 7 the impact of abrupt iatrogenic fusion on spinal motion is of relatively new interest.
Unsurprisingly, lumbar fusion is associated with a decrease in segmental lumbar ROM, especially when fusion occurs across the L4-5 or L5-S1 joints.8,9 Less intuitively, however, fusion causes an asymmetric change in ROM across the lumbar spine. In both simulations and in vivo studies, interbody fusion has been shown to decrease ROM in the caudal adjacent segment and cause compensatory increases in ROM in the cranial adjacent level.10,11
Given the link between changes in lumbar spine ROM and degenerative changes, as well as the link between spinal fusion, ROM, and adjacent segment disease, a better understanding of how fusion changes ROM at the cranial and caudal adjacent segments may play an important role in understanding the factors that drive adjacent segment disease after lumbar interbody fusion. Furthermore, while average change in ROM after surgery has been assessed, it is important to understand whether there are separate clusters of patients that experience different changes in ROM after fusion. We hypothesize that, on average, single level lumbar interbody fusion decreases lumbar segmental ROM and cranial and caudal adjacent segment ROM. However, we believe there may exist clusters of patients that experience differential changes in these parameters.
Materials and Methods
Study Population
Institutional Review Board (IRB) approval from the Hospital for Special Surgery IRB (IRB number 2021-1890) was obtained prior to initiation of this study. This study was exempt from informed consent. Using data collected from a Biobase Registry composed of patients from a large, growing, multi-center, observational cohort, we retrospectively reviewed to identify patients who underwent one-level interbody fusion between L1-2 and L5-S1 using anterior lumbar interbody fusion (ALIF), lateral lumbar interbody fusion (LLIF), transforaminal interbody fusion (TLIF), and posterior lumbar interbody fusion (PLIF). Patients with multi-level fusions or fusions outside of the lumbar spine were excluded from analysis. Patients were included if they had preoperative and 6-month postoperative flexion-extension radiographs of the lumbar spine for assessment of lumbar spine ROM.
Imaging Assessment
Preoperative and 6-month postoperative flexion-extension radiographs were used for assessments of lumbar spine ROM. Segmental ROM changes from L1-2, L2-3, L3-4, L4-5, and L5-S1 were measured as previously described using the Cobb angle method. 12 Changes in overall lumbar L1-S1 ROM were assessed using the same methods. A digital software package (ACES GmbH, Esslingen, Germany) was used to automatically perform radiographic measurements of Cobb angles on preoperative and postoperative flexion/extension radiographs.
Statistical Analysis
Continuous variables are expressed as mean ± standard deviation. Paired two-tailed student’s t-tests were used to compare preoperative and postoperative ROM. One-way analysis of variance was used to compare ROM differences based on interbody fusion technique with homogeneity of variance testing.
K-means cluster analysis was performed using standardized Z scores for differences in preoperative and postoperative range of motion at the fusion level, cranial adjacent level, and L1-S1 as well as (patient-reported outcomes measures) PROMs. This was intended to investigate if, despite the overall trends seen in ROM, there existed specific sub-groups of patients that experienced increases, decreases, or no change in ROM that were masked in the overall average. An α < .05 was considered statistically significant. Statistical analysis was performed using SPSS (SPSS 25.0, IBM, Armonk, NY).
Results
We identified a total of 54 patients who underwent single-level lumbar interbody fusion and had available preoperative and postoperative imaging for ROM assessment. There were 2 fusions performed at L2-3 (4%), 7 at L3-4 (13%), 19 at L4-5 (35%), and 26 at L5-S1 (48%). There were 21 ALIFs (39%), 7 LLIFs (13%), and 26 PLIF or TLIFs (48%).
Overall Differences in Preoperative and Postoperative Range of Motion.

Changes in Range of Motion as a Function of Fusion Level.
Differences in Change of Range of Motion at Fusion Level and Cranial Adjacent Level Based on Interbody Fusion Technique.

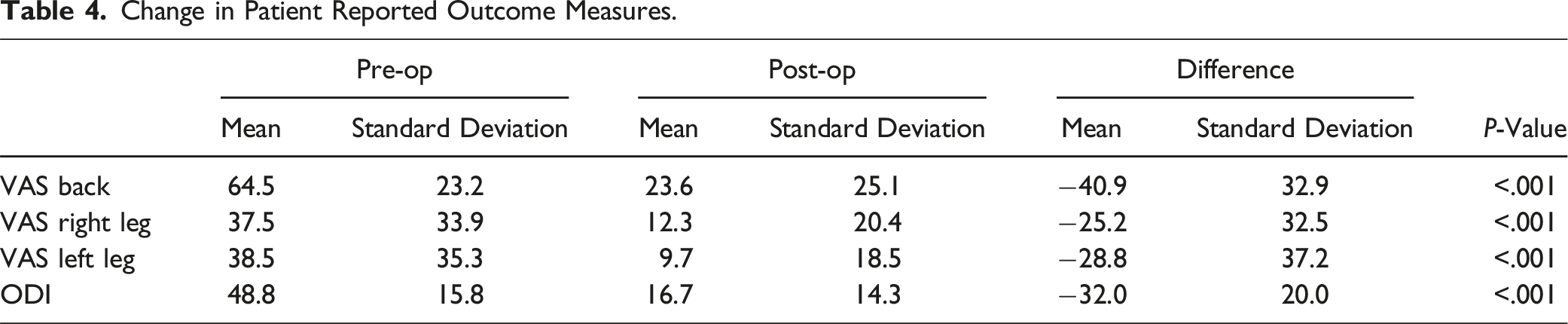
Change in Patient Reported Outcome Measures.
K-cluster analysis of standardized z-scores in differences in ROM and PROMs identified 3 distinct clusters (Figure 1). There were 6 patients in Cluster 1 (11%), 23 patients in cluster 2 (45%), and 22 patients in cluster 3 (43%). There were 3 patients excluded for missing PROMs data. Differences in Z-scores for all variables were significant (P < .05). Cluster 1 had more ROM loss than average with less improvement in PROMs than average. Cluster 2 had less ROM loss than average (experienced slight increases in ROM) with worse PROMs improvement. Cluster 3 did not have changes in ROM and better improvement in PROMs than average. K-means cluster analysis of change in range of motion.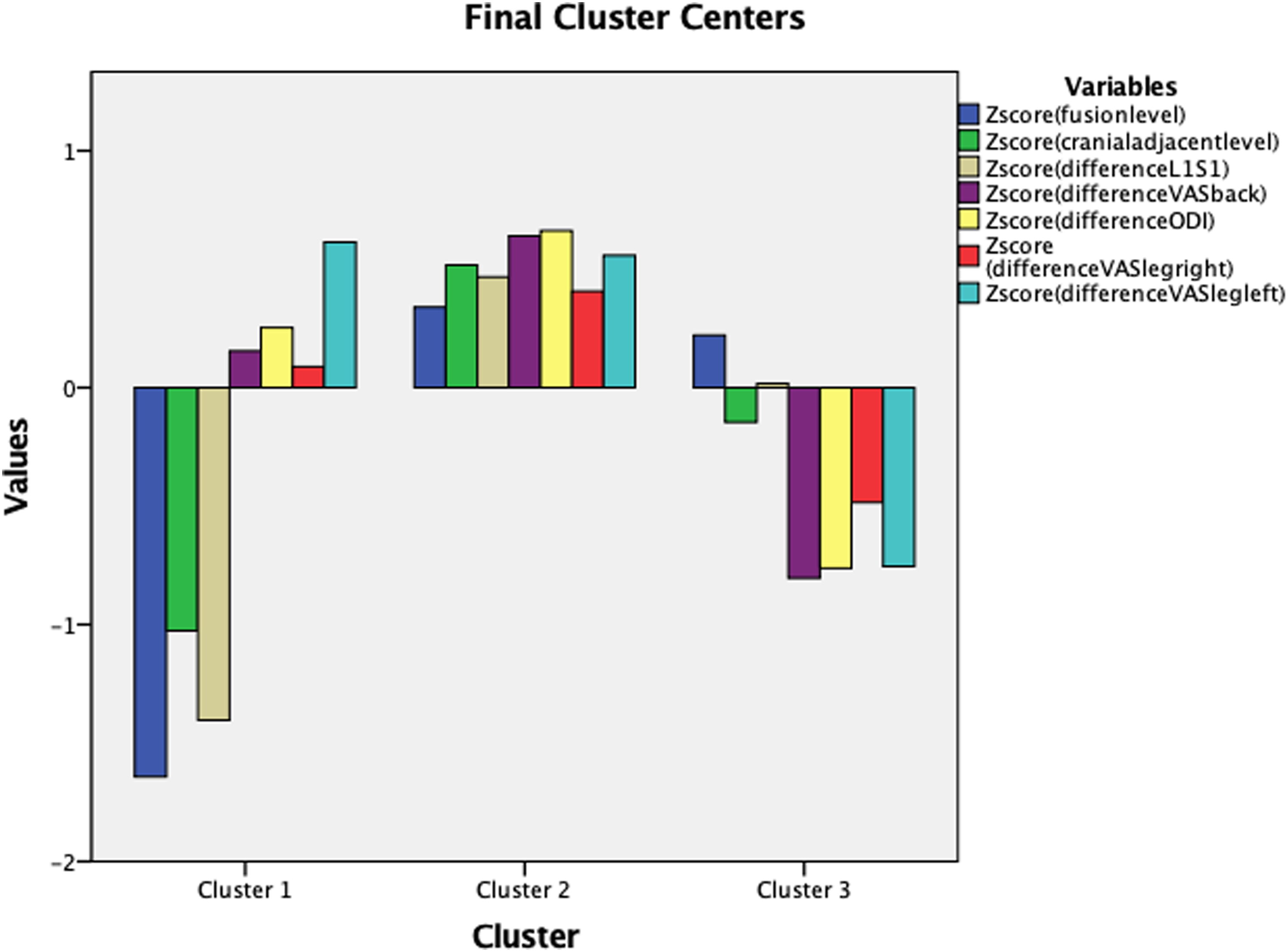
Comparison of Range of Motion and PROMs by Cluster.
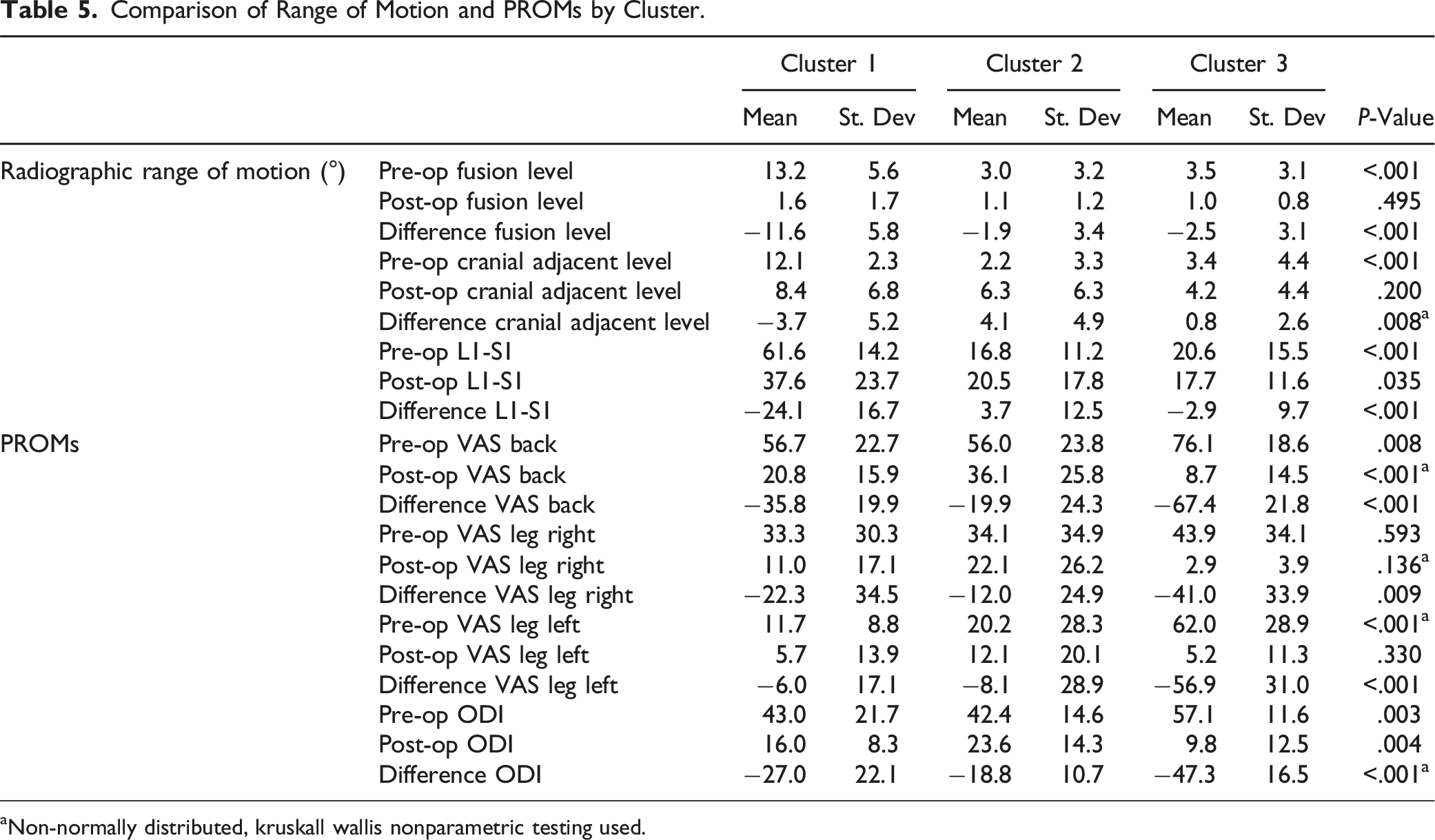
aNon-normally distributed, kruskall wallis nonparametric testing used.
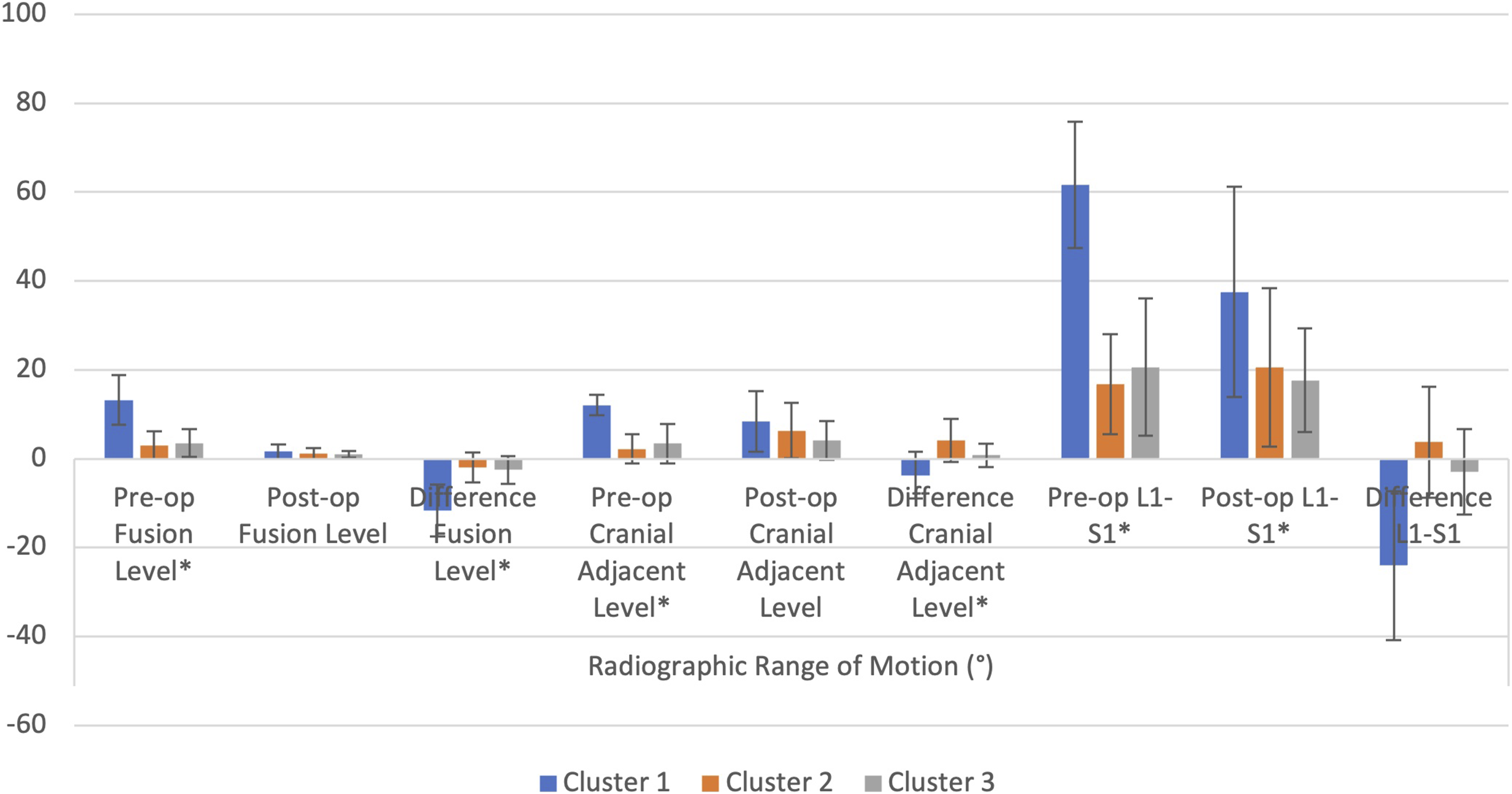
Range of motion by cluster cohorts.
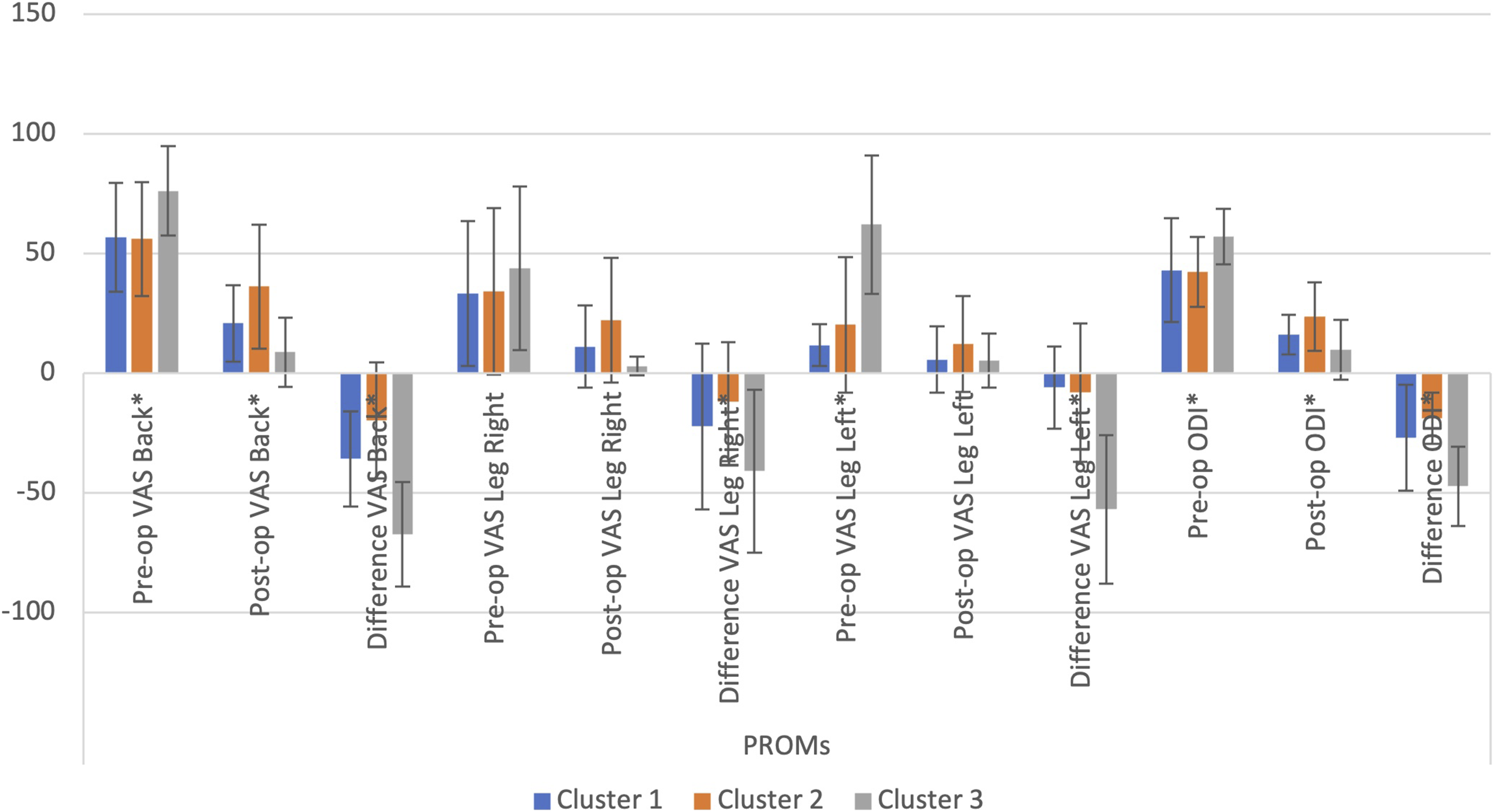
PROMs by cluster cohort.
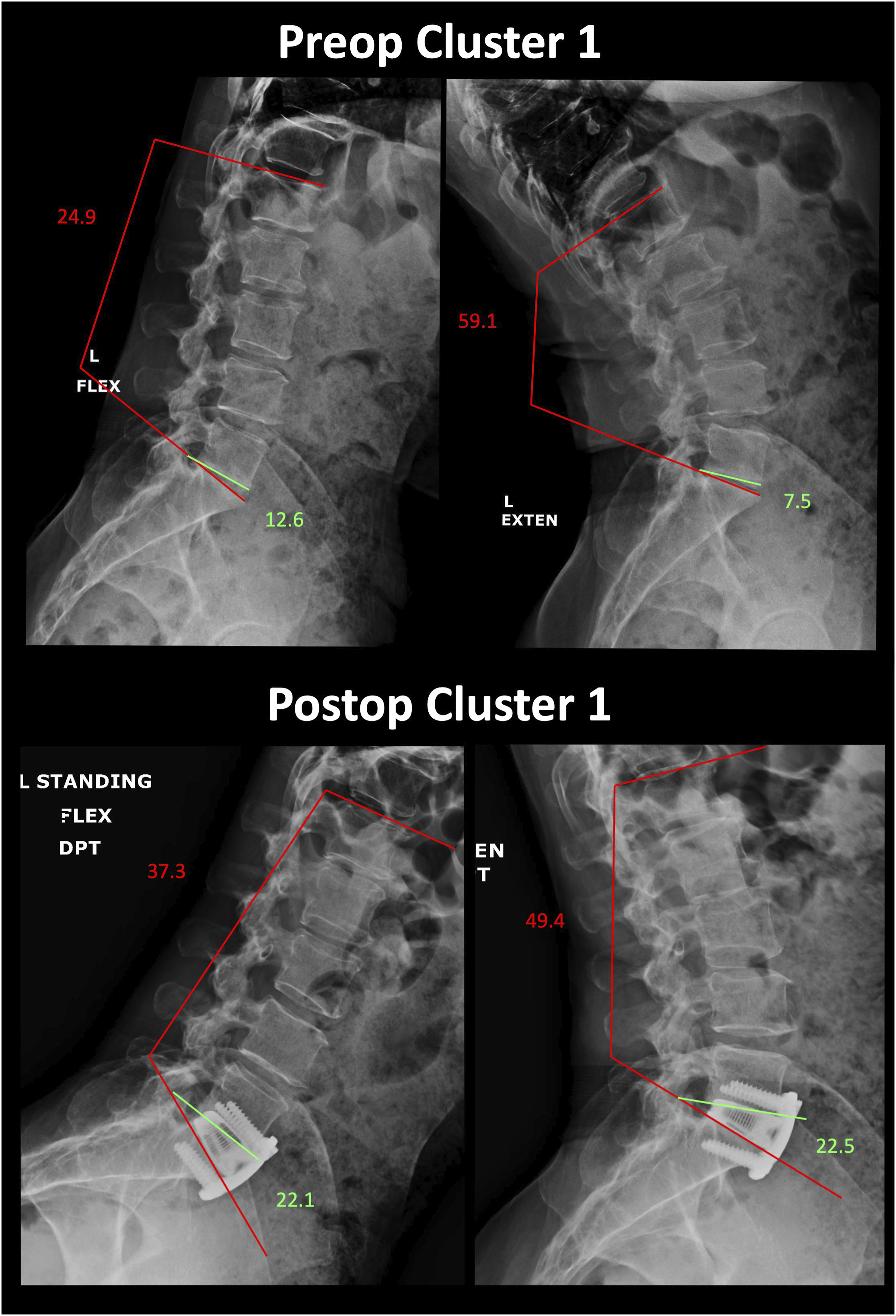
Representative preoperative and postoperative flexion-extension radiographs from a patient in Cluster 1.
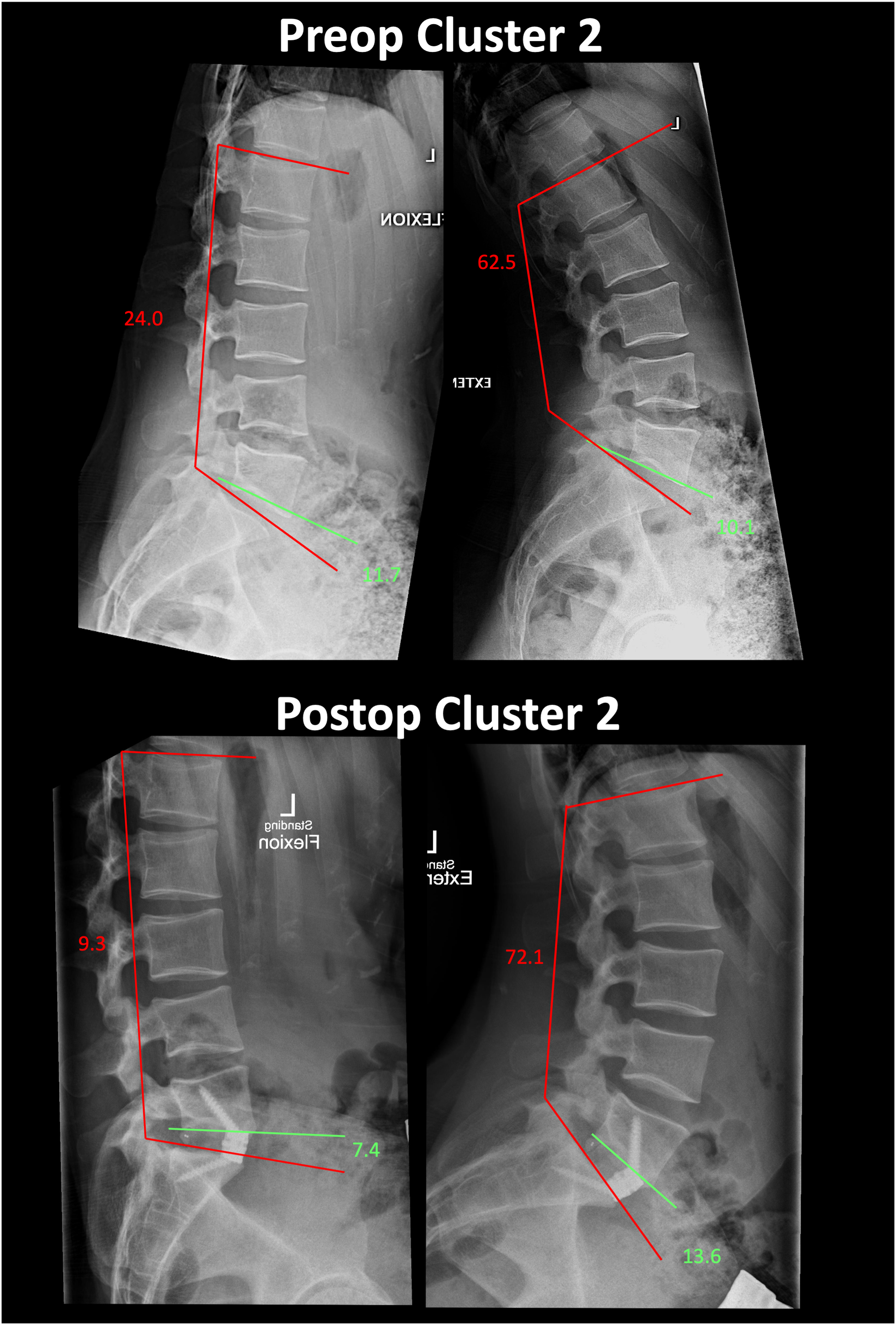
Representative preoperative and postoperative flexion-extension radiographs from a patient in Cluster 2.
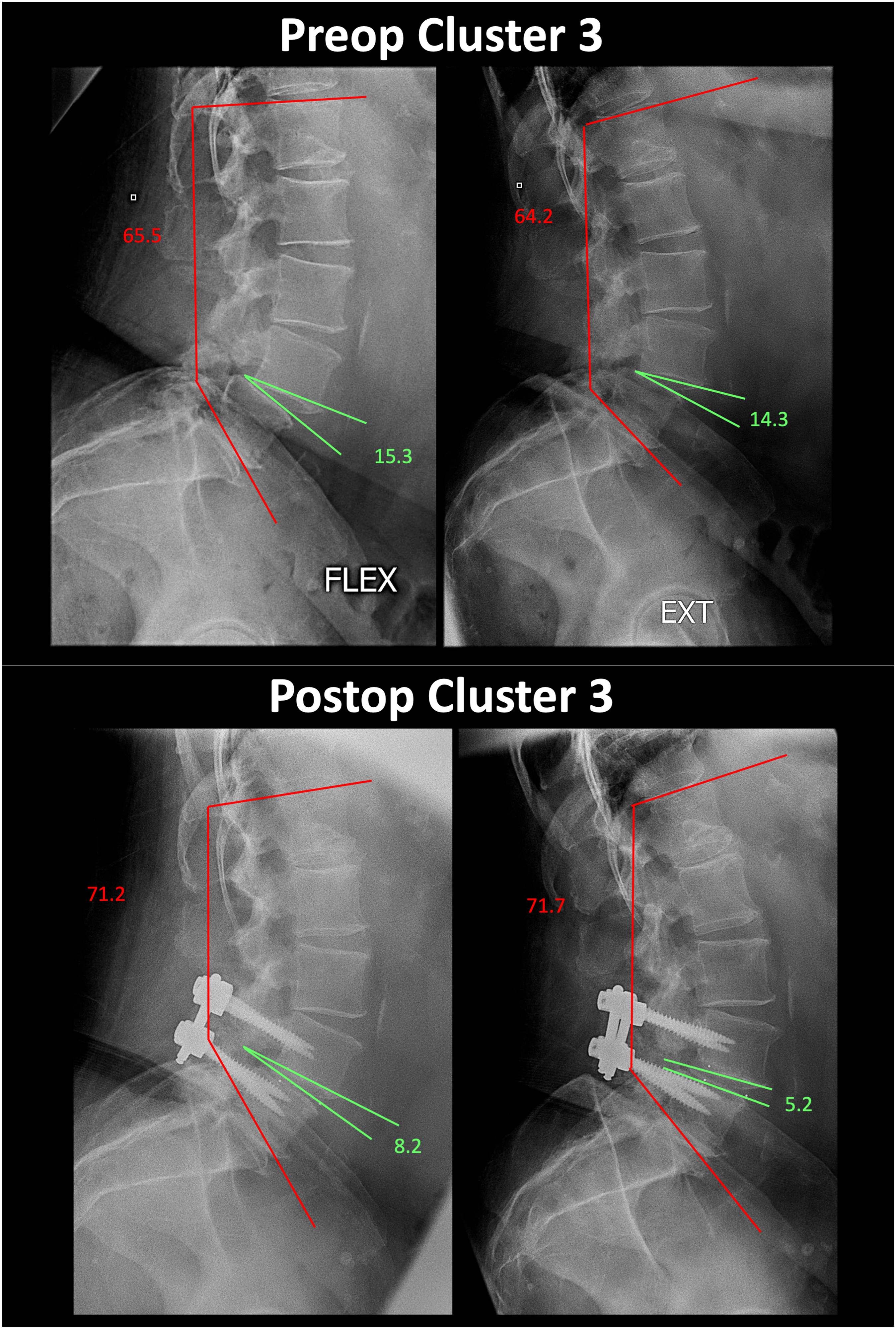
Representative preoperative and postoperative flexion-extension radiographs from a patient in Cluster 3.
Successful fusion was verified in 96% of all instrumented segments with >6 months follow-up (ROM <4°).
Discussion
In the current study, we assessed the impact of interbody type and location on overall, cranial adjacent segment, and caudal adjacent segment ROM following various types of single-level lumbar interbody fusion. Fusion had an expected decrease in ROM at the fusion level and decreased overall lumbar ROM from L1-S1. Interestingly, fusion decreased ROM of the caudal adjacent segment and increased cranial adjacent segment ROM. Patients appeared to cluster into three separate groups: Cluster 1 had greater overall decreases in ROM after fusion, Cluster 2 had less overall ROM and a smaller adjacent segment ROM decrease after fusion, and Cluster 3 had no significant ROM changes after fusion. Interestingly, Cluster 3 had the greatest improvement in PROMs, Cluster 1 had less improvement, and Cluster 2 had the least. These findings suggest that different compensatory changes occur after lumbar fusion and may have associations with post-operative PROMs.
Compensatory changes are important areas of research following spinal fusion for multiple reasons. Firstly, ROM of the lumbar spine is critical for flexion/extension and lateral bending, so maintenance of motion in this region is critical for completion of activities of daily living (ADLs) that require high levels of flexion/extension through the lumbar spine, including squatting and bending forward, sitting and standing from a seated position, and putting on shoes/socks. Squatting and bending forward require >50° ROM, standing from a seated position and sitting from a standing position require >35° ROM, and putting on shoes and socks require >20° ROM. 13 Secondly, changes in the flexibility and motion through this complex region are thought to have a significant impact on adjacent segment disease. However, the relationship between fusion, adjacent segment motion, and adjacent segment disease, is poorly understood.
Multiple finite element analyses have assessed the impact of interbody fusion on lumbar ROM and the risk of adjacent segment disease. Nan et al assessed the impact of LLIF at L4-5 on ROM of the fusion level and cranial adjacent level. They found that fusion led to decreased ROM at the fusion level, with a compensatory increase in cranial adjacent segment ROM. Furthermore, they postulated that the increased ROM at the adjacent segment leads to increased endplate stress and facet loading, which can contribute to adjacent segment disease. 10 Similar results were identified by Li et al when assessing the impact of XLIF at L4-5. ROM was decreased at the index level and increased at the cranial adjacent level. Increased ROM at the cranial adjacent level was found to increase stress on the L3-4 disc. These finite element analyses highlight the possible link between increased adjacent segment motion, intradiscal pressures, and adjacent segment disease following interbody fusion.14,15
Similar to these finite element analyses, Okuda et al. assessed changes in ROM in vivo following PLIF and its impact on symptomatic adjacent segment disease (ASD) requiring revision surgery. They found increased ROM in the cranial adjacent segment, and decreased ROM in the caudal adjacent segment. Patients who developed ASD had larger increases in cranial adjacent segment motion and larger decreases in caudal adjacent segment ROM. 11 Larger postoperative ROM at the cranial adjacent segment, larger changes in cranial adjacent segment ROM, and larger changes in overall lumbar alignment were significant risk factors for ASD. 11
The results of the current study suggest that fusion overall decreases lumbar segment ROM and increases cranial adjacent segment ROM. Based on the results of prior studies, this compensatory hypermobility in the adjacent segment may contribute to ASD. Importantly, this study also identified that not all patients experience the same changes in ROM postoperatively. Cluster 3, which had the most relative improvement in PROMs, had the smallest change in all ROM measures. Cluster 1 had significantly decreased ROM and less improvement in PROMs while cluster 2 had less decrease in ROM and the worst improvement in PROMs. Further study should be performed into whether ROM changes after fusion drive post-operative PROMs or vice-versa. One hypothesis of these cluster findings is that there is an “optimal” level of stabilization that allows for maximal PROMs improvement, while over- or under-stabilization leads to less improvement in PROMs.
These findings likely represent an important area for future study. Both the risk factors for these clusters, as well as the impact of each cluster on outcomes and risk of adjacent segment disease, are important considerations for future analysis. It is possible that certain technical factors, such as interbody type or interbody position, may play a role in these findings. Furthermore, given the relationship between lumbar spine ROM and adjacent segment disease, it is also possible that certain clusters are at an increased or decreased risk for adjacent segment changes. Finally, because maintenance of lumbar spine ROM is important for the completion of many different ADLs, 13 patients in clusters with decreased ROM may be predisposed to worse functional outcomes.
This study had multiple limitations. Firstly, though this study included a modest sample size (50 patients), the inclusion of 5 fusion levels and 3 interbody types created a large number of interbody and level combinations to be assessed. Therefore, while overall lumbar ROM or cranial/caudal adjacent segment ROM may vary as a complex function of both interbody level and interbody type, the number of patients in these sub-groups was small, underpowering this analysis. Secondly, our results are limited to the 6-month postoperative timepoint. It is possible that ROM is dynamic and continues to change beyond this endpoint, which would not be identified by the current study. Our study cannot identify a causal effect changes in ROM on final outcomes, which is an important area for future study. The relationship of ROM and PROMs should be further explored, and the impact of confounders, such as interbody type, pathologic level, and patient comorbidities, should be accounted for.
Conclusions
In the current study, we assessed the impact of single-level lumbar interbody fusion on post-operative lumbar ROM. We found a minor decrease in L1-S1 ROM (14% decrease) and a compensatory increase in the cranial adjacent segment (34%). We identified 3 distinct clusters of patients based on ROM and PROMs, one with increased relative decreases in ROM after fusion with less relative improvement in PROMs, one with less relative decrease in ROM with even worse improvements in PROMs, and a third without significant changes in ROM but greater relative improvements in PROMs. The relationship between post-operative ROM and PROMs should be further explored.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
No direct funding was received for this study. However, this study used REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384.