
Abstract
Study Design:
Retrospective study.
Objective:
To report the technical details of subaxial cervical pedicular screw insertion via the nonanatomic axis (nAA-CPS) and evaluate its clinical safety and accuracy.
Methods:
The nAA-CPS technique was performed in 21 patients. Preoperative and intraoperative management-related details are described, and a manipulation protocol is presented. Clinical outcomes were used to assess the safety and accuracy of screws was evaluated using postoperative computed tomography (CT) according to the pedicle perforation grading system, and the nonanatomic pedicle transverse angle (nPTA) and nonanatomic pedicle axis length (nPAL) were assessed based on pre- and postoperative CT images.
Results:
According to “one constant entry point (EP) and two perpendicular trajectory angles” protocol, nAA-CPS was performed without much interference from the muscles. No intraoperative or postoperative neurovascular complications related to the technique were observed. Of the 112 inserted screws, 78 (69.64%) were assessed as grade 0, 24 (21.43%) as grade 1, 4 (3.57%) as grade 2 and 6 (5.36%) as grade 3. The overall rate of correct position (grades 0 and 1) was 91.07% (102/112), and the rate of malposition was 8.93% (10/112), including five screws implanted medially and the other five laterally. The nPTA was highly consistent on pre- and postoperative CT (P < .05), while postoperative nPAL was significantly shorter than preoperative nPAL (P > .05).
Conclusions:
Clinically, the accuracy and safety of nAA-CPS was similar to the traditional CPS technique. The protocol, derived from previous radiological studies and workshops, greatly helped standardize clinical manipulation; thus, nAA-CPS is a promising alternative to the traditional CPS.
Introduction
Lateral mass screw (LMS) and cervical pedicular screw (CPS) are the two major options for posterior cervical fixation. Inserting screws into the lateral mass is relatively easier and safer than insertion into the cervical pedicle, hence, increasing popularity of LMS fixation.1-4 However, the biomechanical advantage of CPS cannot be overlooked when correction of cervical deformity, or other rigid multiple segmental reconstructions, are required. 5 The pedicle of the subaxial cervical spine presents a smaller diameter and a larger convergence angle than those of the thoracic or lumbar vertebrae, suggesting that CPS insertion poses a risk to the neighboring neurovascular structures. Various techniques have therefore been reported to improve the safety and accuracy of the CPS technique.6-11
In a previous study, we proposed the concept of cervical pedicular screw insertion via the nonanatomic axis (nAA-CPS) to lessen the interference from abundant muscles during screw canal preparation. The entry point (EP), trajectory, and relevant parameters were identified by a radiological study, and the primary manipulation protocol was established by the workshop (Figure 1). These results indicate that nAA-CPS is feasible; however, the advantage of lesser amount of interference from soft tissue, as well as the safety and accuracy of the technique, has not been clinically verified. The present study aimed to address these problems.
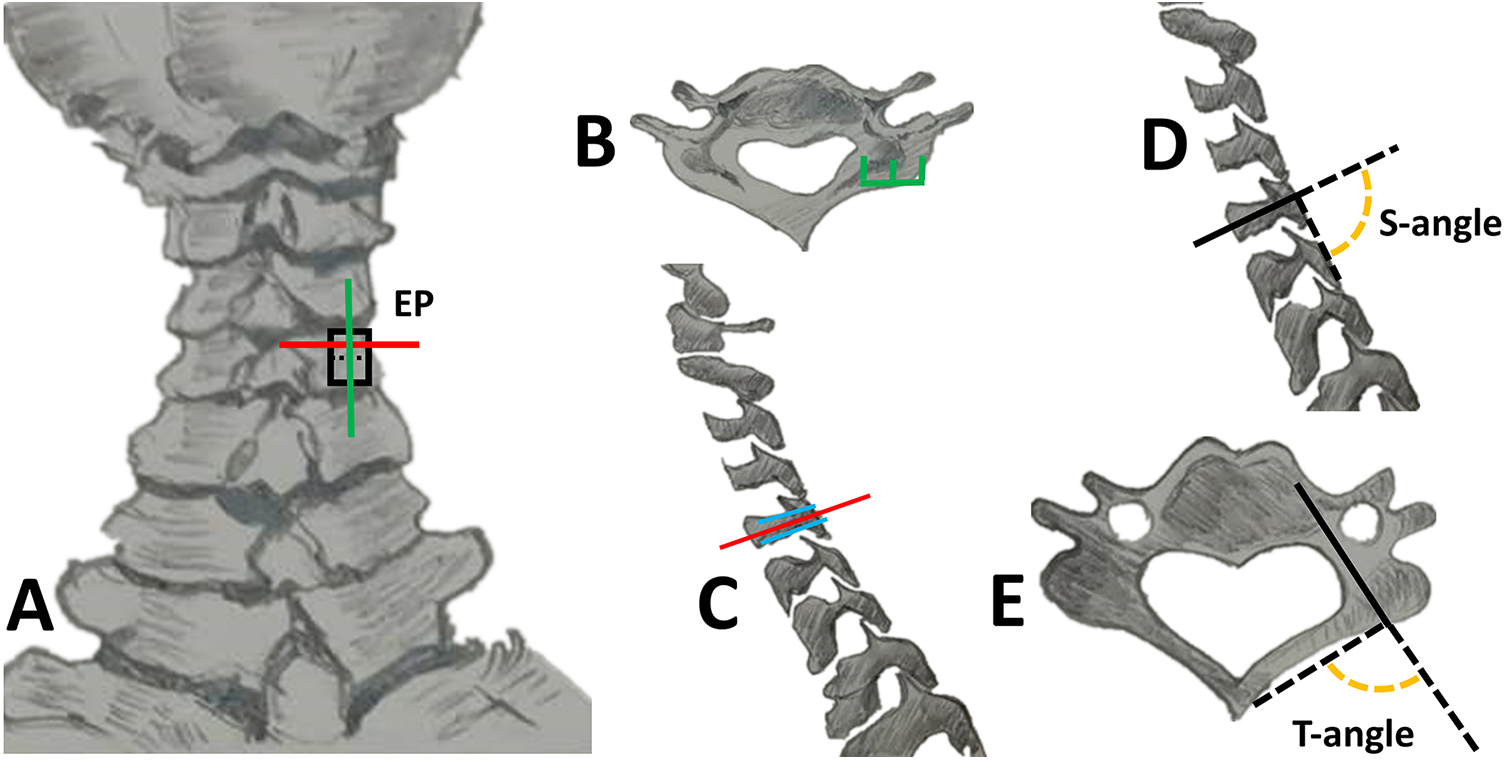
Design of the entry point and two perpendicular angles (A) The entry point (EP) is marked on a dried cervical vertebrae specimen: the green line is the longitudinal midline of the lateral mass (borders outlined by black lines), while the red line is the horizontal line that bisects the upper half of the lateral mass; (B) The EP is located at the midpoint of the lateral mass width (the transverse plane of c5 vertebra on CT scan); (C) Determination of the horizontal coordinate of the EP on the paramedian sagittal plane of C5: the blue lines are the upper and lower borders of the pedicle, and the red line is the pedicular axis in the sagittal view; (D) S-angle: the angle between the nonanatomic axis (nAA) and tangent line of the posterior surface of the lateral mass and the inferior line in the paramedian sagittal plane of the C5 vertebra; (E) T-angle: the angle between the nAA and the line connecting the EP and the conjunction of the ipsilateral lamina and spinal process in the transverse plane of the C5 vertebra.
Materials and Methods
The study was approved by the ethics committee of the Army Medical Center of PLA (IRB approval number: 2019115) and was conducted according to the principles of the Declaration of Helsinki. It was registered in the Chinese Clinical Trial Registry (registration number: ChiCTR2000033821). Between July and November, 2020, nAA-CPS was performed in 21 patients. The enrolled cohort comprised 16 males and 5 females, with an average age of 50.1 (range: 19-75) years. The disease spectrum included trauma (n=19), tuberculosis (n=1), and dumbbell-shaped schwannoma (n=1); in total, 112 nAA-CPSs were inserted.
Preoperative Plan based on Imaging Assessment
Radiologic evaluation of the patients included cervical radiographs in anterior-posterior (AP) and lateral views, computed tomography (CT) (1.0-mm thick slice cuts), and magnetic resonance imaging (MRI) with a 1.5-Tesla scanner. In those with a significant variation in the vertebral artery course, deformity of the screw path, or a diameter of the cervical pedicle less than 4.5 mm, LMS fixation was selected instead of nAA-CPS.
Critical indices related to screw insertion were preoperatively assessed; the nonanatomic pedicle transverse angle (nPTA) referred to the angle between the midline of the vertebral body and the nonanatomic axis (nAA), while the nonanatomic pedicle axis length (nPAL) referred to the distance from the EP to the anterior border of the vertebral body via the nAA.
Surgical Procedure
Exposure and Identification of the EP of nAA-CPS
The posterior midline approach was used. Posterior arches and lateral masses of C3-C7 were exposed. After identifying the boundary of the lateral mass, the center of the upper half of the lateral mass was selected as the EP of nAA-CPS (Figure 2A).
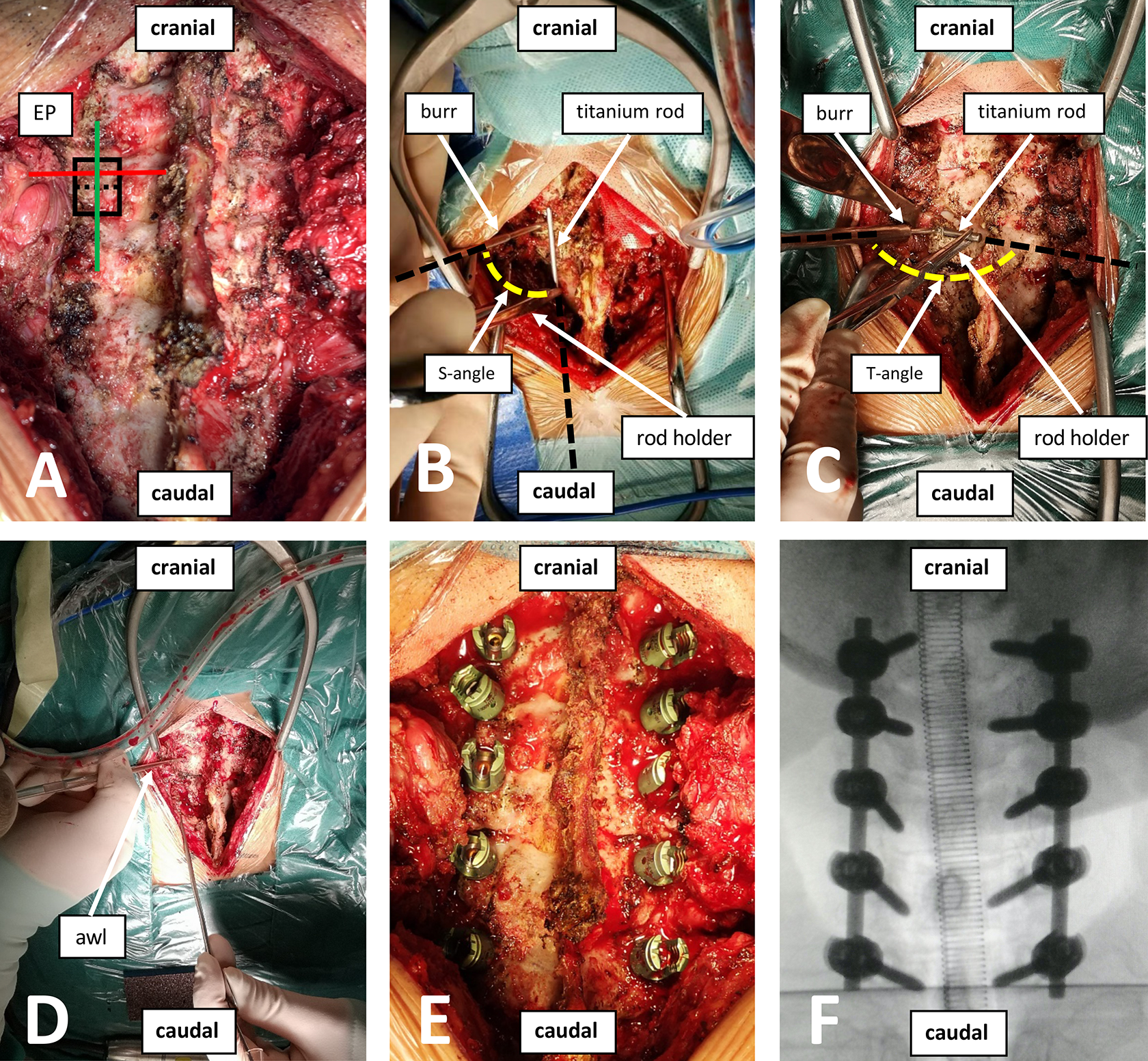
Surgical procedure (A) Identifying the boundary of the lateral mass, the center of the upper half of the lateral mass was selected as the entry point (EP) of the cervical pedicular screw insertion via the nonanatomic axis (nAA-CPS); (B and C) A short titanium rod was used as a reference tool and was placed parallel (on the surface of neighboring lateral mass) to the longitudinal axis of cervical spine, transversely (from EP to root of the spinal process). The angle between the extensions of the 2 dotted white lines is perpendicular (S-angle and T-angle); (D) A high-speed burr, 2mm in diameter, was used to penetrate the cortical surface of EP, and an awl was inserted along the designed trajectory mentioned above until a depth of 18 mm to 20 mm was acquired; (E and F) The integrity of the canal was confirmed by probing the wall of the canal; if no breach was detected, a poly-axial screw of appropriate length, 3.5 mm in diameter, was inserted.
Intraoperative Confirmation of Trajectory in the Sagittal and Transverse Planes
According to our previous radiological study and workshop on dry bone specimens, two perpendicular angles were selected to confirm the trajectory in the sagittal and transverse planes. A short titanium rod, used as a reference tool, was placed parallel (on the surface of the neighboring lateral mass) to the longitudinal axis of the cervical spine (S-angle), transversely from the EP to the root of the spinal process (T-angle) (Figure 2B, C). A high-speed burr with a diameter of 2 mm was used to penetrate the cortical surface of the EP, and an awl was inserted along the abovementioned trajectory until a depth of 18-20 mm was acquired. Probe palpation was performed to confirm the integrity of the canal wall; if no breach was detected, a polyaxial screw of appropriate length, 3.5 mm in diameter, was inserted (Figure 2D-F).
Unusual Situations and Solutions
Intraoperative fluoroscopy is mandatory in unusual situations, such as if there is an abrupt sense of awl failure during canal preparation; if a breach is detected within a short depth of the wall; and if uncommon venous bleeding indicates the canal invading the vertebral artery foramen or spinal canal.
Under ideal conditions, the tip of the screw during nAA-CPS should be located at the level of the lateral 1/4 of the vertebral body in the AP view. During lateral fluoroscopy, the tip of the screw should be located between 1/2 and 3/4 of the vertebral body. A screw tip too close to the spinous process in the AP view indicates that the screw invades the spinal canal; otherwise, the vertebral artery foramen is invaded. Furthermore, a screw tip exceeding 3/4 of the vertebral body in the lateral view indicates the screw penetrating the anterior-lateral cortical bone of the vertebral body.
Assessment of Screw Position and Complications
All patients underwent CT before discharge. Both the nPTA and nPAL were assessed on postoperative CT and compared with preoperative values to evaluate the standardization of the technique. It is noteworthy that the nAA was replaced with the axis of screw for both postoperative nPTA and nPAL.
Screw accuracy was evaluated according to the of pedicle perforation grading system 12 : grade 0 – the screw was located within the pedicle; grade 1 – perforation less than 25% of the screw diameter; grade 2 – perforation between 25% and 50% of the screw diameter; grade 3 – perforation > 50% of the screw diameter. Grades 0 and 1 were classified as the correct position, and grades 2-3 as malposition. Intraoperative and postoperative complications were recorded.
Statistical Analysis
IBM SPSS Statistics (version 19, IBM Corporation, Armonk, NY) was used for statistical analysis. All parameters are presented as mean ± standard deviation. A paired t-test was used to determine significant differences; a P-value less than .05 was considered statistically significant.
Results
Clinical Outcomes
Surgeries were performed as planned; there were no major complications, such as spinal cord injury or vertebral artery involvement, and doctors reported no interference from abundant muscles during screw canal preparation and screw insertion. The average time for a single screw insertion was 6.8 minutes.
Position of Screws
The nAA-CPS technique was consecutively performed in 21 patients. In total, 112 screws were implanted; these were classified as grade 0 in 78 (69.64%), grade 1 in 24 (21.43%), grade 2 in 4 (3.57%), and grade 3 in 6 (5.36%) insertions (Figure 3A-F). The overall rate of correct position (grades 0 and 1) was 91.07% (102/112), while the rate of malposition was 8.93% (10/112). The highest malposition rate was 16.67% for C4, while that for C3 was significantly lower than for other segments (Table 1). The direction of perforation included 5 screws implanted medially, with the other 5 laterally; the average pedicle width (PW) was 5.12 ± 0.96 mm, no serious neurovascular complications directly related to the pedicle screw occurred (Table 2).
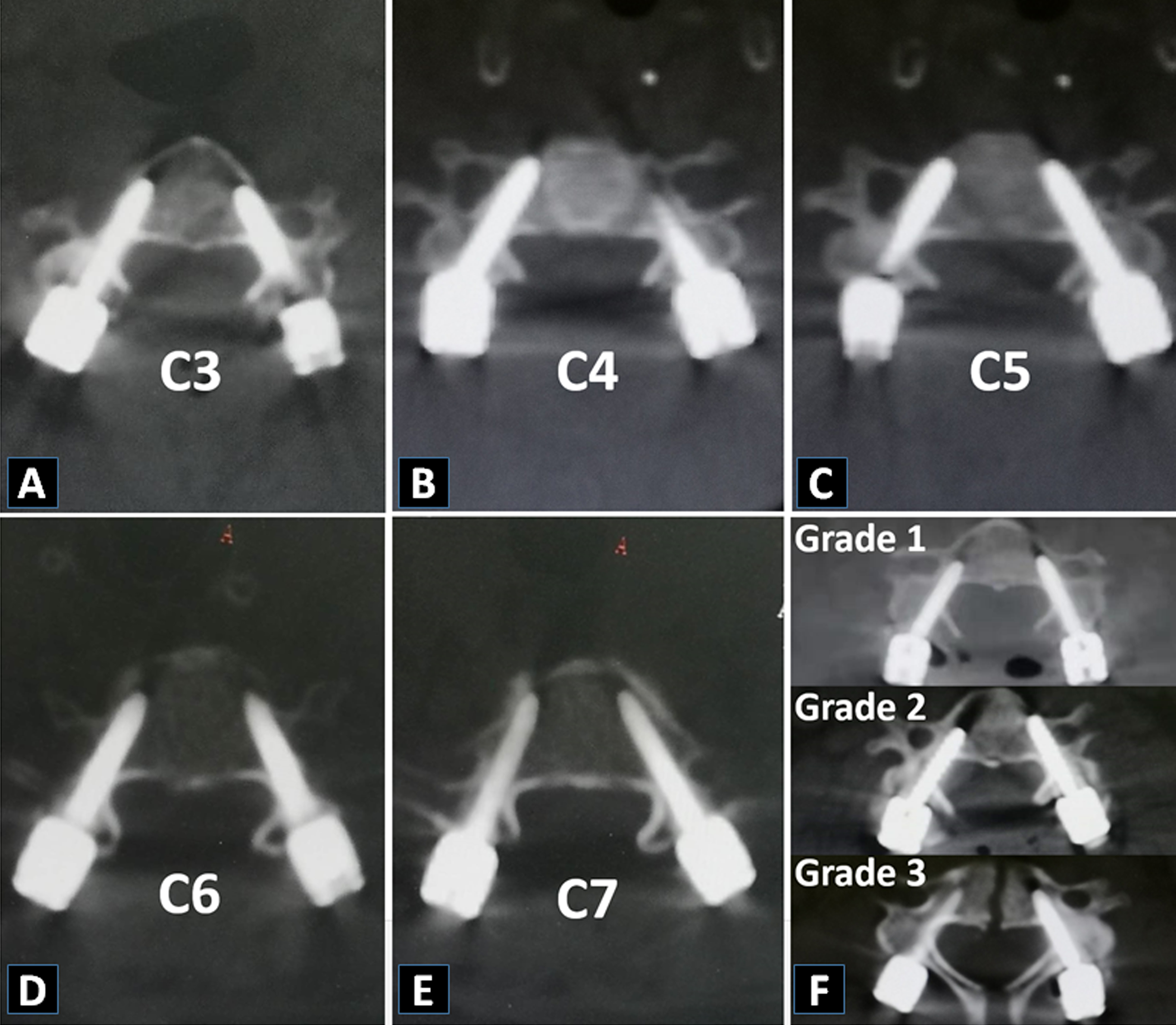
Pedicle perforation grading system (A-E) Grade 0 from C3-C7, grade 0: the screw was located within the pedicle; (F) Three left pedicle screws showed different perforation rate, grade 1: perforation less than 25% of the screw diameter, grade 2: perforation between 25% and 50% of the screw diameter, grade 3: perforation > 50% of the screw diameter.
Distributions of nAA-CPS at Different Segments and Grade of Pedicle Perforation.
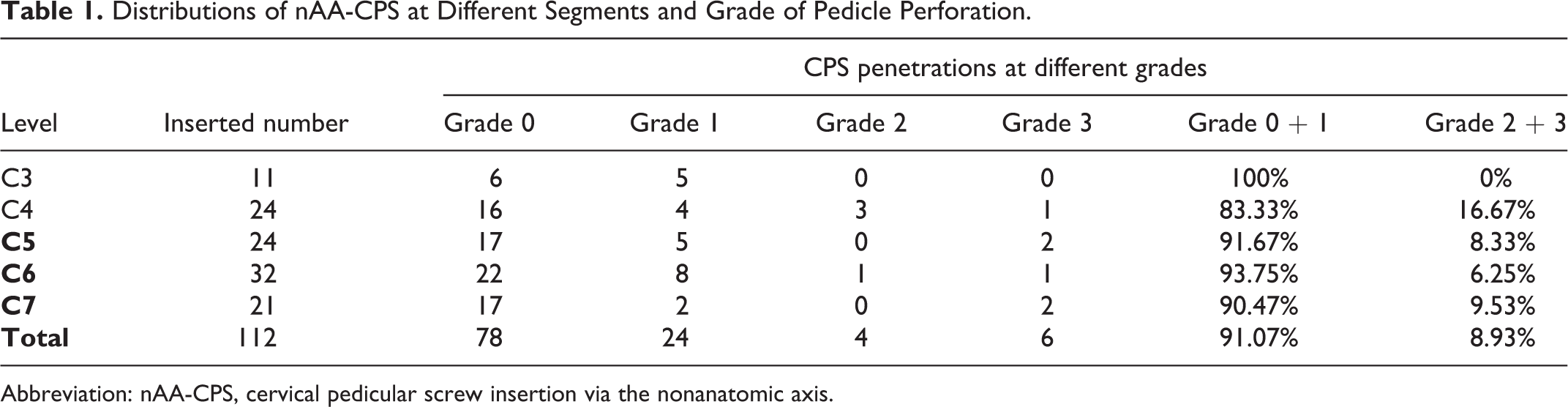
Abbreviation: nAA-CPS, cervical pedicular screw insertion via the nonanatomic axis.
Summary of Malpositioned nAA-CPS.

Abbreviation: nAA-CPS, cervical pedicular screw insertion via the nonanatomic axis; PW, pedicle width.
Consistency of Screw Position Between Preoperative Plans and Final Position
Both nPTA and nPAL were assessed and compared using the pre- and postoperative CT scans (Table 3). There was no significant difference between pre- and postoperative nPTA as demonstrated by the CT results (P < .05), indicating that the trajectory was in accordance with the plan; however, the nPAL on the preoperative CT scan was significantly longer than that observed postoperatively (P > .05).
Comparison Between Pre- and Postoperative nPTA and nPAL.
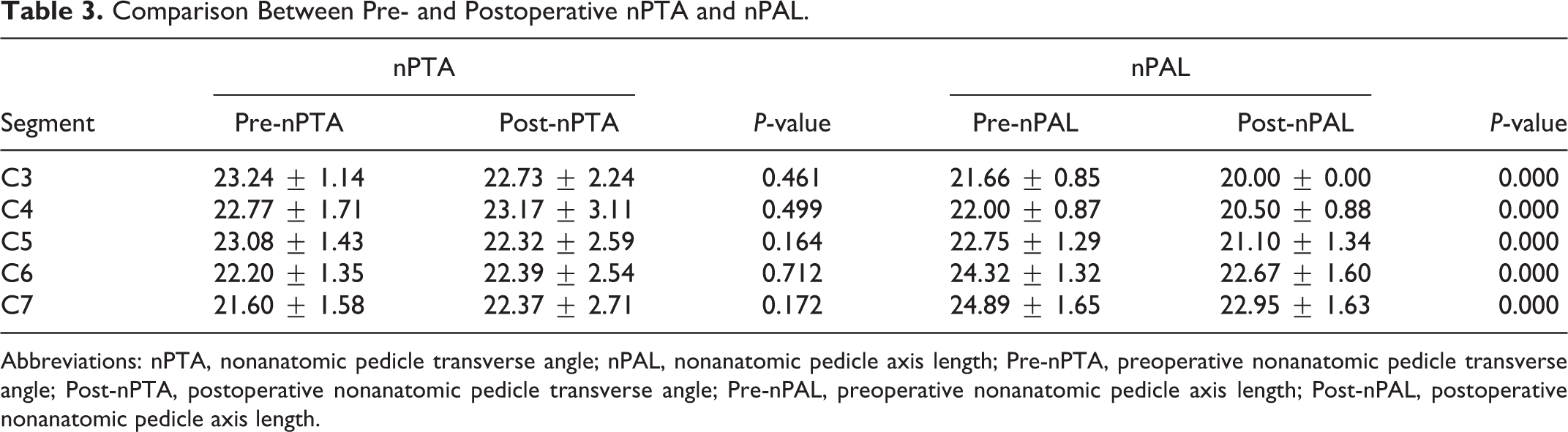
Abbreviations: nPTA, nonanatomic pedicle transverse angle; nPAL, nonanatomic pedicle axis length; Pre-nPTA, preoperative nonanatomic pedicle transverse angle; Post-nPTA, postoperative nonanatomic pedicle transverse angle; Pre-nPAL, preoperative nonanatomic pedicle axis length; Post-nPAL, postoperative nonanatomic pedicle axis length.
Discussion
To our knowledge, this is the first clinical report on nAA-CPS. Our study proved that the aim of nAA-CPS, to decrease the convergence angle of the screw and thereby lessen interference from muscles, could be achieved. Moreover, the standardized manipulation protocol made the technique safe and highly repeatable, an important aspect for the widespread use of freehand technique. The overall accuracy of the 112 nAA-CPSs was comparable with that of traditional CPS insertion.13-17 By medially shifting the EP, the opportunity to penetrate the inner and outer walls of the pedicle during nAA-CPS was almost equivalent (Table 2); Conversely, traditional CPS was more prone to penetrate the outer wall and interfere with the vertebral artery foramen. Pre- and postoperative nPTAs were highly consistent, indicating that the trajectory was fairly standardized when referring to intraoperative neighboring anatomical landmarks.
Computer-assisted navigation improves the accuracy of CPS6-7; however, this inevitably increases the complexity and duration of the procedure. Manual screw placement is therefore the most frequently used technique. Many studies have delineated related manual techniques; however, we found that all focused on inserting screws via the anatomical axis and therefore required a large convergence angle in the transverse plane.11,13-15,18-21 Abumi et al 22 suggested a screw insertion angle of 30-40° in the transverse plane, and recommended creating a funnel-shaped hole to yield a wider range of safe medial angles. Onibokun et al 23 measured 610 C3–C7 vertebrae in 122 patients; the convergence angle of the pedicular anatomical axis ranged from 37.8°-45.3°. In our experience, a large CPS convergence imposes difficulty during screw canal preparation, as the convergence of instruments is frequently interfered with by abundant posterior cervical muscles. Hojo et al 16 evaluated 1065 CPSs and found an overall malposition rate of 14.8% (158/1065), of which 79.7% (126/158) were laterally placed; the present study showed an equal distribution of lateral and medial malposition using nAA-CPS. In our previous radiological study, a decreased convergence angle was achieved by designing the EP and nAA. Moreover, as the convergence of nAA-CPS was small, cervical corpectomy and anterior instrumentation were not bothered by the tips of the pedicle screws.
It is not easy to accurately identify EP on a relatively broad posterior surface of the lateral mass. Lee et al 20 proposed that the optimal EPs of cervical pedicle screws were located 2 mm directly medial to the lateral notch at C3-6, and 1.6 mm lateral and 2.5 mm superior to the center of lateral mass at C7. By comparison, Burcev et al 21 suggested that the coordinates of an optimal EP were located 2 mm from the lateral edge and 2 mm from the upper edge of the lateral mass posterior surface at C3-7. Still, due to the diverse individual differences regarding sex, height, and lateral mass structure, choosing EPs based on fixed values from a frame of reference is surgically challenging and may not be equally applicable to all individuals; therefore, the ideal position of the EP should be relatively constant. EP identification in the present study was derived from our previous work, and was found to be relatively constant and easily identified in clinical practice, providing a solid basis for nAA-CPS.
The trajectory varied according to the shift of EP. Many reports have suggested direct identification of the entry of the pedicle. Abumi et al 22 exposed the entry of the pedicle by removing part of the lateral mass with a burr. Additionally, Lee et al 13 reported a “key slot technique”, while Karaikovic et al 14 suggested a “funnel technique,” which decreased the penetration rates to 9.7% and 7.1%, respectively. These techniques are required to destroy part of the posterior surface of the lateral mass, which may decrease the purchase of the screw tail. In the case of manual failure of the CPS technique, LMS insertion could be disrupted due to posterior cortical bone loss. In our study, we avoided any attempt to directly expose the entry of the pedicle directly; we found that the line connecting the EP and conjunction of the lamina and spinal process was almost perpendicular to the nAA of the pedicle in the transverse plane, while the line of the posterior surface of the lateral mass and inferior one was almost perpendicular to the sagittal axis (Figure 2B, C). In clinical practice, we identified the trajectory using two perpendicular angles as neighboring landmarks, establishing a correct relationship of EP and nAA without destroying the extra cortical surface of the lateral mass (Figure 3A-E). Even if canal preparation for nAA-CPS fails, the major structures of the lateral mass remains intact, meaning that alternation from the CPS to LMS is feasible. The results showed that the protocol was fairly useful for determining the orientation of nAA-CPS; additionally, the rate of correct screw positions was comparable with that of the traditional CPS insertion, suggesting that nAA-CPS is feasible in terms of technical safety and standardization.
This technique has several limitations. First, as screw insertion is via the nAA, a larger pedicle diameter was needed to accommodate the screw. Second, the spinous process and lateral masses are important landmarks for the identification of the EP and trajectory in nAA-CPS; deformity, severe damage to the lateral mass, spinous process, or abnormal pedicle shape would significantly decrease the safety of this technique. Last, the sample size was relatively small; the learning curve of the technique led to less proficiency in the early stage than in the later stage, which may have contributed to a certain deviation from the final statistical results. However, this technique cannot completely avoid the risk of screw malposition.
Conclusions
Compared with traditional CPS insertion, this is a novel technique that introduces the concept of the nAA into clinical practice and effectively reduces soft tissue obstruction during manipulation. Using a standard manual protocol for identifying EP and trajectory, nAA-CPS was proven to be as safe and accurate as the traditional CPS; thus, providing an alternative in clinical practice.
Footnotes
Authors’ Note
Yingbo Wang and Bo Hu contributed equally to this work and should be considered as co–first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Army Medical University Project of Medical Elite Training (2018XLC2024) and the Cooperative projects of Chongqing Scientific and Technological Commission and Health Commission(2020MSXM006).