
Abstract
Study Design
Retrospective review.
Objectives
With increased awareness of the opioid crisis in spine surgery, the focus postoperatively has shifted to managing surgical site pain while minimizing opioid use. Numerous studies have compared outcomes and fusion status of different interbody fusion techniques; however, there is limited literature evaluating opioid consumption postoperatively between techniques. The aim of this study was to assess in-house and postoperative opioid consumption across 3 surgical techniques.
Methods
Patients were stratified by technique: posterior lumbar interbody fusion (PLIF), minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF), and cortical screw (CS) instrumentation with interbody fusion. Age, ASA, BMI, depression, preoperative opioid use, EBL, and OR time were recorded and compared across surgical groups using Welch’s ANOVA and chi-square analysis. Total morphine equivalent dose (MED) was tabulated for both in-house consumption and postoperative prescriptions and was compared across surgical techniques using Welch’s ANOVA analysis, Mann Whitney U tests, and linear regression.
Results
Two hundred and thirty nine patients underwent one- or two-level posterior lumbar interbody fusion between 2016 and 2020. One hundred and twenty one patients underwent CS instrumentation, 95 underwent PLIF, and 83 underwent MIS-TLIF. There was a significantly higher percentage of patients who had a history of depression and preoperative opioid consumption in the CS group (P = .001, P = .009). CS instrumentation required significantly less total post-op opioids per kilogram bodyweight compared to MIS-TLIF and PLIF surgeries (P = .029).
Conclusions
Patients who underwent CS instrumentation required less opioids postoperatively. CS instrumentation may be associated with less postoperative pain due to the less invasive approach, however, patient education and prescriber practice also play a role in postoperative opioid consumption.
Introduction
The use of opioid analgesics is a growing public health concern and the rate of opioid prescribing has quadrupled since 1999. 1 With increased prescribing, there is an associated increase in the number of opioid-related adverse events, including high rates of substance abuse disorders, opioid-related hospital admissions, and overdose deaths. 2 The challenge of surgery is that the majority of patients are prescribed some type of opioid pain medication following surgery to help mitigate pain. 3 Furthermore, orthopedics, including spine surgery is reported to have the highest prevalence of postoperative opioid dependence. 3 Despite making up only 2.5% of United States physicians, orthopedists are responsible for 7.7% of all opioid prescriptions. 4
With increased awareness of the opioid epidemic, physicians, including spine surgeons, face the challenge and balance of optimizing perioperative pain management while limiting the risks of opioid use after surgery. Chronic opioid use both before and after lumbar spine surgery has been shown to be associated with higher healthcare utilization and worse postoperative outcomes.5-8
Lumbar spine fusion surgery is one of the most commonly performed spinal surgeries and there are numerous surgical techniques to accomplish interbody fusion. The posterior lumbar interbody fusion (PLIF) procedure was first introduced by Cloward in 1952; 9 however, since then, newer techniques have been developed including transforaminal lumbar interbody fusion (TLIF) and minimally invasive (MIS)-TLIF to accomplish the same goal—obtaining fusion. The TLIF procedure was introduced 30 years later to provide a more lateral approach to the disc space, reducing the amount of thecal sac and nerve root retraction. 10 MIS-TLIF is performed through paramedian incisions and was developed to reduce approach-related muscle damage from midline incision, subperiosteal dissection, and muscle retraction. 11 The cortical bone trajectory was introduced in 2009 as an alternative to pedicle screw fixation. 12 It is considered a less invasive approach with less soft tissue exposure.
Although there is much in the literature comparing outcomes across different surgical techniques, there is no literature to date that has looked at whether the surgical technique impacts postoperative opioid consumption. The aim of this study was to examine if there was an association between surgical technique performed and postoperative opioid consumption in patients undergoing lumbar interbody fusion surgery. Our hypothesis was that patients who undergo either MIS-TLIF or TLIF with CS instrumentation require less opioids postoperatively.
Materials and Methods
Patient Population
Study approval was obtained through the hospital’s institutional review board (IRB approval number 2020P000467). Informed consent was not required as this was a retrospective chart review and there was a waiver of consent. A retrospective review was performed evaluating all patients who had undergone 1- or 2-level lumbar interbody fusion surgery during the period of April 2016 to March 2020. All procedures were performed by 3 surgeons at a single institution. Patients were excluded from this study if it was a revision surgical procedure, more than two fusion levels, or if surgery was performed for trauma, malignancy, or infection.
Data Collection
Patient and surgical data were collected by review of the institutional electronic medical record. Patient demographics included in the study were age, gender, ASA score, BMI, depression, preoperative opioid use, and tobacco use. Patients were grouped by surgical technique performed: posterior lumbar interbody fusion (PLIF), transforaminal lumbar interbody fusion (TLIF) performed with cortical screw (CS) instrumentation or minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF).
Preoperative opioid use status was determined based on prior opioid prescriptions tracked in the electronic medical record. A patient was considered opioid naïve if they had not taken opioids within 6 months of surgery. Tobacco use was self-reported and listed in the social history in the patient’s medical record.
Operative information included the number of fusion levels (1 vs 2), operative time, intraoperative estimated blood loss (EBL), and intraoperative complications. Operative time was defined as time from incision to time of closure.
Hospitalization data included in-house and post-discharge opioid consumption, discharge location, length of stay (LOS), and 30-day readmission or presentation to a medical center. LOS was defined as the number of days spent in the hospital from the day of surgery to the day of discharge. Discharge destination was recorded as either discharge home or to an interim rehabilitation facility. Opioid naïve patients were compared across surgical techniques. Patients with a history of opioid use were excluded given that there is no clear delineation of their start and stop date of opioids given that they are on opioids chronically.
Surgical Technique
All surgeons performed interbody fusion surgery with screw fixation. The three surgeons differ in their surgical technique to obtain interbody fusion. The first surgeon performs a PLIF, which is performed through a midline incision with pedicle screw instrumentation. The second surgeon performs a TLIF, which is also performed through a midline incision, however, in place of pedicle screws, cortical screws are utilized by this surgeon. The third performs a MIS-TLIF via the paramedian approach with pedicle screws. All patients, regardless of surgeon, receive an injection of local anesthetic at the end of the case.
Opioid Consumption
In-house opioid consumption was calculated by totaling all opioids administered during the patient’s hospitalization and converted to morphine equivalent doses (MED). All patients receive a standardized postoperative pain regimen while in-house. This regimen includes Acetaminophen 1000 mg 3 times daily, a muscle relaxant, an oral opioid as needed (prn) for pain and an IV opioid for breakthrough pain. Oral opioid options include tramadol 25–50 mg every 6 hours prn, oxycodone 5–15 mg every 4 hours prn, and Dilaudid 2–6 mg every 4 hours prn. The muscle relaxant prescribed is tizanidine 2–4 mg every 8 hours prn and the breakthrough IV medication is hydromorphone (.5–1.0 mg every 2 hours prn).
Post-discharge opioid consumption was determined by review of the medical record. The medical record shows all outpatient prescriptions, including opioids, and total opioid consumption was determined based on the number of prescriptions a patient received postoperatively. Opioid prescription data included the type of opioid and number of pills prescribed. The total number of prescriptions and number of pills prescribed were calculated and converted to MED. Date of the last prescription was used to determine length of time on opioids after surgery. The most common types of opioids prescribed postoperatively were tramadol, oxycodone, and hydromorphone.
Statistical Analysis
Kolmogorov-Smirnov normality test for variables of interest.
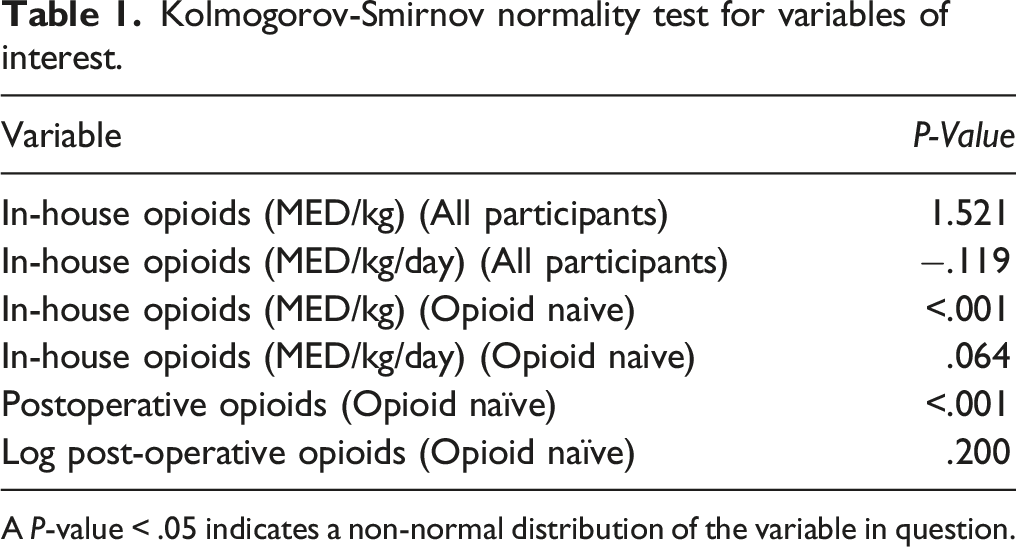
A P-value < .05 indicates a non-normal distribution of the variable in question.
Results
Demographic data and univariate analysis for differences across surgical procedure.
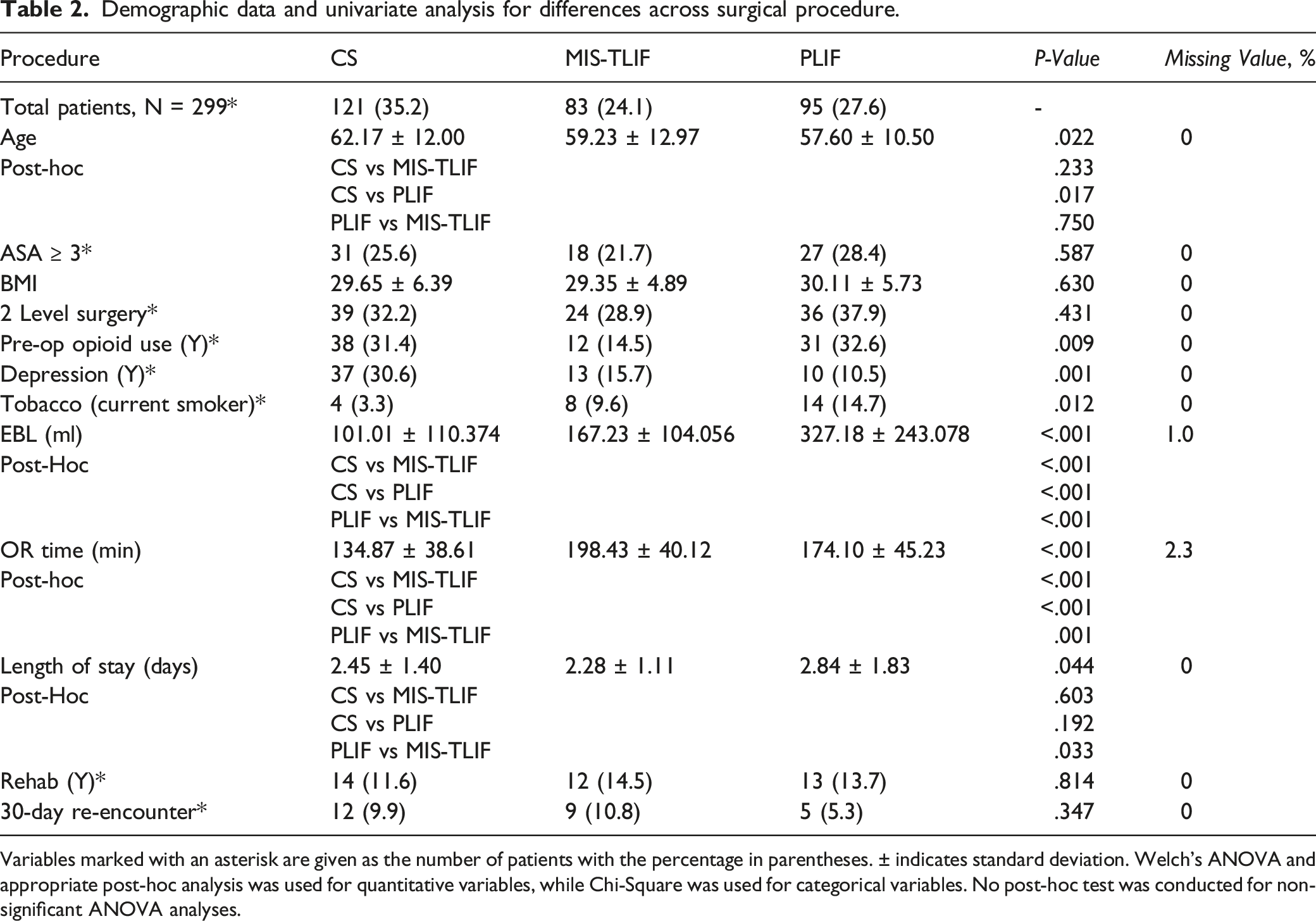
Variables marked with an asterisk are given as the number of patients with the percentage in parentheses. ± indicates standard deviation. Welch’s ANOVA and appropriate post-hoc analysis was used for quantitative variables, while Chi-Square was used for categorical variables. No post-hoc test was conducted for non-significant ANOVA analyses.
Demographic data and univariate analysis for differences across surgical procedure in opioid naïve patients only.
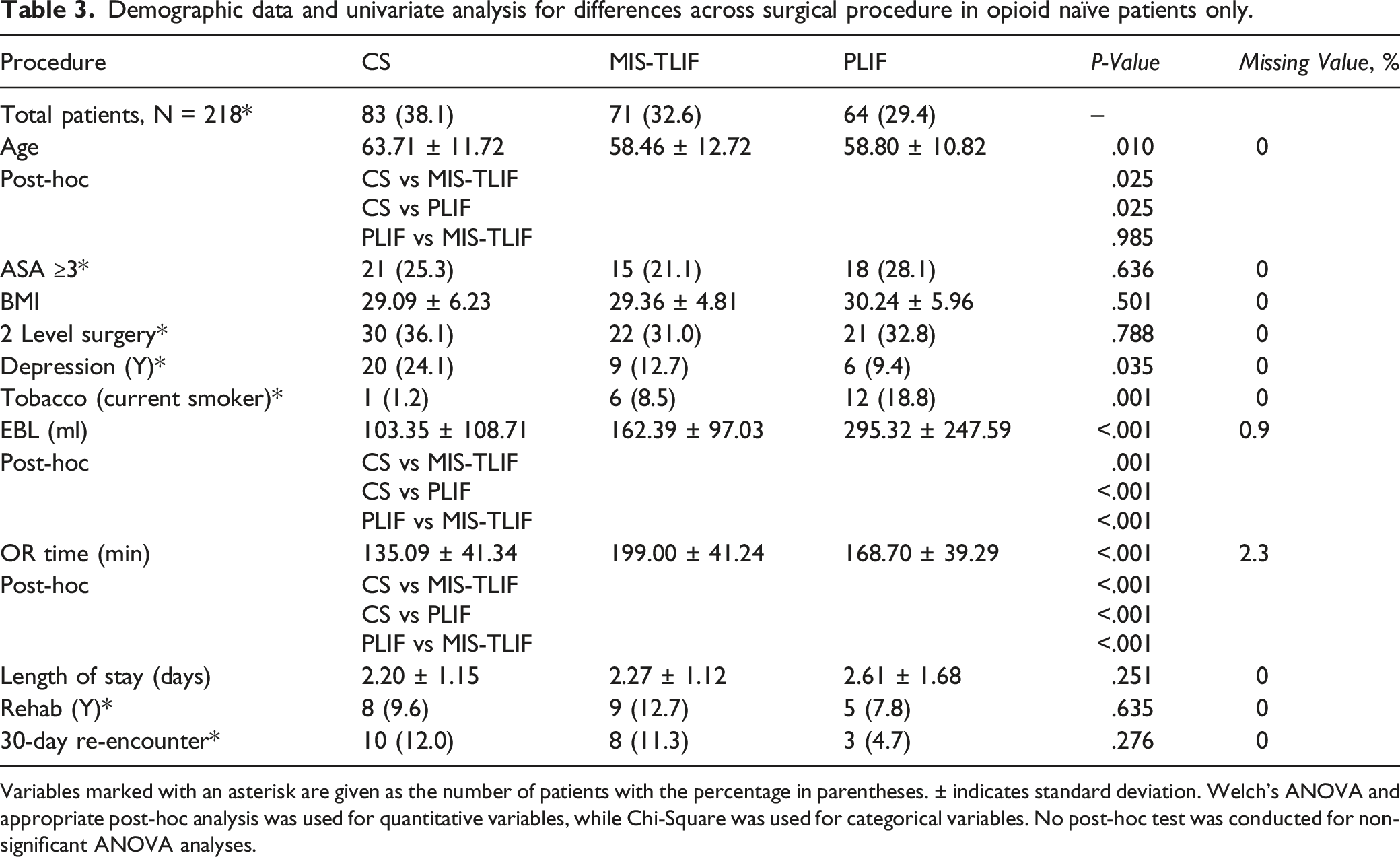
Variables marked with an asterisk are given as the number of patients with the percentage in parentheses. ± indicates standard deviation. Welch’s ANOVA and appropriate post-hoc analysis was used for quantitative variables, while Chi-Square was used for categorical variables. No post-hoc test was conducted for non-significant ANOVA analyses.
Opioid use for opioid naïve patients only: CS vs Non-CS.
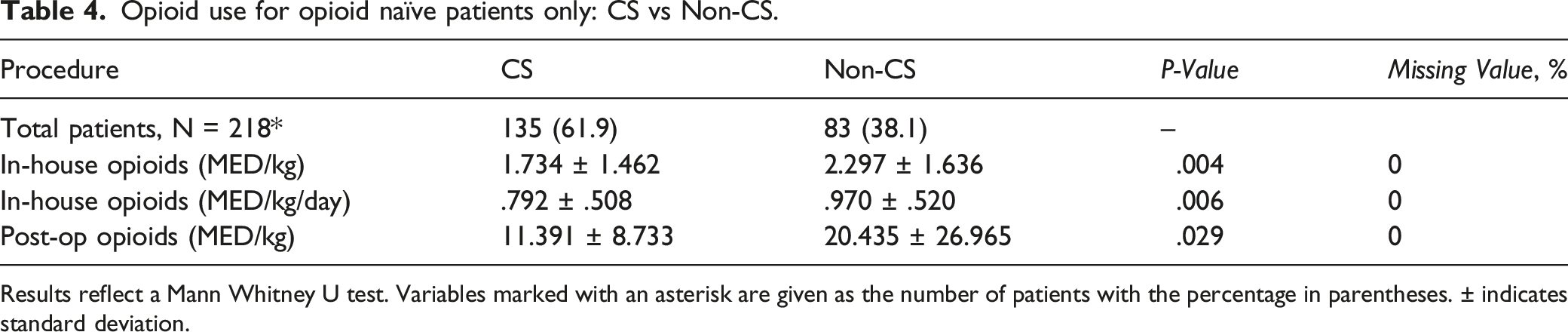
Results reflect a Mann Whitney U test. Variables marked with an asterisk are given as the number of patients with the percentage in parentheses. ± indicates standard deviation.
Opioid use for opioid naïve patients only: CS vs MIS-TLIF vs PLIF.
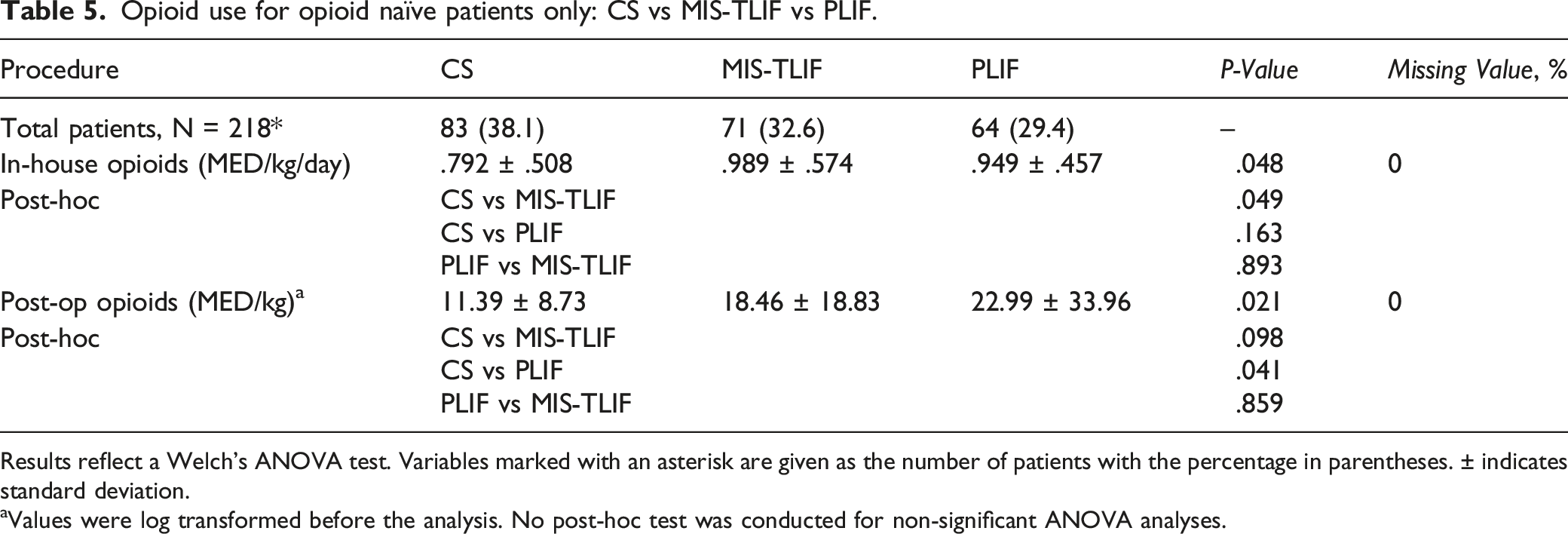
Results reflect a Welch’s ANOVA test. Variables marked with an asterisk are given as the number of patients with the percentage in parentheses. ± indicates standard deviation.
aValues were log transformed before the analysis. No post-hoc test was conducted for non-significant ANOVA analyses.
Multiple Regression for Log post-op MED/kg use in opioid naïve patients between CS and non-CS surgical groups.
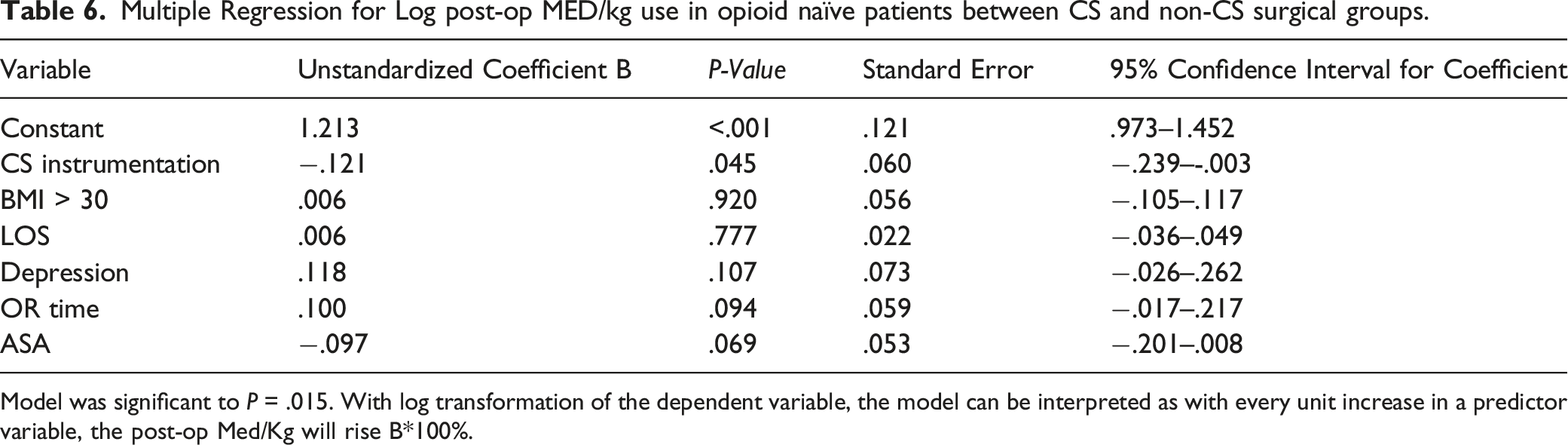
Model was significant to P = .015. With log transformation of the dependent variable, the model can be interpreted as with every unit increase in a predictor variable, the post-op Med/Kg will rise B*100%.
Discussion
This study examined the association between surgical techniques and opioid consumption and found that lumbar interbody fusion performed via TLIF with CS instrumentation is associated with a significantly decreased opioid requirement, both while inpatient and after discharge. There is no difference in discharge destination or 30-day re-encounter rates across surgical techniques.
Recent trends in spine surgery have shown a transition toward minimally invasive surgical approaches over traditional more invasive approaches.13,14 We hypothesized that both MIS-TLIF and TLIF with CS instrumentation would consume less opioids postoperatively, however, we found that TLIF with CS alone consumed the least number of opioids. Cortical bone trajectory (CBT) was introduced in 2009 by Santoni et al., 12 offering an approach with less soft tissue exposure as screws are placed from a medial to lateral trajectory with the starting point between the lateral pars interarticularis and superior articular process. It is considered more minimally invasive than pedicle screws because there is less soft tissue dissection and typically a smaller surgical incision. In comparison, a MIS-TLIF performed via the paramedian approach results in two incisions with dissection through an intermuscular plane between the multifidus and longissimus. The proposed benefit of MIS-TLIF via the paramedian approach is that it is a muscle-sparing approach and maintains the midline structures, however, it does still result in muscle dissection, which could explain why these patients did not consume as low of numbers of opioids compared to TLIF with CS instrumentation.
There is conflicting literature regarding postoperative pain between CS and PS instrumentation. Lee et al 15 found that CBT was associated with lower immediate postoperative pain compared to pedicle screws and attributed this to a smaller incision, decreased disruption of muscle attachments, and less soft tissue dissection. Furthermore, Sakaura et al. 16 investigated Japanese Orthopedic Association (JOA) score between CBT and PS patients and found that both improved compared to preoperative scores, however, recovery rate of JOA score in the CBT group was significantly higher. This is in contrast to Chen et al. 17 who found no difference in postoperative back pain in the immediate postoperative period between the two cohorts. Our study shows that patients who underwent CS instrumentation with TLIF required less in-house and post-discharge opioids, which further supports the findings of previous studies suggesting that CS instrumentation is less invasive resulting in less postoperative pain.
The majority of US state legislatures have passed mandatory opioid prescription limits with the goal to minimize the number of opioids prescribed after spine surgery. The development of effective policies and strategies to minimize long-term opioid use is of paramount importance. Previous studies have shown that the implementation of a statewide opioid-limiting legislation has led to a significant reduction in initial and 30-day opioid prescriptions following lumbar spine surgery.18,19 As prescribers have become more aware of the risks of prolonged opioid use, prescribing practices have changed and many prescribers adopt more stringent postoperative practices to minimize prolonged use. Patient education continues to play an important role and setting patient expectations on postoperative pain and opioid utilization in the perioperative period is critical. All surgeons at our institution prioritize minimizing opioids whenever possible and have created a standard postoperative spine order set that includes a multimodal approach to pain control to help minimize opioid consumption.
We recognize the limitations of the study. As a retrospective examination of collected data, this study is at risk of the biases inherent to all retrospective research. Although the groups were heterogenous, we controlled for potentially confounding variables in the regression analysis. While we were able to summate the total number of prescriptions and total pills prescribed to patients postoperatively, we are unable to determine how many pills patients consumed. Therefore, it is possible that MED consumed may be less than those filled at pharmacies. Another limitation is that each surgeon performs primarily one surgical technique, and we are unable to control for each individual surgeon’s prescribing practices. Although we cannot control for the variability in post-discharge prescribing practices across the 3 surgeons, we do see that while in-house, with the standardized postoperative pain regimen, that patients who underwent TLIF with CS instrumentation consumed less opioids. This speaks to the fact that patients with CS instrumentation required fewer opioids postoperatively rather than looking solely at surgeon prescribing habits after discharge from the hospital.
This is the first study to evaluate the effect of lumbar interbody surgical technique on postoperative opioid use. The results demonstrate that patients who underwent interbody fusion with CS instrumentation consumed less opioids while inpatient and were prescribed less opioids after discharge from the hospital. These results could be the result of the CS technique itself or could also be a result of prescriber practice and patient education.
Conclusions
With increased awareness of the opioid crisis in spine surgery, the focus postoperatively has shifted to managing surgical site pain while minimizing opioid use. Although there is much in the literature comparing outcomes across different surgical techniques, to our knowledge, this is the first study that has evaluated the impact of surgical technique on postoperative opioid consumption. Our current study observed an association between CS instrumentation and less postoperative opioid use, both while inpatient and after discharge. CS instrumentation may be associated with less postoperative pain due to the less invasive approach and decreased disruption of the muscular attachments; however, we recognize the importance of patient education and prescriber practice and the role these play in postoperative opioid consumption. At this time, we understand that our results may not change or determine a surgeon’s surgical technique, and future studies are needed exploring postoperative opioid consumption across surgical techniques. Our results are the first to highlight that surgical technique may play a role in minimizing postoperative opioid consumption.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.