
Abstract
Study Design
Retrospective case series.
Objective
To determine risk factors associated with prolonged opioid use after lumbar fusion and to elucidate the effect of opioid use on patient-reported outcome measures (PROMs) after surgery.
Methods
Patients who underwent 1–3 level lumbar decompression and fusion with at least one-year follow-up were identified. Opioid data were collected through the Pennsylvania Prescription Drug Monitoring Program. Preoperative “chronic use” was defined as consumption of >90 days in the one-year before surgery. Postoperative “prolonged use” was defined as a filled prescription 90-days after surgery. PROMs included the following: Short Form-12 Health Survey PCS-12 and MCS-12, ODI, and VAS-Back and Leg scores. Logistic regression was performed to determine independent predictors for prolonged opioid use.
Results
The final analysis included 260 patients. BMI >35 (OR: .44 [.20, .90], P = .03) and current smoking status (OR: 2.73 [1.14, 6.96], P = .03) significantly predicted postoperative opioid usage. Chronic opioid use before surgery was associated with greater improvements in MCS-12 (β= 5.26 [1.01, 9.56], P = .02). Patients with prolonged opioid use self-reported worse VAS-Back (3.4 vs 2.1, P = .003) and VAS-Leg (2.6 vs 1.2, P = .03) scores after surgery. Prolonged opioid use was associated with decreased improvement in VAS-Leg over time (β = .14 [.15, 1.85], P = .02).
Conclusions
Current smoking status and lower BMI were significantly predictive of prolonged opioid use. Excess opioid use before and after surgery significantly affected PROMs after lumbar fusion.
Introduction
In the field of spine surgery, there has been increasing awareness of the association between chronic opioid usage with postoperative morbidity and mortality. 1 Low back pain represents one of the most prevalent etiologies of chronic pain and is related to disability and low socioeconomic status.2-6 Menendez and colleagues 1 recently reported that patients undergoing spinal arthrodesis had the highest rate of preoperative opioid dependence when compared to patients undergoing other orthopedic procedures. Chronic treatment for back pain with opioid medications remains controversial, yet healthcare expenditures related to opioids and national opioid prescribing patterns continue to rise annually.7-10 For these reasons, opioid use among patients with chronic low back pain remains a critical issue for spine surgeons. 11
Although previous studies have investigated risk factors for prolonged opioid use after spine surgery, there is limited evidence pertaining to patient-reported outcomes associated with opioid use after lumbar fusion.12-18 The primary purpose of this investigation was to identify risk factors that may predict prolonged opioid use after lumbar decompression and fusion. The secondary goal was to determine whether preoperative opioid tolerance or postoperative opioid use may be associated with changes in patient-reported outcome measures (PROMs) after lumbar fusion.
Methods
Patient Selection and Data Collection
After Institutional Review Board approval (IRB#19D.508), patients over 18 years of age who underwent 1–3 level lumbar decompression and fusion at a single, academic center between 2013 and 2017 were retrospectively identified using current procedural terminology codes 22558 and 22585 (anterior lumbar interbody fusion), 22612 and 22614 (posterior lumbar fusion), 22630 and 22632 (posterolateral interbody fusion), 22633 and 22634 (combined posterior and posterolateral interbody technique), and a structured query language search. Waiver was granted for patient informed consent as a minimal risk research study. Procedures were performed by one of seven fellowship-trained spine surgeons. Patients were excluded if they had less than one-year follow-up and if they had received surgical intervention for malignancy, infection, or trauma, or if they were undergoing revision surgery. Patients were also excluded if opioid use records were unobtainable. Demographics gathered from the medical record included the following: age, sex, body mass index (BMI), months of clinical follow-up, smoking status (never, current, or former), preoperative diagnosis, worker’s compensation status, insurance status, and self-reported preoperative mental health history. BMI was defined binarily as either greater or less than 35 kg/m2 to differentiate between obesity and severe obesity.
PROMs included the Short Form-12 Health Survey Physical Component Score (PCS-12) and Mental Component Score (MCS-12), the Oswestry Disability Index (ODI), and the Visual Analogue Scale Back (VAS-Back) and Leg (VAS-Leg) pain scores. Outcomes data were collected using the institution’s OBERD software (OBERD, Columbia, MO USA).
Opioid use data were collected through the Pennsylvania Prescription Drug Monitoring Program (PDMP), which is an initiative that tracks the prescribing and dispensing of Schedule II through V controlled substances within the state. Opioid-use parameters, included (1) duration of usage measured in days, (2) daily dose as measured in morphine milligram equivalent or MME, (3) number of tablets/pills obtained, and (3) prescription-filling pharmacy zip codes. Additionally, given the potential association of increased opioid use with distance traveled to fill prescriptions, the “maximum distance traveled” to fill an opioid medication was calculated with a distance calculation tool (© Free Map Tools) using patients’ home and furthest pharmacy zip code.19,20
To elucidate how preoperative and postoperative opioid use patterns might correlate with outcomes, the cohort was analyzed by the following two strategies. First, preoperative opioid use status was defined as either “chronic” or “non-chronic.” Chronic-opioid users were those that had been consuming opioids for greater than 90 days within one-year prior to surgery. 21 Chronic users must have also been using opioid medications for greater than 50% of those days. 21 Patients that did not fit these criteria were considered non-chronic users preoperatively. Second, postoperative opioid use status was defined as either “prolonged” or “non-prolonged” use. Prolonged opioid usage after surgery was defined as a prescription filled after the 90-day postoperative period based on PDMP data.22,23
Statistical Analysis
Demographics and PROMs were represented by corresponding median, counts, and interquartile range, and categorical values were represented as percentages. Continuous variables were assessed using a Mann–Whitney U-test, and categorical variables were compared using a chi-squared test. Descriptive statistics were used for baseline characteristics when comparing chronic and non-chronic users preoperatively and then prolonged and non-prolonged users postoperatively. To predict prolonged opioid use after lumbar fusion, a multivariable logistic regression model was developed based on preoperative demographics and opioid-use related parameters. Only variables with a P-value <.2 from univariate analyses were included in the regression. Each risk factor was described as an odds ratio (OR) and corresponding 95% confidence interval.
Baseline and postoperative scores for each PROM in the non-chronic and chronic opioid usage groups were compared using a Wilcoxon rank test. The same comparison was done for non-prolonged and prolonged users. Changes in PROMs were assessed using the delta (postoperative minus preoperative scores). Recovery ratios were defined as delta PROMs divided by the difference between optimal and observed scores. Optimal scores were considered either 100 (PCS-12/MCS-12) or 0 (ODI, VAS-Back, and VAS-Leg).24,25 The percentage of patients reaching the minimal clinically important difference (MCID) was calculated using the following established cutoffs: PCS-12: 8.8 points; MCS-12: 9.3 points; ODI: 6.8 points; VAS-Back: 2.1; and VAS -Leg: 2.4 points. 26 Multiple linear regression analysis was then conducted for each PROM adjusting for age, sex, BMI, smoking status, preoperative diagnosis, and worker’s compensation status to determine the effect of opioid use patterns on changes in outcomes over time (delta outcome).
All statistical analyses were performed using SPSS Statistics (Version 26.0; IBM Corporation, Armonk, NY) and R Studio software (R Foundation for Statistical Computing, Vienna, Austria). A P-value of ≤.05 was considered statistically significant.
Results
Characteristics of Non-Chronic and Chronic Opioid Users Preoperatively.
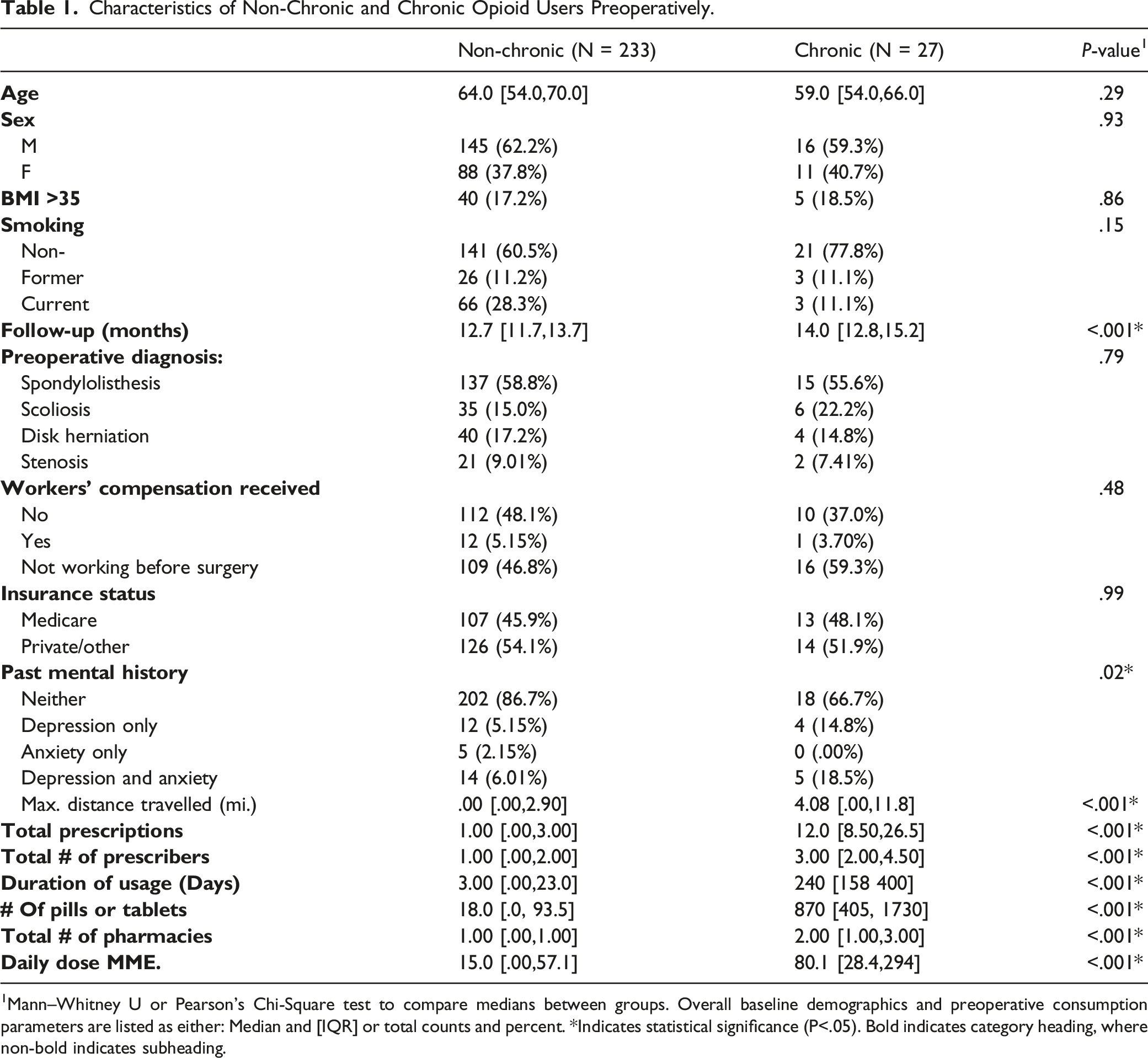
1Mann–Whitney U or Pearson’s Chi-Square test to compare medians between groups. Overall baseline demographics and preoperative consumption parameters are listed as either: Median and [IQR] or total counts and percent. *Indicates statistical significance (P<.05). Bold indicates category heading, where non-bold indicates subheading.
Characteristics of Non-Prolonged Opioid Use and Prolonged Opioid Use Patients Postoperatively.
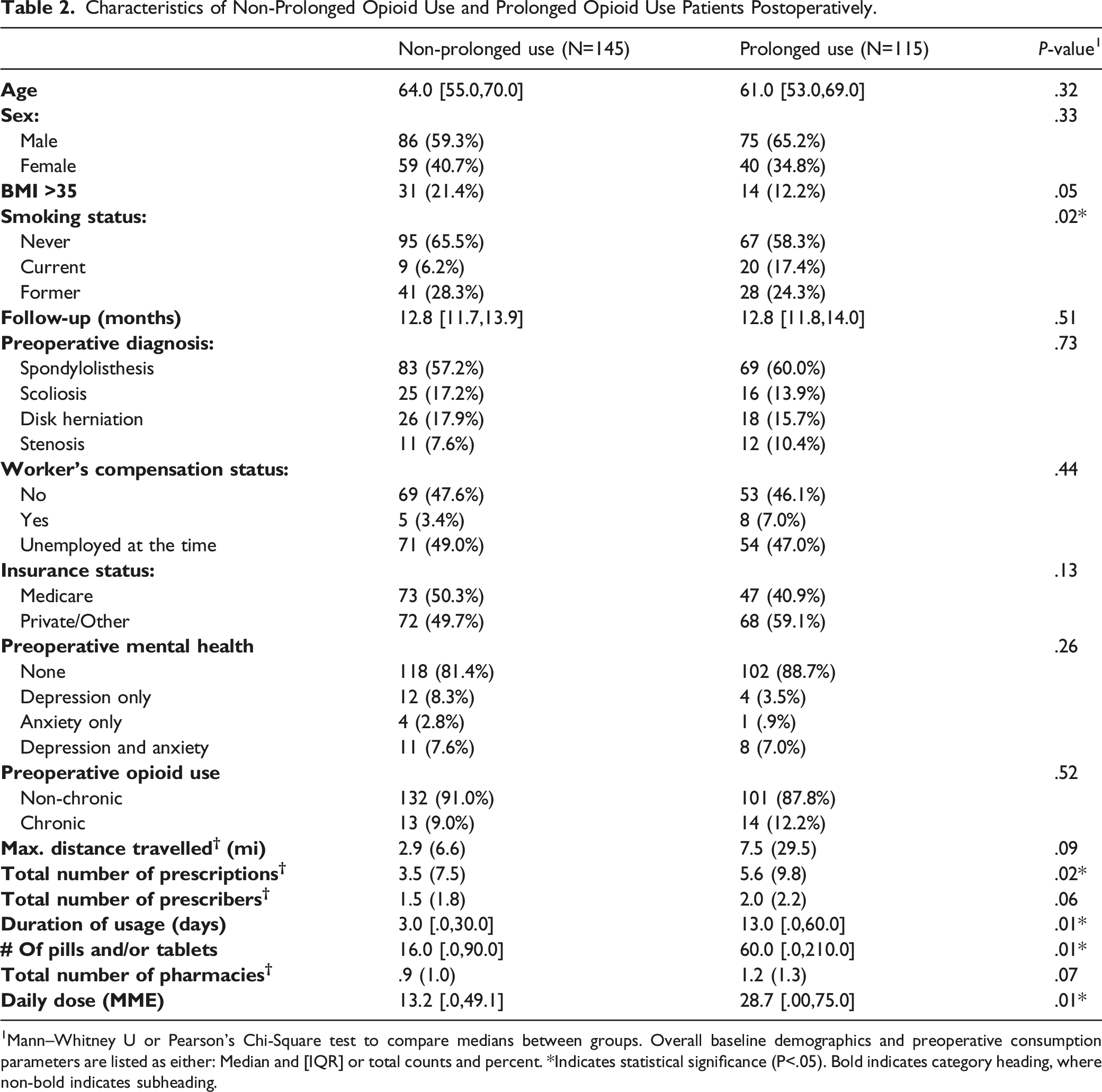
1Mann–Whitney U or Pearson’s Chi-Square test to compare medians between groups. Overall baseline demographics and preoperative consumption parameters are listed as either: Median and [IQR] or total counts and percent. *Indicates statistical significance (P<.05). Bold indicates category heading, where non-bold indicates subheading.
Risk Factors for Prolonged Opioid Use
Risk Factors for Prolonged Opioid Use after Lumbar Fusion.
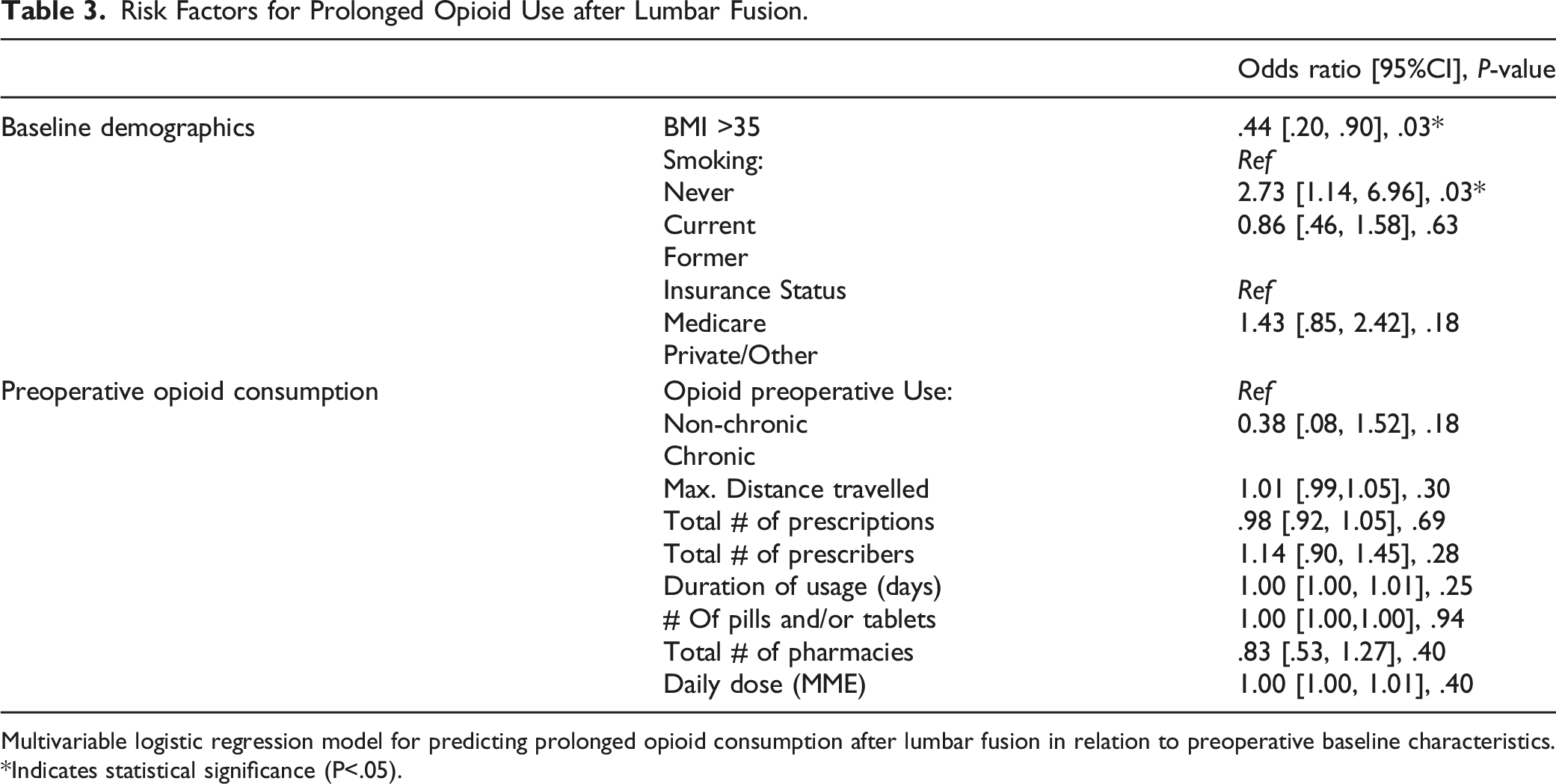
Multivariable logistic regression model for predicting prolonged opioid consumption after lumbar fusion in relation to preoperative baseline characteristics. *Indicates statistical significance (P<.05).
Patient-Reported Outcome Measurements–Chronic vs Non-chronic
Non-Chronic vs Chronic Opioid User Status and Patient Reported Outcomes after Lumbar Fusion.
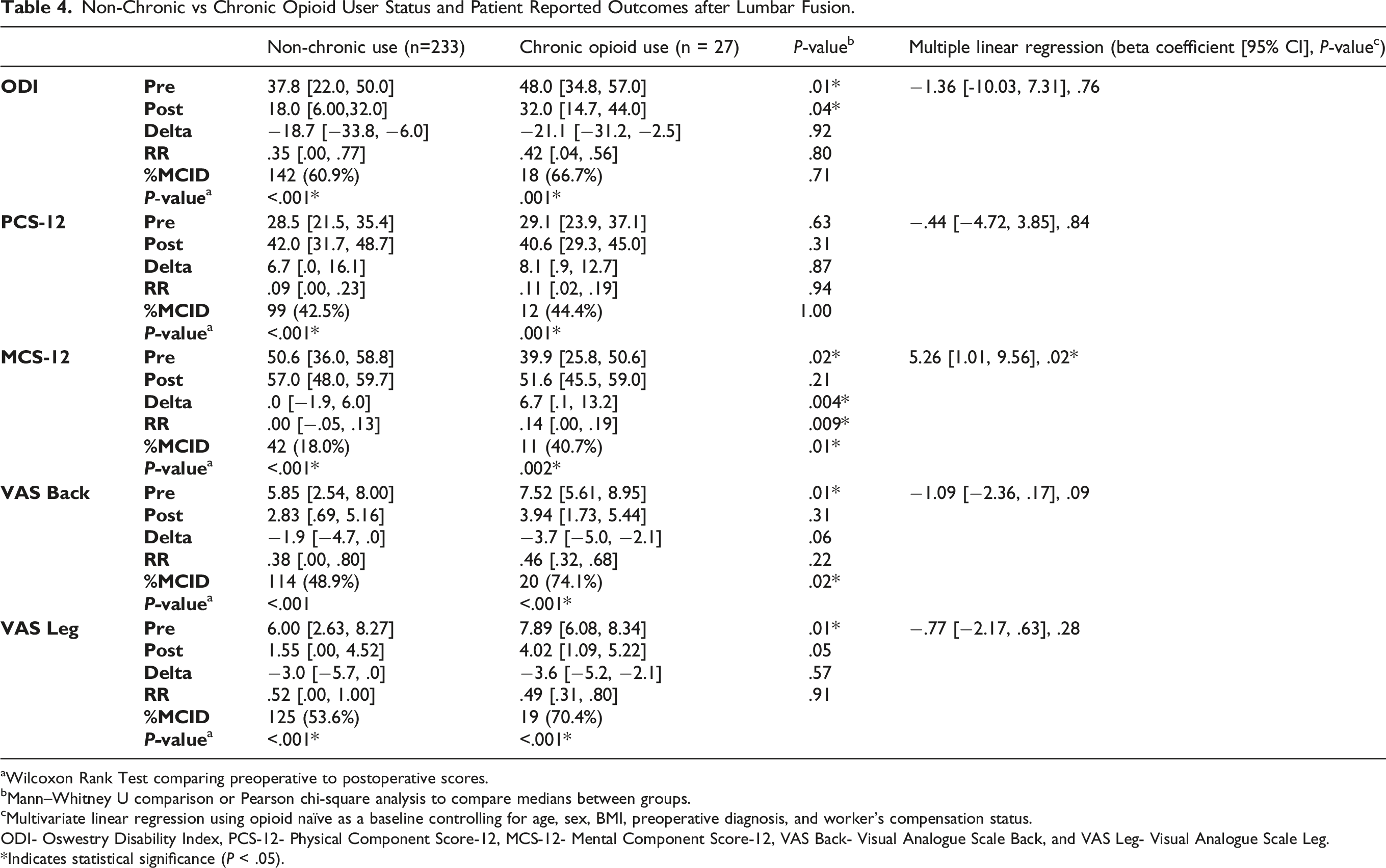
aWilcoxon Rank Test comparing preoperative to postoperative scores.
bMann–Whitney U comparison or Pearson chi-square analysis to compare medians between groups.
cMultivariate linear regression using opioid naïve as a baseline controlling for age, sex, BMI, preoperative diagnosis, and worker’s compensation status.
ODI- Oswestry Disability Index, PCS-12- Physical Component Score-12, MCS-12- Mental Component Score-12, VAS Back- Visual Analogue Scale Back, and VAS Leg- Visual Analogue Scale Leg.
*Indicates statistical significance (P < .05).
After multiple linear regression analysis, chronic opioid use was found to be significantly associated with changes in MCS-12 from baseline to postoperative one-year scores (β = 5.26 [1.01, 9.56], P = .02). Chronic opioid use was not found to be a significant predictor of changes in ODI, PCS-12, VAS-Back, and VAS-Leg scores over time (Table 4).
Patient-Reported Outcome Measurements–Prolonged vs Non-prolonged
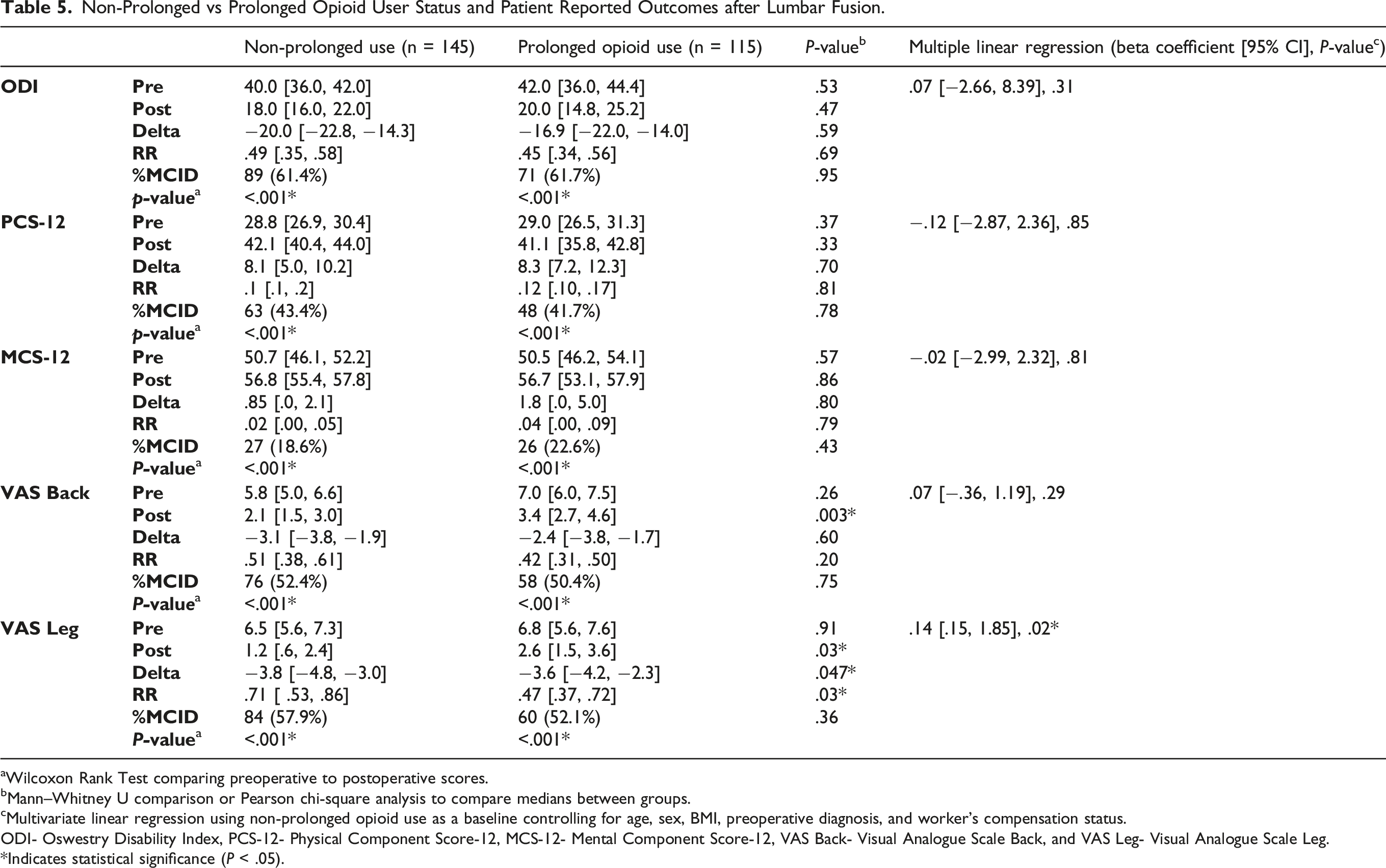
Non-Prolonged vs Prolonged Opioid User Status and Patient Reported Outcomes after Lumbar Fusion.
aWilcoxon Rank Test comparing preoperative to postoperative scores.
bMann–Whitney U comparison or Pearson chi-square analysis to compare medians between groups.
cMultivariate linear regression using non-prolonged opioid use as a baseline controlling for age, sex, BMI, preoperative diagnosis, and worker’s compensation status.
ODI- Oswestry Disability Index, PCS-12- Physical Component Score-12, MCS-12- Mental Component Score-12, VAS Back- Visual Analogue Scale Back, and VAS Leg- Visual Analogue Scale Leg.
*Indicates statistical significance (P < .05).
After multiple linear regression analysis, prolonged opioid use after surgery was found to be significantly associated with worse VAS-Leg score changes over time (β=.14 [.15, 1.85], P = .02). Prolonged opioid use was not predictive of changes in ODI, PCS-12, MCS-12, or VAS-Back (Table 5).
Discussion
For patients with a history of long-term opioid use, spine conditions are among the most common causes for first prescription. 27 And due to the invasive nature of spine surgery, postsurgical pain may remain elevated during the healing process. Thus, this study set out to ascertain risk factors associated with prolonged opioid use after lumbar surgery and elucidate the relationship between chronic preoperative opioid use, prolonged postoperative opioid use, and PROMs.
Our analyses found that current smoking status was most strongly and positively associated with prolonged opioid use after lumbar fusion, while BMI >35 was inversely related. Though chronic opioid users exhibited worse MCS-12 scores preoperatively, they made significantly greater improvements in MCS-12 over time when compared to non-chronic users. Our analyses also demonstrated that prolonged opioid users experienced significantly worse VAS-Back and VAS-Leg scores postoperatively when compared to non-prolonged users. Overall, the cohort exhibited significant improvements across all PROMs after lumbar decompression and fusion.
Consistent with previous reports, our results suggest that current smoking status is a predictor for prolonged opioid use postoperatively.13,28 This observation is likely a byproduct of the link between nicotine and opioid dependence, which has been replicated in widescale population-based investigations. 29 This relationship is multifactorial and involves behavioral sciences, substance use disorders, and socioeconomic vulnerability. 29 However, there may be contention as to how BMI >35 inversely correlates with prolonged opioid use. This finding contrasts a recent national database study by Kalakoti and colleagues 30 that observed an association between “morbid obesity” and prolonged opioid use after lumbar surgery. Although, there are significant methodological differences between Kalakoti’s work and the present study. First, morbid obesity (BMI >40) is a far narrower cohort with a larger comorbidity burden than non-morbid obesity (BMI between 30 and 40). 31 Second, while Kalakoti and colleagues recorded prolonged use at the 1-year postoperative marker, we opted for a stricter cutoff as use beyond 90-days after surgery. Opioid use at the 1-year follow-up may be capturing a subset of patients dealing with chronic pain from conditions unrelated to the lumbar spine. Notably, Rosenthal et al 15 published a prescription drug monitoring program-based study that found that BMI did not predict prolonged opioid use. Another consideration is how much more the contribution of smoking status compares to BMI for predicting prolonged opioid use in our cohort. Cross-sectional studies from the United Kingdom of over 500 000 people have demonstrated that increased smoking correlates with decreased BMI. 32 Furthermore, large scale studies of discordant twin pairs have corroborated this inverse relationship independent of monozygosity vs dizygosity, genetic, and environmental factors. 33 It is plausible that the effects of smoking status and BMI on prolonged opioid use in our cohort are attributable to the population-wide relationship between the two risk factors. Further investigations are warranted on the relationship of smoking and BMI as they pertain to opioid use after spine surgery.
While the present study did not find a link between preoperative mental health comorbidity and prolonged opioid use, our univariate comparisons suggest that the burden of depression and anxiety was significantly higher in the preoperative chronic opioid use group compared to the non-chronic. This builds upon a study of patients undergoing transforaminal lumbar interbody fusion by Villavicencio et al 16 that reported lower MCS-12 scores among opioid users when compared to non-users. The chronic opioid cohort in our investigation reached a median preoperative MCS-12 of 39.9—a score previously thought to be indicative of baseline depression. 34 Furthermore, studies from the cervical spine literature have reported that MCS-12 scores of less than 45.6 predicted worse preoperative physical symptoms. 35 There is reason for optimism despite these trends. Using multiple linear regression, we demonstrated that chronic opioid users before surgery exhibited greater improvement in MCS-12 scores from baseline to one-year postoperatively. Although chronic opioid users ultimately have lower baseline mental function scores, they have more to gain postoperatively than their non-chronic counterparts in this regard. This is in addition to improvements in other PROMs that they are likely to experience after surgery. Altogether, the pattern of MCS-12 scores among chronic opioid use patients is worth consideration by surgeons when risk-stratifying cases and setting expectation for patients before lumbar fusion.
Though increased opioid use both preoperatively and postoperatively contributed negatively to varying outcomes in this study (ODI, VAS-Back, VAS-Leg), patients improved across all outcomes with statistical significance. Our study emphasizes the importance of a patient-centered approach to calibrating opioid prescribing practices before spine surgery. This starts with physicians adhering to strict indications for prescribing opioids to patients undergoing trials of non-operative management. However, the high prevalence of chronic low back pain means that patients are often already on long-term opioids at first visit with a spine surgeon. Thus, recruiting the assistance of pain management specialists prior to surgery for patients with a complicated history of opioid use may lead to reduced risks and improved outcomes. 36 Additionally, patients who are active smokers require supplementary education and guidance given the link between nicotine and opioid dependence. 29 A strategy for minimizing opioid use in this patient population after surgery includes scheduling closer follow-up over the phone or by tele-conference.37,38
Our study does have some limitations. Firstly, the retrospective nature of this case series limited what could be drawn from data collection query. Most notably, patients’ preoperative diagnosis likely varied from their surgical indications since patients are assigned a single primary diagnosis prior to referral. For this reason, the preoperative diagnosis may not fully encapsulate their clinical picture and considerations for decompression and fusion. Furthermore, the analysis between chronic and non-chronic opioid users was limited by the smaller number of patients with chronic use. Although this limits the interpretation of the results, it is notable that we opted for a stricter definition of chronic opioid use to more accurately reflect medication consumption behavior. Previous studies have broadly grouped those with greater than 90-days’ worth of prescriptions based on heterogeneous electronic medical record data alone, without verification of a prescription drug monitoring program. Our strict definition of chronic opioid use also explains how preoperative opioid status was not predictive of prolonged opioid use after lumbar fusion. The proportion of chronic users who achieve normal lengths of opioid use postoperatively is not unfounded and can be as high as 36%.39,40 Additionally, while data collection from a state registry was a notable strength of this study, there are still hypothetical gaps. It is uncertain whether patients consumed medications that were recorded as filled. Even though the Pennsylvania PDMP utilizes an interstate data sharing feature, full implementation with all states is not yet complete, and it is possible some prescription filling may have been unavailable. 41 Furthermore, using only patients who had opioid usage data in the final analysis may introduce selection bias and limit generalizability of these results. Finally, this study did not take into consideration patients who may misuse medications, which could play an important role in preoperative and postoperative opioid usage. 42
Conclusion
Current smoking status and lower BMI were found to be significant predictors for prolonged opioid use after lumbar fusion. Although the retrospective nature of this study does not establish a causal relationship between increased opioid use and worsening patient-reported outcomes, these findings assist spine surgeons when discussing postsurgical pain expectations and expected clinical outcomes with patients who have a history of long-term opioid use.
Supplemental Material
sj-jpg-1-gsj-10.1177_21925682211041968 – Supplemental Material for Predictors of Prolonged Opioid Use After Lumbar Fusion and the Effects of Opioid Use on Patient-Reported Outcome Measures
Supplemental Material, sj-jpg-1-gsj-10.1177_21925682211041968 for Predictors of Prolonged Opioid Use After Lumbar Fusion and the Effects of Opioid Use on Patient-Reported Outcome Measures by Jose A Canseco, Michael Chang, Brian A Karamian, Jennifer Z Mao, Ariana A ReyesMD, John Mangan, Srikanth N Divi, Dhruv KC Goyal, Harold I Salmons, Nicolas Dohse, Noah Levy, Maxwell Detweiler, D Greg Anderson, Jeffrey A Rihn, Mark F Kurd, Alan S Hilibrand, Christopher K Kepler, Alexander R Vaccaro and Gregory D Schroeder in Global Spine Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.