
Abstract
Study Design:
Systematic review and meta-analysis of randomized controlled trials (RCTs).
Objective:
This systematic review and meta-analysis was performed with the aim of exploring the differences in pedicle screw positioning accuracy, surgical time, length of hospital stay, postoperative back and leg Visual Analog Scale, revision surgeries, and intraoperative radiation time and exposure between robot-assisted technology and conventional freehand technique based on RCTs.
Methods:
Several databases, including the Cochrane library, PubMed, and EMBASE were systematically searched to identify potentially eligible articles. Meta-analysis was done using STATA 13 software. The odds ratios and 95% CIs were calculated for the studied categories.
Results:
Seven RCTs involving 290 patients (1298 pedicle screws) in the robot-assisted group and 288 patients (1348 pedicle screws) in the conventional freehand group were analyzed. The results revealed that grade (A) and grade (A+B) screw accuracies were significantly superior in the robot-assisted group (P = .008 and P = .009, respectively). Overall surgical duration and number of revision surgeries were significantly higher in the robot-assisted group (P = .014 and P < .0001, respectively). Intraoperative radiation time and dosage were significantly lower in the robot-assisted group (P < .0001 and P = .036, respectively).
Conclusion:
It was demonstrated that robot-assisted technology is superior to the conventional freehand technique in terms of grade (A) and grade (A+B) screw accuracies and in the reduction of intraoperative radiation time and dosage. On the other hand, the freehand technique showed superior results in terms of overall surgical duration and revision surgery rates.
Introduction
Pedicle screw fixation is a common spinal surgical procedure that has been widely used to stabilize the spine because it provides 3-column control. 1 The accurate insertion of a pedicle screw is challenging because of the morphological variations of individual pedicles. 2 -5 Therefore, a variety of techniques were introduced to assist in screw insertion and to reduce the prevalence of screw malposition.
Conventional freehand pedicle screw insertion uses either anatomical landmarks or C-arm fluoroscopy during the procedure. However, screw malposition cannot be neglected with this technique. It was reported that the percentage of misplaced screws using this technique ranged from 8.3% to 50.3%. 6
Screw misplacement can result in some problems such as dural tear and neural, vascular, or visceral injuries. 7,8 To address that issue, an image guidance system was explored and applied to spinal surgery. 9 -11 Theoretically, this technique can prevent complications by providing more precise anatomical guidance. Verma et al, 12 in their systematic review and meta-analysis of 23 studies that included 5992 pedicle screws, concluded the presence of a significant advantage in terms of accuracy of navigation over conventional pedicle screw insertion. However, navigation does not show statistically significant benefit in reducing neurological complications, and there was insufficient data in the literature to infer a conclusion in terms of fusion rate, pain relief, and health outcome scores.
Robot-guided pedicle screw insertion was developed as a refinement of image guidance or navigated spinal surgeries, with the aim of increasing the accuracy of screw positioning and the reduction of radiation exposure. 13 -15
Retrospective studies have reported a nearly 99% accuracy of screw positioning under robotic guidance. 16,17 However, one study reported the opposite, in which pedicle screw insertion under robotic guidance yielded less accurate positioning, with no difference in surgical time, intraoperative blood loss, duration of hospital stay, and intraoperative radiation exposure, compared with the conventional freehand technique. 18
This systematic review and meta-analysis was performed with the aim of exploring the differences in pedicle screw positioning accuracy, surgical time, length of hospital stay, postoperative back and leg VAS, revision surgeries, and intraoperative radiation time and exposure between robot-assisted technology and the conventional freehand technique, based on RCTs.
Methods
Search Strategy
Several databases, including the Cochrane library, PubMed, and EMBASE were systematically searched to identify potentially eligible articles. All the above databases were searched up to June 2019. The search strategy was based on the combination of the following keywords: robot, robotic, robotics, pedicle screw, bone screw, accuracy, instrumentation, and freehand technique. The reference lists of selected literature were also reviewed. Institutional review board approval was not necessary.
Inclusion and Exclusion Criteria
Inclusion criteria were established before the search, and the following criteria were used: (1) Type of study: randomized controlled trials (RCTs) of robot-assisted pedicle screw placement and conventional freehand technique. (2) Types of participants: patients presenting with spinal pathologies that mandate pedicle screw insertion; they were divided into the experimental group, who received robot-assisted pedicle screw insertion, and the control group, who had pedicle screw insertion using the conventional freehand technique. (3) Intervention: spinal pathologies that mandate pedicle screw insertion with no particular indication. (4) Outcome measurement: the primary outcome was assessing the accuracy of pedicle screw placement by postoperative computed tomography (CT) scans. Secondary outcomes included surgical duration, intraoperative radiation exposure, length of hospital stay, postoperative back and leg VAS, and revision surgery.
Exclusion criteria were as follows: (1) cohort studies, review articles, case reports, or expert opinion reports; (2) cadaveric and animal studies; (3) pedicle screw insertion without robotic assistance; (4) non-English language studies; and (5) repetitive studies. A flowchart of literature selection was generated (Figure 1).
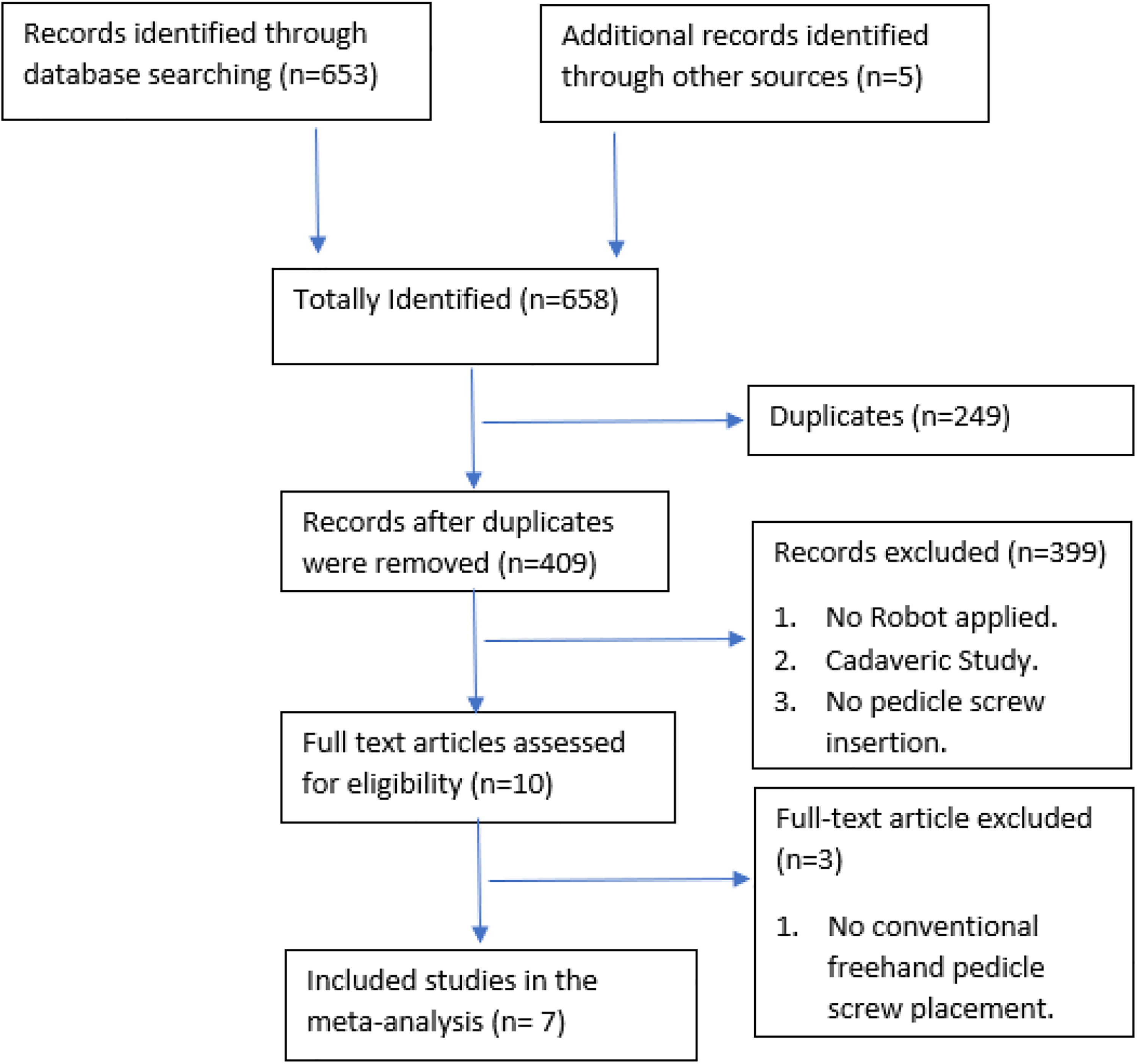
Flowchart of literature selection.
Surgical Technique
In the robot-assisted technique, generally and irrespective of the robot type used, the patient is placed prone on a radiolucent spinal table. A midline incision was done to place the robot platform. Once the platform was firmly attached, an array was attached to it. Three-dimensional fluoroscopy images were obtained. Following the registration procedure, a robotic manipulator was mounted on the bone-fixed platform and aligned itself with the preplanned trajectory according to the surgeon’s commands. The robot’s drilling guide was used to insert the pedicle screws.
In the conventional freehand technique, the patient is placed prone on a radiolucent spinal table. A midline incision was done to fully expose the facet joints and transverse processes, which are used as anatomical landmarks for pedicle screw insertion. A fluoroscopic image is obtained at the beginning of the procedure for level check and at the end to ensure satisfactory alignment of the metal works. Fluoroscopy has been used occasionally during the procedure to assist in screw placement if needed.
Data Extraction
All potentially eligible studies were obtained as full articles. The 2 reviewers independently assessed the studies for the predetermined inclusion and exclusion criteria. Controversial studies were discussed by the 2 reviewers to reach consensus. Information extracted on each eligible study included the first author, year of publication, type of study, patient characteristics, number of patients and number of screws implanted in different groups, robot type, method of pedicle screw insertion, assessment of screw insertion accuracy, and clinical outcome assessments (Table 1).
Main Characteristics of Included Studies.
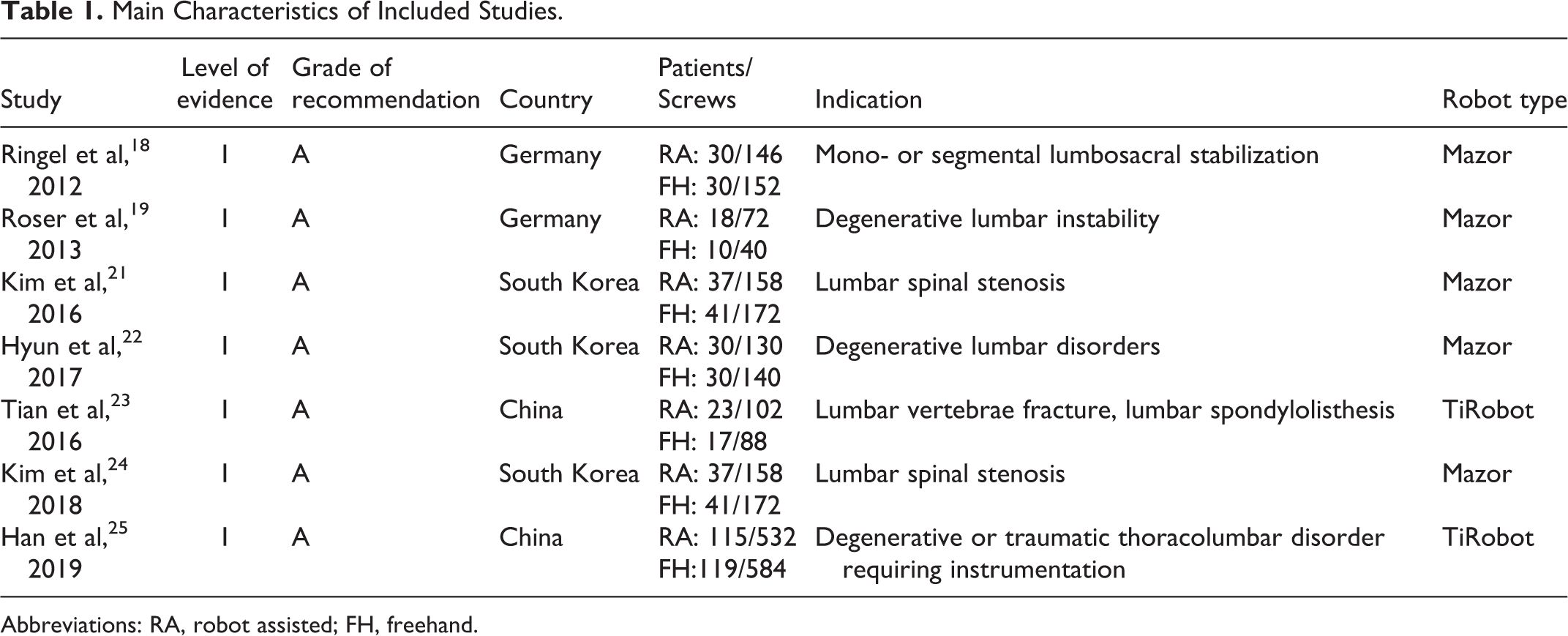
Abbreviations: RA, robot assisted; FH, freehand.
Quality Assessment
The Cochrane tool was used for assessing the risk of bias for the included RCTs. The risk of bias in the selected RCTs was based on 7 parameters (Figure 2). All studies claimed randomization. Allocation concealment was well conducted in all studies except two. 18,19 Blinding of participants and personnel were considered unclear in all studies. Two studies failed to report the blinding of outcome assessment and, thus, were judged to have unclear risk of bias. Incomplete outcome data was judged to be high risk in one study because the results reported were preliminary without statistical evaluation to describe trends. 19 The 2 reviewers assessed the risk of bias among studies independently. Disagreements regarding the risk of bias assessment were settled by discussion and consensus between reviewers.
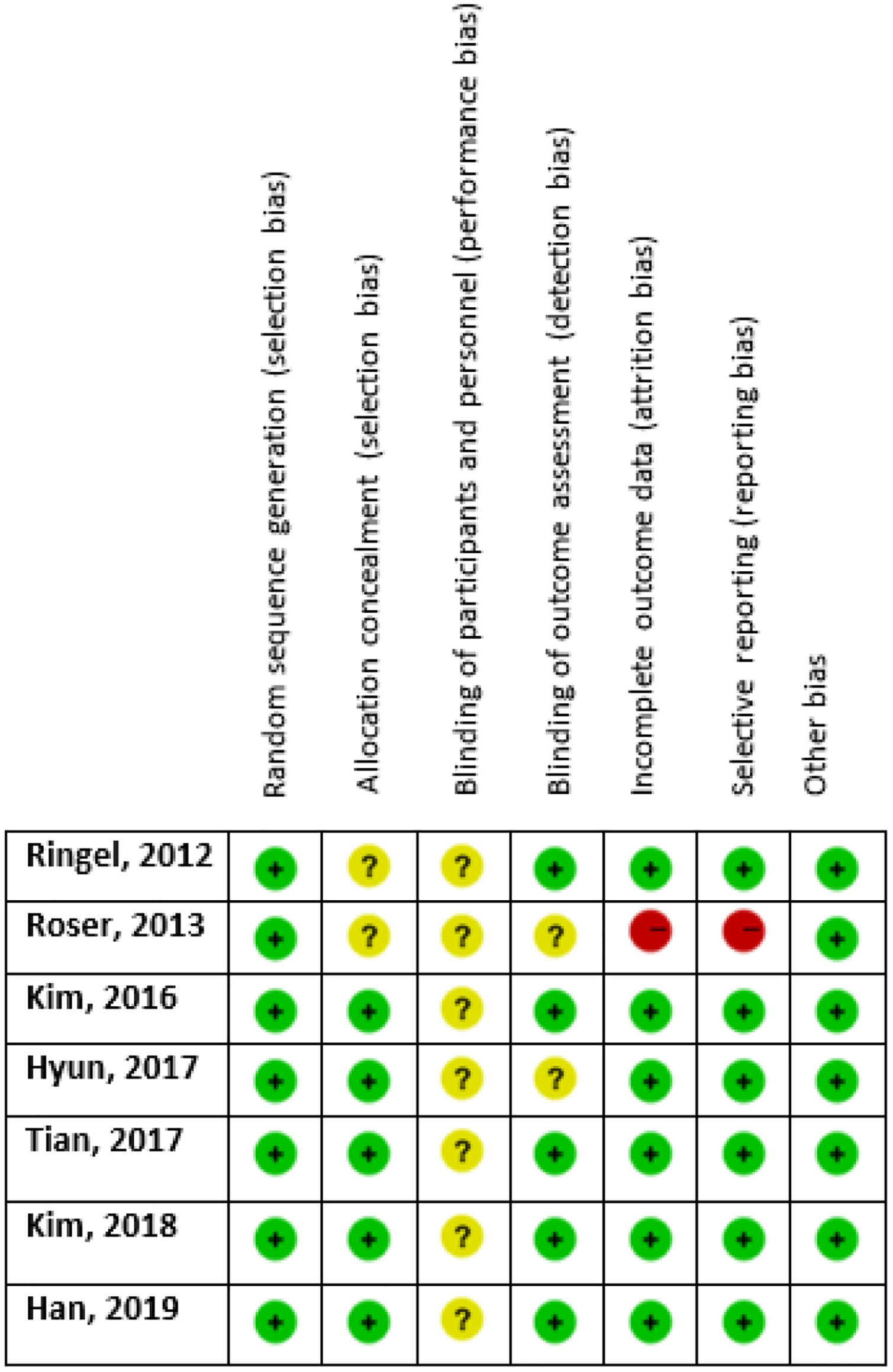
Risk of bias summary: review authors’ judgments about each risk of bias item for each included study.
Statistical Analysis
STATA software version 13 was used for meta-analysis. Odds ratios and 95% CIs were calculated for accuracy of pedicle screw insertion as well as clinical outcome assessments. The level of significance was set at P <.05. Heterogeneity was evaluated using I2 statistics and the χ2 test. If heterogeneity was significant (I2 > 50% and P < .10), the random-effects model was used. Alternately, the fixed-effects model was used. A forest plot was generated to compare the primary and secondary outcomes in the experimental and control groups.
Outcome Measures
Outcome measures were categorized into primary and secondary outcomes. Primary outcome involved interpedicular screw accuracy according to the Gertzbein-Robbins classification. Secondary outcomes included surgical duration, intraoperative radiation time and exposure, length of hospital stay, postoperative back and leg VAS, and revision surgery.
Results
Study Inclusion and Characteristics
This systematic review and meta-analysis of RCTs was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 20 Figure 1 shows the summary of the identification and selection process of the study. After reviewing the titles, abstracts, and full texts, we identified 7 published studies that met all our inclusion criteria. 18,19,21 -25 The characteristics of the included studies are summarized in Table 1.
Meta-analysis Results
Primary Outcomes
Screw position according to grade (A) criteria
Six RCTs studied the accuracy rate of screw insertion using the Gertzbein-Robbins grading system. 18,19,21 -23,25 More than 90% of screws inserted using robot-assisted technology were in grade (A) compared with 86.4% of screws in the freehand technique. The findings of these RCTs were pooled using meta-analysis (Figure 3). The results showed statistically significant differences between the 2 groups in favor of robot-assisted technology (P = .008).
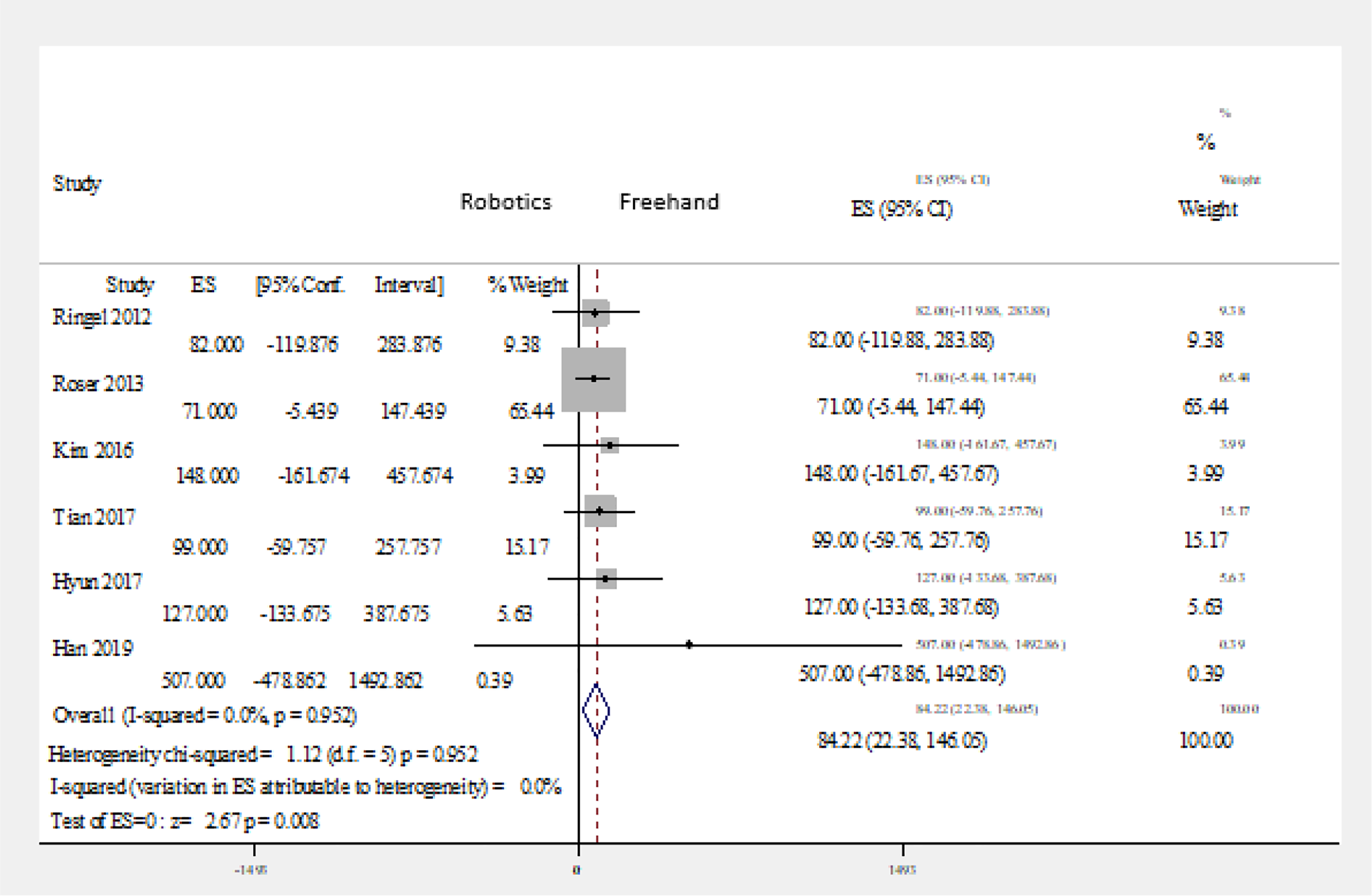
Forest plot of robot-assisted versus conventional freehand technique: screw position according to grade (A) criteria. Abbreviation: ES, effect size.
Screw position according to grade (A+B) criteria
Six RCTs studied the accuracy rate of screw insertion using the Gertzbein-Robbins grading system. 18,19,21 -23,25 A total of 97% of screws inserted using the robotic-assisted technique were in A or B grade compared with 95.4% using the freehand technique. The findings of these RCTs were pooled using meta-analysis (Figure 4). The results showed statistically significant differences between the 2groups in favor of robot-assisted technology (P = .009).
Forest plot of robot-assisted versus freehand technique: screw position according to grade (A+B) criteria. Abbreviation: ES, effect size.
Screw position according to grade (C+D+E) criteria
Six RCTs studied the accuracy rate of screw insertion using the Gertzbein-Robbins grading system. 18,19,21 -23,25 Only 31 screws out of 1140 screws (2.7%) inserted using the robotic-assisted technique were in grades C, D, or E compared with 4.5% (n = 53/1176) using the freehand technique. The findings of these RCTs were pooled using meta-analysis(Figure 5). The results showed nonsignificant differences between the 2 groups (P = .430).
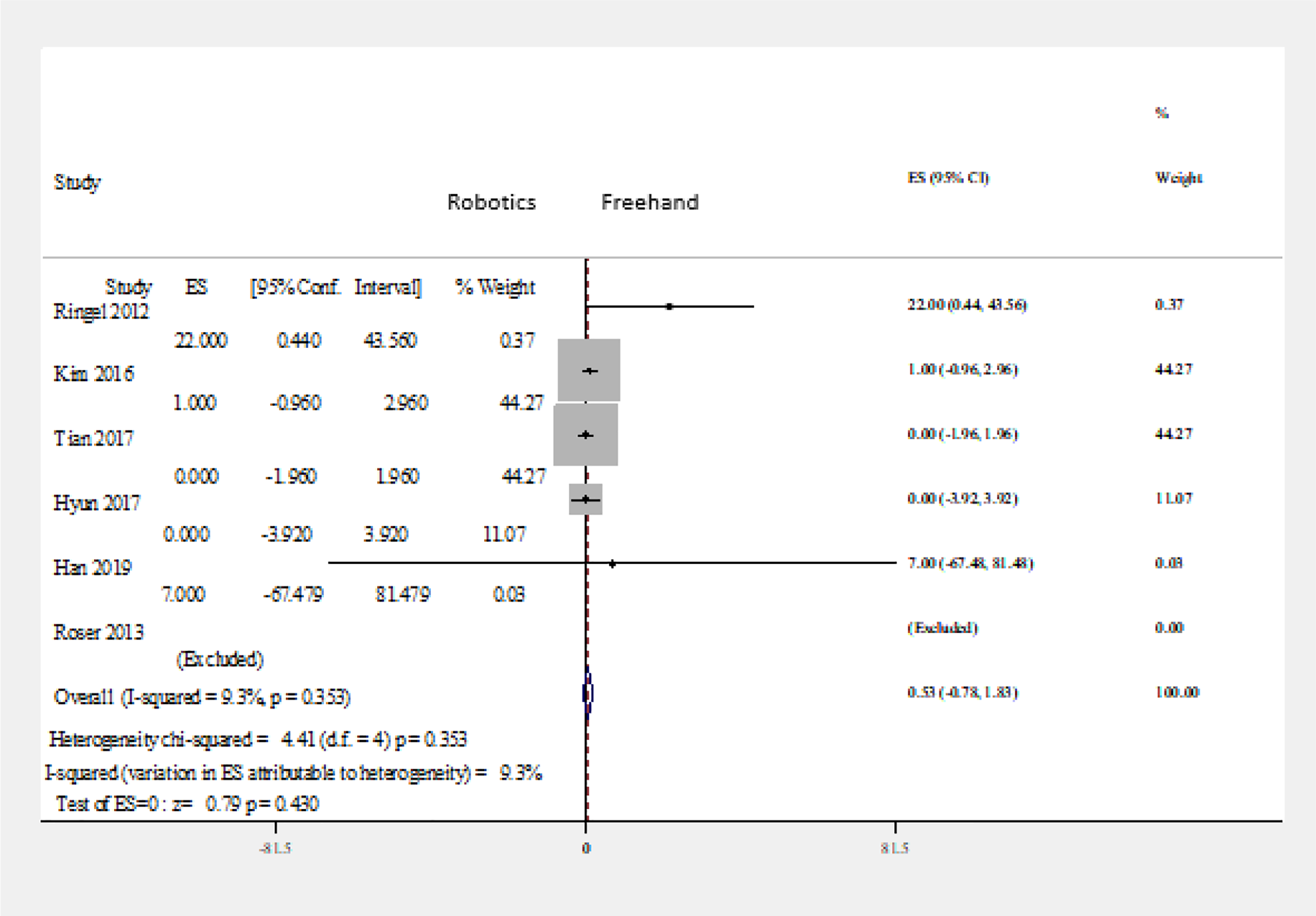
Forest plot of robot-assisted versus freehand technique: screw position according to grade (C+D+E) criteria. Abbreviation: ES, effect size.
Secondary Outcomes
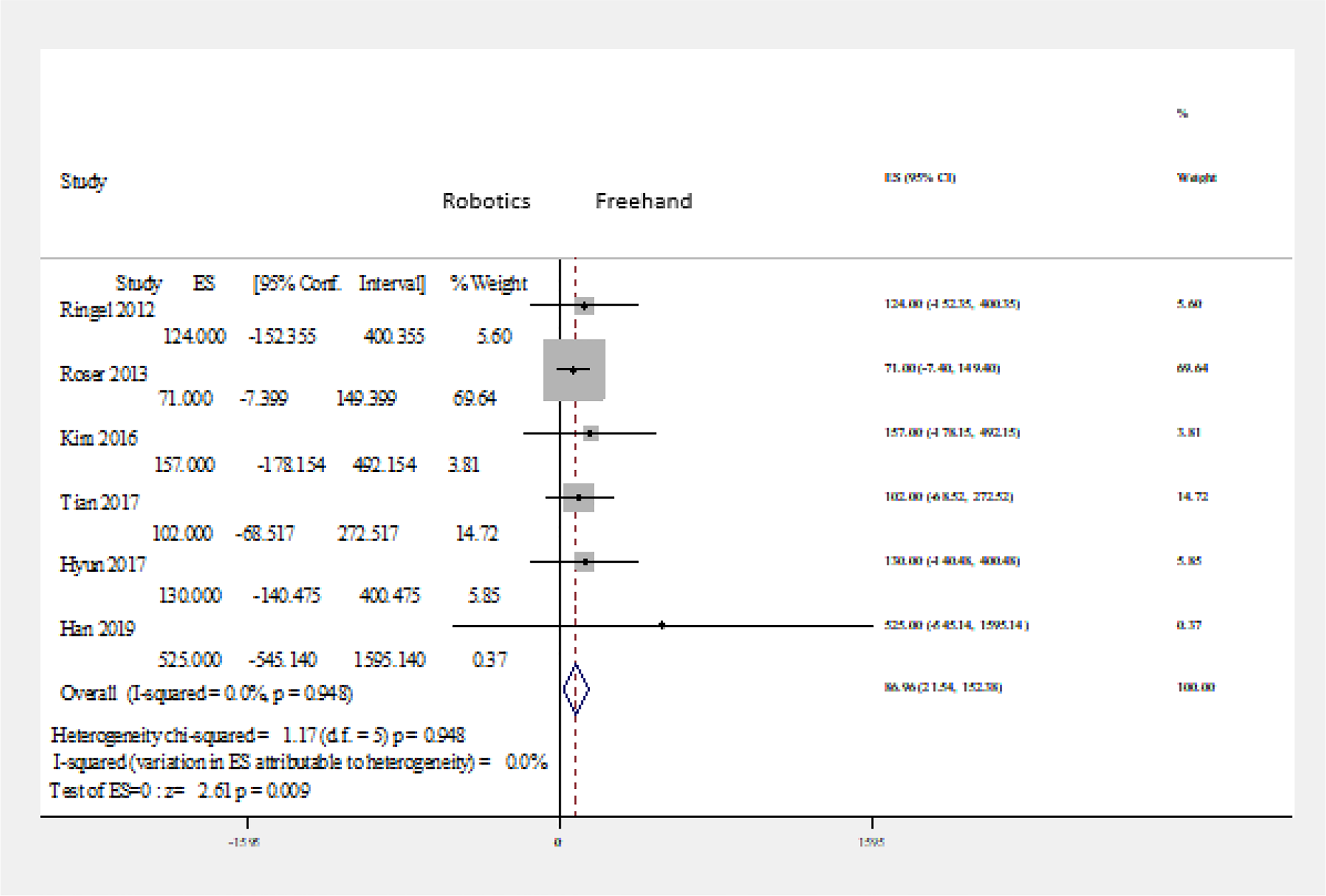
Surgical duration
Five RCTs mentioned the overall surgical time from skin to skin. 18,21 -23,25 All the studies were in favor of the freehand technique, except 1 study that showed equal results. 22 The findings of these RCTs were pooled using meta-analysis (Figure 6). The overall surgical duration differed significantly between robot-assisted technology and conventional freehand pedicle screw implantation in favor of the freehand technique (P = .014).
Forest plot of robot-assisted versus freehand technique: surgical duration. Abbreviation: ES, effect size.
Intraoperative radiation: time and exposure
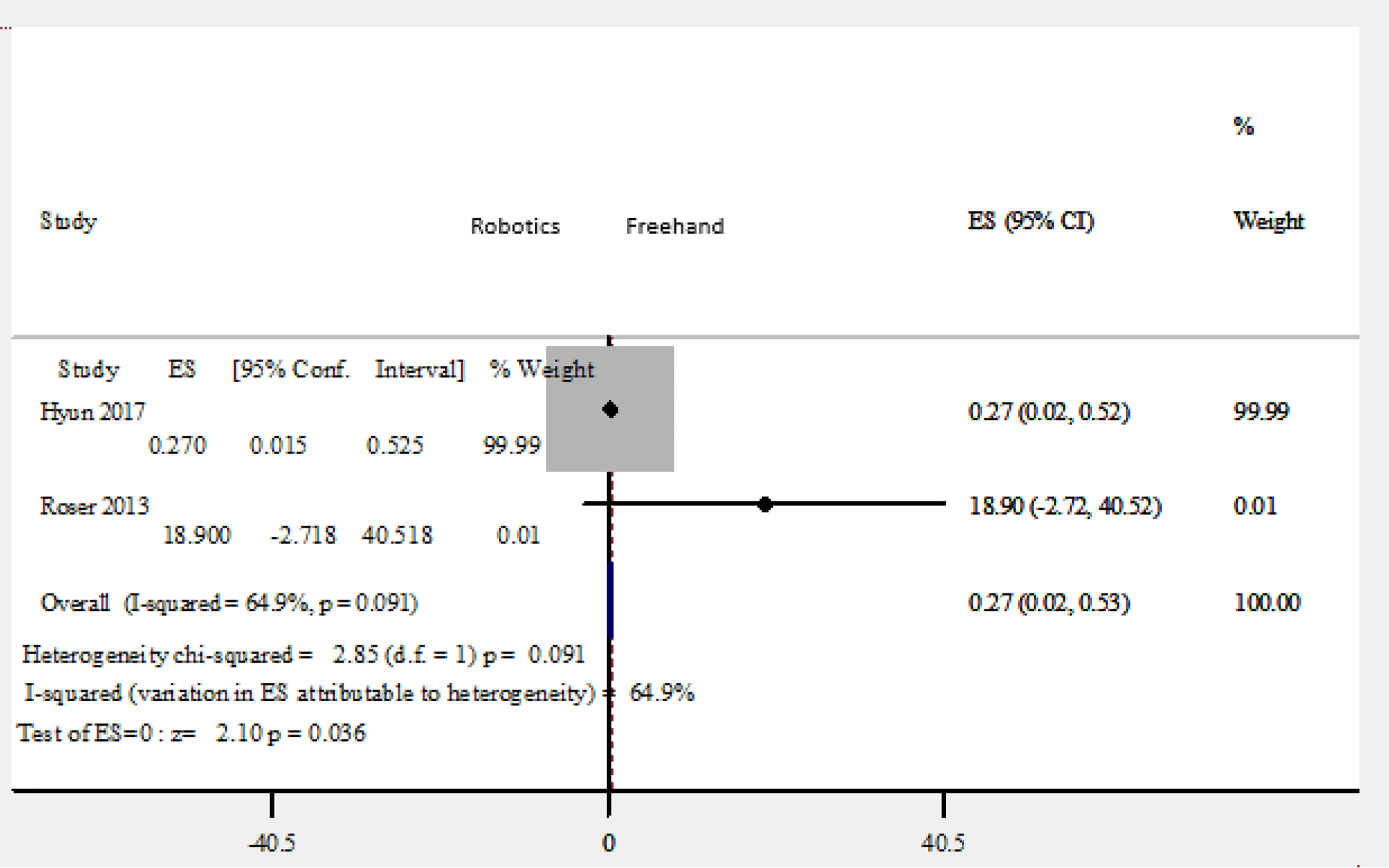
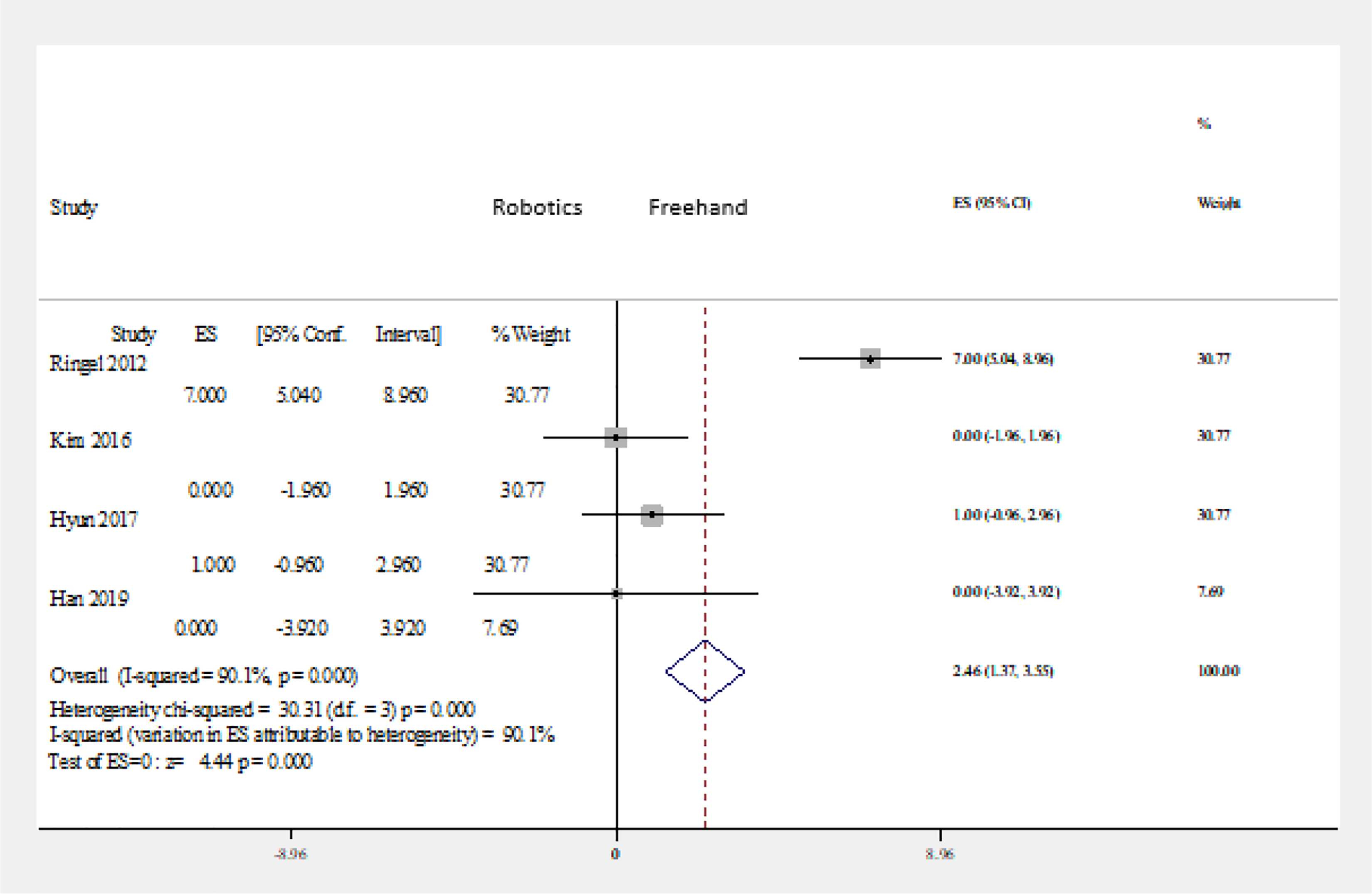
The intraoperative radiation exposure was measured by both direct operational outputs recorded by the C-arm (in milli-Sieverts [mSv] and seconds of fluoroscopy). Two RCTs mentioned the intra-operative radiation time and radiation exposure. 19,22 The findings of these RCTs were pooled using meta-analysis (Figures 7 and 8). The intraoperative radiation time and exposure showed statistically significant difference between the 2 groups in favor of robot-assisted technology (P < .0001 and P = .036, respectively).
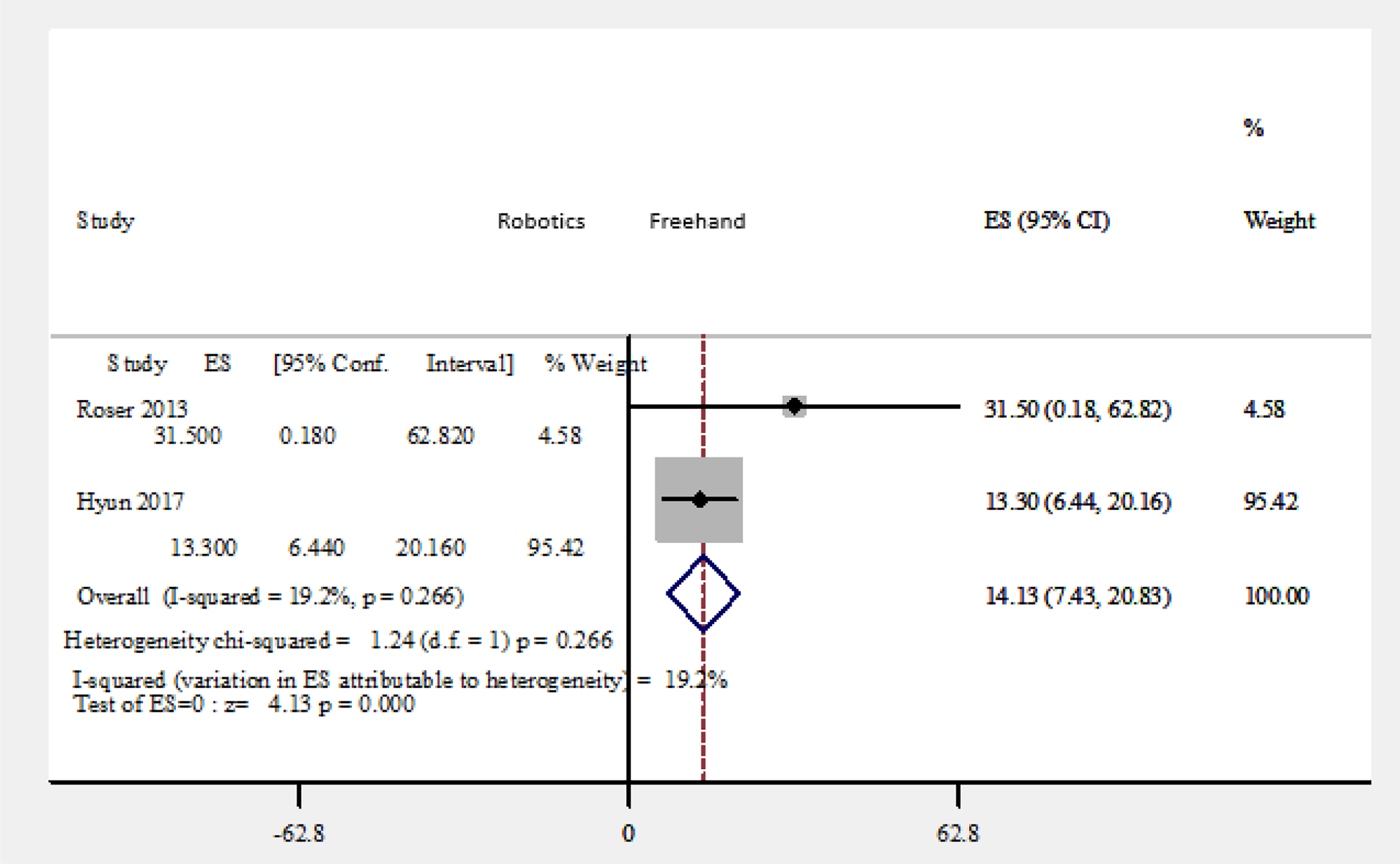
Forest plot of robot-assisted versus freehand technique: intraoperative radiation time (seconds of fluoroscopy). Abbreviation: ES, effect size.
Forest plot of robot-assisted versus freehand technique: intraoperative radiation exposure (mSv). Abbreviation: ES, effect size.
Postoperative stay in hospital (days)
Three RCTs mentioned the postoperative hospital stay. 18,22,25 Two studies were in favor of robotics. 22,25 The findings of these RCTs were pooled using meta-analysis (Figure 9). The duration of postoperative hospital stay showed a nonsignificant difference between the 2 groups (P = .106).
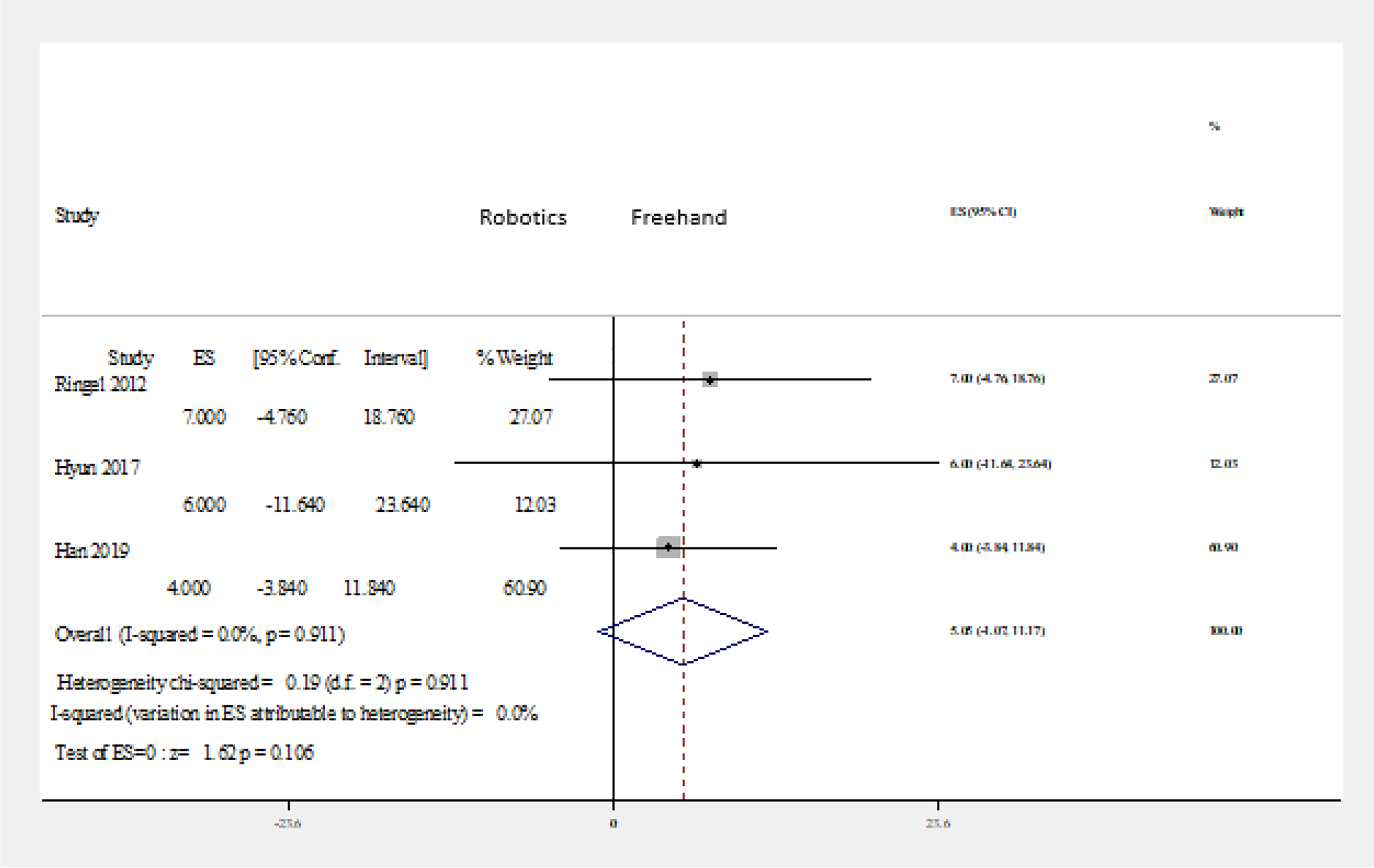
Forest plot of robot-assisted versus freehand technique: postoperative hospital stay (days). Abbreviation: ES, effect size.
Postoperative VAS back
Two RCTs mentioned the postoperative VAS back. 22,24 In both studies, the results were in favor of the robot-assisted group. The findings of these RCTs were pooled using meta-analysis (Figure 10). The level of VAS back showed a nonsignificant difference between the 2 groups (P = .254).
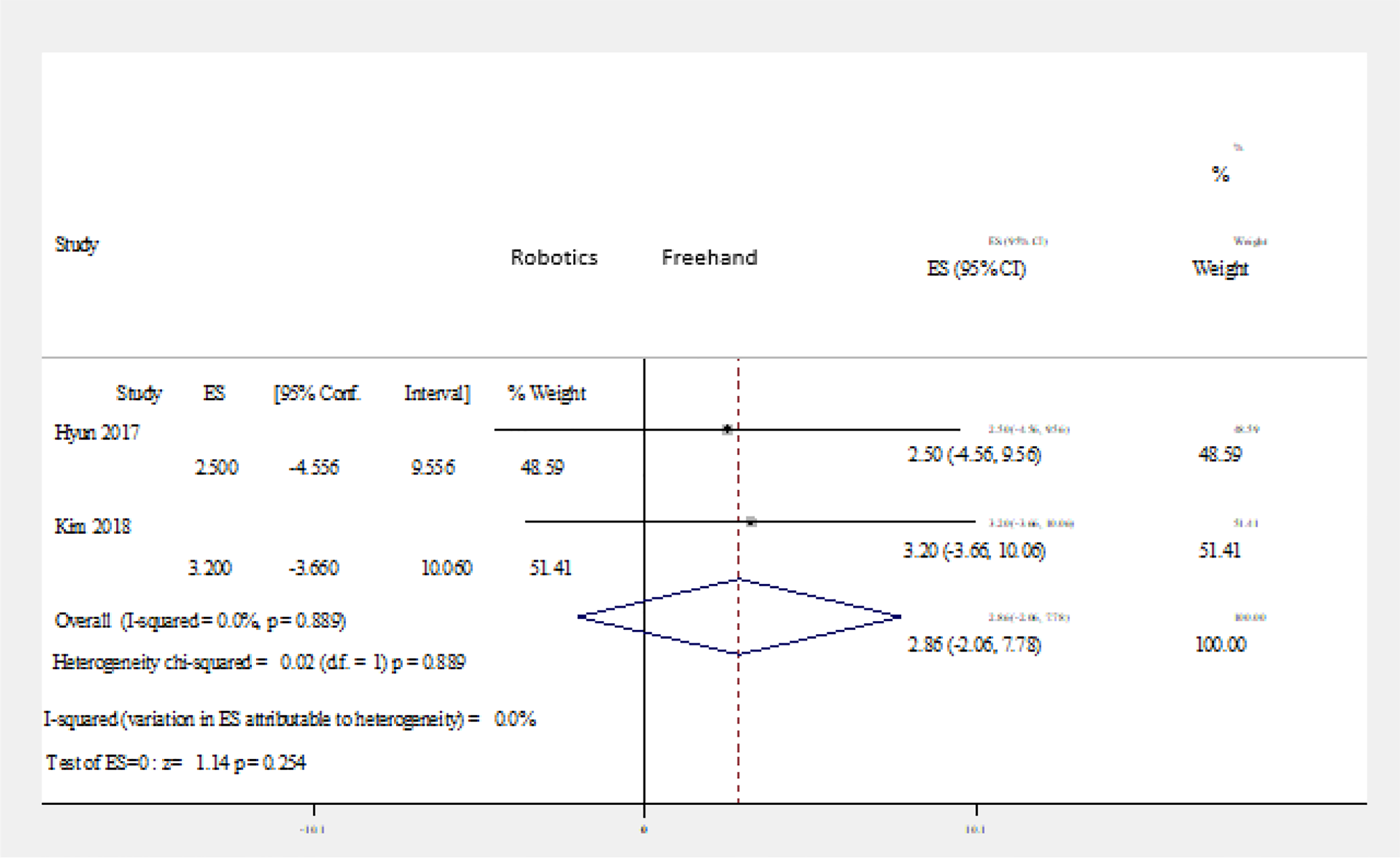
Forest plot of robot-assisted versus freehand technique: postoperative Visual Analog Scale back. Abbreviation: ES, effect size.
Postoperative VAS leg
Two RCTs mentioned the postoperative VAS leg. 22,24 In both studies, the results were in favor of the robot-assisted group. The findings of these RCTs were pooled using meta-analysis (Figure 11). The level of VAS leg showed a nonsignificant difference between the 2 groups (P = .249).
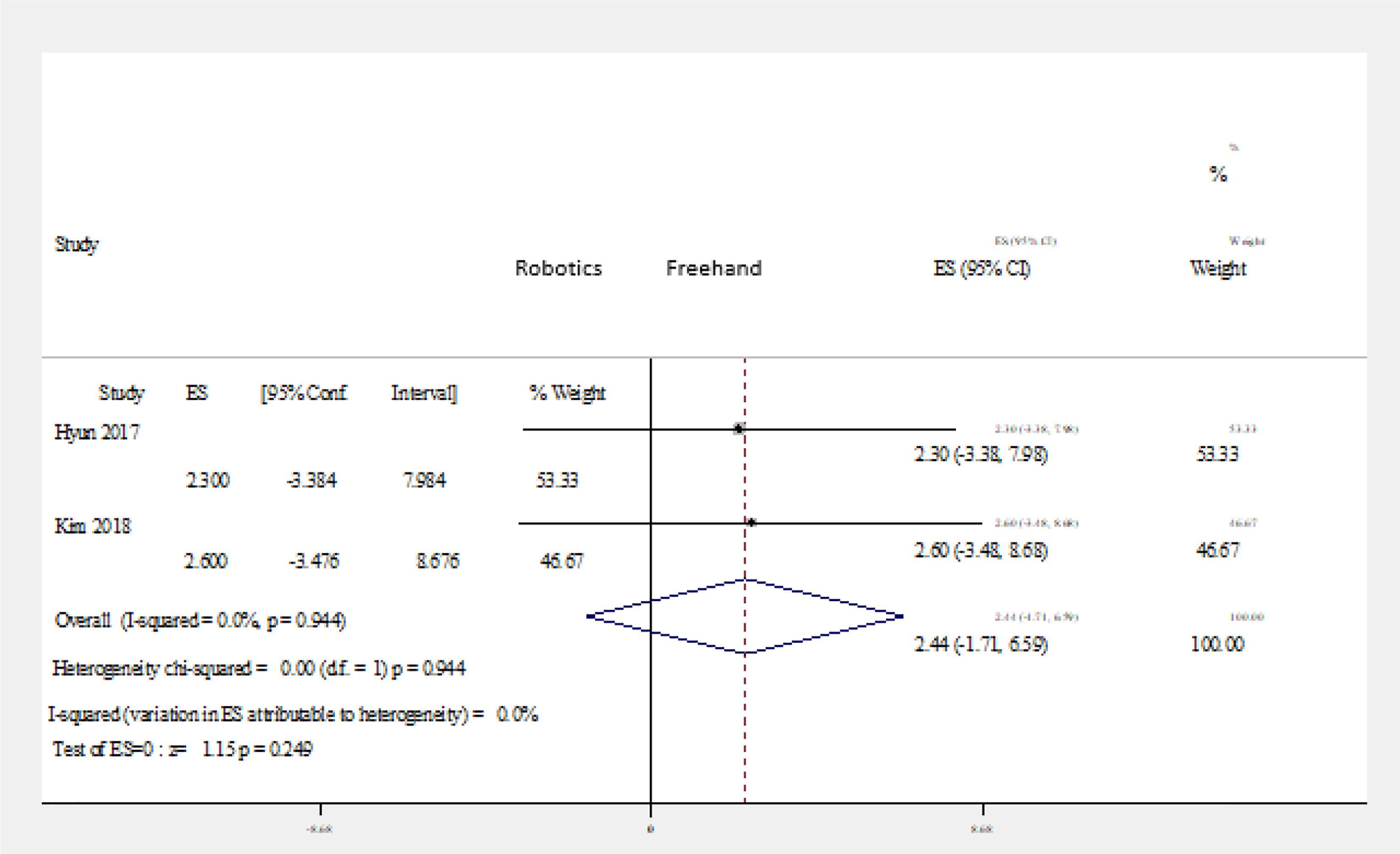
Forest plot of robot-assisted versus freehand technique: postoperative Visual Analog Scale leg. Abbreviation: ES, effect size.
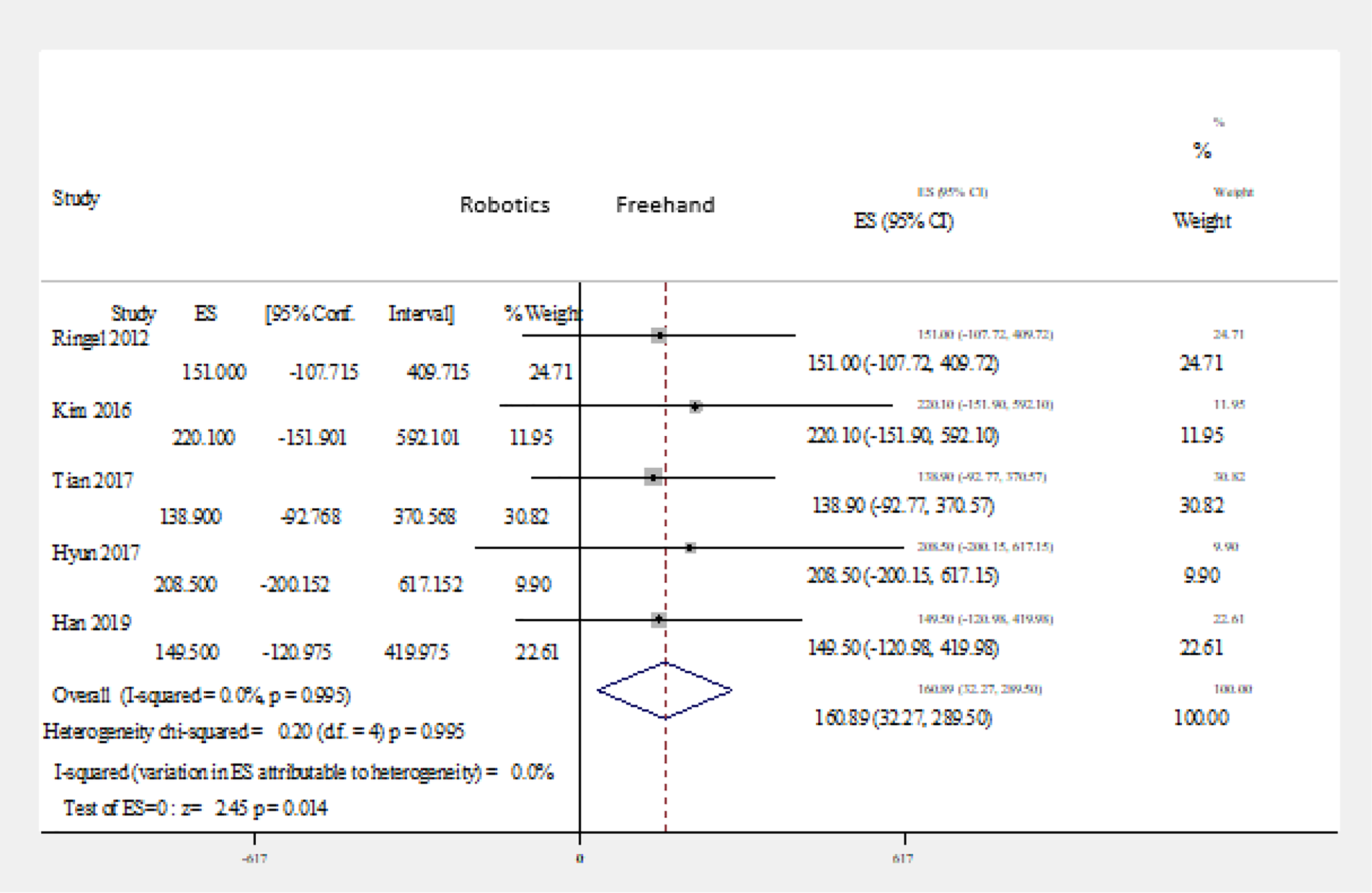
Revision surgeries(immediate/delayed)
Four RCTs studied the rate of revision surgeries in both freehand and robotic-assisted techniques. 18,21,22,25 Three studies showed either equal rate of revision surgeries in both studied groups or better results in robotic-assisted technology compared with the freehand technique. 22,21,25 The remaining study showed higher revision rates in the robotic-assisted surgery compared with freehand surgery. 18 The findings of these RCTs were pooled using meta-analysis (Figure 12). The results showed statistically significant differences between the 2 groups in favor of the freehand technique (P < .0001).
Forest plot of robot-assisted versus freehand technique: revision surgery. Abbreviation: ES, effect size.
Discussion
Screw fixation is a fundamental issue in spinal surgery that can be technically challenging because of the wide anatomical variations of the vertebrae and the surrounding vital structures, such as spinal cord, nerve roots, and blood vessels. In the conventional freehand technique, pedicle screw placement depends on the selection of the correct entry point at the posterior cortex of the vertebra being instrumented. This is accomplished based on anatomical landmarks and intraoperative fluoroscopy.
The need for improving accuracy of pedicle screw insertion has led to the development of various new techniques, such as navigation-guided and robot-assisted techniques. There have been conflicting results regarding the safety and accuracy of robot-assisted pedicle screw fixation. 16 -18 Therefore, this meta-analysis and systematic review of RCTs was intended to assess these points in comparison with the conventional freehand technique.
The accuracy of pedicle screw placement is of major concern among spine surgeons. The definition of accuracy of pedicle screw insertion was consistent across all the selected studies—namely, the Gertzbein-Robbins classification. 26 Grade A, the screw is completely within the pedicle; grade B, the screw breaches the pedicle’s cortex by <2 mm; grade C, pedicle cortical breach <4 mm; grade D, pedicle cortical breach <6 mm; and grade E, pedicle cortical breach >6 mm. The accuracy of pedicle screw placement was evaluated using postoperative axial, sagittal, and coronal views on CT scans.
Ringel et al 18 found that screw accuracy is less in robot-assisted technology compared with the freehand technique in grade A alone and grades A+B combined. Roser et al 19 found that robot-assisted technology was more accurate in achieving grade A screws; however, the results were in favor of the freehand technique when both A+B groups were combined.
The results of this meta-analysis showed a statistically significant difference in screw accuracy placement grade A and grade (A+B) in favor of robot-assisted technology: P = .008 and P = .009, respectively. On the other hand, the results showed no statistically significant differences between the 2 groups (P = .430), in grades (C+D+E) screw accuracy.
The first parameter to start with in the secondary outcome is the overall surgical time. Hyun et al 22 reported no difference in the overall surgical time between robot-assisted technology and the conventional freehand technique. However, Ringel et al, 18 Kim et al, 21 Tian et al, 23 and Han et al 25 reported a longer surgical time in the robot-assisted group. In our study, the overall surgical duration differed significantly between robot-assisted technology and the conventional freehand pedicle screw implantation (P = .014) in favor of the freehand technique.
The increase in surgical time in robot-assisted technology can be attributed to the fact that robot-assisted pedicle screw insertion is in its early stages of clinical application and requires a learning curve before reaching a proficient state. Moreover, the intraoperative preparation may also contribute to the longer surgical duration.
Ringel et al 18 reported longer hospital stays in the robot-assisted group, whereas Hyun et al 22 and Han et al 25 showed the opposite. Regardless of the variation in hospital stay between the 2 groups, the differences were not statistically significant (P = .106).
One valuable advantage of robot-assisted technology is to lessen reliance on intraoperative fluoroscopy. The intraoperative radiation exposure was measured by both direct operational outputs recorded by the C-arm (in milli-Sieverts [mSv] and seconds of fluoroscopy). Roser et al 19 and Hyun et al 22 reported less radiation time and exposure in the robot-assisted technique. Our study showed that intraoperative radiation time and exposure are statistically significantly different between the 2 groups in favor of the robot-assisted technology. The present meta-analysis also demonstrated that the 2 surgical techniques showed no statistically significant differences in postoperative back or leg VAS.
The rate of screw revision was analyzed. Hyun et al 22 showed equal revisions rates between the robot-assisted screw placement technology and the freehand technique. Kim et al 21 and Han et al 25 reported no revisions at all. Interestingly, Ringel et al 18 showed that 10 screws in 7 patients required a conversion to freehand technique after the robot-guided drill hole was in the soft tissue lateral to the vertebral body and pedicle without sufficient bone contact. In this study, the results showed statistically significant differences in favor of the freehand technique between the 2 groups (P < .0001).
Several points should be acknowledged in this study. First, we studied robot-assisted technology in screw placement regardless of the robot manufacturer. Second, the method of screw placement (freehand vs robot) was studied without taking into account the surgical approach used (open vs minimally invasive) and their effects on the surgical outcome.
The limitation of this study is that it included pedicle screw insertion regardless of the underlying pathology. Future research specifying the accuracy rate in relation to the pathology (trauma, degenerative, and deformity) is needed.
Conclusion
The robot-assisted technology was associated with equivalent results in terms of length of hospital stay, postoperative back VAS, postoperative leg VAS, and grade (C+D+E) screw insertion accuracy. It was demonstrated that the robot-assisted technique is superior to the conventional freehand technique in terms of grade (A) and grade (A+B) screw accuracy and in the reduction of intraoperative radiation time and exposure. On the other hand, the freehand technique showed superior results in terms of overall surgical duration and revision rates.
Robotics in spine surgery holds a promising future. However, the effectiveness of robotics in spinal instrumentation has been researched less than might be expected. This systematic review and meta-analysis provided an evaluation of the available RCTs on the outcome of pedicle screw insertion using the robot-assisted technique and the conventional freehand technique. To validate the beneficial role of robotics in spine surgery more RCTs with higher sample sizes are encouraged.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.