
Abstract
Study Design:
Retrospective review.
Objective:
To determine the effectiveness of erector spinae plane (ESP) blocks at improving perioperative pain control and function following lumbar spine fusions.
Methods:
A retrospective analysis was performed on patients undergoing
Results:
There were 37 in the block group and 39 in the control group. There was no difference in preoperative opioid use (P = .22). On postop day 1, MED was reduced in the block group (32 vs 51, P < .05), and more patients in the block group did not utilize any opioids (22% vs 5%, P < .05). The block group ambulated further on postop day 1 (312 ft vs 204 ft, P < .05), and had reduced length of stay (2.4 vs 3.2 days, P < .05). The block group showed better PROMIS PI scores postoperatively (58 vs 63, P < .05). The novel delivery technique was validated and successful in targeting the correct level and plane.
Conclusions:
ESP blocks significantly reduced postop opioid use following lumbar fusion. Block patients ambulated further with PT, had reduced length of stay, and had improved PROMIS PI postoperatively. Validation of the block demonstrated the effectiveness of a novel fluoroscopic delivery technique. ESP blocks represent an underutilized method of reducing opioid consumption, improving postoperative mobilization and reducing length of stay following lumbar spine fusion.
Introduction
Postoperative pain control following lumbar spine surgery presents a significant challenge for anesthesia and orthopedics. The present opioid epidemic has highlighted the importance of alternative methods of pain control following surgery.1-3 Regional anesthesia is highly utilized in orthopedics and has helped to improve perioperative pain control in most orthopedic subspecialties. Despite this, the use of regional anesthesia for lumbar spine surgery is not well established. Erector spinae plane (ESP) blocks represent a relatively new non-opioid regional anesthesia pain management technique with promising early results. ESP blocks represent a possible regional anesthetic option for lumbar spine surgery but have yet to be widely implemented or studied.
ESP blocks were first described by anesthesia for the management of thoracic neuropathic pain in 2016. 4 Since their introduction there has been rapid implementation across both surgical and medical fields. ESP blocks have demonstrated effectiveness at improving pain control postoperatively across other specialties including cardiothoracic, oncologic, vascular, and general surgery.5-9 In addition, ESP blocks have been employed for pain control for many nonsurgical conditions. For example, emergency medicine, medical oncology and palliative care have utilized ESP blocks effectively to reduce pain for a variety of post traumatic and general medical ailments.10,11 Additionally, multiple studies have demonstrated the effectiveness of ESP blocks at reducing opioid consumption postoperatively and for non-surgical conditions.12,13
Despite the proliferation of research surrounding ESP blocks, there is a paucity of literature concerning its use for lumbar spine surgery. ESP blocks for lumbar spine surgery have only been described in limited studies.14-18 A recent systematic review of ESP blocks for spine surgery highlighted only 11 total publications with 171 total patients on the topic. Only 3 referenced studies were not either case reports or case series. 14 This review concluded that ESP blocks in the lumbar spine are controversial and highlighted the need for additional studies. Of the 2 known higher-level studies, each study had 40 or fewer total patients. One study noted postoperative pain improvements with ESP blocks but only examined lumbar decompressions, while the other utilized thoracic (not lumbar) ESP blocks for all comer spine surgery with inconclusive results.15-16 Additionally, ESP block delivery by ultrasound guidance is the traditional described delivery technique and the only technique described in the literature. 4 We know of no studies demonstrating ESP block delivery via fluoroscopic technique without ultrasound, or of any studies where ESP blocks are performed by spine surgeons themselves as opposed to an anesthesia team. There were 2 main aims of this study. The first aim was to determine whether ESP blocks improve postoperative pain control and function following lumbar fusions. The second aim was to demonstrate a novel fluoroscopically guided technique for the delivery of these blocks in the lumbar spine.
Materials and Methods
Study Design and Patient Population
This is a retrospective cohort study with patient collection from May to December 2019. Following approval from the Institutional Review Board approval, all patients undergoing 1 to 3 level lumbar decompressive laminectomies with posterolateral lumbar instrumented fusions for degenerative conditions were identified. Patients were excluded who were less than 18 years old, undergoing revision surgery, or having surgery for trauma, tumor, or infection. All patients were treated at the same tertiary university-based spine center by 4 different spine surgeons. All patients that were included in the study had surgery performed in the traditional open fashion without any major technical surgical variations. Two cohorts were identified for comparison; patients who received a preoperative ESP block via fluoroscopic technique (composed of patients of 2 surgeons who routinely performed ESP blocks), and patients who did not receive a block (composed of patients of 2 surgeons who do not perform ESP blocks). In-hospital data was collected via the electronic medical record Epic (Verona, WI). Additionally, pre- and post-operative patient reported outcomes, including Numerical Rating Scale (NRM, VAS) for back and leg pain, Oswestry Disability Index (ODI) and Patient Reported Outcomes Measurement Information System (PROMIS) Physical Function and Pain Interference Computer Adaptive Test measures (PF CAT and PI CAT) were collected at all physician clinic visits.
Fluoroscopic Technique for Erector Spinae Plane Block
After intubation in the OR, patients were flipped prone onto an open belly Jackson Frame (Mizhu OSI, Union City, CA) in standard fashion. The lumbar spine was cleaned with Chloraprep. AP fluoroscopy was used to identify the transverse processes of a single level. 0.4 mg Dexamethasone and 30cc’s of 0.5% bupivacaine were mixed in sterile fashion and attached to a 22-gauge spinal needle via extension IV tubing. The spinal needle was advanced under fluoroscopic guidance until contacting the middle to lateral third of the transverse process. 15cc’s were then delivered in the subfascial plane. This process was repeated for the contralateral side. Significant pressure is encountered when in the correct subfascial plane, which lies on and just above the transverse process. The patients were then prepped and draped in the usual sterile fashion. The technique of ESP delivered by the surgical team via fluoroscopic technique was validated against the traditional ultrasound method by the anesthesia team. Omnipaque contrast was added to the block cocktail in a 1:1 concentration for easy radiographic identification. AP and lateral fluoroscopy were used to record the lumbar level blocked, the cranial caudal extent of medication spread and the depth of delivery in a 5-patient cohort prior to the study (Figures 1 and 2). Time required for delivery was also recorded. All measures for the fluoroscopic technique met or exceeded the ultrasound technique in less time (Table 1).
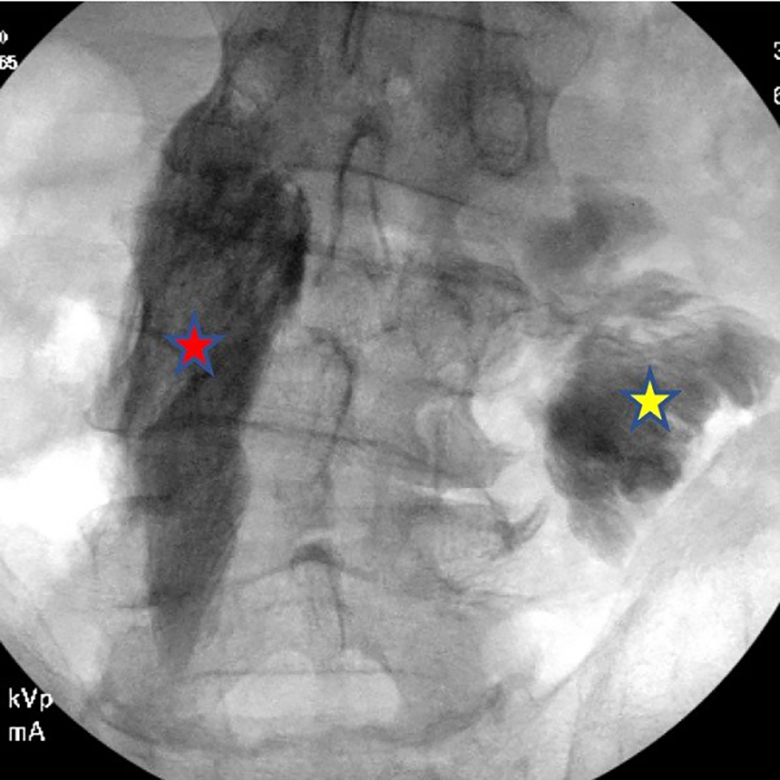
AP fluoroscopic image showing ESB delivered on the left L4 level via novel technique (red star) and via the traditional ultrasound method at the right L4 level (yellow star). Omnipaque contrast demonstrates correct fascial plane spread of the block from L3-L5 from the novel technique on the left, and failed delivery by the traditional ultrasound guided method in the intramuscular plane on the right with spread limited to the L4 level.
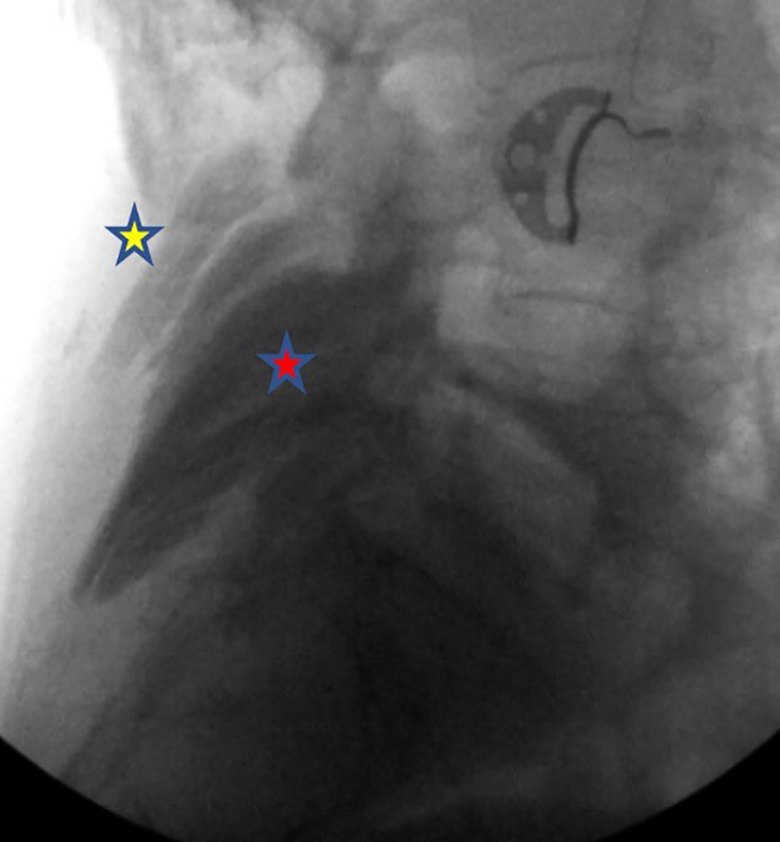
Lateral fluoroscopic image showing ESB delivered at the L5 level via the novel fluoroscopic technique. Omnipaque contrast (red star) demonstrates fascial plane spread of the block at the appropriate depth. Superficial contrast (yellow star) demonstrates failed delivery by the traditional ultrasound guided method in the intramuscular plane on the contralateral side.
Technique Validation Data.
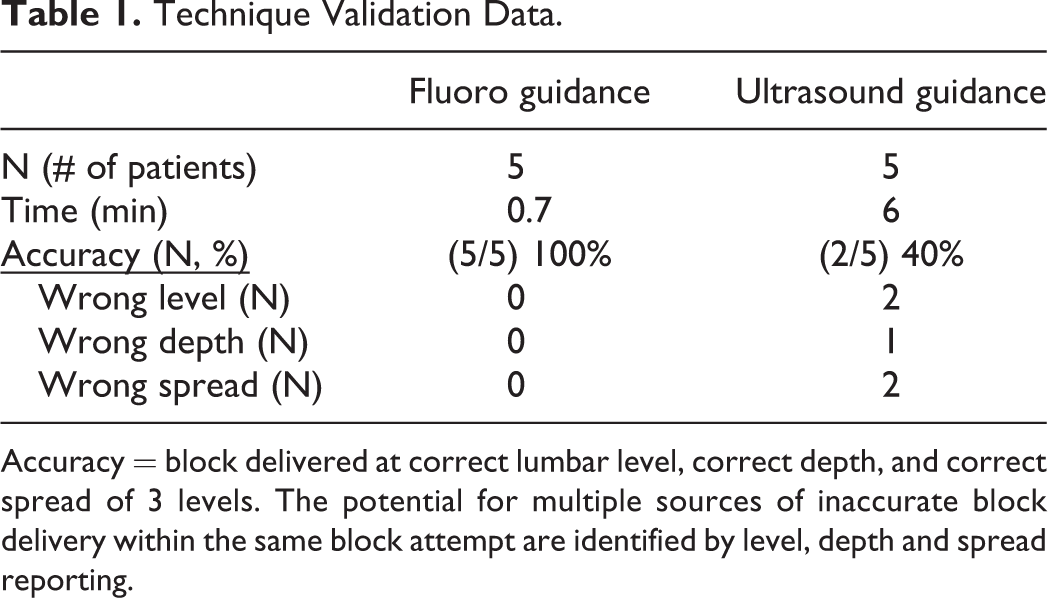
Accuracy = block delivered at correct lumbar level, correct depth, and correct spread of 3 levels. The potential for multiple sources of inaccurate block delivery within the same block attempt are identified by level, depth and spread reporting.
Outcome Tools
Morphine Equivalent Dosage (MED)—All opioid usage while in the hospital was converted to morphine equivalent dosing using opioid equianalgesic calculations. Ambulation—Physical therapy visited all patients on postop day 1 per standard protocol. They recorded patient ambulation in feet at each therapy session. Length of Stay—EPIC admission and discharge time stamp documentation was used to calculate patient length of stay in hour increments. Patient demographics were analyzed using standard descriptive statistics including mean and standard deviation. Basic descriptive statistics and confidence intervals were calculated for all outcome measures. Two-tailed student’s T-test and Chi-square analysis were used for all comparisons between groups with statistical significance set at P
Of note, the frequency distribution for postop day 1 MED was right skewed, but had reasonably similar standard deviations and variances between the cases and controls. A formal Shapiro-Wilks test confirmed a non-normal distribution. Because there was some evidence of a violation of the assumptions for a t-test with equal variance we examined our results using t-test with unequal variances, as well as with log-transformed data. These alternative parameterizations did not change the inferences or conclusions. As such, we have reported our primary findings based on the assumption of equal variance.
Results
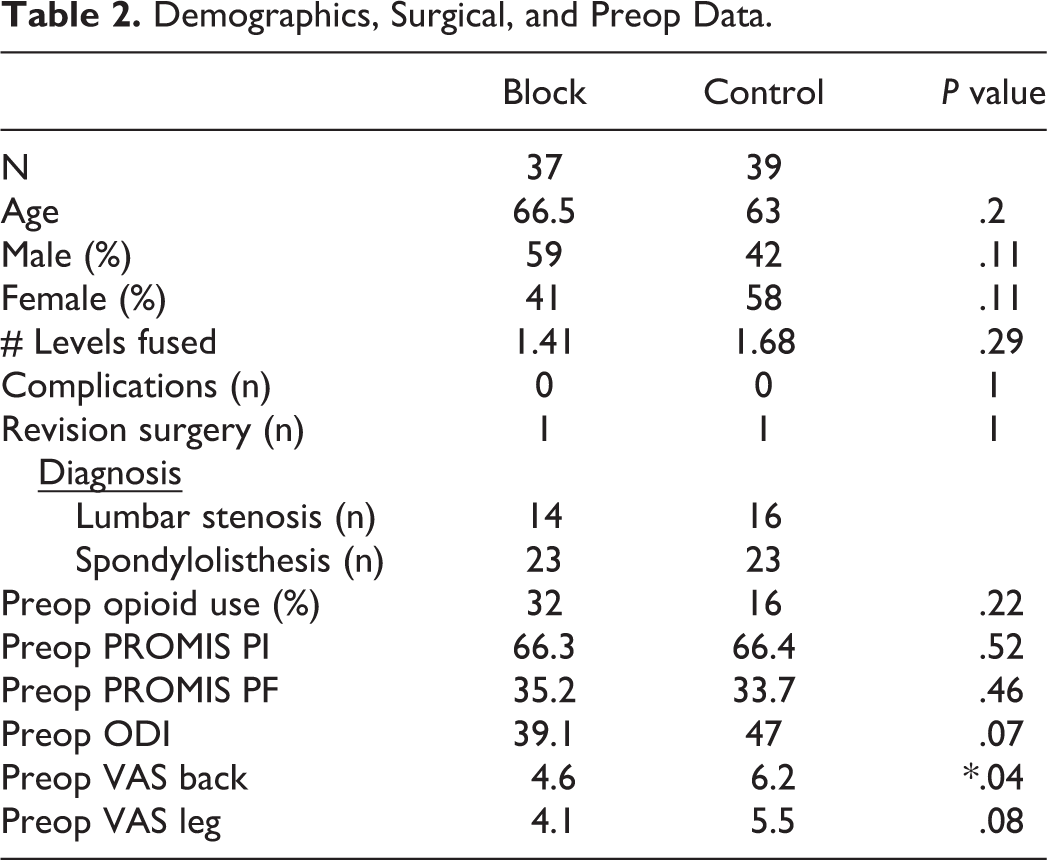
A total of 76 patients met inclusion criteria. Thirty-seven patients received a preoperative ESP block (Block group) and 39 patients were included in our control group. The average age was 66.5 years in the block group and 63 years in the control group (P = .2). The block group was 59% male, while the control group was 42% male (P = .11). The most common diagnosis was lumbar spinal stenosis (n = 30/76, 39%) and lumbar degenerative spondylolisthesis with stenosis (n = 46/76, 61%). The average number of levels fused was 1.4 in the block group and 1.7 in the control group (P = .29, range 1-3 levels). There were no reported complications in either group. One patient returned for revision surgery in each group for a traumatic compression fracture adjacent to the fusion. 32% of the block patients reported using narcotic pain medications preoperatively compared to 16% in the control group (P = .22). There were no preoperative differences in outcome measures between groups with the exception of VAS Back which was worse in the Control group (P = .04). Demographic and surgical data is summarized in Table 2.
Demographics, Surgical, and Preop Data.
The block group utilized significantly less opioid pain medication on postop day 1 (Average MED = 32) compared to the control group (Average MED = 51) (P = .04). Significantly more patients did not utilize any opioids on postop day 1 in the block group (n = 8/37, 22%) compared to the control group (n = 2/39, 5%) (P = .03). Patients in the block group ambulated further with physical therapy on postop day 1 compared to the control group (312 feet vs. 204 feet, P = .01). Patients in the block group had reduced length of stay compared to the control group by nearly 1 day on average (2.4 days vs. 3.2 days, P = .03). Data is summarized in Table 3.
Group Comparisons.
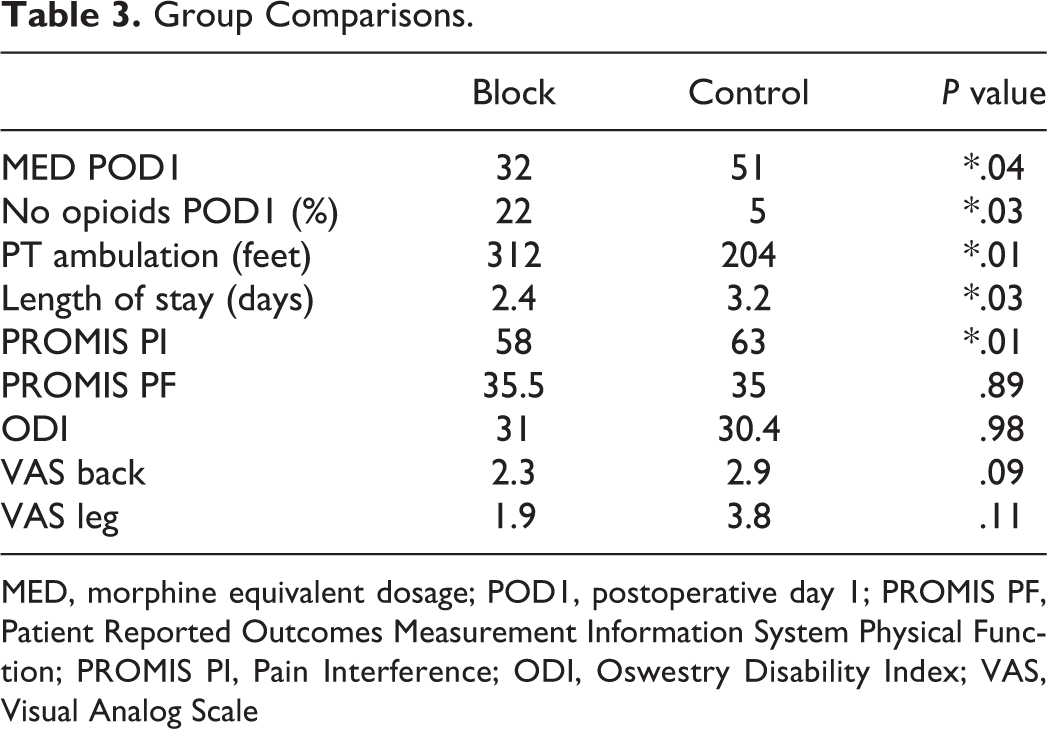
MED, morphine equivalent dosage; POD1, postoperative day 1; PROMIS PF, Patient Reported Outcomes Measurement Information System Physical Function; PROMIS PI, Pain Interference; ODI, Oswestry Disability Index; VAS, Visual Analog Scale
At the first follow up visit at 6 weeks patients in the block group had lower average PROMIS PI scores compared with the control group (58 vs 63, P = .01). There were no significant differences in PROMIS PF or ODI between groups at 6 week follow up. There was an overall trend toward lower VAS leg and VAS back pain scores in the block group compared to control group at 6 weeks, but these differences did not reach significance (VAS Leg = 1.9 vs 3.8, P = .11, VAS Back = 2.3 vs 2.9, P = .09). VAS Leg in the block group approached MCID (Minimal Clinically Important Difference) for VAS with a difference of 1.9 (MCID = 2). Data is summarized in Table 3. Both groups had significant improvements in all outcome measures from preop compared to the 6 week follow up with the exception of PROMIS PF. Data is summarized in Table 4.
Outcomes Data.
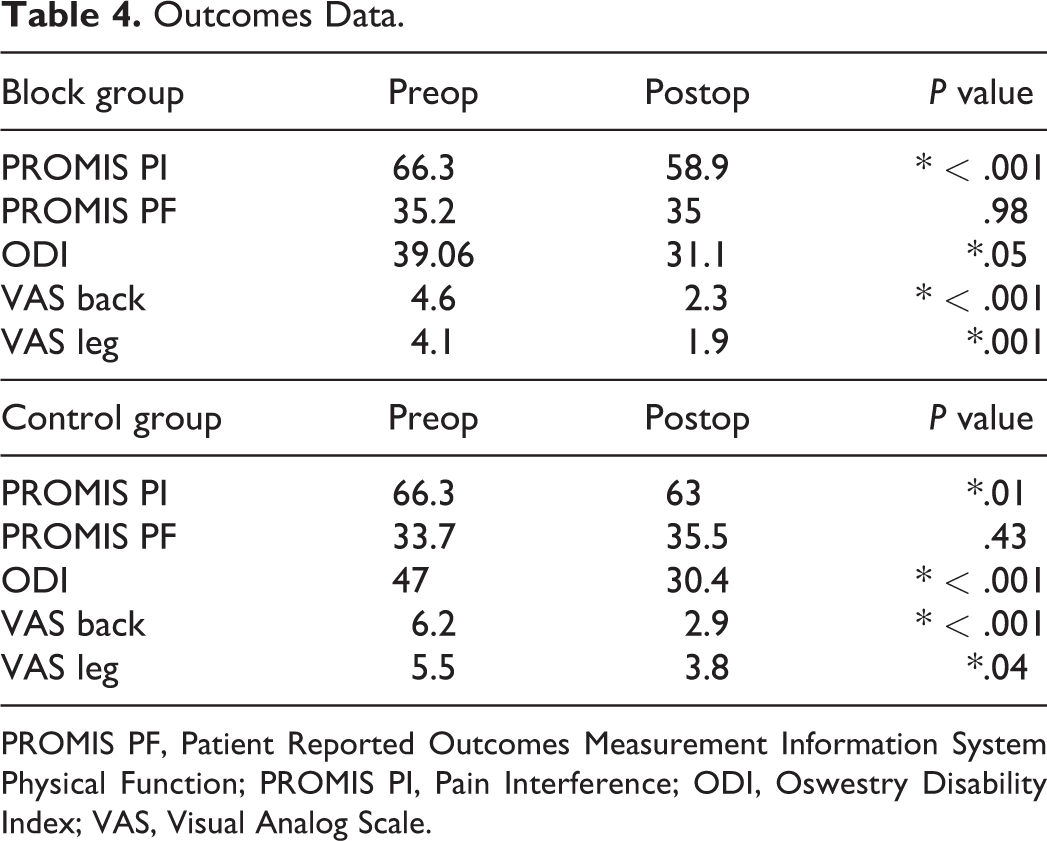
PROMIS PF, Patient Reported Outcomes Measurement Information System Physical Function; PROMIS PI, Pain Interference; ODI, Oswestry Disability Index; VAS, Visual Analog Scale.
Discussion
Pain control following lumbar spine surgery presents a significant challenge and has drawn additional focus in the present opioid epidemic.1-3 Despite the wide success of regional anesthesia in orthopedics, spine surgeons have been slow to adopt any such treatments. ESP blocks have seen success in operative and nonoperative pain control efforts across specialties since their initial description 4 years ago. 4 Specific attention has been given to their ability to reduce opioid consumption postoperatively. Even though ESP blocks have been well described, minimal research exists within the field of spine examining the potential benefits for lumbar spine surgery.14,15 The objectives of the present study were to determine whether ESP blocks improve postoperative pain control and function following lumbar fusions, and to demonstrate a novel fluoroscopic technique for the delivery of these blocks in the lumbar spine.
ESP blocks were first described by Forero et al in 2016 as a novel anesthetic technique for the management of thoracic neuropathic pain via the targeting of the dorsal and ventral rami of spinal nerves. 4 They described ESP blocks as simple and safe to perform, in addition to noting the potential benefits for postoperative care and posttraumatic conditions. Since then over 200 studies have been published on the benefits of ESP across specialties. Surgical specialties operating in and around the thorax and abdomen such as general, cardiac, thoracic, vascular, and oncologic surgery have all described significant benefits for postoperative pain control.7-9,12,13 Specifically, general surgeons have noted improved pain control following ventral and inguinal hernia repair and bariatric surgery, and thoracic surgeons have effectively improved pain control following lobectomies. 7-9,12,13 Oncologic breast surgeons implemented ESP blocks early on, noting significant improvements in pain control in randomized control trials. 9 Surgeons have also noted significant reductions in opioid consumption and improved function postoperatively across multiple fields. A prospective matched cohort study of patients undergoing elective cardiac surgery with cardiopulmonary bypass showed substantial reduction in postoperative opioid consumption, earlier mobilization, and reduced adverse postoperative events. 5 A systematic review of breast surgeries identified over 30 articles and 6 randomized control trials showing reduced opioid consumption and improved satisfaction following ESP blocks. 7 Emergency departments have utilized ESP blocks for renal colic, burns, rib fractures, and pancreatitis with similar results. 11
Limited case series in spine surgery have also demonstrated improved pain control and reduced opioid consumption following lumbar surgeries but have significant limitations. For example, 1 such case series examined 5 patients who underwent bilateral thoracic ultrasound guided ESP blocks prior to lumbar spine surgery. 15 Patient results implied improved postoperative pain control but no statistical analysis was performed. Additionally, the patients had wide ranging diagnoses and procedures and they examined very few outcome measures. The other known study examined 18 patients who received a lumbar ESP block prior to lumbar decompression without fusion. Results showed improved pain control and opioid use compared to controls. 14 However, that study only examined micro-endoscopic decompressions and only collected the NRS (Numeric Rating Scale) for pain and the number of IV opioid boluses delivered postoperatively, limiting the overall conclusions. Both series lack significant patient numbers, common diagnoses and/or procedures and broad outcome metrics examined over time. Additionally, no prior study has examined ESP blocks delivered via fluoroscopy by the surgical team.
The results of this study demonstrate multiple statistically significant postoperative advantages for patients in the block group. Block group patients required significantly less postoperative opioids, ambulated further with physical therapy, and discharged nearly 1 day earlier than their control counterparts with nearly a quarter of block patients not requiring any postop opioids. At the first postoperative follow up, block patients had significantly lower PROMIS PI scores than control patients, demonstrating a potential longer-term benefit of the block. In addition, the validation of the fluoroscopic technique demonstrated that the novel technique met or exceeded the accuracy of the traditional ultrasound technique in less time, and highlighted the reliable administration of the block when performed by the surgeon.
Overall the findings of this study agree with prior literature on ESP blocks. Our results are in line with multiple studies across surgical subspecialties demonstrating improved pain control following surgery. Additionally, our findings align well with multiple prior studies demonstrating a significant reduction in postoperative opioid use. The results of this study agree with and expand significantly upon the limited studies demonstrating improved pain control with ESP blocks following lumbar spine surgery, filling a notable void in the spine literature. Our study is the first to focus on the effect of ESP blocks on specific degenerative lumbar diagnoses treated by decompressive laminectomies and posterior instrumented fusions. In addition, it is the largest study examining ESP blocks to date in the lumbar spine and includes a control group. This study is the first to examine physical function in addition to pain control in the form of ambulation with physical therapy, time to discharge, and multiple legacy outcome metrics. Interestingly, our results demonstrate a significant reduction in opioid use despite nearly twice as many patients in the block group using opioids preoperatively. This reduction in opioid use in a group with nearly double the rate of preoperative opioid use is especially interesting given the fact that many studies have demonstrated worse pain control post operatively in patients using opioids preoperatively. Finally, we are the first study to describe the effectiveness and efficacy of a novel ESP delivery technique performed by spine surgeons under fluoroscopy. This technique demonstrated success with all measures, meeting or exceeding the traditional ultrasound technique in less time in technique validation. This study suggests that spine surgeons do not need to rely on anesthesia to perform ESP blocks, and may empower surgeons to perform their own blocks with a safe and easy technique.
In light of these results, it is important to mention the reasons for performing the ESP block in the manner described. Administering the block prior to skin incision is critical in that it creates a high-pressure pocket of anesthetic fluid in the subfascial plane that rapidly expands across multiple spinal levels. If the block is performed after incision and disruption of the paraspinal musculature this high-pressure pocket would not form and could theoretically limit the spread of medication. In addition, delivering the block prior to disruption of the tissue planes may help to prevent the rebound pain effect described via the pain receptor sensitization theory. 19 All of these factors likely contribute to the effectiveness of ESP blocks seen in this study.
There are several limitations to the present study. We recognize that there are unavoidable technical differences and variation between surgeons in the 2 groups, and that it is not possible to fully and properly control such differences in this type of retrospective analysis. We attempt to limit this by all surgeons treating select diagnoses in the same traditional open fashion, but this still does not fully remove the effects of surgeon variation. Because of this and the additional limitations below, we have initiated and are currently enrolling patients in a prospective study with a proper power analysis to follow up our retrospective observations with more powerful research. Overall patient numbers were limited due to the short amount of time that our group had been performing ESP blocks at the time of the study. Preoperative VAS back scores were higher in the control group, which could have had an effect on the results. Additionally, while not statistically significant, there were more females present in the control group. Similarly, due to the retrospective nature of the study and limited patients fitting inclusion criteria, our group did not have enough patients to properly power a study examining a single diagnosis or a specific number of total levels fused. This study also lacked an arm specifically comparing the outcomes of the traditional ultrasound method to the novel technique. Additionally, longer-term studies are required to evaluate improvements in ODI and PROMIS PF as we would not expect to see marked improvements in these categories at 6 weeks.
Our future goals for investigation include the development of a larger multicenter randomized control trial. This would provide the well-known benefits of such a study including higher power, randomization and patient matching. We also plan to perform a similar study on patients undergoing isolated lumbar decompressions to see if that patient population would enjoy similar benefits to those patients undergoing fusions. Additionally, we plan to further investigate the accuracy of both fluoroscopic and ultrasound guided lumbar ESP block delivery, as there are no studies examining block accuracy in the literature. The clinical applications of this study are significant. As the benefits of ESP blocks for lumbar spine surgery continue to be examined, we hope their application will become more widespread among spine surgeons. Our description of a novel technique that is both easy to perform and reproducible is essential to accomplishing that goal. ESP blocks are well suited to become a useful tool for improving patient pain control and function and for limiting opioid use following lumbar spine surgery. The novel ESP block technique allows spine surgeons to easily and safely incorporate these blocks into their own practice with their own hands.
In conclusion, ESP blocks delivered via a novel fluoroscopic technique significantly reduce postoperative opioid use following lumbar fusions. Block patients ambulate further with PT, have reduced length of stay, and have improved PROMIS PI postoperatively. ESP blocks are an underutilized method of improving perioperative pain control following lumbar spine fusions and may represent an adjunct to current practices that can substantially impact the patient experience.
Footnotes
Authors’ Note
The manuscript submitted does not contain information about medical device(s)/drug(s). Relevant financial activities outside of the submitted work: grants. The study was approved by our institutional IRB and did not require informed consent given the data reviewed was deidentified and collected in accordance with the institutions standard of care. IRB approval number 00 069 703.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.