
Abstract
Study Design
Retrospective Cohort Study.
Objectives
This study aimed to examine the effect of state legislation on prescribing behavior after a commonly performed spinal procedure, posterior lumbar interbody fusion (PLIF).
Methods
Two cohorts of patients from the Pearl Diver Database were created based on patients who underwent PLIF surgery in 2014-15 and 2018-19. We compared opioid prescription rates and morphine-milli-equivalent (MME) between states with and without prescription legislation.
Results
We analyzed 50 958 PLIF patients from 2014-15 and 46 751 patients from 2018-19. Among them, 38 states passed opioid prescription laws in 2016-2017, while 12 states did not. The percentage of patients receiving opioid prescriptions within 365 days post-surgery remained similar in both time periods (49% in 2014-15 and 48% in 2018-2019). This trend was consistent across states with and without prescription legislation (50% vs 48% in 2014-2015, and similar in 2018-19). Opioid prescription quantity significantly decreased in all states between 2014-15 and 2018-19. In states with legislation, average MME dropped from 9198 ± 21 002 to 4932 ± 13 213 (46.4% decrease), and in states without legislation, it decreased from 9175 ± 21 032 to 4994 ± 11 687 (45.6% decrease). However, these differences were not statistically significant (P = .7985).
Conclusion
From 2014 to 2018, there was a significant decrease in the number of opioids prescribed after PLIF. However, this decrease occurred irrespective of state legislation on prescribing practices being passed. We believe the reduction in opioids prescribed was due to increased awareness surrounding the dangers of opioids among physicians.
Keywords
Introduction
The opioid epidemic in the United States set its roots in the widespread belief that opioids were safe for the treatment of chronic pain. Without an adequate understanding of the addictive qualities of opioids in combination with cultural norms that place a high value on pain relief, the dangers of this drug class went unrealized for many years.1,2 The percentage of the global population represented by Americans is merely 5%, yet they utilize 80% of the total annual opioids distributed.3-5 Insufficient regulation contributed to a steady increase in opioid overdoses and deaths, with this trend continuing despite efforts to address the issue.6,7 By 2010, the role of opioid prescribing practices was determined to be a major factor in the rising death toll in the absence of prescription limitation laws and treatment resources. 1 In response to the growing crisis, the Department of Health and Human Services declared a public health emergency in 2017, leading to increased legislative action at the state level. Many states passed laws aimed at reducing the number of opioid prescriptions and the dose of morphine milligram equivalents (MME) that could be prescribed to patients, as well as the length of time providers could prescribe opioids following surgical interventions.
Despite these efforts, the opioid epidemic remains a significant public health challenge. In 2020, there were nearly 57 000 deaths caused by opioid overdoses, with prescription opioids accounting for nearly 18% of these cases. 8 This marks a 16% increase in prescription opioid overdose deaths compared to the previous year. 8 The number of drug overdose deaths involving prescription opioids rose 5-fold between 1999 and 2017, with a brief dip in deaths between 2017 and 2019, before the trend resumed its upward trajectory in 2020. 9
Patients suffering from degenerative spine disorders often experience symptoms such as pain, which is a subjective and challenging experience to quantify due to various influencing factors. Consequently, many patients are prescribed pain medications before surgery to alleviate their discomfort. Effective pain management is equally important in the postoperative period since patients who experience less pain tend to have faster recovery rates following surgery.10,11 Striking a balance between the risks and benefits of opioids in pain management poses a challenging task for healthcare providers. Moreover, given the historical undertreatment of pain among racial and ethnic groups in the United States, discussions on scaling back prescribing practices and proper pain management become even more intricate.12,13
In the context of spine surgery, opioid prescribing practices have undergone changes. In response to the opioid epidemic, state-level publications report a decrease in the number of opioids prescribed by providers, aiming to reduce long-term opioid dependency.14,15 Although literature exists on the impact of legislation and opioid prescribing patterns in specific states,16,17 there is a lack of national-level studies in this area.
The objective of the present study is to evaluate the influence of state legislation on the prescription rates of opioids during a commonly performed surgical procedure known as Posterior Lumbar Interbody Fusion (PLIF).
Methods and Materials
The present study, deemed exempt from informed consent by the Institutional Review Board, adopted a retrospective cross-sectional design utilizing the PearlDiver Inc. M151 database. The M151 database is a vast repository of de-identified medical record claims data collected from 151 million patients, randomly sampled from all payers with the exception of Kaiser and Tricare, longitudinally tracked between 2010 and 2020. The study collected patient data, such as the Current Procedural Terminology (CPT) codes, opioid utilization, and geographical location of the procedures by states.
This investigation analyzes the number of PLIF procedures performed between 2014-2015 and 2018-2019 and assesses the number of prescriptions for opioids written 90 days prior to, 90 days following, and 365 days following the procedure. To evaluate the impact of state legislation on opioid prescribing practices, we compared the prevalence rate of opioid prescription and total cumulated morphine-milli-equivalent (mme) between the patients in states with and without the passage of opioid legislation.
All query was executed in the PearlDiver database. The query captured all posterior lumbar interbody fusion (PLIF) procedures, employing the CPT codes 22633 and 22630, with exclusion criteria applied to exclude those who underwent an additional spine-level procedure, as identified by the CPT codes 22552 and 22600. Only single-level PLIF patients were analyzed in this study to ensure consistency and minimize potential confounding variables associated with more complex surgical procedures, which can lead to increased pain and higher opioid consumption.
22630 Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar 22633 Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar
Subsequently, patients were segregated into two major cohorts for each query, with each major cohort further divided into two sub-groups, resulting in four groups for each query. The pre-policy groups consisted of patients who underwent their respective procedures during 2014-2015, as this period preceded the passing of most state policies on opioid prescription limits. The post-policy groups consisted of patients who underwent their respective procedures during the years 2018-2019, after the passage of most state policies on opioid prescription limits. Within each major cohort, patients were further separated into two groups based on whether or not the state where the procedure occurred had passed a policy on opioid prescription limits. Ballotpedia.org, a trusted and non-partisan online encyclopedia known for its credibility in providing comprehensive information about political policies and laws, was used as the source for obtaining information on opioid prescription policies and laws in different states.
Statistical Analysis
Univariate chi-squared analysis was used to compare the number of patients who were prescribed opioids for each group in each query. Unpaired t test analysis was used to compare the average mme values for patients prescribed opioids for each group in each query. The statistical significance was set to P < .05. Odds ratios were used to assess the magnitude of differences in chi-squared analysis, while Cohen’s d values were used to assess the effect size in t test analysis.
Results
Demographics
A total of 260 158 patients were identified to have PLIF procedures. Out of these patients, 50 958 had the procedure during 2014-2015, while 46 751 had the procedure during 2018-2019.
From 2016 to 2018, 12 out of 50 states did not enact any laws or policies to reduce opioid prescription limits. These states included Arkansas, California, Georgia, Idaho, Illinois, Kansas, Mississippi, Montana, New Mexico, South Dakota, Wisconsin, and Wyoming. The remaining 38 states had implemented at least one law or policy aimed at reducing opioid prescription limits during the same time frame.
90 Days Before Surgery
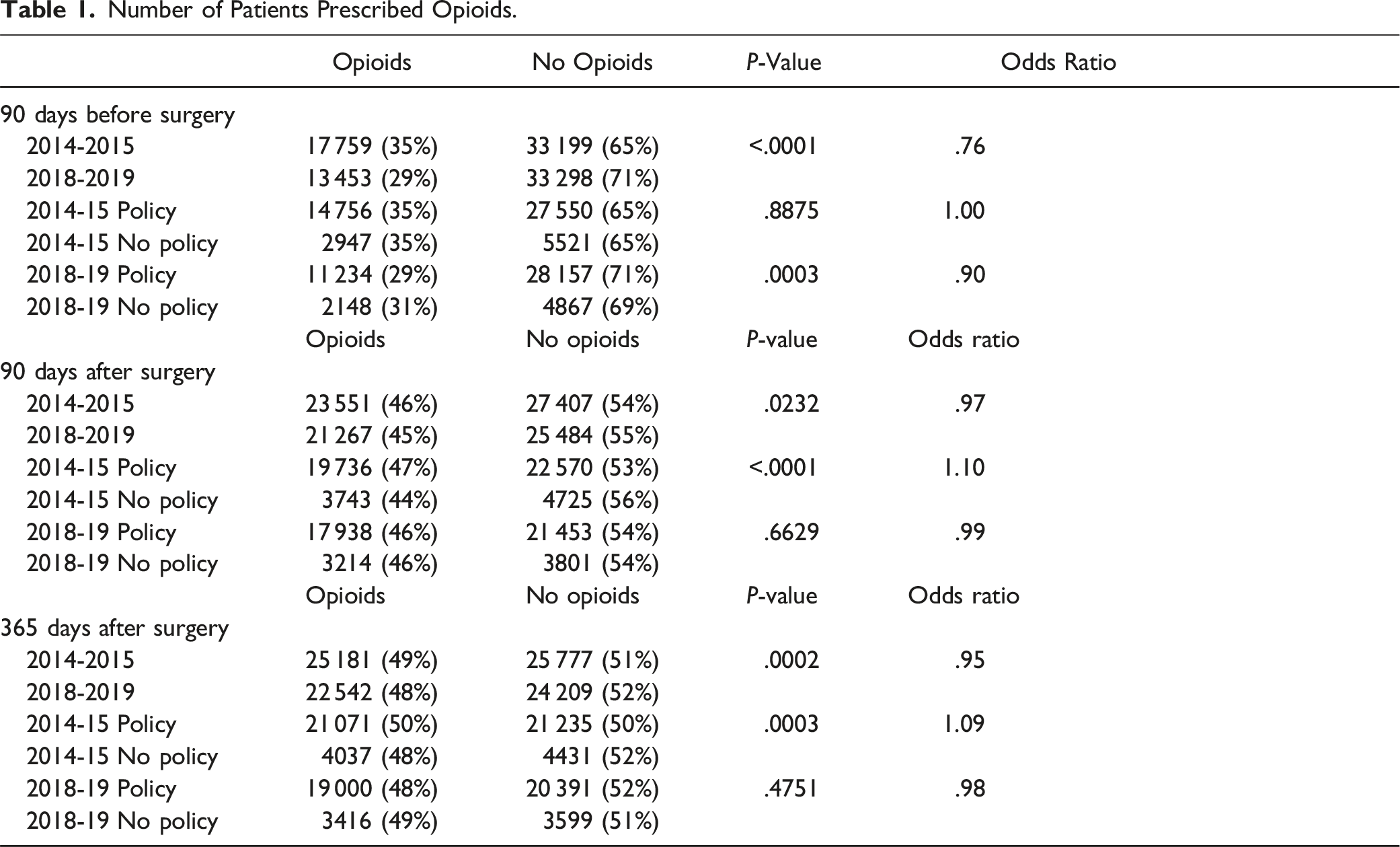
Number of Patients Prescribed Opioids.
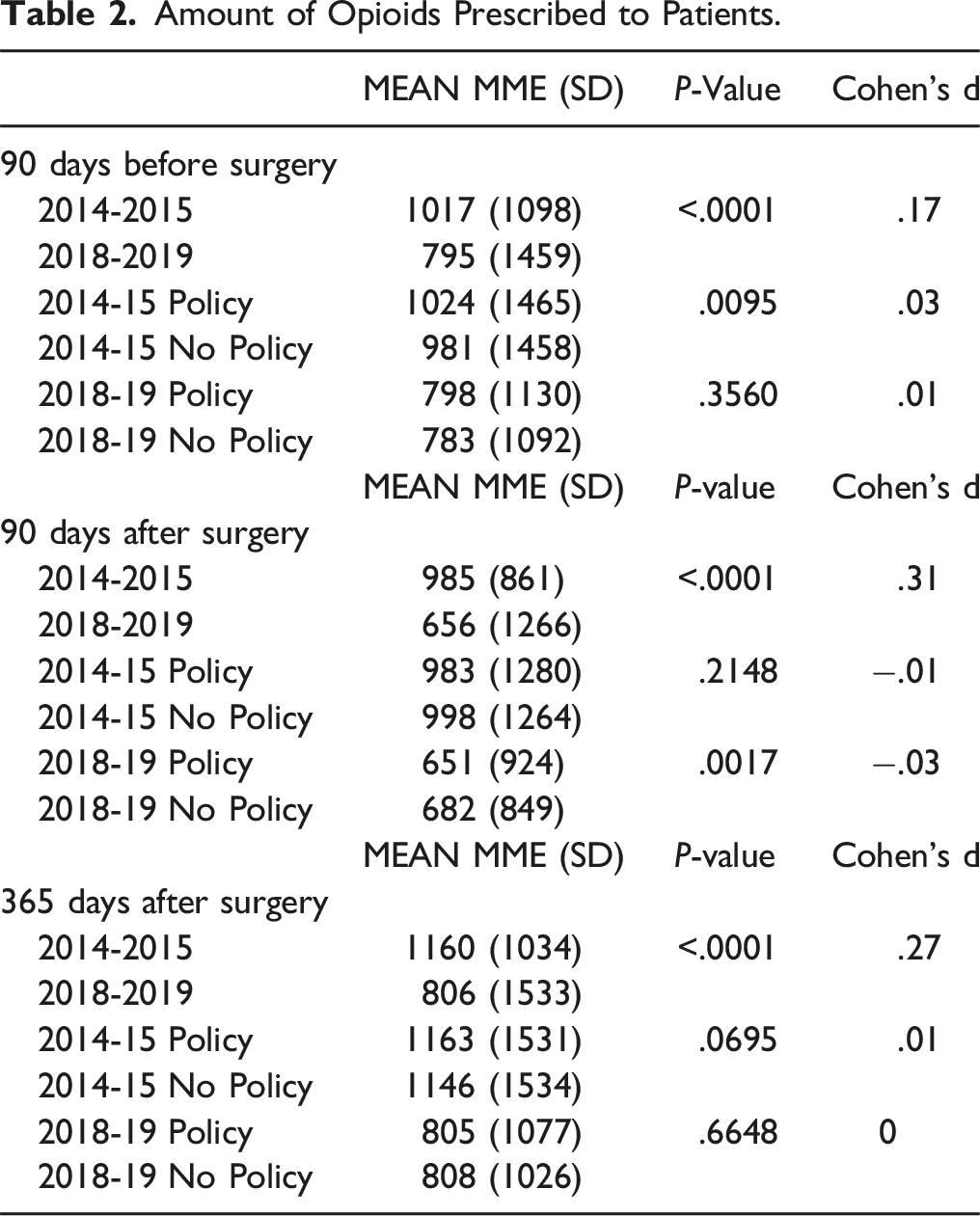
Amount of Opioids Prescribed to Patients.
90 Days After Surgery
Univariate chi-squared analysis showed that the percentage of PLIF patients prescribed opioids decreased from the pre-policy group (46%) to the post-policy group (45%) (OR = 97, P = .0232) (Table 1). In the pre-policy group, the percentage of PLIF patients prescribed opioids was significantly higher in states that passed a policy (47%) compared to those that did not (44%) (OR = 1.10, P < .0001) (Table 1). In the post-policy group, there was no difference in the percentage of PLIF patients prescribed opioids between states that passed a law (46%) and those that did not (46%) (OR = .99, P = .6629) (Table 1).
Univariate t test analysis indicated that the average MME taken per PLIF patient was significantly higher in the pre-policy group (985 ± 861 MME) compared to the post-policy group (656 ± 1266 MME) (Cohen’s d = .31, P < .0001) (Table 2). In the pre-policy group, there was no difference in the average MME taken per PLIF patient between states that passed a policy (983 ± 1280 MME) and those that did not (998 ± 1264 MME) (Cohen’s d = −.01, P = .2148) (Table 2). In the post-policy group, the average MME taken per PLIF patient was lower in states that passed a law (651 ± 924 MME) compared to those that did not (682 ± 849 MME) (Cohen’s d = −.03, P = .00165) (Table 2).
365 Days After Surgery
Results of the univariate analysis revealed that there was a significant decrease in the proportion of PLIF patients with opioid prescriptions
Univariate t test analysis showed that the average MME taken per PLIF patient was observed from the pre-policy group (1160 ± 1034 mme) to the post-policy group (806 ± 1533 mme) (Cohen’s d = .27, P < .0001) (Table 2). However, in the pre-policy group, there was no significant difference in the average mme of PLIF patients between states that passed a policy (1180 ± 1419 mme) and those that did not pass a policy (1142 ± 1476 mme) (Cohen’s d = .01, P = .3577) (Table 2). Additionally, in the post-policy group, no significant difference was observed in the average mme of PLIF patients between states that passed a law (800 ± 1226 mme) and those that did not pass a law (788 ± 1212 mme) (Cohen’s d = .00, P = .6026) (Table 2).
Discussion
Following the declaration of the opioid epidemic by the Centers for Disease Control and Prevention (CDC) in 2011, policymakers across the United States began passing laws aimed at reducing the number of opioids prescribed and the length of opioid treatment following procedures such as PLIF. The legislation focused on limiting the number of days patients could receive opioids following surgery, the MME that patients could receive, or both. Analysis of PLIF procedures from 2014 to 2018 shows a reduction in the number of opioids prescribed across all 50 states in the U.S. Between those years, a difference was observed in the prescribing practices among states that invoked legislation limiting the number of opioids allowed to be prescribed (Table 2). However, in 2018-2019, no significant difference was found in the number of opioids prescribed in states that had opioid limitation laws vs those without, suggesting that the reduction in opioids prescribed following spine procedures from 2014 to 2018 was not significantly impacted by the presence or absence of policy at the state level.
Our findings are not supportive of our initial hypothesis that states with opioid prescription limitation laws would experience a greater reduction in opioids prescribed when compared to states without policies regarding opioids. However, it does provide us with useful information when considering how to optimize our approach to the opioid epidemic. In 2012, the FDA established the Opioid Analgesic Risk Evaluation and Mitigation Strategy (REMS) to increase drug monitoring and emphasize the importance of patient education on opioid risks and benefits. 6 Following the initial approval of REMS in 2012 and the publication of CDC Guidelines for opioid prescribing in 2016, there was a shift toward safer opioid prescribing habits by clinicians, seeing a trend toward writing fewer opioid prescriptions altogether. 18 Drug monitoring programs and the National All Schedules Prescription Electronic Reporting Act (NASPER) are utilized widely by providers when prescribing opioids, and from 2006 to 2013, these resources were shown to reduce the total amount of opioids prescribed by 8% and prescription opioid overdose-related mortality by 12%. 19
Pain management may involve a range of treatments, including but not limited to medications and cognitive therapy. One medication example is buprenorphine, a partial agonist at the mu-opioid receptor. It provides pain relief without eliciting a maximum response from the receptor. 20 In the United States, our acceptance of buprenorphine therapy for opioid use disorder (OUD) has been slow due to the required “waiver” and training necessary to prescribe the medication.21,22 However, in France, expanding access to buprenorphine for OUD resulted in a 79% reduction in opioid overdose deaths over a 6-year period. 23 Notably, as of January 2023, the Drug Enforcement Administration’s “X-waiver” has been lifted, allowing all providers to prescribe buprenorphine for patients with OUD. 24 Programs aimed at educating physicians and the public about the dangers of opioid dependence and addiction may have a larger impact on the opioid crisis than initially thought. By investing in programs, there may be a change in the cultural perspectives surrounding opioids, and patients would have additional support from providers as they navigate addiction. Adding additional resources for pain management and support for addiction treatment help create a more holisitc and effective environment to address the crisis. 1
The opioid epidemic is a product of past beliefs that opioids were safe and non-addictive when used for chronic pain and a lack of appropriate regulation and oversight of opioid distribution and use.1,7 This highlights the importance of considering the historical context and long-term consequences of current actions and policies, as well as the need for continuous education and reassessment in the field of medicine and public health. While there has been progress in reducing opioid prescriptions and increasing awareness of the risks of opioid use, there is still much work to be done to address the opioid epidemic. For example, the opioid crisis has disproportionately affected certain populations, such as rural communities and people of color, and addressing these disparities requires targeted efforts and resources.25-27 While there is support for the role state legislation played in reducing opioid prescriptions in some settings, such as oculoplastic and orbital procedures before and after the opioid limiting policy was passed in Michigan, 28 the effect of state policy was not widespread, as is seen in our results. Efforts involving state legislation may not have had as significant of an impact in isolation as they did in combination with increased awareness and education of physicians and patients alike.
This study has limitations due to its retrospective nature. Additionally, it specifically analyzes the changes in opioid prescribing practices across the nation in the context of PLIF operations, with and without public policy intervention. Our findings suggest that the decrease in opioid prescribing practices was not solely driven by policy changes but rather influenced by various factors in the setting of PLIF. While the data revealed a minor distinction in opioid prescription rates in the pre-policy groups, this discrepancy was largely attributed to the substantial sample sizes, and both policy groups eventually converged post-policy, showing no significant difference in prescription rates. This convergence stands as the primary takeaway message: Regardless of a state’s policy status, the rate of patients receiving opioid prescriptions remains consistent across both groups in the post-policy period. Nonetheless, the observed shifts in the number of patients prescribed opioids from pre-policy to post-policy periods, all less than 2%, suggest that any potential impact of the policies on prescription rates may be limited. Additionally, we acknowledge that surgical techniques, such as minimally invasive procedures, which gained popularity during the study period, could have influenced postoperative pain management and opioid consumption. Therefore, while our study sheds light on the relationship between state-level policies and opioid prescriptions, it does not account for other potentially influential variables in the evolving landscape of spinal surgery and pain management. It is also important to note that these results may not be generalizable to all settings or procedures, as there are instances where policy is believed to have significantly impacted opioid prescriptions. 28 Furthermore, it is essential to recognize that prescribing policies do not necessarily reflect actual usage. Patients may have been prescribed opioids but chose not to take the medications. 29 While we acknowledge the limited scope of this analysis regarding opioid prescribing in the context of PLIF, it is worth considering the significant time and resources invested in developing public policy, which should ideally have a widespread effect on prescribing practices.30-32 The lack of influence observed in the setting of spine surgery raises concerns about how we allocate resources in our fight against opioid addiction and overdose. 33 Future studies analyzing the impact of public health policy incentivizing alternative approaches to chronic pain management in spine surgery will help us understand how other resources, besides pain medication, can be used to manage a patient’s pain. 34
Conclusion
In conclusion, from 2014 to 2018, there has been a significant decrease in the number of opioids prescribed after PLIF, however, this decrease occurred irrespective of state legislation on prescribing practices passed. We believe the reduction in opioids prescribed was due to increased awareness surrounding the dangers of opioid use among physicians and an increase in resources that help providers monitor and treat opioid use in their patient populations. This study suggests the importance of physician awareness in implementing better patient practices to address the ongoing opioid epidemic effectively.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.