
Abstract
Study Design
Biomechanical human cadaveric study.
Objectives
Transforaminal lumbar interbody fusion (TLIF) is a well-established procedure for treating degenerative lumbar spine pathologies. However, posterior fixation has been reported to accelerate adjacent segment degeneration (ASD). Posterior fixation can be omitted in screw-anchored stand-alone anterior lumbar interbody fusion (ALIF). The present study aimed to compare the cranial adjacent segment motion of ALIF vs TLIF in specimens with reduced bone mineral density (BMD).
Methods
Sixteen fresh-frozen lumbosacral spines with reduced BMD (donors’ age 71 ± 13years, BMD 95.7 ± 34.5 mg HA/cm3) were used. Range of motion (ROM) and Neutral Zone (NZ) of the cranial adjacent segment were analyzed in flexion-extension, lateral bending, and axial rotation in native state and after TLIF or stand-alone screwed ALIF instrumentation.
Results
No significant differences between TLIF and stand-alone screwed ALIF were observed for both absolute ROM and NZ of the cranial adjacent segment in instrumented state across all tested motion directions (P ≥ .267). Decreased relative ROM of the fused segment – normalized to the corresponding segmental ROM in native state – resulted in compensatory increased relative ROM of the cranial adjacent segment after instrumentation. However, the relative adjacent segment ROM did not differ significantly between TLIF and stand-alone screwed ALIF (P ≥ .172).
Conclusions
This study found no clinically significant difference in adjacent segment motion when comparing TLIF with stand-alone screwed ALIF. Hence, both techniques appear to have a negligible impact on adjacent segment motion in poor bone quality. This suggests that neither TLIF nor stand-alone screwed ALIF increase the risk of ASD due to compensatory motion resulting from an operated adjacent segment.
Keywords
Introduction
Chronic low back pain associated with degenerative disc disease (DDD) is the leading cause of global disability. Degenerative diseases of the lumbar spine are prevalent worldwide, with DDD-related lower back pain alone affecting approximately 266 million individuals with a global incidence of 3.63%. 1 When non-operative treatments fail, lumbar fusion surgery may be indicated. Lumbar fusion increases the risk of adjacent segment disease (ASD). To achieve fusion of a segment, its motion is restricted. As a compensatory mechanism, more movement occurs in the segments above and below the fused segment,2-4 potentially leading to ASD manifesting as DDD, olisthesis, or fracture.5,6 Frequencies of ASD are reported to reach up to 30%. 6 An analysis of 1751 patients in 2020 found an ASD rate of 27.8% on X-rays, with 7.6% of symptomatic ASD, and 4.6% of the cases requiring reoperation. 7
Transforaminal lumbar interbody fusion (TLIF) is a well-established and frequently performed fusion technique, with a consistent upward trend in incidence rates.8-10 Compared to TLIF, anterior lumbar interbody fusion (ALIF) carries a higher vascular risk, however, it is thought to be more effective at restoring lumbar and segmental lordosis, which are protective factors against ASD.11-13 Studies comparing TLIF to screw-anchored stand-alone ALIF concerning ASD remain inconclusive.6,14,15 Specifically, stand-alone ALIF using a cage with an integrated plate for vertebral anchoring screws – referred to as the modern-era single-level ALIF – differs from traditional ALIF as no additional posterior instrumentation is needed. Previous research has indicated that posterior fixation is associated with increased ASD, 5 suggesting that its absence may reduce compensatory motion at the adjacent level and potentially lower the risk of ASD compared to traditional TLIF. However, there is limited biomechanical data available on adjacent segment motion for this approach.16,17
The aim of the present study is to compare the range of motion (ROM) and neutral zone (NZ) of the cranial lumbar adjacent segment of stand-alone screwed ALIF vs an instrumented TLIF in degenerative lumbar specimens with reduced bone mineral density (BMD). The null hypothesis asserts that TLIF results in a significantly bigger increase in ROM and NZ of the cranial adjacent segment compared to stand-alone screwed ALIF.
Materials and Methods
Specimen Preparation
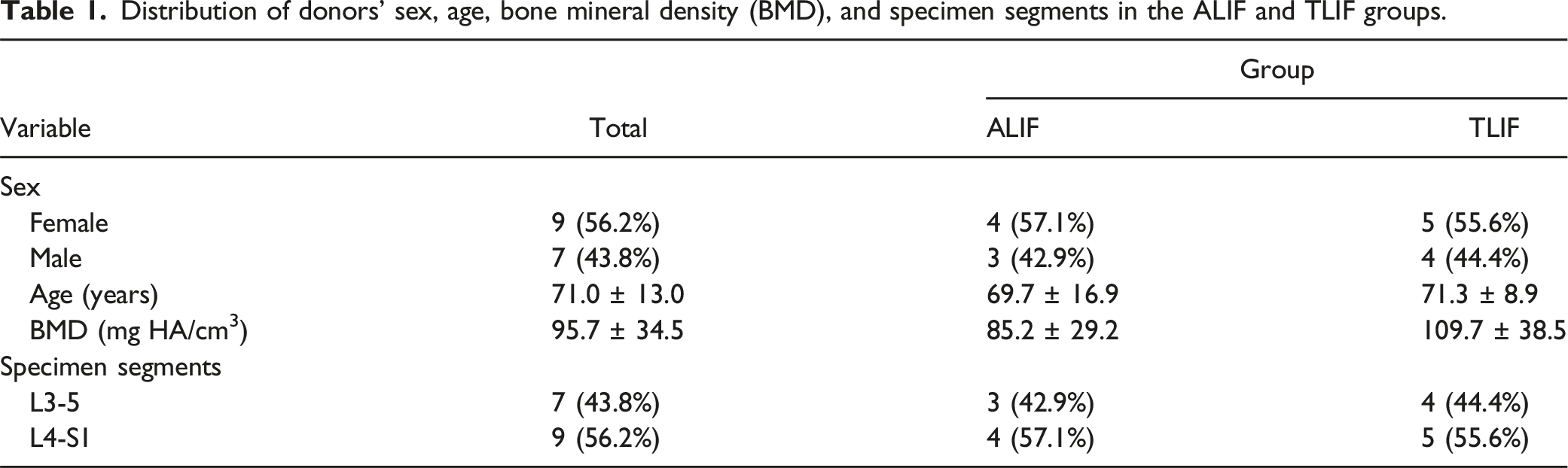
Distribution of donors’ sex, age, bone mineral density (BMD), and specimen segments in the ALIF and TLIF groups.
Surgical Technique
ALIF or TLIF were conducted in the in the L3-5 spines at the L4-5 level, and in the L4-S1 specimens at the lumbosacral junction, thus leaving the lumbar cranial adjacent segments L3-4 and L4-5 for analysis, respectively.
TLIF
The technique described by Jeszenszky and Harms was followed. 18 First, the pedicle screws were placed to allow distraction for facilitated disc removal. Common anatomical landmarks were used to select the entry points of the screws. The mid transverse process and lateral border of the superior articular facet were used. After opening of the cortex the pedicle finder was used. Before final placement, palpation with a probe confirmed bone surrounding the screw channel in all directions. Following the determination of the screw length, titanium polyaxial pedicle screws (EXPEDIUM VERSE Spinal System, Johnson&Johnson MedTech) were inserted under radiographic control into the pedicles of the vertebrae L5 and S1. Facetectomy was performed on the left side. The posterior supraspinous and interspinous ligaments at L3-4 were incised to allow interspinous distraction. Temporary rods were used to hold distraction during discectomy. The anterior and lateral part on the right side of the annulus fibrosus were preserved to prevent migration of the cage. Endplate preparation involved careful removal of the cartilaginous layers using ring curettes. Trial implants determined the height of the selected polyether ether ketone (PEEK) TLIF spacers (T-pal Ti, Johnson&Johnson MedTech). The T-pal cage was placed in the anterior third of the disc space in the median sagittal plane. Correct placement was confirmed radiologically, before the replacement of the temporary rods with final ones. Under compression, the pedicle screw inserts were tightened using a 9 Nm torque limiter. Final biplanar X-rays verified correct screw trajectory and implant placement.
ALIF
A SynFix-LR implant (Johnson&Johnson MedTech) – a PEEK cage with an integrated titanium plate – was used for stand-alone screwed ALIF. Its four locking screws allow fixation in the upper and lower vertebra. The anterior longitudinal ligament (ALL) was resected, and the disc was partially removed. The implant height was selected to achieve press fit. Once correctly positioned, the cage was fixated by the 4 locking screws. Final X-rays in 2 planes verified correct implant placement.
Biomechanical Testing
Biomechanical testing was performed on a biaxial servo-hydraulic material testing machine (MTS 858 Mini Bionix II, MTS Systems, Eden Prairie, MN, USA) equipped with a 100 Nm/4 kN load cell (HUPPERT 6, HUPPERT GmbH, Herrenberg, Germany) according to the in vitro testing criteria for spinal implants.
21
A previously established biomechanical test protocol19,20 was adopted as follows: ROM and NZ of the cranial adjacent segment to the ALIF or TLIF instrumentation were assessed in flexion-extension (Flex-Ext), right and left lateral bending (LB), and right and left axial rotation (AR). The machine’s torsional actuator was used to load the specimens in 3 different setup configurations (Figure 1). A cardan joint and XY-table were used to passively neutralize artifactual shear forces and bending moments. The axial load was actively kept at a constant level of 0 N throughout the tests. This ensured unconstraint movement around the intended anatomical axis. The loading protocol consisted of 3 bidirectional ramps up to ±7.5 Nm at a rate of 4°/sec. Test setup for range of motion testing in flexion-extension (A, left), lateral bending (B, middle), and axial rotation (C, right) with XY-table (XY), cardan joint (ca), reference marker set for motion tracking (1), PMMA embedding (2), and base fixation (3).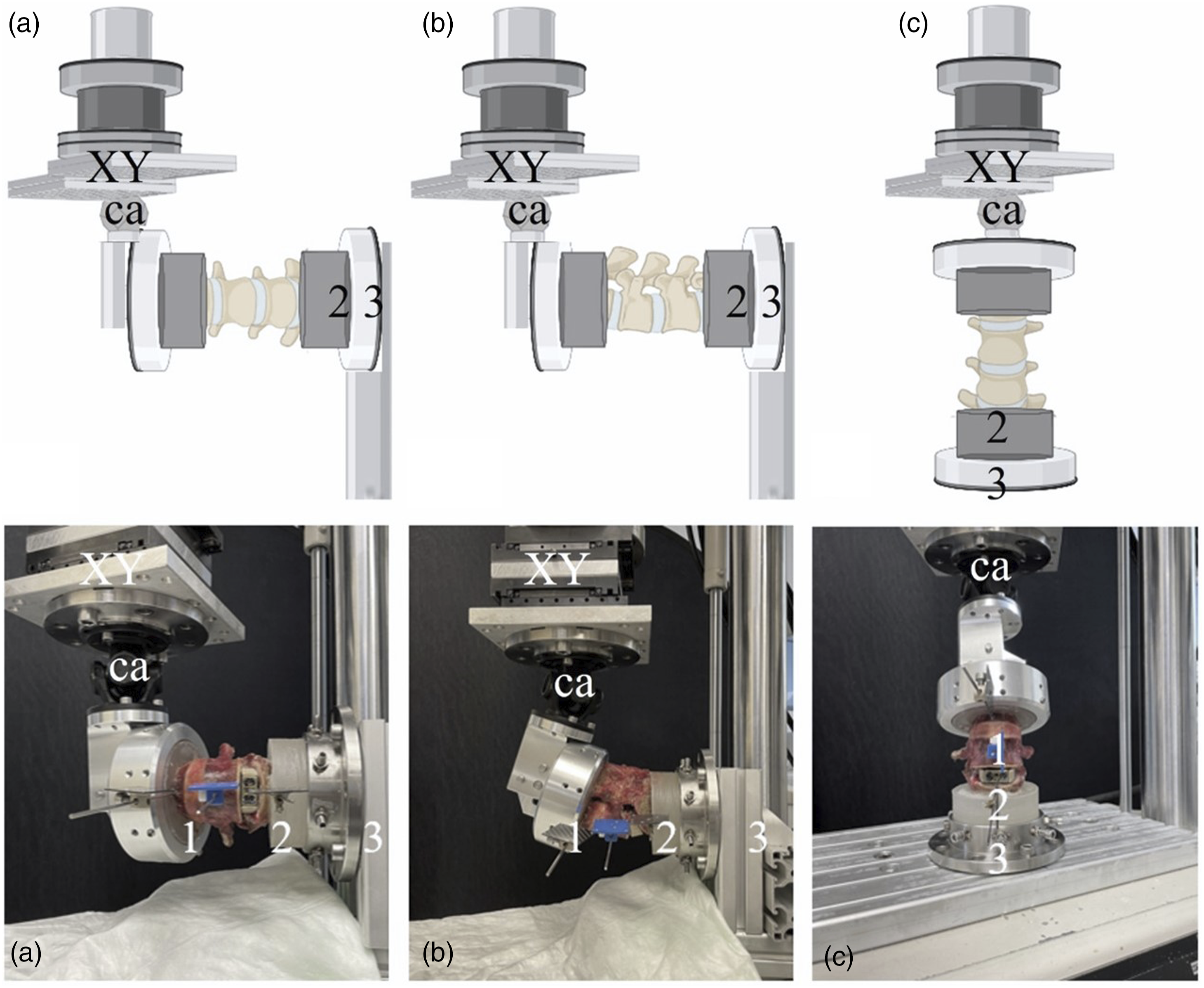
An optical marker set was attached to each vertebra using a Kirschner wire for optical motion tracking. The marker set of L4 was aligned with its anatomical axes and planes, defining the reference coordinate system.
Data Acquisition and Evaluation
Machine data of axial load, axial displacement, torsion angle and torque were continuously acquired at 128 Hz throughout each test. In addition, the coordinates of the optical markers attached to each vertebra were continuously tracked using a stereometric optical measurement system (GOM Aramis SRX, Carl Zeiss GOM Metrology GmbH, Braunschweig, Germany) operating at a resolution of 12 megapixel and a maximum acceptance error of 0.02 mm. Based on synchronized machine and optical motion tracking data, NZ of the adjacent segment was calculated for each loading direction and instrumentation state as the range of motion where minimal resistance is provided by the implant material, reflecting a critical parameter for stability assessment. Furthermore, ROM of the adjacent segment was assessed as the peak deflection movement for each loading direction and instrumentation state separately. Further data processing included normalization of the ROM outcome measures to the native state.
Statistical analysis was carried out using GraphPad Prism software (version 10.2.3, San Diego, CA, USA). Normality of data distribution of both the absolute and normalized data was assessed using the Shapiro-Wilk test. Descriptive data are presented as mean value ± SD or counts and percentages (%). Contingency analyses with Pearson’s Chi-Square test were used to compare the proportions of the categorical variables. Independent-Samples t-test was used to identify significant differences regarding the group characteristics ROM and NZ between the ALIF and TLIF groups. Paired-Samples t-test was used to analyse the change in adjacent segment ROM and NZ between the intact and instrumented state in each separate group. F-test was used to compare variances. Level of significance was set at P = .05.
Results
There were no significant differences in baseline characteristics between the groups (Table 1).
Cranial Adjacent Segment ROM
Range of motion (ROM, nean value ± standard deviation) of the cranial adjacent segment in the native state and after ALIF and TLIF instrumentation of the caudal segment for flexion, extension, right and left lateral bending (LB), and right and left axial rotation (AR).
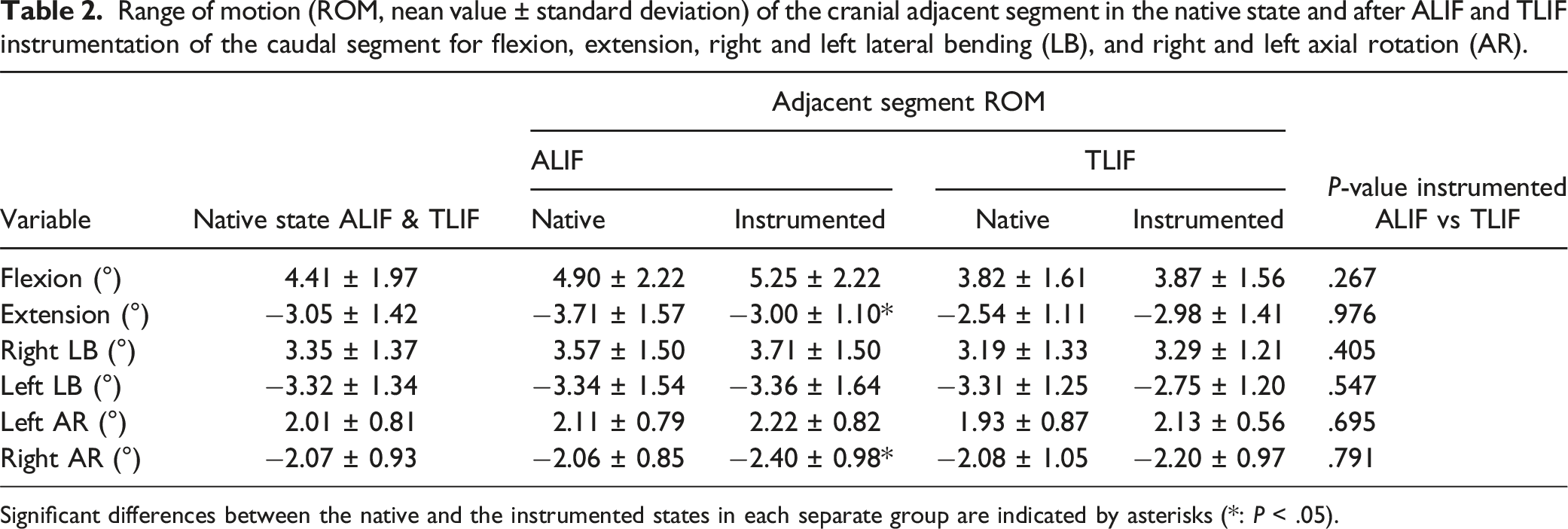
Significant differences between the native and the instrumented states in each separate group are indicated by asterisks (*: P < .05).
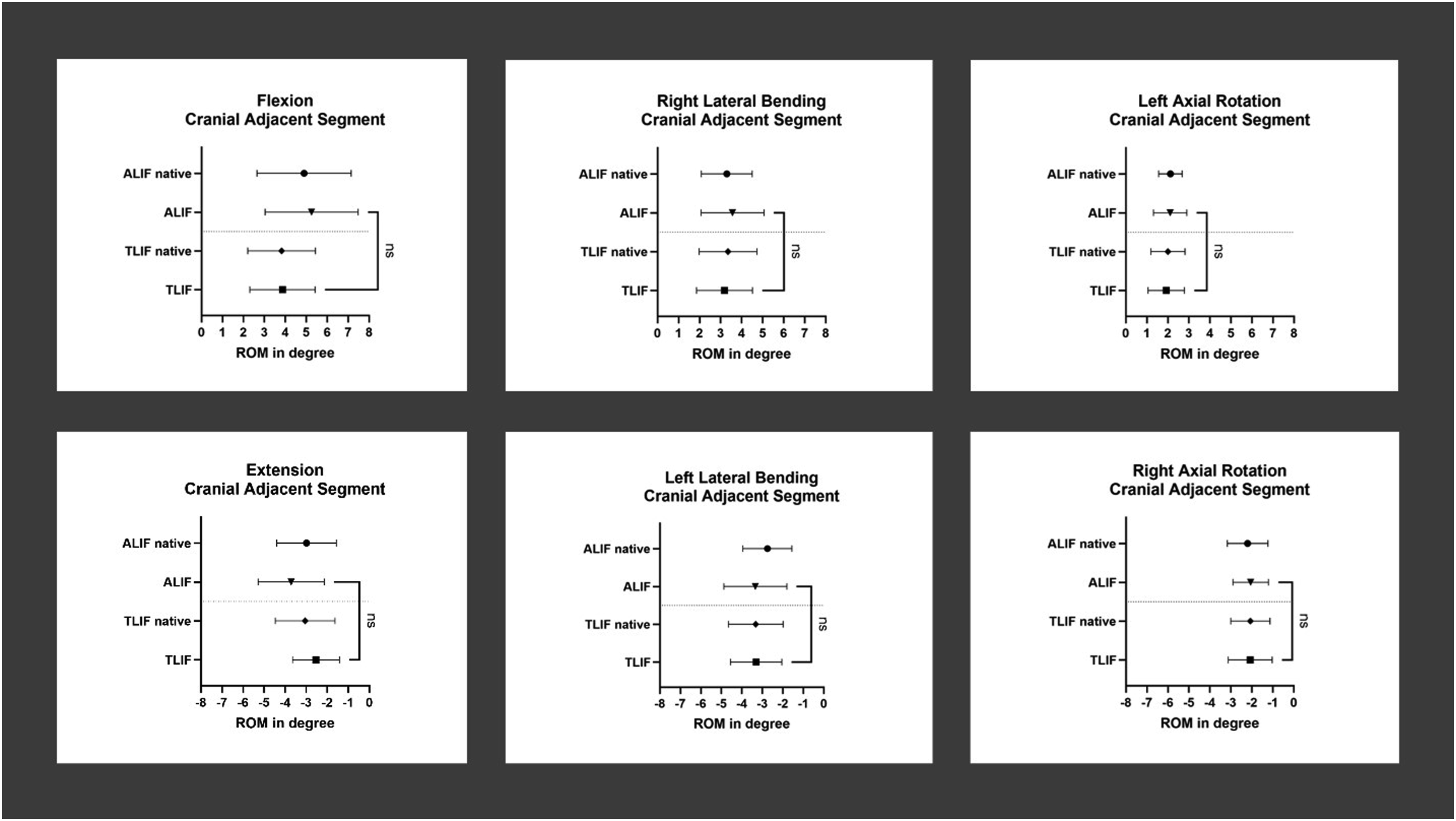
Range of motion (ROM, mean value ± standard deviation) at the cranial adjacent segment of TLIF and ALIF for flexion-extension (left) lateral bending (middle), and axial rotation (right). Comparisons between the instrumented ALIF and TLIF groups are indicated (ns: not significant).
For flexion, no significant change in ROM of the segment adjacent to the instrumentation was observed between native and instrumented state within each group (TLIF: P = .876, ALIF: P = .216). There were no significant differences between the ALIF and TLIF groups regarding the adjacent segment motion in native state (difference 0.86 ± 0.99°, P = .400) and after instrumentation (difference 1.09 ± 0.94°, P = .267). Extension motion of the adjacent segment showed no significant change after instrumentation in the TLIF group (P = .127), however, it decreased significantly after instrumentation in the ALIF group by 0.71 ± 0.70° (P = .037). For extension, there were no significant differences between the ALIF and TLIF groups regarding the adjacent segment motion in the native state (difference 1.17 ± 0.67°, P = .101) and after instrumentation (difference 0.02 ± 0.65°, P = .976).
For left LB of the adjacent segment, no significant change was indicated between native and instrumented state in both TLIF (difference 0.55 ± 1.19°; P = .202) and ALIF (difference 0.02 ± 0.63°; P = .941) groups. There were no significant differences between the ALIF and TLIF groups regarding the adjacent segment motion in native state (difference 0.04 ± 0.70°, P = .960) and after instrumentation (difference 0.61 ± 0.71°, P = .405). For right LB of the adjacent segment, no significant change was indicated between native and instrumented state in either group (TLIF: difference 0.11 ± 0.61°; P = .611; ALIF: difference 0.14 ± 0.66°; P = .586). There were no significant differences between the ALIF and TLIF groups regarding the adjacent segment motion in native state (difference 0.38 ± 0.71°, P = .600) and after instrumentation (difference 0.42 ± 0.67°, P = .547).
Right AR of the adjacent segment increased between native and instrumented state in the TLIF group by 0.12 ± 0.59° (P = .544) and significantly increased in the ALIF group by 0.34 ± 0.34° (P = .037). There were no significant differences between the ALIF and TLIF groups regarding the adjacent segment motion in native state (difference 0.02 ± 0.49°, P = .965) and after instrumentation (difference 0.20 ± 0.49°, P = .695). Left AR of the adjacent segment increased between native and instrumented state in both TLIF (difference 0.20 ± 0.68°; P = .405) and ALIF (difference 0.11 ± 0.46°; P = .544) groups without reaching statistical significance. There were no significant differences between the ALIF and TLIF groups regarding the adjacent segment motion in native state (difference 0.18 ± 0.42°, P = .671) and after instrumentation (difference 0.09 ± 0.34°, P = .791).
Relative Cranial Adjacent Segment ROM
There were no significant differences of the relative cranial adjacent segment and fused-segment ROM – being normalized to the corresponding segmental ROM in native state – between the instrumented ALIF and TLIF groups (P ≥ .172). Figure 3 shows the change in cranial adjacent segment ROM after instrumentation normalized to the corresponding native state. Relative range of motion (ROM, mean value ± standard deviation) of the fused segment (TLIF / ALIF) and the cranial adjacent segment (TLIF / ALIF Cranial Adjacent Segment) after TLIF or ALIF instrumentation, normalized to the corresponding segmental ROM in the native state for flexion-extension (Flex-Ext, left), lateral bending (LB, middle), and axial rotation (AR, right). The horizontal gridline indicates 100% native motion before lumbar interbody fusion.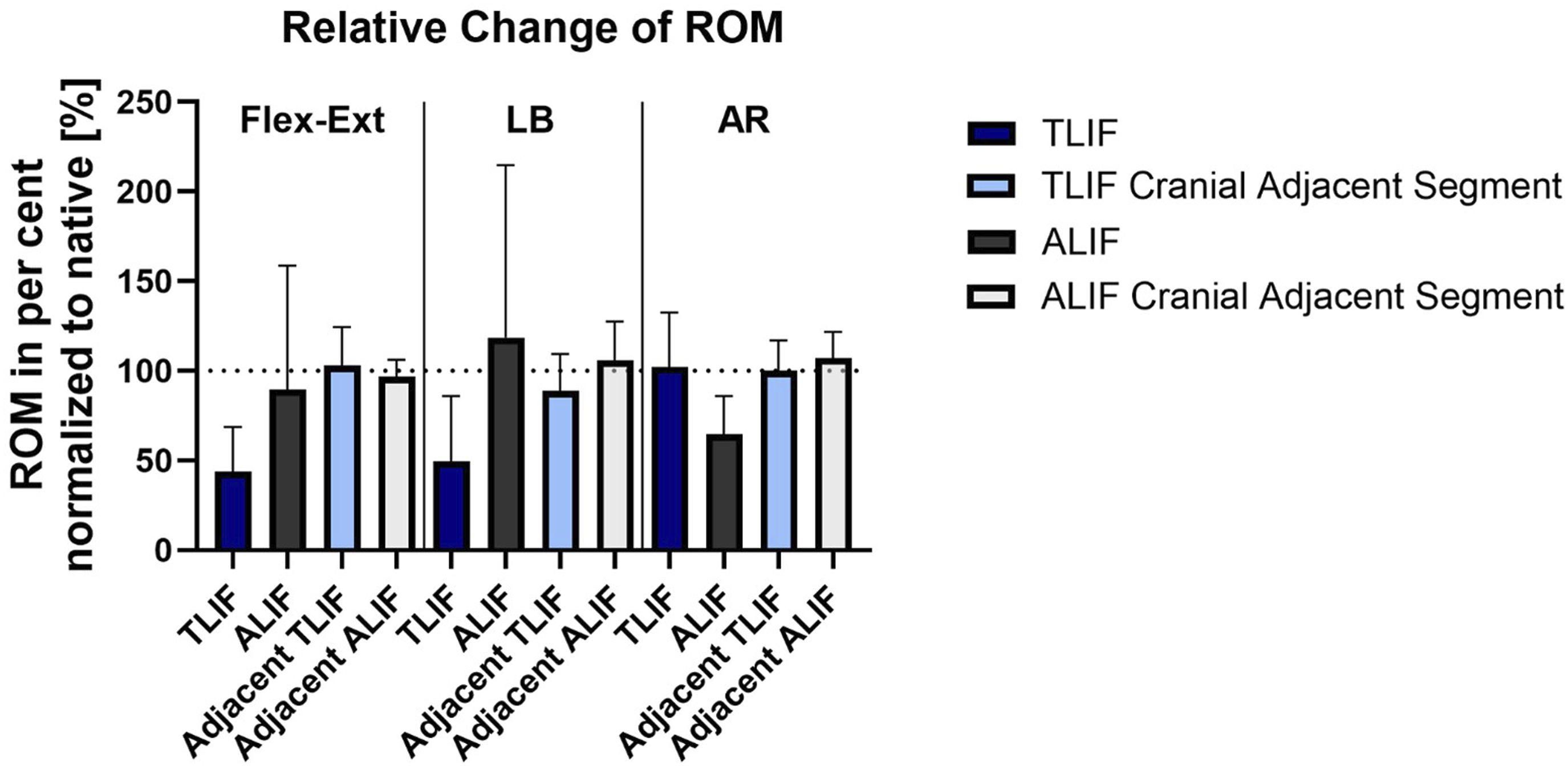
Cranial Adjacent Segment NZ
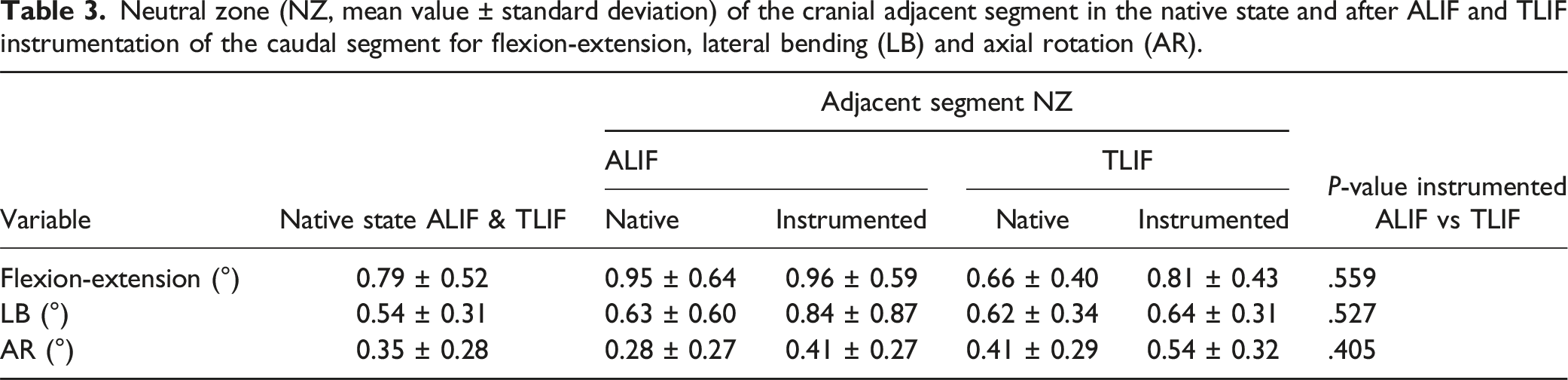
Neutral zone (NZ, mean value ± standard deviation) of the cranial adjacent segment in the native state and after ALIF and TLIF instrumentation of the caudal segment for flexion-extension, lateral bending (LB) and axial rotation (AR).
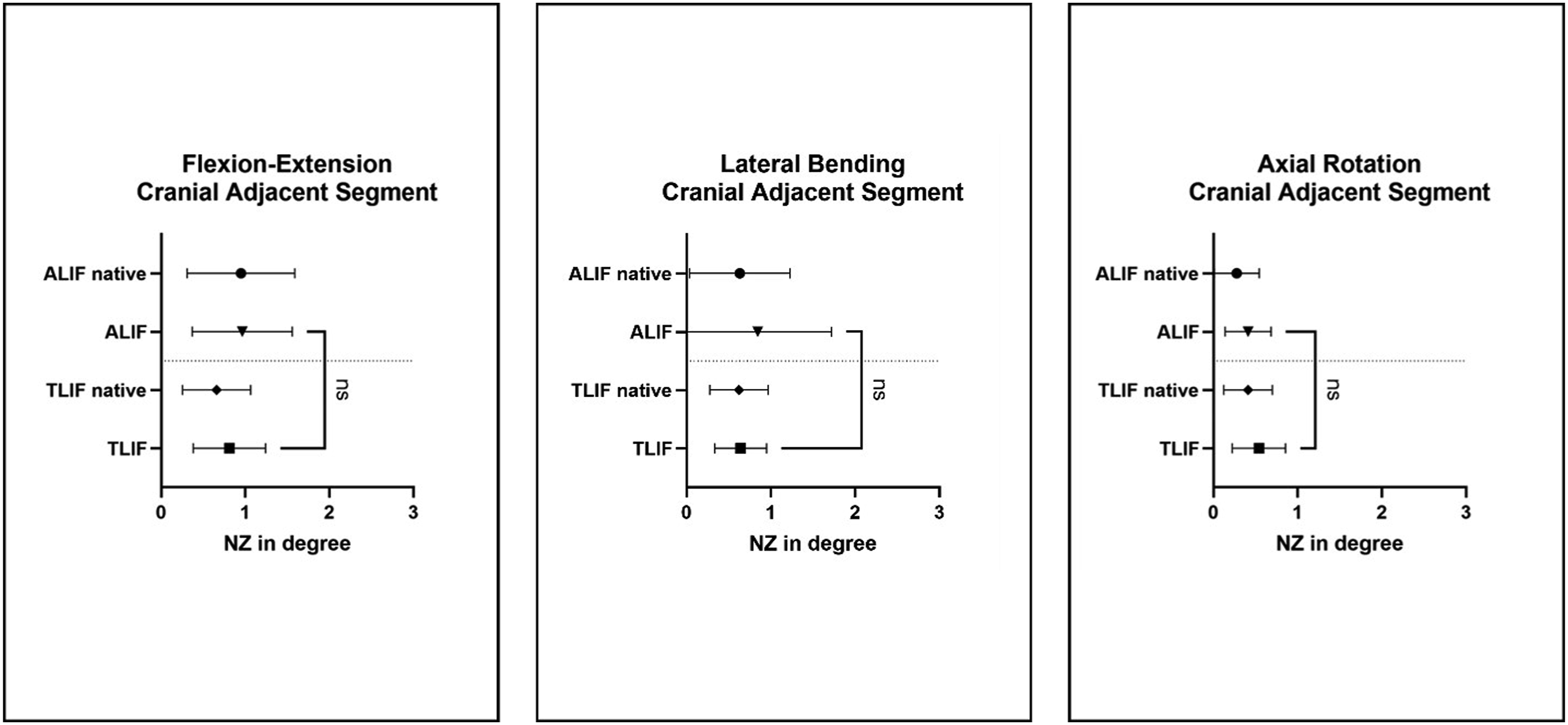
Neutral zone (NZ, mean value ± standard deviation) at the cranial adjacent segment of TLIF and ALIF for flexion-extension (left), lateral bending (middle), and axial rotation (right). Comparisons between the instrumented ALIF and TLIF groups are indicated (ns: not significant).
Discussion
The present study aimed to investigate differences in segmental ROM and NZ of the cranial adjacent segment of ALIF compared to TLIF. The null hypothesis was rejected, as TLIF did not result in a significantly bigger increase in ROM and NZ of the cranial adjacent segment compared to screwed stand-alone ALIF. The present data suggests that adjacent segment motion compensates for ROM restriction caused by lumbar fusion surgery. However, the absolute changes in ROM and NZ of the cranial adjacent segments after instrumentation were minimal and there were no significant differences between the TLIF and ALIF groups. Hence, both techniques appear to have a comparable impact on adjacent segment motion, suggesting that neither TLIF nor ALIF is clearly preferable in terms of reducing the risk of ASD.
Biomechanical Mechanisms
ALIF offers additional anterior column support and leaves posterior stabilizing structures intact, whereas TLIF offers more posterior support. Hence, ALIF is less effective in flexion-extension and most effective in providing stability in AR.22-27 Most biomechanical studies focused on ROM and NZ of TLIF and stand-alone screwed ALIF in the operated segment in not severely degenerated specimens and their findings are consistent with the observations of the present work. In the current study, 2 significant changes of adjacent segment ROM from native to fused state were observed in AR and extension in the ALIF group. In right AR, ROM of the cranial adjacent segment increased significantly after instrumentation, however, the absolute change was as small as 0.3°. In extension, ROM decreased significantly after instrumentation, but the change was less than 1°, with a standard deviation equal to the observed change. Given the minimal absolute values of the changes after instrumentation and the fact that there were no significant differences between the ALIF and TLIF groups in adjacent segment ROM after instrumentation, these 2 significant changes in the ALIF group do not appear to indicate a clinically meaningful difference compared to the TLIF group. Hence, it can be concluded that, based on the present data, both techniques seem to equally predispose degenerated spines of reduced BMD for ASD, which is in agreement with prior clinical research reporting no significant differences between ALIF and TLIF outcomes and reoperation rates.12,16,28,29
Literature Review
Previous biomechanical in vitro studies have predominantly been conducted using healthy bone with normal BMD. Volkheimer et al. conducted a systematic review to summarize the results of these previous in vitro studies focusing on the impact of spinal instrumentation on the adjacent segments with regard to the protocol and loads applied. Their review highlighted that the observed adjacent segment motion after fusion highly depends on the testing protocol and the load application. Only for dynamic implants, most studies did not find significant changes in the adjacent segment motions, independent of which test protocol was used. 30 It remains a subject of debate whether the assumptions underlying the different protocols reflect the postoperative situation of the patients. In this context Malakoutian et al. examined the in vivo kinematics and found that the assumption made for both the stiffness and hybrid protocols – namely that patients move exactly the same way after fusion – does not match the in vivo behavior. 31 The motion of the whole lumbar spine tends to decrease after fusion surgery. Therefore, the gold-standard protocol considering pure bending moment flexibility seems to better reflect postoperative motion. When such protocols are used, the difference in the kinematic changes between the cranial and caudal adjacent segment could be reproduced in specimens with normal BMD. 30 The results of the present study are consistent with these findings and showed comparable results for degenerated spines with reduced BMD. In the current work, the gold-standard pure-bending-moment protocol was implemented following established testing criteria of spinal implants. 21 However, no significant increase in ROM after instrumentation and no significant differences between the 2 investigated techniques were detected. Nonetheless, our team is of the opinion that a testing protocol designed to force the spine more agressively to fulfill a predetermined ROM would not reflect in vivo conditions and should not be used to provoke significant differences.
Compared to previous data using specimens with normal BMD, the present study exhibited greater data scattering.25,30,31 This variability may be attributed to the use of degenerated specimens. Unlike the majority of previous reports, the current specimen set exhibited a lower BMD, potentially leading to reduced screw purchase and weaker fixation with less change of ROM after instrumentation. However, degenerative changes can also involve localized sclerosis with increased density which may enhance fixation in some cases. 32 This duality, characterized by reduced overall BMD with regions of increased density, could have contributed to the greater variability observed in the present data. 33 Moreover, the heterogeneous nature of degenerative changes may have involved asymmetries resulting in inconsistencies and leading to differences between left and right motions.
The pathogenesis of ASD remains unknown. Even though the present study did not identify major differences in adjacent segment ROM between the groups, there may still be some existing differences in the biomechanics of ALIF vs TLIF relevant for ASD. These findings could lead to rethinking of the ASD risk mitigation by prioritizing preoperative management, such as BMD modification, rather than only focusing on procedural modifications. Prior work indicated that segments adjacent to the fusion experience increased stresses and higher disc pressure,34,35 clinically manifesting as accelerated DDD or instability.36-38 Previous biomechanical studies using finite element analysis observed variations in the stress distribution between ALIF and TLIF.39,40 In this context, ALIF demonstrated advantages in stress distribution over TLIF, attributed to its larger footprint. 41 Some clinical studies suggest that posterior fixation favors ASD due to increased motion of the adjacent segment,5,42 whereas other investigations on adjacent segment motion found that ALIF cages had a greater impact on the motion compared to TLIF cages. Such deviations from the results of the present study could be explained by the use of different implants – the majority of previous studies used conventional (not stand-alone) ALIF cages or expandable TLIF cages.23,34
Increased ROM of the adjacent segment alone after instrumentation may not be the primary cause of ASD. Multiple risk factors for ASD have been identified. Patient-based risk factors include severe preoperative existing adjacent segment DDD, high body mass index (BMI), advanced age, reduced BMD, and surgery-related risk factors considering the length of the construct and its sagittal alignment.43-45 Data suggests that in long term patients benefit strongly from properly restored sagittal profile.46,47 Mechanical complications are closely linked to the spinal shape and sagittal parameters can greatly assist surgeons. 48 Both lordosis distribution and inflection point are directly related to patient outcomes and reoperation rates, however, they are not used for surgery planning of short-segment stabilization in all centers. 46
To prevent ASD, semi-rigid fixation techniques have been developed. Designed for long constructs, these techniques aim to reduce stress on the adjacent segments by creating a gradual transition zone at the proximal end of a fusion construct. There are 2 main approaches: pretensioning of the cranial level of the construct and reinforcement of the motion segment adjacent to the construct. An example for the pretensioning approach is the tether pedicle screw system that smoothens the transition at the upper instrumented vertebra. Reinforcement methods include sublaminar tape, pretensioned suture loops, transverse hooks, and lamina hooks. A biomechanical study on sublaminar band tensioning at the cranial adjacent segment observed that the ROM increase at this segment (L2-3) after fusion (L3-S1) could be reduced without increase at the level above (L1-2).49,50 Semi-rigid fixation techniques may not be optimal for short-segment stabilization due to insufficient stability, loss of alignment, and potential higher stresses on screws. Increase micromotion could accelerate loosening and insufficient rigidity can potentially lead to delayed fusion. Overall, semi-rigid fixation techniques are considered as a possible alternative for selected long-segment constructs, where flexibility can help distribute loading across multiple levels and avoid stress concentrations to minimize adjacent segment degeneration. In short segment-constructs, however, these benefits are outweighed by the need for stability and rigidity.51,52
Limitations
This study has some limitations. First, the small sample size limits statistical power. Second, sample heterogeneity limits comparability. Like all transitional zones, the lumbosacral junction has a distinct anatomy making it less comparable to lumbar motion segments. 53 To address this heterogeneity, we reported relative ROM of the operated L4-5 and L5-S1 segments which was normalized to the corresponding native state. The present study focused on cranial L4-5 or L3-4 adjacent segment motions, which are comparable, rather than on the motions of the fused segments as examined in previous studies. 54 Third, isolated directions of motion without physiological influences of muscle forces of soft tissue were investigated. 55 Hence, the results cannot be directly applied to the complex dynamic movements in vivo. However, we used a standardized validated quasi-static loading protocol. 56 Fourth, the present human cadaveric study followed established testing standards without simulation of muscle forces, body weight, and abdominal pressure.21,56 These factors may have a compensatory effect for minor instabilities or, conversely, higher forces may act on the spine in vivo and accelerate instability.55,57 The results of the current in vitro study cannot be directly transferred to the complex movement patterns of the human spine in vivo and only primary stability was assessed.
To our knowledge, the presented study is the first to investigate the adjacent motion of stand-alone ALIF vs TLIF in human spines of reduced BMD. As this is an ex vivo biomechanical work, these findings cannot immediately reframe surgeons’ risk assessment, however, they offer new insights and serve as a valuable foundation for future clinical research. When interpreted within its limitations, the findings of this study may help understand in which cases ASD may occur and how optimal outcome of lumbar spinal fusion surgery can be achieved.
Outlook
To investigate causality, biomechanical predictors of ASD need to be identified for stand-alone ALIF and TLIF. The interplay between patient-specific factors (eg, sagittal alignment, BMI) and surgical technique needs to be investigated in clinical studies. A setup with simulation of muscle forces and moments would make the results more transferable.
Conclusion
This study found no clinically significant difference in adjacent segment motion when comparing TLIF with stand-alone screwed ALIF. Hence, both techniques appear to have a negligible impact on adjacent segment motion in poor bone quality. This suggests that neither TLIF nor stand-alone screwed ALIF increase the risk of ASD due to compensatory motion resulting from an operated adjacent segment.
Footnotes
Acknowledgments
The authors are not compensated and there are no other institutional subsidies, corporate affiliations, or funding sources supporting this work unless clearly documented and disclosed. This investigation was performed with the assistance of the AO Foundation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
ORCID iDs
Data Availability Statement
Data and materials are available on reasonable request.