
Abstract
Study Design
Retrospective cohort study.
Objective
The purpose of this study was to see whether upgrades in newer generation robots improve safety and clinical outcomes following spine surgery.
Methods
All patients undergoing robotic-assisted spine surgery with the Mazor X Stealth EditionTM (Medtronic, Minneapolis, MN) from 2019 to 2022 at a combined orthopedic and neurosurgical spine service were retrospectively reviewed. Robot related complications were recorded.
Results
264 consecutive patients (54.1% female; age at time of surgery 63.5 ± 15.3 years) operated on by 14 surgeons were analyzed. The average number of instrumented levels with robotics was 4.2 ± 2.7, while the average number of instrumented screws with robotics was 8.3 ± 5.3. There was a nearly 50/50 split between an open and minimally invasive approach. Six patients (2.2%) had robot related complications. Three patients had temporary nerve root injuries from misplaced screws that required reoperation, one patient had a permanent motor deficit from the tap damaging the L1 and L2 nerve roots, one patient had a durotomy from a misplaced screw that required laminectomy and intra-operative repair, and one patient had a temporary sensory L5 nerve root injury from a drill. Half of these complications (3/6) were due to a reference frame error. In total, four patients (1.5%) required reoperation to fix 10 misplaced screws.
Conclusion
Despite newer generation robots, robot related complications are not decreasing. As half the robot related complications result from reference frame errors, this is an opportunity for improvement.
Introduction
Pedicle screw fixation provides superior postoperative spinal stability. The freehand approach for screw placement relies on a combination of anatomical landmarks and fluoroscopic guidance. 1 However, reports of screw misplacement using this method have varied widely, ranging from 8.3% to as high as 50.6%.2,3 This is a concern, as malpositioned screws can lead to major neurological, vascular, and visceral complications. In the last decade, the use of robotics in spine surgery has become more popular for its purported increased precision and ability to be unaffected by fatigue. Additionally, robotic-assisted pedicle screw delivery in minimally invasive surgery was viewed as ideal due to the limited need for extensive tissue dissection. Recent radiographic outcome studies have reported superior radiologic accuracy, nearing an accuracy rate of 99% with the newest generation robot.4-11 The purpose of this investigation was to see whether updates in these newest generation robots also result in improved safety and clinical outcomes.
Methods
The Cedars-Sinai Medical Center Institutional Review Board (IRB) approved this retrospective cohort study (00002314). The study does not require informed consent given the data reviewed was deidentified and collected in accordance with the institution’s standard of care. This study included consecutive patients undergoing robotic-assisted spine surgery between December 2019 to November 2022. Robots for assisted pedicle screw placement were used by 14 surgeons utilizing the Mazor X Stealth EditionTM (Medtronic, Minneapolis, MN). Only patients undergoing pure sacroiliac joint fusions were excluded from this study. All remaining patients, regardless of age and available follow-up time, were included in the final analysis. Diagnoses indicating surgery, number of instrumented levels, number of planned robot screws per patient, robot related complications, and robot related reoperations were recorded. Only descriptive statistics (mean, standard deviation) were used as this was not a comparative study.
Results
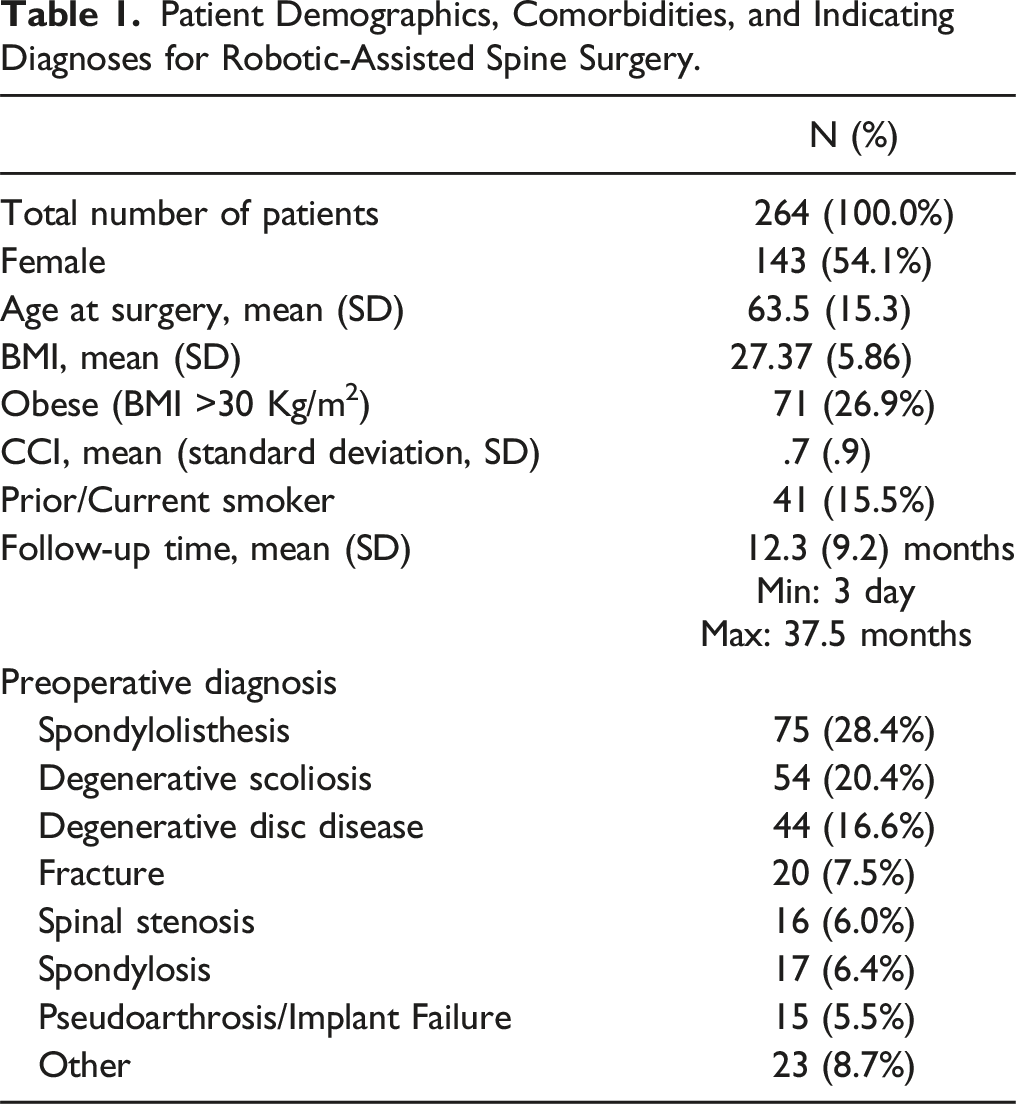
Patient Demographics, Comorbidities, and Indicating Diagnoses for Robotic-Assisted Spine Surgery.
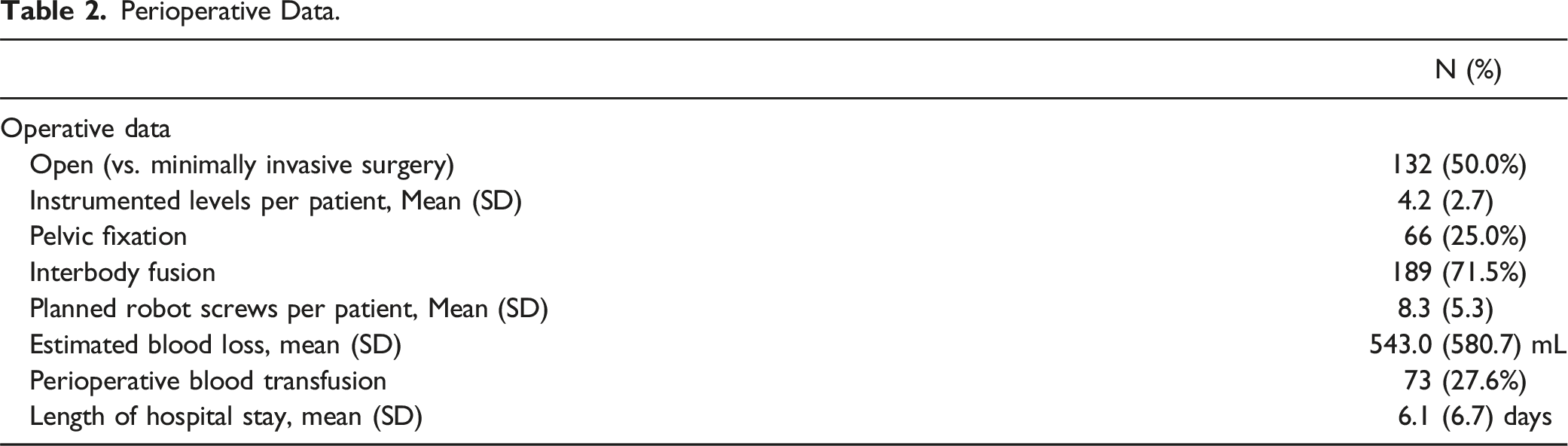
Perioperative Data.
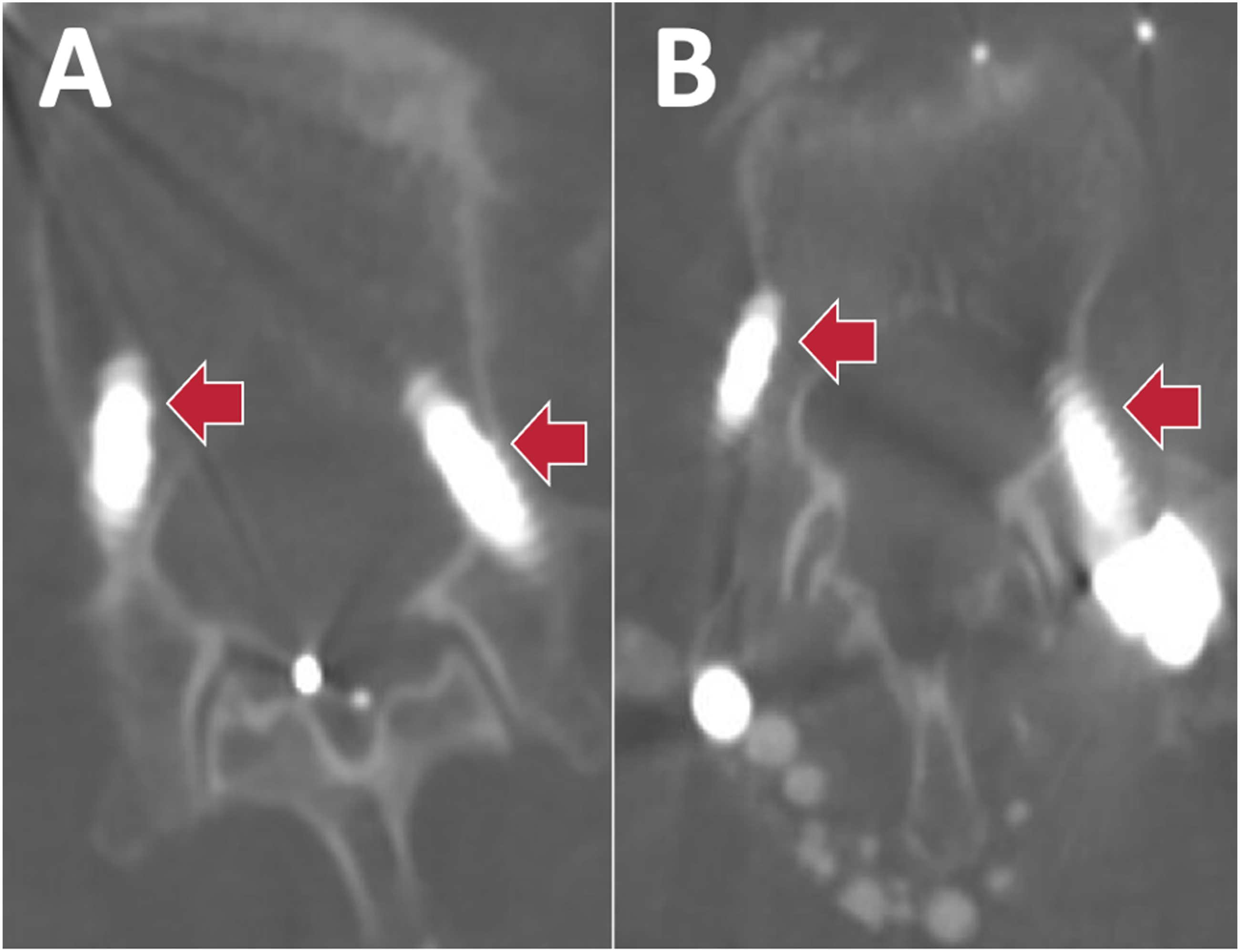
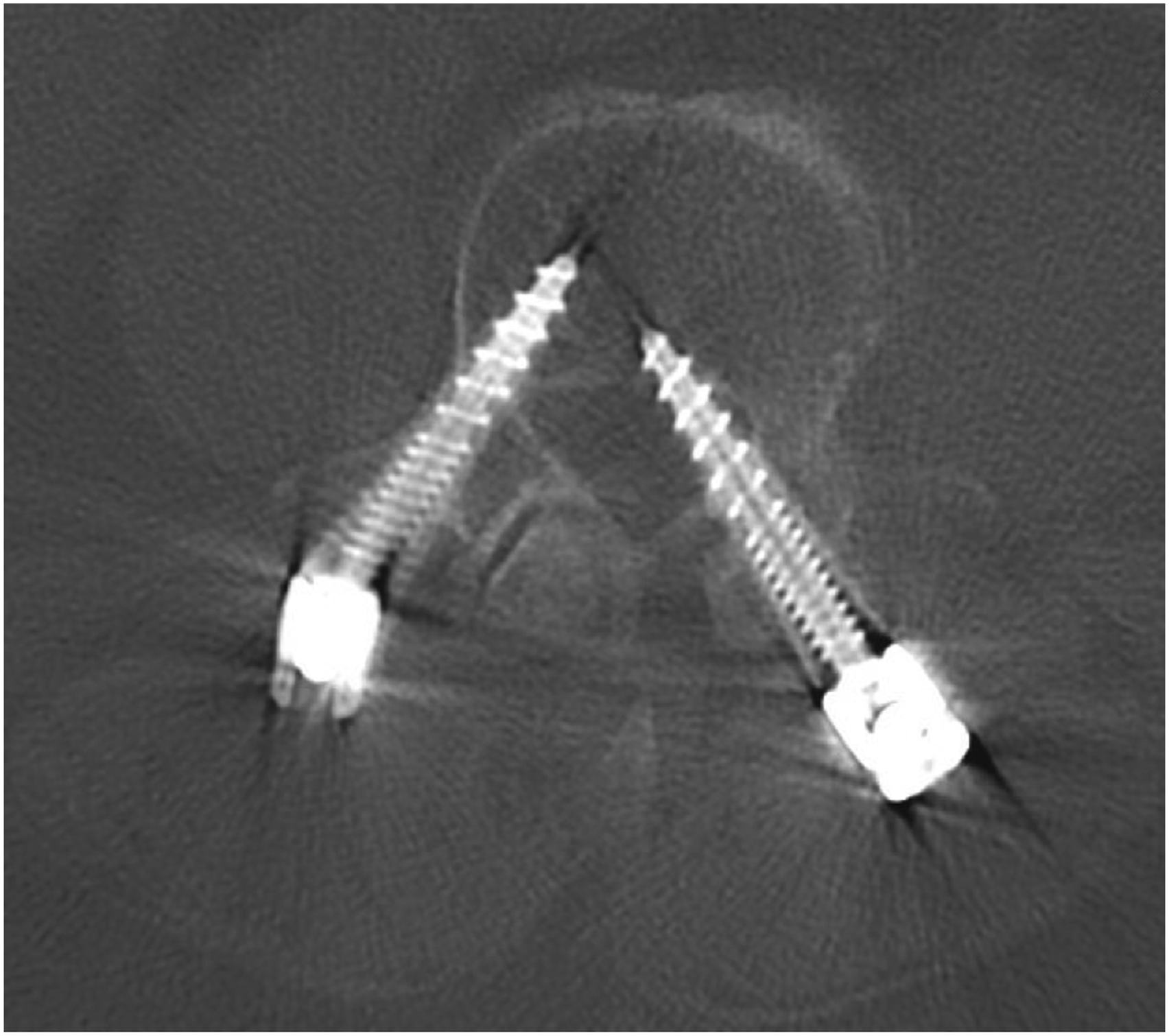
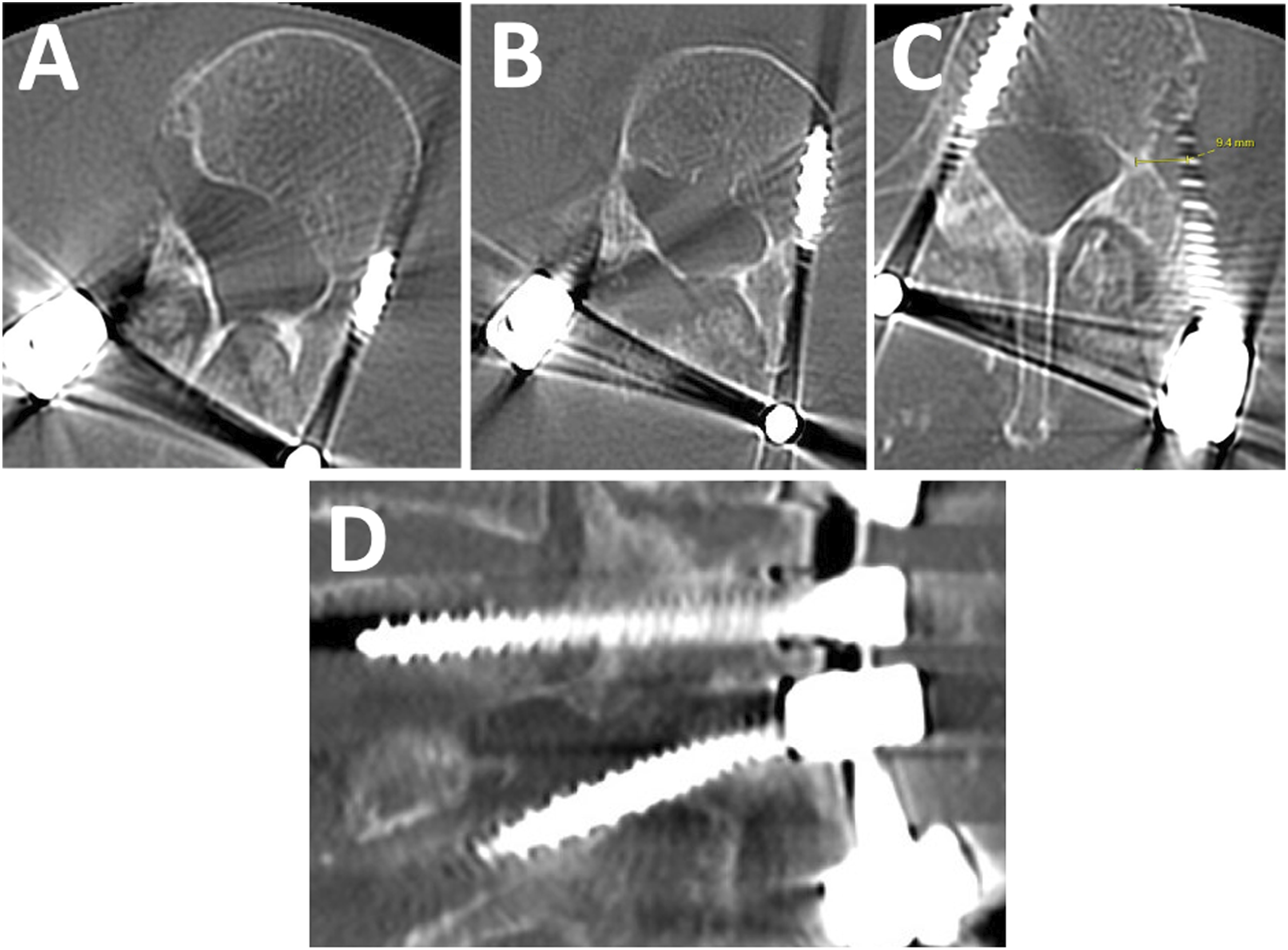
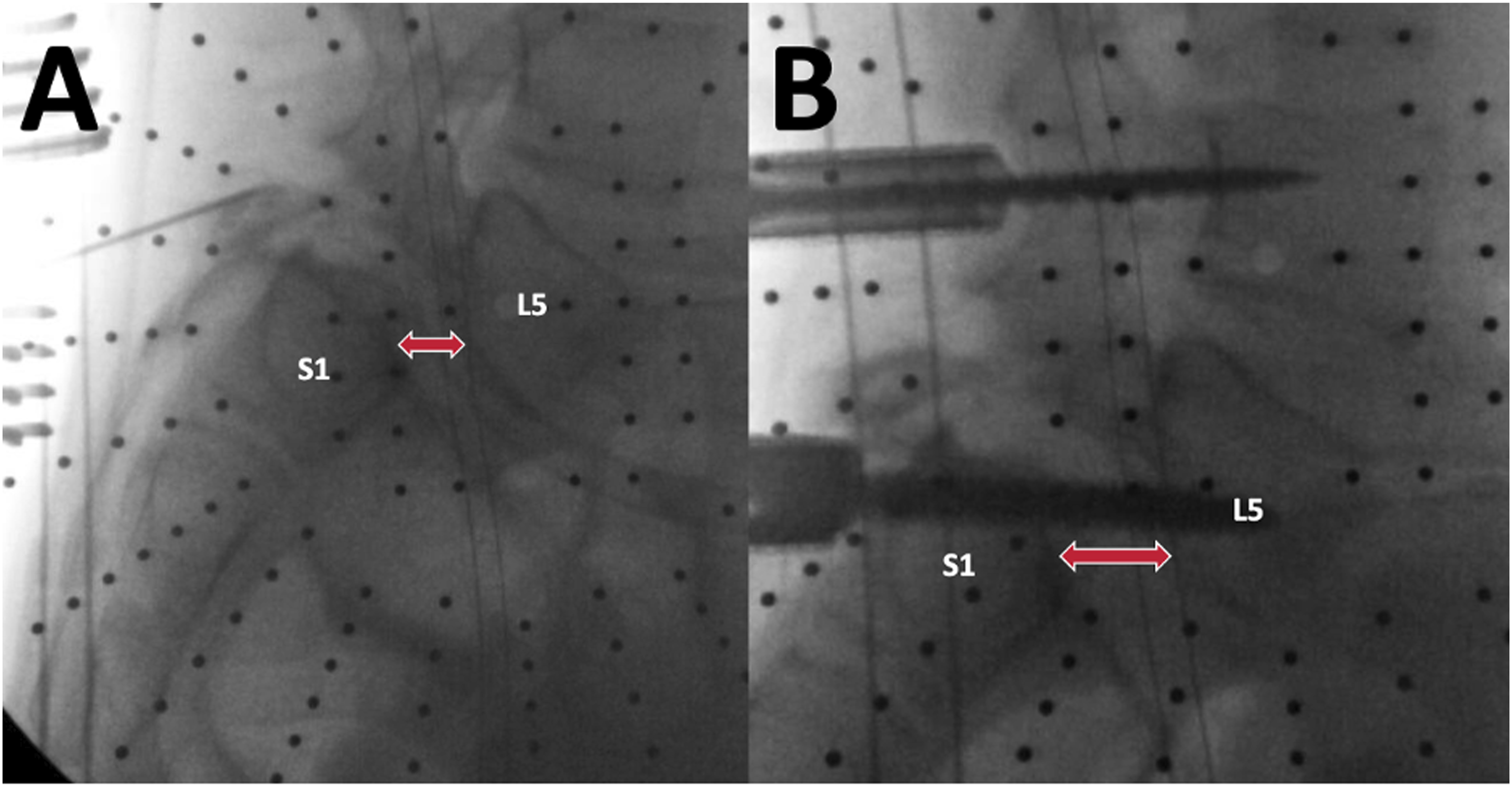
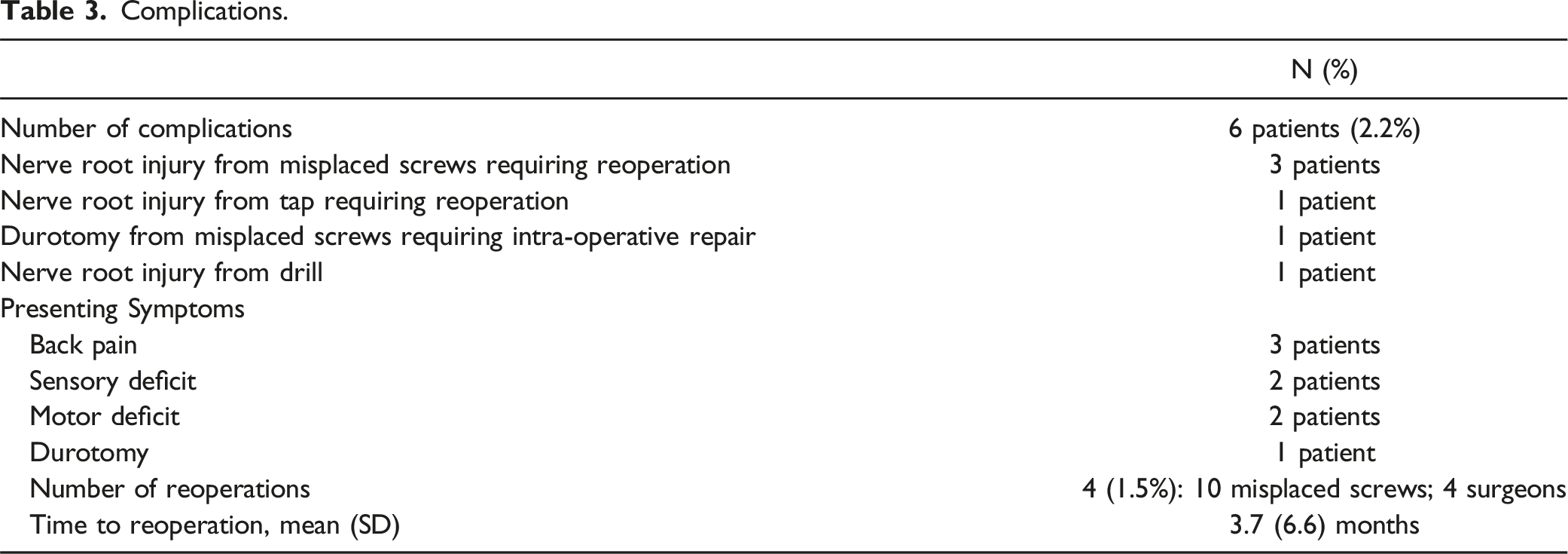
There were six patients (2.2%) who had robot related complications. Three patients had temporary nerve root injuries from misplaced screws that required reoperations (Figures 1-3), one patient had a permanent 1/5 motor deficit from the tap wrapping the L1 and L2 nerve roots that required a reoperation (Figure 4), one patient had a durotomy from a misplaced screw that required laminectomy and intra-operative repair, and one patient had a sensory L5 nerve root injury from the drill (Figure 5). Half of these complications (3/6) were due to a reference frame error. In total, four patients (1.5%) required reoperations to fix 10 misplaced screws (Table 3) (Figures 1-4), and they were all performed by four different surgeons. Years in practice for these surgeons ranged from 9 years to 27 years, and all had freehand navigation experience. These complications were not clustered in the early learning curve of robot usage of the surgeons. Average time to robotic related reoperations was 3.7 months ± 6.6 months (range 5 days – 1.1 years). (A) Medial breach of right T10 pedicle screw with lateralized left T10 pedicle screw and (B) medial breach of right T11 pedicle screw with lateralized left T11 pedicle screw in a 76 year old male presenting with worsening thoracic back pain after a left lateral T12-L1 discectomy + T10-L3 PSF. Both screws were shifted towards one side by about 10 mm (red arrows). The authors believe that the reference frame placed on the posterior superior iliac spine was too far from T10/T11, resulting in movement over the distance that was not detected. The patient later required a reoperation for screw replacement. Legend: PSF, posterior spinal fusion. (A) Medial breach of left L1 pedicle screw and (B) lateralized right L2 pedicle screw in a 71 year old female presenting with back pain and new 1/5 weakness of the right quadriceps and iliopsoas muscles after L1-Pelvis PSF. The authors believe this patient had a reference frame problem, as both screws were shifted by about 10 mm (red arrows) in the same direction. The reference frame was placed on the posterior superior iliac spine. The patient later required reoperation for screw removal. Medial breach of left L4 pedicle screw in a 70-year-old male who presented with numbness and 3/5 weakness in the left lower extremity after undergoing L4-S1 ALIF + PSF. The attending surgeon believes that the soft tissue pushed against the cannula, resulting in a medial breach of the spinal canal at L4. The patient later required a reoperation to remove screw. Of note, the reference frame was placed on the posterior superior iliac spine. Legend: ALIF, anterior lumbar interbody fusion; PSF, posterior spinal fusion. (A) Lateralized left L2 pedicle screw, (B) lateralized left L3 pedicle screw, (C) lateralized left L4 pedicle screw, and (D) superior misplacement of left L5 pedicle screw into the L4-L5 disc space in a 76-year-old female who presented with new back and left lower extremity pain after undergoing L4-S1 ALIF and T10-Pelvis PSF for long-standing scoliosis. Of note, the reference frame was docked on to the spine, rather than the posterior superior iliac spine. Patient later required a reoperation to replace screws. Legend: ALIF, anterior lumbar interbody fusion; PSF, posterior spinal fusion. This patient had a grade IV spondylolisthesis at L5-S1. When the S1-L5 transdiscal screw was placed, L5 was pushed away relative to the reference frame on the posterior superior iliac spine, which the surgeon believes resulted in the drill hitting the nerve root. This resulted in an immediate spike in the patient’s EMGs, her leg kicked, and she had went on to have 3 months of a burning sensation on her dorsal foot. (A, B) demonstrate the distance between L5 and S1 (red arrow) before and after the transdiscal screw was placed, respectively. Complications.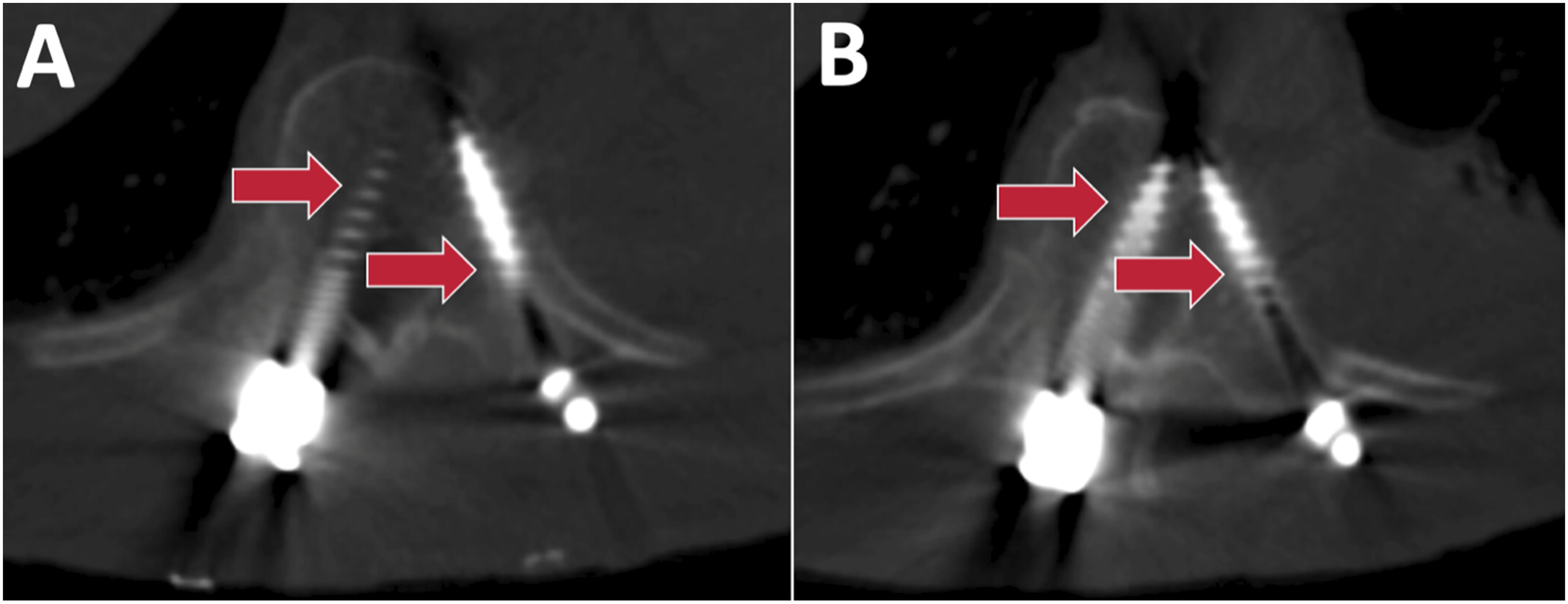
Discussion
Despite using the newest generation robot, the complication rate remains substantial at 2.2% and surgical reoperation rate to fix misplaced pedicle screws at 1.5% (4/268 patients).
Previous studies on earlier generation robot-assisted screw systems reported comparable accuracy results to conventional free-hand technique. Using the Gertzbein and Robbins Scale, Schatlo et al 12 observed 83.6% of screws as perfect trajectories (Grade A) and 7.8% of screws as Grade B, which was similar to the fluoroscopic guided group. A later study reported similar results, finding 84.4% of robotic screws had trajectories of either Grade A or B. 13 In contrast, one report by Ringel et al 4 found the free-hand group to perform superiorly, with 93% of screws achieving acceptable positions compared to 85% in the robotic group. These earlier studies used a first generation robot, SpineAssistTM (Mazor Robotics Ltd., Caesarea, Israel), introduced in 2004. Later studies reporting on an updated robotic system platform, the Mazor XTM (Mazor Robotics Ltd., Caesarea, Israel) introduced in 2016, have shown improvements. The first study to report on the Mazor X system evaluated 20 patients and 75 screws, finding an accuracy rate of 99%. 14 When compared to CT-image guided navigation (CT-IGN) systems without robot, Mazor X achieved a similar screw accuracy of 99.5%, compared to 95.2% in the navigation group. 15 Mao et al also found a similar screw accuracy between 39 Mazor X cases and 46 CT-IGN cases, and also reported that the robot-assisted technology achieved a higher percentage of grade A type screws (robot: 86.2% vs navigation: 66.0%). 16
Summary of Studies Reporting on Reoperations for Misplaced Pedicle Screws Using Robotic-Assistance.
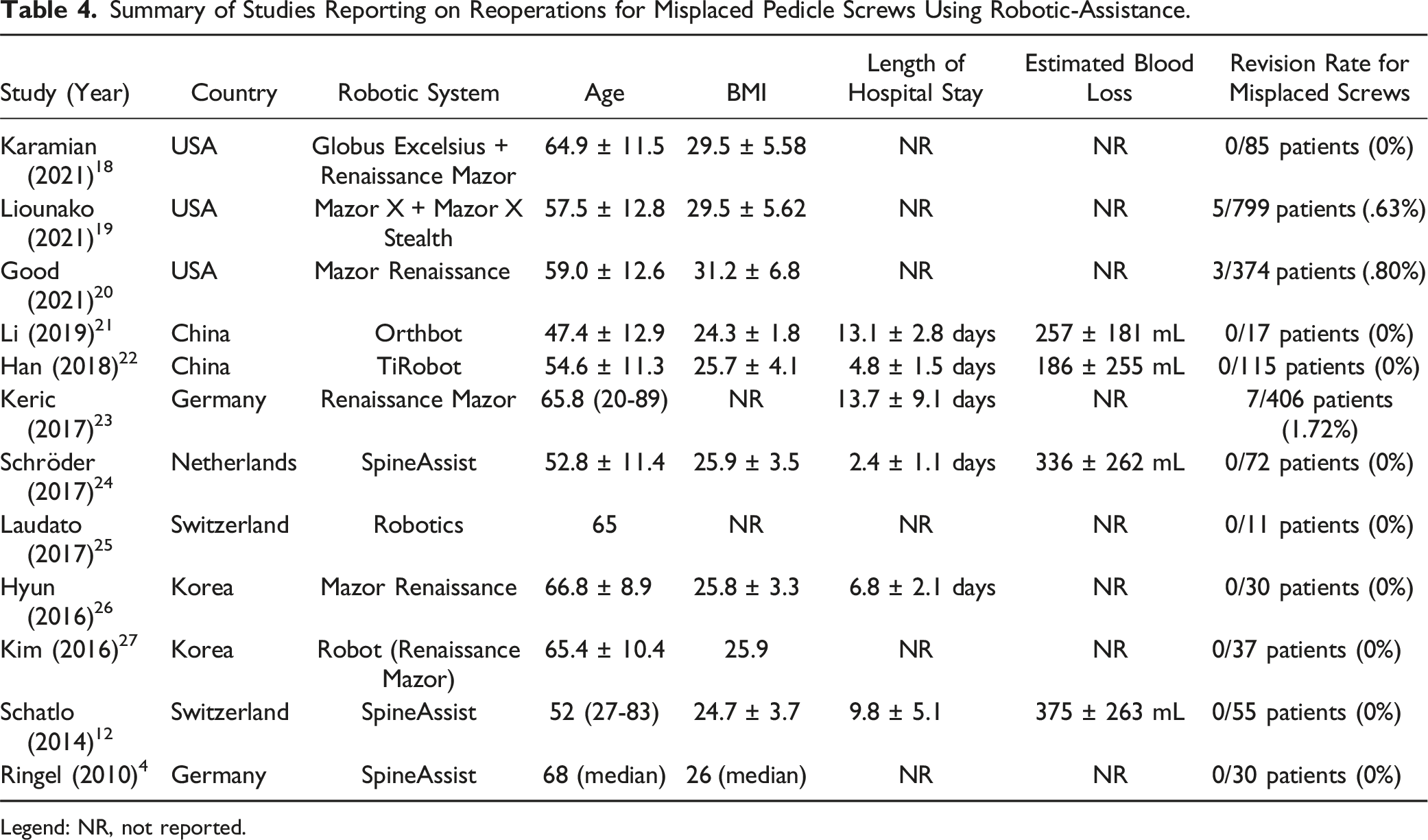
Legend: NR, not reported.
There was no case in which it seemed the mechanical part of the robot failed. Instead, complications in our cohort could better be described by navigation failures. In particular, half (3/6) of the patients from our study who had a robot related complication were found to have reference frame errors: likely a technical error on the part of the surgeon that occurred while using the robot, resulting in the reference frame unintentionally moving during surgery. Thus, reducing the frequency of navigation failures is a potential area for improvement to optimize robotic spine surgery. Based upon our cases, we do not recommend placing pedicle screws using only a spinous process clamp as a reference frame since it is not rigid and is prone to unintended movement. Additionally, we recommend placing the reference frame as close as possible to the levels of surgery. There were two patients who had complications from misplaced screws far from the posterior superior iliac spine where the pelvic reference frame was placed, with misplaced screws found at T10 and T11 for one patient, and at L1 and L2 for a second patient (Figures 1, 2). When using the Mazor robot, a pedicle screw based reference frame is preferred.
Limitations
There are several limitations to this study. First, this was a retrospective analysis and is thus limited by patients potentially lost to follow-up, though most of these complications were noted in the perioperative period. Secondly, intraoperative screw malposition and revision prior to exiting the operating room was not recorded. Third, the retrospective nature of the study limited the ability to analyze other variables, including bone preparation technique and general workflows of each surgeon and the frequency of their accuracy checks. However, the authors of the current study recommend frequent accuracy checks with a chicken foot prior to bone preparation for each screw, and the use of a high speed burr for those bone preparations. Lastly, this study is also limited by the absence of a non-robot comparative group.
Conclusion
Despite using the latest generation robot, we found complication rates to be 2.2% (6/268) and reoperation rates to fix misplaced pedicle screws to be 1.5% (4/268 patients), occurring amongst four different surgeons. This is a higher rate than most previous studies using earlier generation robot systems. As half the robot related complications resulted from reference frame errors, this is an opportunity for improvement.
Footnotes
Author Contributions
Skaggs: Royalties on Zimvie and Medtronic Tether, Zimvie fusion system; consultant for Zimvie and Globus. Kim: Consultant for Medtronic, DePuy. Nomoto: Teaching agreements with Globus, NuVasive, Medtronic, DePuy. Baron: Royalties for textbooks by McGraw Hill and Elsevier. Walker: Consulting for Glonbus. Sy and Farivar: None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.