
Abstract
Study Design:
A multicenter, retrospective case series.
Objective:
In the past several years, screw fixation of the cervical spine has become commonplace. For the most part, this is a safe, low-risk procedure. While rare, screw backout or misplaced screws can lead to morbidity and increased costs. We report our experiences with this uncommon complication.
Methods:
A multicenter, retrospective case series was undertaken at 23 institutions in the United States. Patients were included who underwent cervical spine surgery from January 1, 2005, to December 31, 2011, and had misplacement of screws requiring reoperation. Institutional review board approval was obtained at all participating institutions, and detailed records were sent to a central data center.
Results:
A total of 12 903 patients met the inclusion criteria and were analyzed. There were 11 instances of screw backout requiring reoperation, for an incidence of 0.085%. There were 7 posterior procedures. Importantly, there were no changes in the health-related quality-of-life metrics due to this complication. There were no new neurologic deficits; a patient most often presented with pain, and misplacement was diagnosed on plain X-ray or computed tomography scan. The most common location for screw backout was C6 (36%).
Conclusions:
This study represents the largest series to tabulate the incidence of misplacement of screws following cervical spine surgery, which led to revision procedures. The data suggest this is a rare event, despite the widespread use of cervical fixation. Patients suffering this complication can require revision, but do not usually suffer neurologic sequelae. These patients have increased cost of care. Meticulous technique and thorough knowledge of the relevant anatomy are the best means of preventing this complication.
Introduction
Techniques for instrumented fixation and fusion of the cervical spine have rapidly advanced in the past 30 years. These techniques have helped surgeons adequately manage complex trauma, tumor, and degenerative pathologies. For the most part, these are safe, low-risk procedures. Hadra in 1890 described the use of wiring and graft techniques to perform the first spinal fusion procedures. 1,2 These techniques were standard until the start of modern cervical spinal fusion with Roy-Camille in the 1970s. 1,3 Since this time there have been improvements in technique and implants, which have made the procedures safer, thus leading to increased adoption of instrumented cervical fusion.
Within the United States, approximately 150 000 cervical fusion procedures are performed each year. 4 Around 90% of cervical fusions are anterior with 10% being posterior. 4 The use of plate and screw instrumentation for anterior cervical fusion has become a mainstay, so much so that in 2010 the American Medical Association combined 2 Current Procedural Terminology codes into a comprehensive code. The indications for cervical fusion are well established, based on an abundance of studies showing clinical and biomechanical efficacy. 5 -10
Despite these studies there is a paucity of literature detailing the complications associated with cervical spinal fusion. Most studies are retrospective in design, contain a small numbers of patients, report single-institution data, relate to a single indication, or contain information with outdated procedures. 9,11 -29 The overall complication rate for cervical fusion procedures is low, and these earlier studies may not reliably provide data on less common complications.
While rare, screw backout or misplaced screws can lead to morbidity, the need for revision surgery, and increased costs. Previous studies report a low incidence of this particular event. We report our experiences with this uncommon but potentially harmful complication.
Methods
We have conducted a retrospective multicenter case series study involving 21 high-volume surgical centers from the AOSpine North America Clinical Research Network, selected for their excellence in spine care and clinical research infrastructure and experience. Medical records for 17 625 patients who underwent cervical spine surgery (levels from C2 to C7) between January 1, 2005, and December 31, 2011, inclusive, were reviewed to identify occurrence of 21 predefined treatment complications. The complications included reintubation requiring evacuation, esophageal perforation, epidural hematoma, C5 palsy, recurrent laryngeal nerve palsy, superior laryngeal nerve palsy, hypoglossal or glossopharyngeal nerve palsy, dural tear, brachial plexopathy, blindness, graft extrusion, misplaced screws requiring reoperation, anterior cervical infection, carotid artery injury or cerebrovascular accident, vertebral artery injuries, Horner’s syndrome, thoracic duct injury, tetraplegia, intraoperative death, revision of arthroplasty and, pseudomeningocele. Trained research staff at each site abstracted the data from medical records, surgical charts, radiology imaging, narratives, and other source documents for the patients who experienced one or more of the complications from the list. Data were transcribed into study-specific paper case report forms. Copies of case report forms were transferred to the AOSpine North America Clinical Research Network Methodological Core for processing, cleaning, and data entry.
Descriptive statistics were provided for baseline patient characteristics. Paired t test was used to analyze changes in clinical outcomes at follow-up compared to preoperative status. A total of 12 903 cervical procedures qualified for screening for the complication of misplaced screw requiring reoperation.
Results
A total of 12 903 patients met the inclusion criteria and were analyzed. There were 11 instances of misplaced screws requiring reoperation, for an incidence of 0.085%, translating to a rate of 8.5 per 10 000 cervical spine surgeries (Table 1). A total of 8887 cases screened were specifically only anterior procedures making the incidence 3/8887 (0.034%). The remaining cases screened could be posterior or posterior/anterior combined procedures. We do not have enough information on the remaining cases to make a determination of the incidence of misplacement of posterior screws requiring reoperation, but suspect it would a higher rate. The average age of the patients was 53 years, and there were 4 female patients. No patients had evidence of osteoporosis at the time of surgery. Three of the patients were current smokers, and 5 patients had previously smoked. Myelopathy and radiculopathy were the most common reasons for initial operation, 6/11 (55%) and 5/11 (45%), respectively, with 1 patient having both symptoms. The average hospital length of stay was 9.25 days. There were 4 anterior and 7 posterior procedures. Importantly, there were no changes in the health-related quality-of-life metrics due to this complication. There were no new neurologic deficits; patients most often presented with pain, and screw backout was diagnosed on postoperative plain X-ray or computed tomography scan. Five of 11 (45%) and 3/11 (27%) patients were diagnosed within the original hospital admission or postoperative clinic follow-up, respectively, while we were unable to obtain these data on 3 cases. Two patients with anterior screw backout had swallowing problems, which resolved with reoperation. The most common location for screw backout was C6, 4/11 (36%); 2 patients had screw backout at C2. Patient 4 had aggressive removal of an osteophyte complex and an anterior cervical screw penetrated into the central canal (Figure 1A and B). The patient had symptoms of right-sided proximal upper extremity weakness, which resolved with removal and revision of the C5 penetrating screw (Figure 1C).
Case Information.
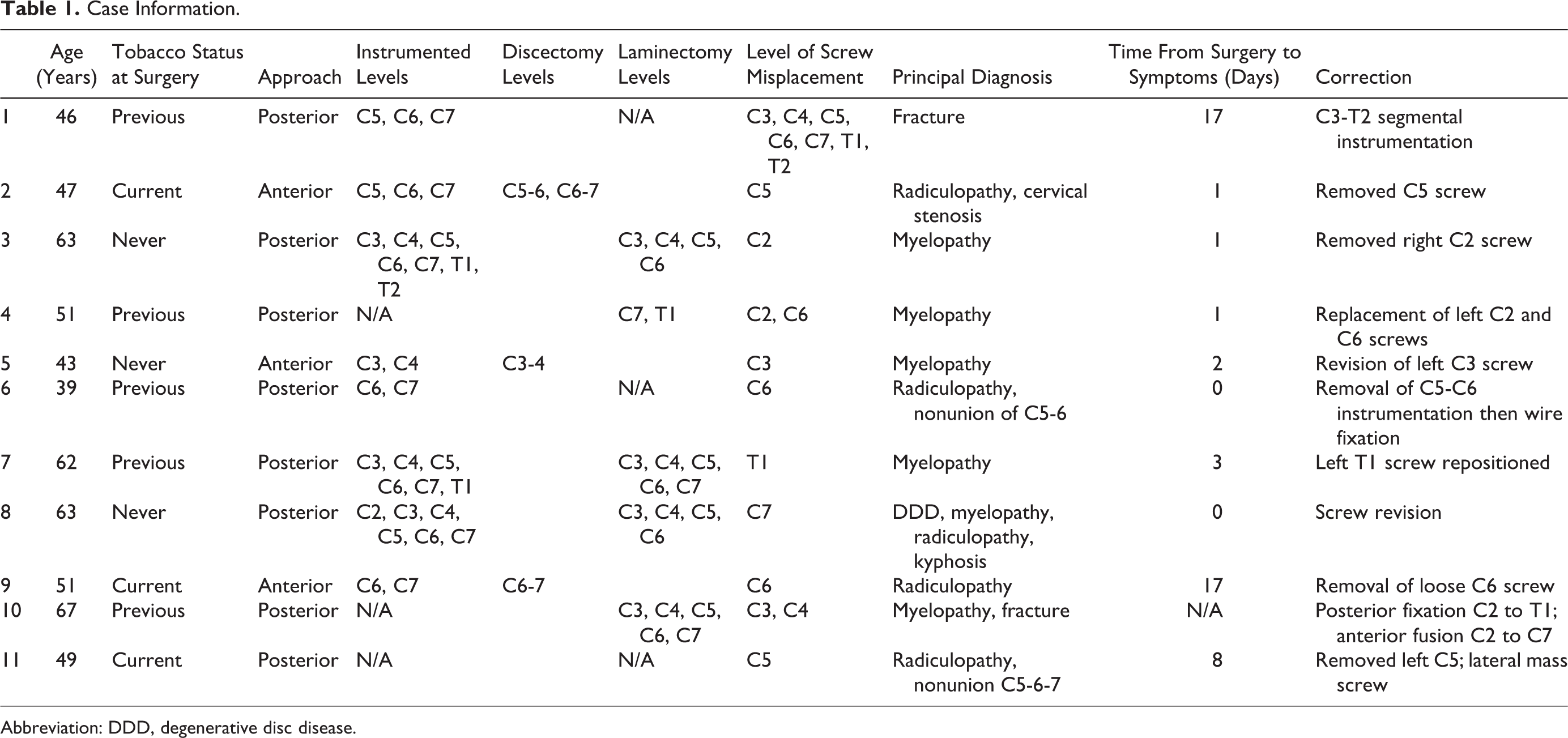
Abbreviation: DDD, degenerative disc disease.
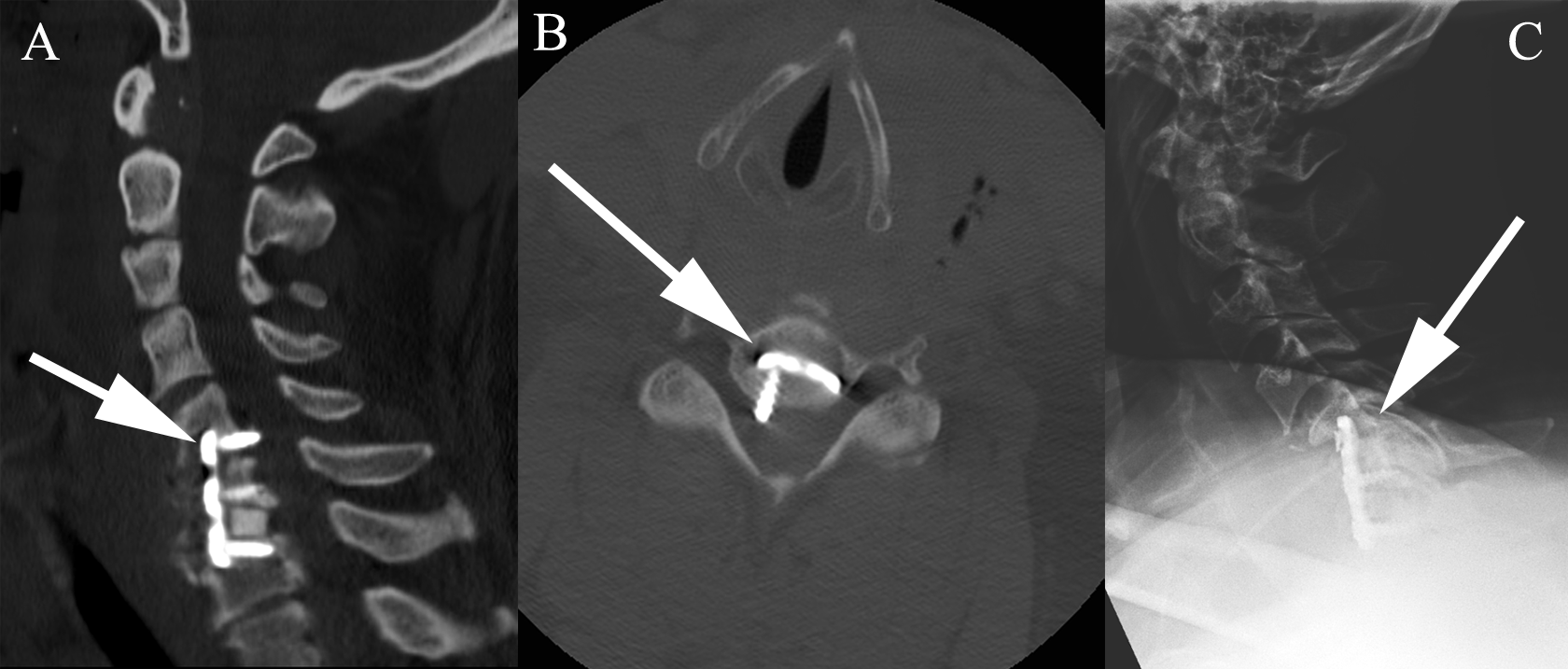
(A) Sagittal computed tomography scan with arrow demonstrating misplaced right C5 screw. (B) Axial computed tomography scan with arrow demonstrating misplaced right C5 screw. (C) Postoperative lateral cervical spine X-ray demonstrating removal of misplaced C5 screw.
Discussion
Due to the risk and complexity associated with cervical spinal surgery, current techniques and approaches did not become popular until the mid-20th century. The initial procedures mainly included posterior decompression and posterior wiring for stabilization. Anterior approaches developed from surgery for head and neck pathology separate from spinal disease. Advances in imaging, operative microscopes, and instrumentation have allowed cervical spinal surgery to progress to the current state.
Since 1891 when the first cervical fusion procedure was performed there have been sequential advances described by many authors to develop the early fixation techniques. 1 -3,30 -43
Several biomechanical animal and cadaver studies have been performed during the rapid advancement in cervical spinal instrumentation over the past 30 years. Posterior instrumented fusion studies have consistently proven the stiffness of the constructs to be equal to or greater than that of an intact spine. 6,8,9,30,44 -47 The most common failure in these studies was screw pullout at a predictable amount of force. 46 Anterior plating studies have strongly guided the development of each type of system and have shown continued improvement in the efficacy of constructs. 44,45,47
Incidence of Complications
The advancements and improvements in cervical spinal instrumentation would be expected to decrease the rate of hardware-related complications. The overall complication rate of cervical spinal surgery is estimated to be 0.2% to 17.8%. 4,17,27,48 After 30 days, the most common complication is related to instrumentation dislodgement, breakage, or both, and occurs in 2% to 25% of cases of spinal fusion procedures. 27 Reoperation rate for instrumented spinal fusions is reported between 2% and 25%, with the majority related to pseudoarthrosis. 27
There have been few studies looking at the complications related to instrumented cervical fusion. The majority of information is based on case reports, retrospective reviews, and small series of patients. There are few recent articles addressing the rate of screw backout or misplacement requiring reoperation, and many older studies include the use of unrestricted devices that permitted screw backout.
Fehlings et al prospectively collected 302 cervical spondylotic myelopathy patients and found a perioperative complication rate of 15.6%, with 11.6% minor and 7.0% major perioperative risk. 17 Three patients had instrumentation malposition/migration for a rate of 1% in the perioperative period. The risk of delayed complications was 4.4%. Three patients had instrumentation/graft migration or instrumentation failure, making the risk of delayed hardware complications 1.1%. Not all patients in this small study received spinal instrumentation. 17
Shapiro et al 27 reported on 299 consecutive spinal instrumentation cases. Of 195 anterior cervical plating procedures, 5 (2.6%) required reoperation for hardware failure. 27 Some of these failures were due to trauma around the time of surgery. Cole et al used the MarketScan Database and identified 13 662 patients who underwent anterior or posterior cervical fusion for degenerative disc disease. 48 The rate of any complication excluding dysphagia was 12.3% and 17.8% for anterior and posterior approaches, respectively. There is, however, no specific mention of the reason for reoperation in the study. 48
In 2011, Katonis et al 9 reported on 1662 consecutively placed lateral mass screws. Screw pullout occurred in 3 (1.3%) patients, but they did not mention if these patients required reoperation or if the system was a screw-plate or polyaxial screw-rod implant system. The report also mentioned 11 (0.6%) screws had a suboptimal trajectory but no patient required reoperation for removal or replacement of hardware. 9 Al Barbarawi et al 49 had 2 screw pullout cases out of 430 lateral mass screw-rod fixation cases. Two (4.0%) cases were found to have screw pullout in the study by Kim et al using Yoon’s method. 50
Kasimatis et al included 74 patients from 1990 to 2005 who underwent anterior cervical treatment of cervical spine trauma in their study looking at complications. Screw backout was reported in 4 (5.4%) cases, all of which were unrestricted backout plates. Seven cases (9.5%) had “less-than-ideal” positioning of the construct with only one case requiring reoperation because of a malpositioned screw being completely in the intervertebral space. 23 Veeravagu et al looked at the MarketScan Database from 2006 and 2010 and found in 28 777 patients a reoperation rate of 9.13% and 10.7% for single-level and multilevel anterior cervical fusion, respectively. 51 Unfortunately, their data did not include data about the rate of reoperation related specifically to hardware failure. Shapiro et al found no screw pullout when using locking screw fixation in 246 consecutive anterior cervical fusion cases. 52
Several reports exist in the literature of screw pullout resulting in dysphagia and sometimes erosion into the gastrointestinal tract. 53 -55 They continue to document the incidence of screw pullout related to misplacement to be uncommon, but can result in complications with serious morbidity and increased costs.
Frequently screw pullout is related to malpositioned placement at the time of implantation. There are few studies that look directly at this relation. Coe et al performed a systematic review of lateral mass screw fixation, and implant removal was defined as a surgical procedure to correct malpositioned screws, screw breakout, or loosening. Reoperation as defined was necessary for 27 (1.2%) of 2185 screws placed in 294 patients across 5 studies. 10,56 -60
The limitations of the study pertain largely to it being retrospective in nature. Limited information was available to determine the number of patients with screw misplacement that did not require reoperation. There was also insufficient information within the screening population to determine the number of screws placed for comparison. The screening population was divided into anterior only and posterior or anterior/posterior combined groups. This does not allow for calculation of the incidence of posterior misplacement requiring revision, and it can only be speculated that this number would be much higher than the rate for anterior alone procedures.
Conclusions
This study represents the largest series to analyze and tabulate the incidence of screw backout or misplacement requiring reoperation following cervical spine surgery. The data suggest this is a very rare adverse event, despite the widespread use of cervical fixation. Due to the methodology of this study, there is a potential for underestimation of screw misplacement requiring reoperation within this series of patients. This potential for underreporting is more likely to occur in the case of posterior cervical fusion as this could not be calculated based on this study. The data therefore represents a lower limit for the incidence of screw misplacement requiring reoperation. Patients suffering this complication require hardware revision, but do not usually suffer neurologic sequelae. These patients have extended hospital stays, which add to the cost of care. Meticulous technique and thorough knowledge of the relevant anatomy are the best means of preventing this complication.
Footnotes
Authors’ Note
This study was ethically approved by the institutional ethics committees at all participating sites.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jeremy C. Peterson reports grants from AOSpine North America during the conduct of the study; Wellington K. Hsu reports grants from AOSpine North America during the conduct of the study, personal fees from Medtronic, personal fees from Stryker, personal fees from Bacterin, personal fees from Graftys, personal fees from Ceramtec, personal fees from Relievant, personal fees from Bioventus, personal fees from Globus, personal fees from SpineSmith, outside the submitted work; Michael G. Fehlings reports grants from AOSpine North America during the conduct of the study; Robert A. Hart reports grants from AOSpine North America during the conduct of the study, other from CSRS, other from ISSLS, other from ISSG Exec Board, personal fees from Depuy Synthes, personal fees from Globus, personal fees from Medtronic, other from Evans, Craven & Lackie, other from Benson, Bertoldo, Baker, & Carter, personal fees from Seaspine, personal fees from Depuy Synthes, other from Spine Connect, personal fees from Depuy Synthes, outside the submitted work; Alan S. Hilibrand reports grants from AOSpine North America during the conduct of the study, other from Amedica, Vertiflex, Benvenue, Lifespine, Paradigm Spine, PSD, Spinal Ventures, outside the submitted work, and in addition, Dr. Hilibrand has a patent Aesculap, Amedica, Biomet, Stryker, Alphatec, with royalties paid; Tony Tannoury reports grants from AOSpine North America during the conduct of the study; Thomas E. Mroz reports other from AO Spine during the conduct of the study, personal fees from Stryker, personal fees from Ceramtec, other from Pearl Diver, outside the submitted work; Bradford L. Currier reports grants from AOSpine North America during the conduct of the study, personal fees from DePuy Spine, personal fees from Stryker Spine, personal fees from Zimmer Spine, other from Zimmer Spine, other from Tenex, other from Spinology, other from LSRS, other from AOSNA, outside the submitted work; Jeremy L. Fogelson reports grants from AOSpine North America during the conduct of the study and Previous Consultant for one day to Depuy-Synthes March 2014; Bruce C. Jobse reports grants from AOSpine North America during the conduct of the study; Eric M. Massicotte reports grants from AOSpine North America during the conduct of the study, grants from Medtronic, Depuy-Synthes Spine Canada, personal fees from Watermark Consulting, grants from AOSpine North America, nonfinancial support from AOSpine North America, outside the submitted work; and K. Daniel Riew reports personal fees from AOSpine International, other from Global Spine Journal, other from Spine Journal, other from Neurosurgery, personal fees from Multiple Entities for defense, plaintiff, grants from AOSpine, grants from Cerapedics, grants from Medtronic, personal fees from AOSpine, personal fees from NASS, personal fees from Biomet, personal fees from Medtronic, nonfinancial support from Broadwater, outside the submitted work; Paul M. Arnold reports grants from AOSpine North America during the conduct of the study; other from Z-Plasty, other from Medtronic Sofamore Danek, other from Stryker Spine, other from FzioMed, other from AOSpine North America, other from Life Spine, other from Integra Life, other from Spine Wave, other from MIEMS, other from Cerapedics, other from AOSpine North America, outside the submitted work; Zachary A. Smith reports grants from AOSpine North America during the conduct of the study; Ahmad Nassr reports grants from AOSpine North America during the conduct of the study; Ra’Kerry K. Rahman reports grants from AOSpine North America during the conduct of the study; in addition, Dr. Rahman has a patent Deformity System & Pedicle Screws pending. Chadi A. Tannoury reports grants from AOSpine North America during the conduct of the study; Anthony F. De Giacomo Dr. De Giacomo reports grants from AOSpine North America during the conduct of the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by AOSpine North America Inc, a 501(c)3 nonprofit corporation.