
Abstract
Study Design:
A prospective study.
Objectives:
We present a largest study until date performed over a period of 10 years assessing the perioperative complications. The primary aim of this study was to review the incidence of perioperative complications of minimally invasive transforaminal lumbar interbody fusion (MI-TLIF) in single-level lumbar degenerative diseases.
Methods:
A prospective study performed over a period of 10 years involving 560 patients who underwent single-level lumbar MI-TLIF. Perioperative clinical and radiological parameters, postoperative complications, and satisfactory outcomes in the form of Wang’s criteria were evaluated. All patients were scrutinized into 5 different categories based on the descriptive classification for perioperative complications suggested by the authors.
Results:
The mean age was 61.8 ± 12.7 years and male to female ratio was 0.8:1. The overall incidence of the perioperative complication was 25.5%. In all, 19.64% patients developed single complication, 4.64% patients were with 2 complications, and 1.25% patients developed 3 complications from the described categories. A total of 16.78% patients developed early (<6 months postsurgery) and 8.75% patients developed late (>6 months postsurgery) complications.
Conclusion:
This study showed 25.5% incidence of perioperative complications in MI-TLIF for degenerative lumbar disease over a period of 10 years with a higher incidence rate during the initial 3 years of practice. The described classification for perioperative complications is helpful to record, to evaluate and to understand the etiology based on its duration of occurrence in the perioperative period. MI-TLIF is an effective procedure with substantial clinical benefits in the form of excellent to good clinical-radiological outcomes.
Keywords
Introduction
Minimally invasive transforaminal lumbar interbody fusion (MI-TLIF) is well established approach for lumbar degenerative disorders with instability. 1,2 It allows access to interbody space at any level of the lumbar spine with minimal retraction of the neural structures. 3,4 The rationale for such a swing in momentum from open surgery to minimally invasive spine surgery (MISS) includes reduced soft tissue damage, lesser blood loss, faster recovery, and reduced perioperative morbidities. 1 -6 The advantages related with MI-TLIF requires further investigations to assess its affection with the perioperative complications so that its efficacy and safety can be established. With increasing life expectancy and advances in technology and instrumentation in the recent years, the number of MI-TLIF surgeries for various lumbar pathologies is on a rise. 5,6 The evaluation of surgical complications is one of the important parameters in spine surgery because it improves the efficacy and feasibility of the particular procedure and hence the safety and quality of patient care. There are no specific classifications defining surgical complications of MI-TLIF and evaluating its incidence in the perioperative period in the current spine literature. Majority of studies evaluating complication rate of MI-TLIF are limited by small patient samples. 7 -10 Although some authors have previously defined and classified the various perioperative complications in spine surgeries, but such studies are very few with regard to MI-TLIF for single level lumbar degenerative diseases. 11 -14 We present a largest study till date performed over a period of 10 years reviewing the incidence of perioperative complications in MI-TLIF with minimum 2 years of follow-up period.
The primary aim of this study was to review the incidence of perioperative complications of MI-TLIF at single-level lumbar degenerative diseases. The secondary aim was to classify the complications to understand the efficacy and safety of MI-TLIF.
Materials and Methods
It was a prospective study performed at single institute over a period of 10 years (2009-2019). The institutional ethical and review committee approved the study. A total of 635 consecutive patients undergoing single-level primary MI-TLIF for degenerative lumbar spine disorders (degenerative lumbar canal stenosis with instability, prolapsed intervertebral disc, degenerative/dysplastic/isthmic spondylolisthesis) with minimum follow-up of 24 months were reviewed. A comprehensive clinical-radiological evaluation was conducted on more than one occasion to ascertain the indication of surgery in all patients and only those patients whose symptoms were not resolving to dedicated conservative trial with effects on activities of daily life were considered for surgical intervention. A single surgeon at a single institute performed all the surgeries included in the study following the same preoperative evaluation and postoperative mobilization protocols. Patients with tandem stenosis, revision surgery, and nondegenerative pathology like trauma, tumor, infection, and multilevel surgery were excluded from this study. Patients who did not complete minimum 24 months of follow-up were also excluded from the study.
Surgical Technique
Patients who underwent MI-TLIF had screws placed through paramedian incisions approximately 2 cm long and 3 to 5 cm lateral to the midline. The pedicle was cannulated with a Jamshidi needle under anteroposterior and lateral fluoroscopic guidance. The needles were exchanged for guidewires. The serial dilators were used to dilate over the guidewires and the pedicles were tapped using a cannulated tap. Screws were placed with corresponding screw extenders and the rod was introduced with a device through a separate proximal stab incision. After placement of locking-cap screws through the screw extenders and application of compression, the screws were torqued and the screw extenders were removed. Tubular decompression (20/22 mm tubes, METRx system, Medtronics) with partial unilateral laminectomy and inferior facetectomy done under a microscope. Next steps were discectomy, end plates preparation and titanium cage insertion with locally achieved bone graft through the same incision from where screws were inserted followed by closure in layers 15 (Figure 1).
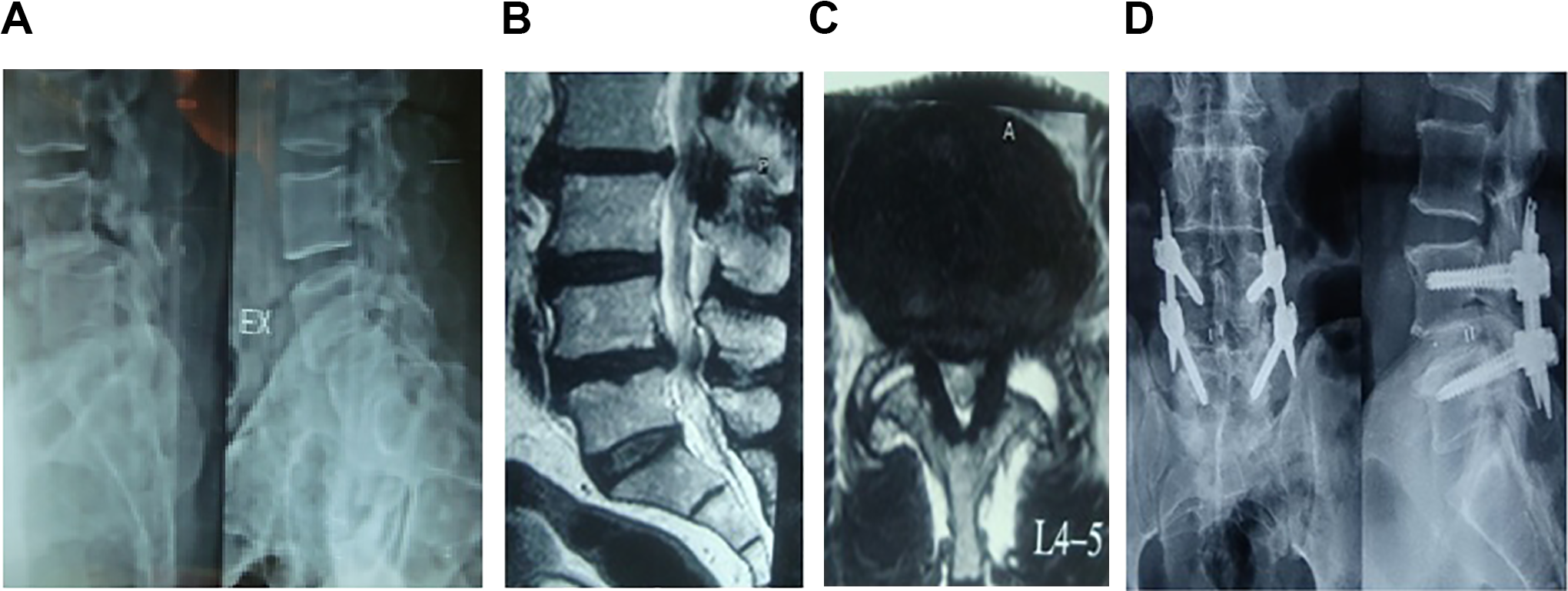
(A) Dynamic lumbar spine X-ray with instability and listhesis at L4-L5 level in a 75-year-old male patient. (B) Magnetic resonance imaging (MRI) showing L4-L5 degenerative spondylolisthesis pseudodisc bulge and canal stenosis in sagittal T2. (C) Bilateral facet effusion (left > right) in axial T2 with lumbar canal and lateral recess stenosis. (D) Postoperative standing lumbar spine X-ray showing implant with screws and interbody cage in situ at L4-L5 level (minimally invasive transforaminal lumbar interbody fusion [MI-TLIF]).
A total of 560 patients who underwent single-level lower lumbar MI-TLIF and who satisfied the aforementioned inclusion criteria were isolated for analysis and 75 patients were excluded. Preoperative data like demographic (age, sex, body mass index), level of fusion, clinical (visual analogue scale [VAS], Oswestry Disability Index [ODI], neurology), medical comorbidities, and radiological data was evaluated and recorded prospectively (Table 1). Intra- and postoperative parameters like operative time, blood loss, intraoperative adverse events (dural tears), hospital stay, and time required to become pain-free postsurgery were collected from medical records and review was done by 2 independent observers who are fellowship-trained spine surgeons (Table 1). The authors have proposed a descriptive classification for early (<6 months postsurgery) and late (>6 months postsurgery) perioperative complications of MI-TLIF procedure with 5 broad categories. All the patients of study group were divided and allotted into 5 categories depending on the respective complications they developed in their follow-up periods. This etiological and descriptive classification as suggested by the senior author has included most commonly seen complications in immediate and late postoperative period. All the complications were evaluated by senior author, senior physician, and recorded by 2 fellowship-trained spine surgeons. The patients who developed 2 or more complications from different categories were also recorded. Most of the patients were mobilized out of bed on first postoperative day and assisted to walk using walker. All the patients with and without classified complications were followed up with evaluation of VAS, ODI, and neurological parameters at periodic intervals of 1, 3, 6, 12, and 24 months. Fusion, screw loosening, pseudoarthrosis, and cage slippage were assessed with dynamic X-rays, computed tomography (CT) scan and magnetic resonance imaging (MRI) at the same regular follow-up protocols (Figure 2). Screw loosening is defined as a halo or lysis around screw in imaging studies and implant failure was defined as screw or rod get displaced from its original position and breakage of implant with loss of alignment. Statistical analysis was established with logistic regression analysis, analysis of variance (ANOVA), odds ratio, chi-square test, and Student t test. P value <.05 was considered as significant.
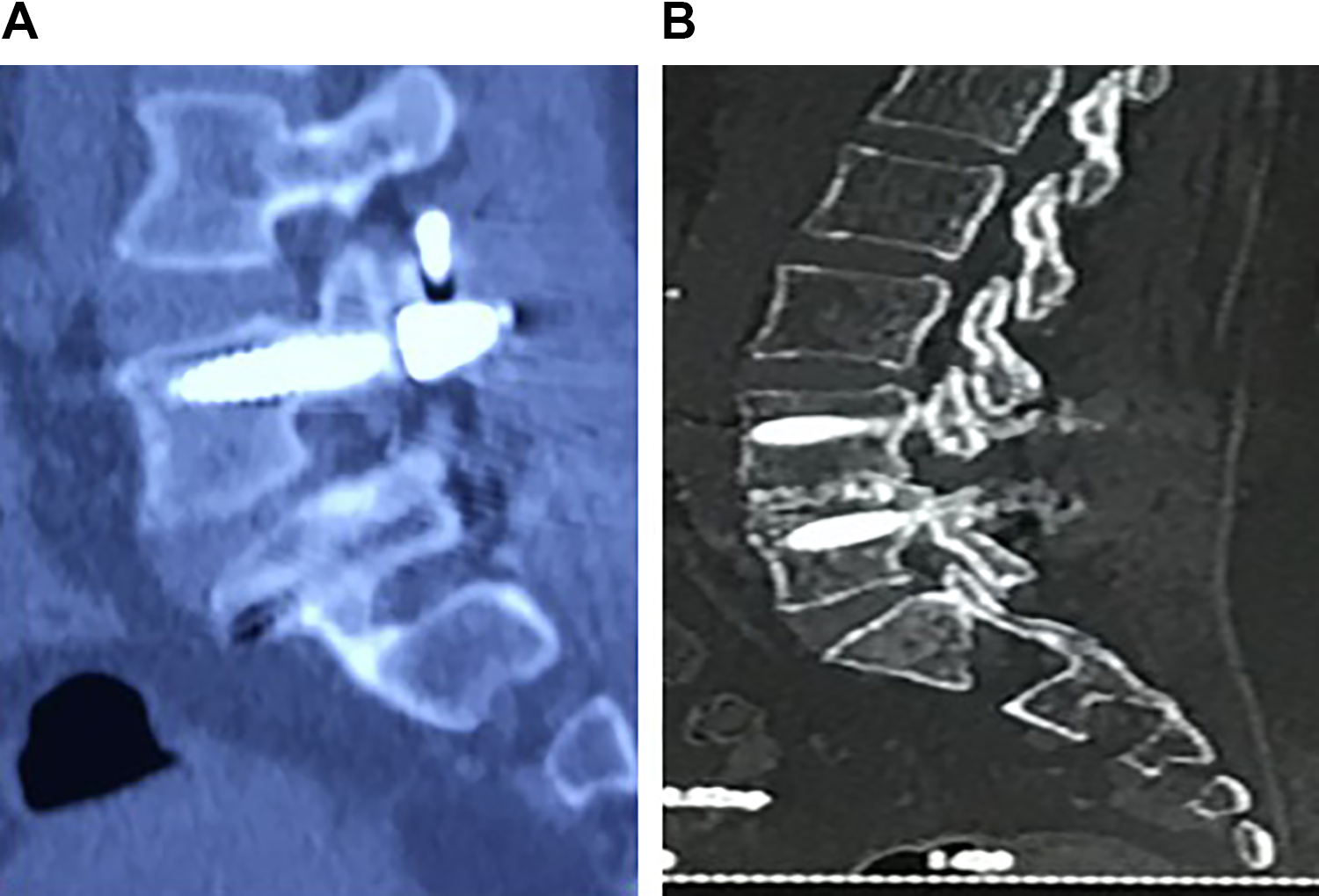
(A) Postoperative lumbar spine X-rays showing posterior migration of cage with screw loosening, implant failure, and pseudoarthrosis in a 71-year-old female. (B) Postoperative lumbar spine computed tomography (CT) scan showing rigid bone union at L4-L5 level in 68-year-old male.
Patient Demographic Data.
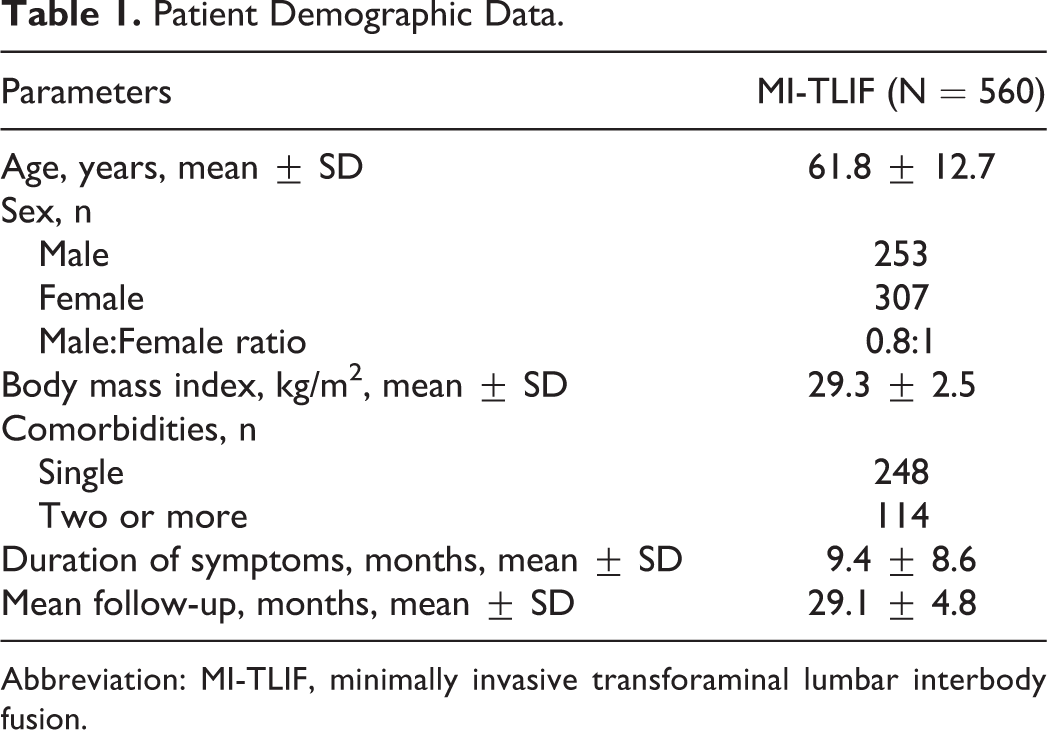
Abbreviation: MI-TLIF, minimally invasive transforaminal lumbar interbody fusion.
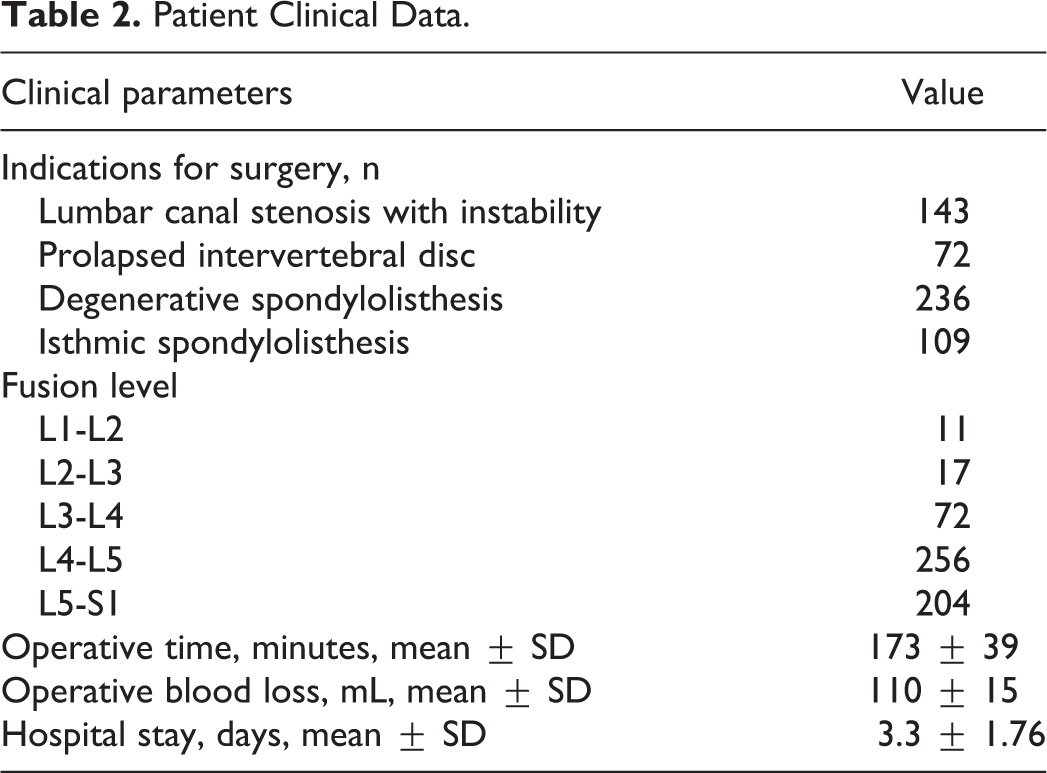
Patient Clinical Data.
Results
The study group comprised 560 patients with 253 males and 307 females. The mean age was 61.8 ± 12.7 years (age range 36-88 years). The mean body mass index (BMI) was 29.3 ± 2.5 kg/m2 (Table 1). A total of 348 patients were with single medical comorbidity and 114 patients were with 2 or more comorbidities (Table 1). Majority of the patients had mechanical low back pain and neurogenic claudication as the presenting symptom with mean duration of symptoms for 9.4 ± 8.6 months before index surgery. The most common indication for MI-TLIF was degenerative spondylolisthesis (42.14%) followed by lumbar canal stenosis with instability (25.53%) and isthmic spondylolisthesis (19.4%) (Table 2). The most commonly operated lumbar level was L4-L5 (45.7%) followed by L5-S1 (36.5%) level. The mean operative time was 173 ± 39 minutes and the mean operative blood loss was 110 ± 15 mL. The intraoperative minor dural tears were found in 16/560 (2.85%) patients and most of them were during the initial cases (first 50) of surgeon’s learning curve. All dural tears were managed with fibrin glue through the tubular dilators and watertight fascia closure with no postoperative dural tear–related complications. One patient developed significant intraoperative blood loss without any obvious reasons detected and required multiple blood transfusions in the postoperative period ending into a volume overload. No other major intraoperative complications were noticed. The mean hospital stay was 3.3 ± 1.76 days and mean follow-up was 29.1 ± 4.8 months.
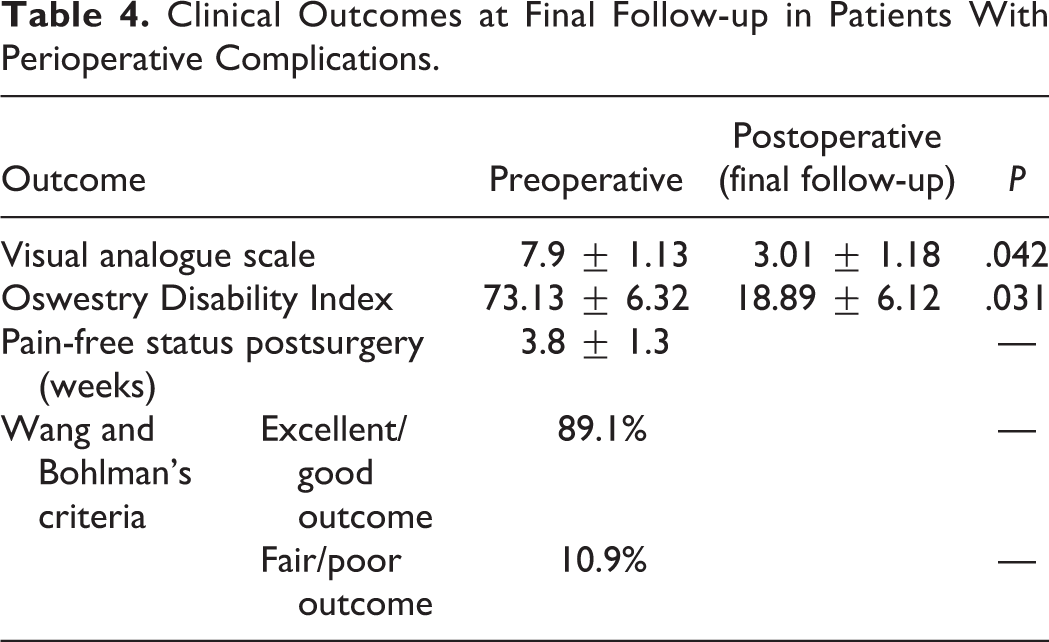
The overall incidence of the total complication was 25.5% (143/560) with no mortality (Table 3). The initial 3 years of learning curve comprised total 178 procedures with 44.3% rate of complication and last 7 years of practice comprised 382 patients with 16.75% rate of complication (Table 3). A total of 110 patients (19.64%) developed only 1 complication, 26 (4.64%) patients developed 2 complications, and only 7 patients (1.25%) developed 3 complications from the described categories. Ninety-four (16.78%) patients developed early (<6 months postsurgery) perioperative complications and 49 (8.75%) patients developed late (>6 months postsurgery) complications (Table 3). The most common postoperative complications were transient paresthesia in legs (3.21%) and superficial wound infections (3.39%), which were managed with regular dressing and antibiotics. Three patients (with known medical comorbidities diabetes and smoking) developed deep infections (0.5%) and wound dehiscence (0.35%) requiring open debridement with drain placement on seventh to ninth postoperative day without adding any additional morbidities. One patient developed transfusion-related problems after multiple blood transfusions on third postoperative period, which turned into acute respiratory distress syndrome. Two patients with previous history of coronary heart disease developed unstable angina and managed with cardiac team in the intensive coronary care unit. Although most patient were mobilized the next postoperative day, 3 patients with high-risk factors and associated morbidities developed deep vein thrombosis (DVT) that were managed with anticoagulation medications and pneumatic stockings prolonging the hospital stay. Seven patients developed new neurological deficit within 6 months to 1 year postoperative period due to various reasons like screw loosening, nerve root compression, posterior cage migration, and implant failure. All these patients were thoroughly evaluated with new dynamic X-ray, CT scan, and contrast MRI. Urinary complications were in the form of urinary tract infections (1.60%) and SIADH (syndrome of inappropriate antidiuretic hormone; 1.96%) that required prolonged catheterization in 8 (1.42%) patients. Surgical complications (MI-TLIF procedure related) were found in 44 (7.85%) patients. The early surgical complications like screw malposition (0.35%) and loosening (1.60%) were managed with reexposure and revision/removal of screw in symptomatic patients. The late surgical complications including pseudoarthrosis (0.71%), implant failure (0.35%), cage migration (0.5%), and adjacent segment disease (1.25%) were managed with revision surgeries after thorough clinical-radiological evaluation (Figure 2). The mean ODI and VAS scores showed significant improvement (P < .05) at final follow-up with considerable improvement in clinical parameters (Table 4). As per Wang’s criteria, 89.1% patients had satisfactory outcomes (excellent to good) and 10.9% had fair to poor outcomes at final follow-up (Table 4). The mean time required to become pain-free postsurgery was 3.8 ± 1.3 weeks in patients with perioperative complications. Revision surgeries were done in total 21 patients with perioperative complications after thorough clinical-radiological evaluation over a follow-up period of 2 years: 4 cases of pseudoarthrosis, 2 cases each of implant failures and cage slippage, 3 cases each of deep wound infections and symptomatic adjacent segment disease, 5 cases of screw loosening and malpositioning and 2 cases with newly arising neurological deficits.
Perioperative Complications.
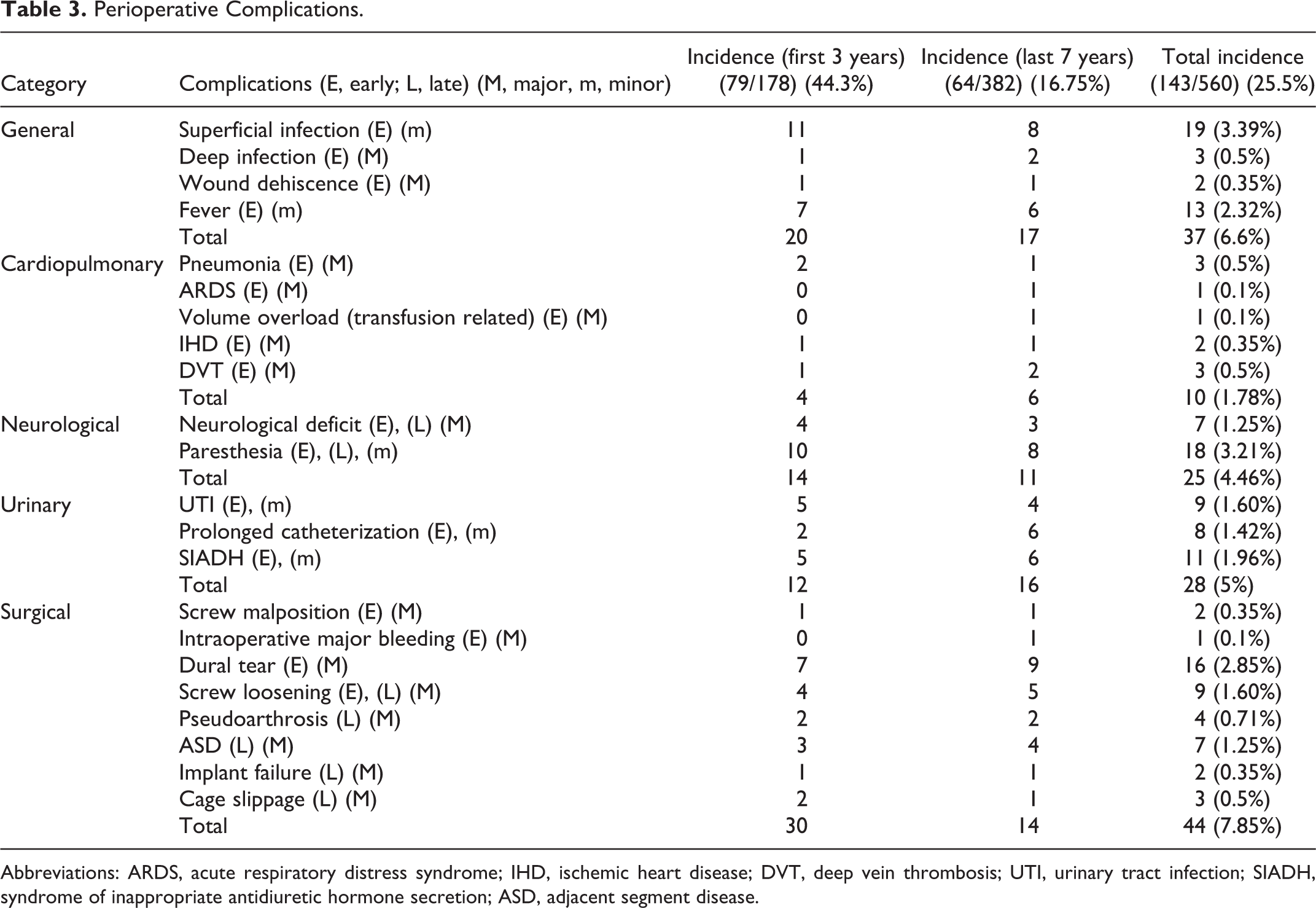
Abbreviations: ARDS, acute respiratory distress syndrome; IHD, ischemic heart disease; DVT, deep vein thrombosis; UTI, urinary tract infection; SIADH, syndrome of inappropriate antidiuretic hormone secretion; ASD, adjacent segment disease.
Clinical Outcomes at Final Follow-up in Patients With Perioperative Complications.
Discussion
The recent advances in surgical techniques, anesthesiology, patient care, and instrumentation design have made MI-TLIF a safer technique with improved outcomes and decreased morbidity rates. 1,16 This technology has allowed more complex procedures to be performed in populations considered to be at an increased surgical risks. Despite these advancements, studies evaluating the reliability and feasibility of MI-TLIF in view of perioperative complications are scanty either with less sample size or with lack of good evidence. Although reducing the approach-related complications is a primary aim of MI-TLIF, this must be accomplished without compromising the efficacy or outcome of the technique and without increasing the risk of the perioperative complications. 1 -4,10 The restricted anatomical view, lack of tactile perception, and steep learning curve inherent to MI-TLIF can increase the perioperative complications rate in treating degenerative lumbar diseases. Many studies have demonstrated satisfactory short-term clinical outcomes of MI-TLIF but studies evaluating the long-term outcome and perioperative complications are still lacking. Several previous studies have defined perioperative complications of MI-TLIF in varied ways that makes it difficult to compare the incidence of complications among studies. 17 -22 The authors have proposed a simple and descriptive classification for perioperative complications of MI-TLIF based on the duration of its occurrence and relation to the procedure. This study had 25.5% (143/560) overall incidence of the perioperative complication with no mortality (Table 3). The reasons for such a high incidence of perioperative complications might be the inclusion criteria and classification system used by the authors that is very simple and basic. However, all these complications happened over 10 years of experience with most of the complications during the initial 3 years of practice while going through the learning curve (Table 3). The authors have noted a substantial reduction in the complication while chasing the learning curve and mastering the technique. Ninety-four (16.78%) patients developed early (<6 months postsurgery) complications and 49 (8.75%) patients developed late (>6 months postsurgery) complications. Dural tear was the commonest intraoperative complications (2.85%) mostly in the first year of learning curve without any long-term clinical adverse effects such as wound breakdown, infection, and neurologic deficit. One of the benefits with tubular MI-TLIF is that soft tissue and muscles get collapsed into place while removing the tube thus reducing the dead space for CSF and hematoma formation. Urine retention, SIADH, and transient lower extremities paresthesia were the commonest early postoperative complications (Table 3). Acute urinary retention occurred in 8 patients (1.42%) who were elderly patients with comorbidities requiring prolonged catheterization for few days without permanent bladder involvement. The experience of surgeon and adequacy of decompression can determine immediate postoperative paresthesia that may be transient related to poor nerve handling due to limited operating window or permanent related with inadequate decompression. Among the late complication group, pedicle screw loosening and newly arising neurological deficit due to various causes like recurrent disc herniations, nerve root compression, posterior cage migration, and implant failure were common entities. All patients who complain of new radicular symptoms after MI-TLIF surgery should be thoroughly evaluated with new CT and MRI to identify pedicle screw loosening, graft dislodgement, and implant failure. Even with proper fluoroscopy, misplacement of the pedicle screws is possible due to lack of tactile perception and limited vision of anatomical landmarks. The previous studies have reported screw malposition rate 0.35% to 13%, which is in accordance with our result. 23,24 It is very important to get adequate pedicle margins from intraoperative fluoroscopy imaging and proper preoperative study of pedicle dimensions in imaging to reduce the rate of screw malposition and perforation. Tormenti et al 25 reported 25.4% (135/531) incidence of procedure-related complication in patients who underwent an open TLIF procedure during the study period. The incidence of dural tear, infection, and symptomatic pedicle screw displacement were 14.3%, 3.8%, and 2.1%, respectively, which are comparable to our clinical results. However, most of the complications in their study occurred in patients undergoing revision surgeries or multilevel TLIF procedures and current study had evaluated complications in single level MI-TLIF. Wu et al 26 had demonstrated similar results with fewer complications (7.5%) in the MI-TLIF group compared to higher complications (12.6%) in open TLIF; however, the fusion rates were comparable in both MI and open TLIF procedures. Peng et al 16 reported statistically similar good long-term clinical outcomes with fewer complications in patients undergoing MI-TLIF procedures (6.9%) compared with those who had undergone open TLIF (13.8%). Although in one review study reported by Chaudhary et al, 27 which includes several studies published after 2009, the authors stated that the drawbacks of MI-TLIF procedure included the higher complication and reoperation rates during the learning phase of the surgeon. However, the evidence presented is of low quality. A statistical comparison of the complications is difficult between our study and others because there is no consensus in the literature to define or classify the complications of MI-TLIF and clinical data after spine surgery. However, in current study the authors described simple classifications for peri-operative complications in MI-TLIF to evaluate particular complication depending on its duration of occurrence in each category. In view of the lower complication rate of MI-TLIF compared with open TLIF as reported in previous studies, our results need reevaluation by comparing MI-TLIF with open TLIF. The clinical outcomes in terms of satisfaction after surgery, as well as pain and functional improvement (89.1% excellent to good outcome) appear to be comparable to open TLIF. However, the quality of the evidence as it stands is poor and randomized controlled trials or well-controlled prospective cohort studies are needed to more accurately determine the complication risk and efficacy of MI-TLIF.
The main limitations of study are retrospective design without randomization even though data collected prospectively. Another limitation was that this study was that the study was limited to patients undergoing single-level MI-TLIF performed by a single surgeon and so results might not be applicable to patients undergoing multilevel MI-TLIF. The learning curve and experience of operating surgeon could also change the outcome and complication rate. In addition, the authors did not evaluate different age groups, comorbidities, and bone mineral density for all the patients and so could not determine causative relationship between complications and comorbidities/bone mineral density in patients undergoing MI-TLIF. Finally, a midterm follow-up of 2 years has been analyzed here. It does not allow us to know whether differences will appear over a longer period.
Conclusion
This article represents the largest study of perioperative complications in MI-TLIF (total incidence 25.5%) for degenerative lumbar disease in the literature. MI-TLIF is an effective procedure with substantial clinical benefits in the form of excellent to good clinical-radiological outcomes. The described classification for perioperative complications is helpful to record, to evaluate, and to understand the etiology based on its duration of occurrence in the perioperative period.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.